Βιοαπορροφήσιμες...
41
Παύλος Στουγιάννος Καρδιολόγος ΓΝΑ «Η ΕΛΠΙΣ»
Transcript of Βιοαπορροφήσιμες...

Παύλος ΣτουγιάννοςΚαρδιολόγος
ΓΝΑ «Η ΕΛΠΙΣ»

Historical overview of the most prominent advances in stent technology
Bioabsorbable scaffolds : the fourth revolution in interventional cardiology

Concerns-problems with the use of stents
Vascular Health and Risk Management 2012:8 125–132
Sustained inflammation attributed to the presence of apermanent foreign body in the vessel wall
Risk of stent thrombosis at long-term follow-up
Prolonged double antiplatelet therapy
Future treatments in the vessel if needed (either PCI orCABG)
Access to side branches initially jailed by the stent
Follow-up with noninvasive techniques such as MSCT

Potential advantages of bioresorbable scaffolds (BRS) over BMS and DES
Vascular Health and Risk Management 2012:8 125–132


Leading compounds and degradation end-products according to type of polymer family
Onuma Y, Serruys P. Circulation 2011;123:779-797

Mechanical properties and degradation time for different polymers
Onuma Y, Serruys P. Circulation 2011;123:779-797

The reaction pathway for hydrolytic degradation of the PLA family of polymers

Igaki-Tamai PLLA stent
Coronary angiography performed 10 years after implantation


The Absorbable Metallic StentAMS-1 magnesium alloy
Onuma Y, Serruys P. Circulation 2011;123:779-797
High restenosis rate TLR at 1 year 45%

DREAMS G2
Improved design
Limus derivative drug
Clinical study
AMS
Magnesium alloy
No drug coating
Clinical study
DREAMS
Refined magnesium alloy
Paclitaxel drug + PLGA
Clinical study
Purpose
To evaluate the clinical feasibility of the AMS (Absorbable Metal Scaffold)
Conclusion
Concept safe and feasible
Need for prolonged scaffolding time and an anti-proliferative drug
Study design
Prospective, multi-center, non-randomized trial
Timing
2010 (patient enrollment)
Results
TLF 6.8% at 24-months
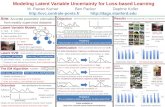
From AMS to DREAMS 2nd generationDevice evolution

The Lancet 381, Issue 9869, 9–15 March 2013, 836–844

BIOSOLVE-1: IVUS and OCT findings after implantation and at 6 and 12 mo follow-up
The Lancet 381, Issue 9869, 9–15 March 2013, 836–844

Tyrosine polycarbonate stent: the REVA stent
RESORB study (27 patients)high TLR rate (66.7%) between 4 and 6 mo
This has led to a new design, the ReZolve stent, which has improved robustness of the polymer and is able to elute sirolimus.



Patient enrollment was initiated in March 2013 and is currently ongoing
REVA announced initial clinical results in TCT in Oct. 28, 2013 first 65 pts 30-day follow-up,
• no reported MACE• no incidences of ischemic TLR, myocardial infarction or stent
thrombosis.

Everolimus-eluting bioresorbable scaffoldBVS 1.0 and 1.1

Bioresorbable Polymer
Polymer backbone
Drug/polymer matrix
Everolimus/PDLLA Matrix Coating
• Thin layer
• Amorphous (non-crystalline)
• 1:1 ratio of Everolimus/PDLLA matrix
• Conformal coating, 2-4 m thick
• Controlled drug release
PLLA Scaffold
• Semi-crystalline
• Provides device structure
• Processed for required radial strength
Everolimus-eluting bioresorbable scaffoldBVS 1.0 and 1.1

OCT and histology at 28 days, at 2, 3, and 4 years after stent implantation in a porcine model
Onuma Y, Serruys P, et al. Circulation 2010;122:2288 –2300
28 days
2 years
3 years
4 years


IVUS echogenicity, palpography and VH of BVS 1.0
Onuma Y, Serruys P. Circulation 2011;123:779-797
Echogenicity
Palpography
Virtual Histology

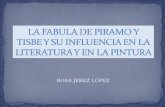
Serial changes in OCT images after implantation of BVS
Onuma Y, Serruys P. Circulation 2011;123:779-797
BVS 1.0
BVS 1.1

Changes from after the procedure to 6 months in the vessel area, scaffold area, lumen area, and NIH area and percent VO in Xience V, BVS 1.0 and BVS 1.1
Onuma Y, Serruys P. Circulation 2011;123:779-797

Late lumen loss of different fully bioabsorbablevascular scaffolds

How About Clinical Outcomes?
Cutlip DE,et al. Circulation. 2007;115: 2344–2351.
At 3 years, clinical follow-up was obtained from 29 of 30 enrolled patients.
There was only 1 non–Q-wave myocardial infarction (peak troponin, 2.21ng/mL) related to the treatment of a non–flow-limiting stenosis (QCAdiameter stenosis, 42%) in a patient implanted with the BVS 46 days earlier.Furthermore, this patient experienced a single episode of angina at restwithout any ECG evidence of ischemia.
Otherwise, there were no new MACEs between 6 months and 3 years andno instances of ST as defined by the protocol or Academic ResearchConsortium definitions.
In total, the MACE rate at 3 years was 3.4%

PW Serruys, et al. J Am Coll Cardiol 2011;58:1578–88

PW Serruys, et al. J Am Coll Cardiol 2011;58:1578–88
OCT, IVUS Gray-Scale, and IVUS-VH at Baseline and 12 Months
Two patients experienced peri-procedural and iatrogenic MI, respectively,whereas 2 underwent repeat intervention, resulting in the MACE rate of 7.1%

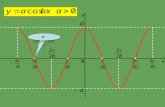
Serial Cineangiograms Before, After Procedure, and at 12-Month Follow-Up
PW Serruys, et al. J Am Coll Cardiol 2011;58:1578–88

Vasomotion Test Results at 12 Months
PW Serruys, et al. J Am Coll Cardiol 2011;58:1578–88

Information contained herein for use with physicians outside the US and Japan only.
Absorb is authorized for sale in CE Mark and certain independently regulated countries outside the United States. Please check the
regulatory status of the device in your geographical location before distribution. Not to be reproduced, distributed or excerpted.
©2013 Abbott. All rights reserved. AP2937781 Rev. D 07/13 32
ABSORB Clinical Trial Program
Note: Sample sizes reflect Absorb patients only.
2011 2012 2013 2014 2015 2016
Total Pts Studied n=~599 n~800 n~5,474 n~13,253 n~13,253 n~13,253
ABSORB IIIn = ~1,500
Enrollment & Follow-Up
ABSORB Japann = ~267
Enrollment & Follow-Up 2 Y1 Y
ABSORB Chinan = ~220
Enrollment & Follow-Up 2 Y1 Y
ABSORB IIn = ~335
2 Y 3 Y1 YEnrollment & Follow-Up
ABSORB FIRST* n = 10,000
Enrollment & Follow-Up
ABSORB Extendn= ~800
2 Y 3 Y1 YEnrollment & Follow-Up
ABSORB Cohort Bn = 101; FIM
1 Y 2 Y 3 Y 4 Y 5 Y
ABSORB Cohort An = 30; FIM
5 Y
2 Y1 Y
2 Y1 Y
* n= 10.000 f/u at 1 year. 1.000 patients f/u at 3 years, 1.000 patients at 2-4 years
3 Y

Takashi Kajiya, et al. EuroIntervention 2013;9:501-504 published online ahead of print May 2013

Takashi Kajiya, et al. EuroIntervention 2013;9:501-504 published online ahead of print May 2013
These are the first real-world data using BVS in patients with STEMI. The ABSORB™ BVS may be safely used in patients with STEMI undergoing primary PCI with favourable short-term outcome.

Tommaso Gori, et al. EuroIntervention 2013; 9online publish-ahead-of-print September 2013

Clinical outcomes at 30 days
BVS implantation for patients with ACS is safe, with outcomes comparable with those of drug-eluting metal stents.
Tommaso Gori, et al. EuroIntervention 2013; 9online publish-ahead-of-print September 2013


Absorb Study cohort B at 6, 12, 24 and 36 months
PW Serruys, et al. EuroIntervention 2013; 9-online publish-ahead-of-print December 2013
Between one and three years, LLL remained unchanged (6 mo: 0.19
mm, 1 yr: 0.27 mm, 2 yrs: 0.27 mm, 3 yrs: 0.29 mm)
The in-segment angiographic restenosis rate for the entire cohort B
(n=101) at 3 years was 6%.
In the entire cohort B (n=101), the three-year MACE rate was 10.0%
without any scaffold thrombosis.

Comparison of Absorb B cohort with SPIRIT
PW Serruys, et al. EuroIntervention 2013; 9-online publish-ahead-of-print December 2013

Conclusions
Bioabsorbable stents appear as one of the most promising fields in
interventional cardiology, with several potential advantages over
permanent metallic stents.
Professor Serruys, one of the pioneers in PCIs, has named them “the fourth
revolution” after balloon angioplasty, bare-metal stents, and drug-eluting
stents
Trials have shown the safety and efficacy of the BRS in simple lesions in
stable patients
Larger studies are required to evaluate the performance of the device in
other clinical and angiographic scenarios.