Clinical Aspects and Laboratory — Iron Metabolism, Anemias || Erythropoiesis
7
F Fundamentals Erythropoiesis Physiological Cell Maturation An adult has on average 5 liters of blood and an erythrocyte count of 5 × 10 6 /μL, giving a total erythrocyte count of 2.5 × 10 13 . Since the mean life span of an erythrocyte is normally 120 days, about 2 × 10 11 new eryth- rocytes need to be formed daily to maintain this erythrocyte pool. For this to happen, 20–30% of the medullary stem cells must be differentiated to cells of erythropoiesis. Different stages in maturation can be identified on the basis of cell morphology and biochemical capacity. e immature nucleated cells, such as proerythroblasts and erythroblasts (macroblasts), with their high DNA, RNA, and protein synthesizing capacity, ensure that there is adequate proliferation of erythrocyte precursors. However, this requires the availability of sufficient cobalamin (vita- min B 12 ) and folic acid, which act as carriers of C 1 units in the synthesis of nucleic acids. Vitamin B 12 (daily requirement about 2 μg) is derived mainly from foods of animal origin. Absorption in the terminal ileum calls for the production of sufficient intrinsic factor by the parietal cells in the fundus/body region of the stomach. By contrast, folic acid (daily requirement >200 μg) is derived mainly from foods of plant origin and, probably for the most part, via synthesis by intestinal bacteria, and ab- sorbed in the jejunum. Both vitamins are mainly stored in the liver. Most of the hemoglobin synthesis occurs during the normoblast stage of the erythrocyte precursors. is is morphologically visible by the conversion of so-called basophilic into oxyphilic normoblasts (with red cytoplasm). In parallel, the transferrin receptor is expressed at a high rate which is necessary to channel a sufficient quantity of transfer- rin-bound iron into the cells. Cell nucleus and mitochondria are then expelled and the cells leave the bone marrow as reticulocytes. At this stage, the cells’ ability to divide and most of their biochemical synthesis capabilities are lost. However, since a considerable amount of Hb-coding mRNA, a high concentration of membrane-bound transferrin receptors, and residual cell organelles persist they are still capable to synhesize Hb for 1–2 days (until mRNA, TfR, and cell organelles are degraded). Within this time about 20% of the mature erythrocyte’ s Hb is synthesized. Subsequently, the cells cir- culate in the peripheral blood as highly specialized, mature erythrocytes M. Wick et al., Clinical Aspects and Laboratory - Iron Metabolism, Anemias © Springer-Verlag/Wien 2011
Transcript of Clinical Aspects and Laboratory — Iron Metabolism, Anemias || Erythropoiesis

FFund
amen
tals
Erythropoiesis
Physiological Cell Maturation
An adult has on average 5 liters of blood and an erythrocyte count of 5 × 106/μL, giving a total erythrocyte count of 2.5 × 1013. Since the mean life span of an erythrocyte is normally 120 days, about 2 × 1011 new eryth-rocytes need to be formed daily to maintain this erythrocyte pool. For this to happen, 20–30% of the medullary stem cells must be diff erentiated to cells of erythropoiesis. Diff erent stages in maturation can be identifi ed on the basis of cell morphology and biochemical capacity. Th e immature nucleated cells, such as proerythroblasts and erythroblasts (macroblasts), with their high DNA, RNA, and protein synthesizing capacity, ensure that there is adequate proliferation of erythrocyte precursors.
However, this requires the availability of suffi cient cobalamin (vita-min B12) and folic acid, which act as carriers of C1 units in the synthesis of nucleic acids. Vitamin B12 (daily requirement about 2 μg) is derived mainly from foods of animal origin. Absorption in the terminal ileum calls for the production of suffi cient intrinsic factor by the parietal cells in the fundus/body region of the stomach. By contrast, folic acid (daily requirement >200 μg) is derived mainly from foods of plant origin and, probably for the most part, via synthesis by intestinal bacteria, and ab-sorbed in the jejunum. Both vitamins are mainly stored in the liver.
Most of the hemoglobin synthesis occurs during the normoblast stage of the erythrocyte precursors. Th is is morphologically visible by the conversion of so-called basophilic into oxyphilic normoblasts (with red cytoplasm). In parallel, the transferrin receptor is expressed at a high rate which is necessary to channel a suffi cient quantity of transfer-rin-bound iron into the cells.
Cell nucleus and mitochondria are then expelled and the cells leave the bone marrow as reticulocytes. At this stage, the cells’ ability to divide and most of their biochemical synthesis capabilities are lost. However, since a considerable amount of Hb-coding mRNA, a high concentration of membrane-bound transferrin receptors, and residual cell organelles persist they are still capable to synhesize Hb for 1–2 days (until mRNA, TfR, and cell organelles are degraded). Within this time about 20% of the mature erythrocyte’ s Hb is synthesized. Subsequently, the cells cir-culate in the peripheral blood as highly specialized, mature erythrocytes
M. Wick et al., Clinical Aspects and Laboratory - Iron Metabolism, Anemias© Springer-Verlag/Wien 2011

Erythropoiesis18
FFund
amen
tals
serving almost exclusively for the transportation of oxygen. Th is whole process of erythropoiesis takes approximately 5 days.
All forms of anemias that are not primarily hemolytic have their roots in disturbances of cell proliferation or hemoglobin synthesis or in defi ciencies at bone-marrow level. Th e simplest indicator of erythropoi-esis is the reticulocyte count.
Hemoglobin Synthesis
In the fetus, hemoglobin (Hb) is made up of 2 α- and 2 γ-polypeptide chains (HbF (αγ)2), whereas in adults it predominantly consists of 2 α- and 2 β-chains (HbA0 (αβ)2), with a small portion of 2 α- and 2 δ- chains (HbA2 (αδ)2).
Each of these chains carries a heme as prosthetic group, which in turn is capable of binding an oxygen molecule. Th e total molecular weight of this tetramer is about 64,500 D.
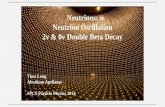
Th e formation of the normal quaternary structure is dependent on the regular synthesis not only of the peptide chains but also of the heme constituent, and in particular on the adequate adhesion of the heme and protein components by means of iron which also guarantees oxygen binding. An overview of hemoglobin synthesis is given in Fig. 11.
Fig. 11: Hemoglobin synthesis

Erythropoiesis 19
FFund
amen
tals
Erythropoietin
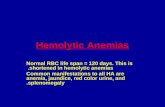
Erythropoietin (EPO) consists of 165 amino acids and has a molecular weight of ~35,000 D (Fig. 12). Approximately 40% of its molecular mass is made up by 4 carbohydrate chains. Th e hematopoietic growth factor acts synergistically with other growth factors to cause maturation and proliferation from the stage of burst-forming unit erythroid (BFU-E) and CFU-E (colony-forming unit erythroid) to the normoblast stage of erythroid cell development. Th us, EPO acts primarily on apoptosis to decrease the rate of cell death in erythroid progenitor cells in the bone marrow.
During the fetal and neonatal period of life, EPO is primarily produced by the liver. Aft er birth EPO production is shift ed to the peri-tubular interstitial cells of the renal cortex. Th e liver keeps its capability to produce EPO also in the adult, but its contribution is not more than 10%.
Fig. 12: Molecular structure of erythropoietin

Erythropoiesis20
FFund
amen
tals
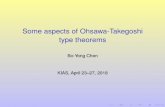
EPO production increases in response to tissue hypoxia, low arte-rial PO2, and increased oxygen affi nity (HbF) of red blood cells. Th e hypoxic induction of EPO production is regulated by a negative feed-back mechanism at the transcriptional level, which involves binding of HIF-1 (Hypoxia-Inducible Factor-1). HIF-1 acts as an oxygen sensor, which ensures that EPO production is increased when oxygen supply to the tissue is low and the demand for new erythrocytes is high, while EPO production is shut down when red blood cell numbers/and or tis-sue oxygen supply returns to normal [129]. Th e characteristics of this control system are depicted in Fig. 13.
Erythropoietin activates target erythroid colony-forming cells by bind-ing and orienting two cell surface erythropoietin receptors. Th e EPO re-ceptors are primarily expressed on erythroid cells between the CFU-E (Colony-Forming Unit E) and the pronormoblast stages of erythroid cell development. Th e cell diff erentiation stages between CFU-E and the pro-erythroblasts have the highest EPO receptor density.
Fig. 13: Stimulation and regulation of erythrocyte formation by erythro poietin

Erythropoiesis 21
FFund
amen
tals
Th e orientation of the EPO receptors is critical for effi cient signal-ing. Proper binding triggers an intracellular phosphorylation cascade, which activates both the Ras/MAP kinase pathway and the STAT (signal transducer and activator of transcription) pathway. Th ese pathways play a major role in cytokine-induced signaling and are involved in increased cell proliferation in response to EPO [52].
Th e erythroid progenitor cells are sensitive to EPO and other growth factors for survival, proliferation, and diff erentiation for only 5 days. Th e young, just matured erythrocytes require EPO for further 9 days, to prevent their cytolysis in the spleen and the reticuloendothelial system (RES).
In adults, the mean endogeneous EPO level is about 8 mU/mL, with a wide range of variation. Th e strongest stimulus of renal EPO production is an anemic condition. EPO levels typically increase when the level of Hb falls below 12 g/dL. By reducing the O2 transport capa-city of Hb, carbon monoxide also leads to a distinct increase of the EPO concentration. Further stimuli of EPO production are an in-creased affi nity of Hb to bind O2 (HbF), an acceleration of the basal metabolic rate by, e.g. thyroid hormones, benignant and malignant kidney tumors, and a decrease in the O2 partial pressure in the arterial blood which occurs e.g. with cardiopulmonary illness or defi ciency of oxygen in the respiratory air. Th e stimulation of EPO production by hypoxia is used, e.g. by athletes to increase their erythrocyte count by high altitude training.
An increase of the erythrocyte mass, renal diseases, fasting and re-section of the hypophysis lead to a decrease of the EPO production.
Up to now the determination of erythropoietin has been of limited diagnostic value. It can be used, for example, to diff erentiate between primary causes of erythrocytosis, polycythemia vera and secondary causes such as increased production of erythropoietin, e.g., in lung dis-eases with hypoxia or certain tumors. In renal anemia, the decreased erythropoietin production can usually be the cause. In every case where a true erythropoietin defi ciency does not exist but rather an adequate erythropoietin response, i.e., anemia with normal erythropoietin lev-els, the determination of erythropoietin is suitable for detecting this inadequate erythropoietin response.
Increased EPO concentrations in serum are measured in patients with cardiac and pulmonary insuffi ciency, for example, and in patients

Erythropoiesis22
FFund
amen
tals
with erythrocytosis with high oxygen affi nity (e.g., HbF). EPO levels typically increase in serum when the Hb level falls below 12 g/dL.
A decrease in EPO concentrations is observed in patients with impaired renal function. Patients with chronic renal insuffi ciency develop anemia and erythropoiesis is inadequate. Additional extracor-poral factors (e.g., hemolysis) can also play a role in the development of anemia.
Erythrocyte Degradation
Phagocytosis of Old Erythrocytes
During the physiologic aging process, the circulating erythrocytes lose more and more of the terminal neuraminic acid residues of their mem-brane glycoproteins, which leads to increased binding of IgG. Th e changed membrane surface structure is the signal in particular to the spleen and liver macrophages to start phagocytosis of the aged erythro-cytes. About 0.8% of the erythrocyte pool or 2 × 1011 erythrocytes are phagocytozed each day, maintaining equilibrium with the daily new for-mation rate.
Hemoglobin Degradation
Th e globin component of the hemoglobin is hydrolyzed by proteases to amino acids which are either available for the synthesis of new proteins or are further degraded. To avoid toxic eff ects, the released Fe2+ is oxi-dized to Fe3+ and incorporated into basic isoferritins for interim storage. In this process, the macrophages of the RES (reticuloendothelial sys-tem) in the spleen in particular serve as short-term stores from which ferritin-bound iron can be remobilized and transported via transferrin to the bone marrow for the synthesis of new hemoglobin. At a physio-logic hemolysis rate, about 6.5 g per day of hemoglobin is degraded, and the corresponding quantity newly synthesized, giving an iron turnover of about 25 mg/24 h [123, 126]. Given a daily iron absorption of 1 mg, this again shows clearly that the iron requirement can be met only by extensive reutilization.

Erythropoiesis 23
FFund
amen
tals
Th e porphyrin ring of the heme is degraded via biliverdin to bilirubin. Since the unjconjugated bilirubin has poor aqueous solubility it has to be converted into a better water-soluble form to be suited for excretion. For this purpose bilirubin is transported bound to albumin to the liver where it is conjugated with glucuronic acid. Th e conjugated bilirubin is then excreted with the bile (Fig. 14).
Fig. 14: Hemoglobin degradation
Cp: Ceruloplasmin.