Beta-Carotene: The Controversy Continuesaltmedrev.com/publications/5/6/530.pdf · The three...
16
Page 530 Alternative Medicine Review ◆ Volume 5 Number 6 ◆ 2000 Copyright©2000 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission Beta-Carotene: The Controversy Continues Lyn Patrick, ND Introduction More than 600 carotenoids have been isolated in nature, β-carotene being the best known. 1 Approximately 50 carotenoids have been found in the human diet and 20 have been identified in plasma and tissues. 2 β-carotene has been shown to act as an immune modulator, quench singlet oxygen, and reduce peroxyl radicals at a low partial oxygen pressure. 3 β-carotene also enhances gap-junc- tion communication 4 and, in the rat model, induces hepatic enzymes that detoxify carcinogens. 5 In both observational and case control studies, the intake of carotenoid-rich fruits and veg- etables has been found to be inversely correlated with risk for cardiovascular disease. 6 Numer- ous retrospective epidemiological studies have established an inverse relationship between di- etary carotenoid levels and the incidence of specific cancers. 7,8 Numerous animal and labora- tory studies have substantiated β-carotene’s ability to inhibit tumor cell growth and the progres- sion of carcinogenesis. 9 Abstract The three β-carotene intervention trials: the Beta-Carotene and Retinol Efficacy Trial (CARET), Alpha-Tocopherol, Beta-Carotene Cancer Prevention Study (ATBC), and Physician’s Health Study (PHS) have all pointed to a lack of effect of synthetic β-carotene in decreasing cardiovascular disease or cancer risk in well-nourished populations. The potential contribution of β-carotene supplementation to increased risk of lung cancer in smokers has been raised as a significant concern. The safety of synthetic β-carotene supplements and the role of isomeric forms of β-carotene (synthetic all-trans versus “natural” cis-trans isomeric mixtures), in addition to the importance of the protective role of other carotenoids like lycopene and lutein, have become topics of debate in the scientific and medical communities. This review addresses the biochemistry and physiology of the cis versus trans isomers of β-carotene as well as relevant studies comparing the absorption and storage of the synthetic versus natural forms of β-carotene. In addition, the risk of potential pro-oxidant effects of synthetic β-carotene supplementation in intervention trials is evaluated. (Altern Med Rev 2000;5(6):530-545) Lyn Patrick, ND – Associate Editor, Alternative Medicine Review; Private Practice, Tucson, AZ Correspondence address: 540 W Prince, Ste A, Tucson, AZ 85705
Transcript of Beta-Carotene: The Controversy Continuesaltmedrev.com/publications/5/6/530.pdf · The three...

Page 530 Alternative Medicine Review ◆ Volume 5 Number 6 ◆ 2000
Copyright©2000 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
Beta-Carotene:The Controversy Continues
Lyn Patrick, ND
IntroductionMore than 600 carotenoids have been isolated in nature, β-carotene being the best known.1
Approximately 50 carotenoids have been found in the human diet and 20 have been identified inplasma and tissues.2
β-carotene has been shown to act as an immune modulator, quench singlet oxygen, andreduce peroxyl radicals at a low partial oxygen pressure.3 β-carotene also enhances gap-junc-tion communication4 and, in the rat model, induces hepatic enzymes that detoxify carcinogens.5
In both observational and case control studies, the intake of carotenoid-rich fruits and veg-etables has been found to be inversely correlated with risk for cardiovascular disease.6 Numer-ous retrospective epidemiological studies have established an inverse relationship between di-etary carotenoid levels and the incidence of specific cancers.7,8 Numerous animal and labora-tory studies have substantiated β-carotene’s ability to inhibit tumor cell growth and the progres-sion of carcinogenesis.9
AbstractThe three β-carotene intervention trials: the Beta-Carotene and Retinol Efficacy Trial(CARET), Alpha-Tocopherol, Beta-Carotene Cancer Prevention Study (ATBC), andPhysician’s Health Study (PHS) have all pointed to a lack of effect of synthetic β-carotenein decreasing cardiovascular disease or cancer risk in well-nourished populations. Thepotential contribution of β-carotene supplementation to increased risk of lung cancer insmokers has been raised as a significant concern. The safety of synthetic β-carotenesupplements and the role of isomeric forms of β-carotene (synthetic all-trans versus“natural” cis-trans isomeric mixtures), in addition to the importance of the protectiverole of other carotenoids like lycopene and lutein, have become topics of debate in thescientific and medical communities. This review addresses the biochemistry andphysiology of the cis versus trans isomers of β-carotene as well as relevant studiescomparing the absorption and storage of the synthetic versus natural forms of β-carotene.In addition, the risk of potential pro-oxidant effects of synthetic β-carotenesupplementation in intervention trials is evaluated.(Altern Med Rev 2000;5(6):530-545)
Lyn Patrick, ND – Associate Editor, Alternative Medicine Review; Private Practice, Tucson, AZCorrespondence address: 540 W Prince, Ste A, Tucson, AZ 85705

Copyright©2000 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
Beta C
arotene
Alternative Medicine Review ◆ Volume 5, Number 6 ◆ 2000 Page 531
Digestion and Absorption of Beta-Carotenes
Carotenoids are found in foods in acomplex with proteins or in crystalline caro-tenoid complexes.10 Heating appears to im-prove the bioavailability of carotenoids bybreaking down these complexes, as has beenshown for lycopene in cooked versus raw to-matoes.11 Typical dietary β-carotene intakes ofAmerican adults are 0.5-6.5 mg/day (833 IU-10,829 IU).12
Absorption of β-carotene and othercarotenoids from vegetables is usually 5-30percent of the absorption from syntheticsupplements, due to the food matrix surround-ing β-carotene. This matrix of fiber or proteinmust first be broken down by mastication, gas-tric acid, pancreatic enzymes, and bile acids.13
The Effect of Gastric pHGastric pH level has also been found
to alter β-carotene absorption. In the BostonNutritional Status Survey, conducted between1981 and 1984, the median serum carotenoidvalues were lowest for those subjects with se-vere atrophic gastritis, a condition in whichlittle or no hydrochloric acid is secreted by thestomach.14 Since 30 percent of the U.S. popu-lation over age 60 is estimated to have atro-phic gastritis,15 the potential malabsorption ofβ-carotene in this population subset appearsto be significant.
In another study of β-carotene absorp-tion and gastric pH, the effect of omeprazole-induced hypochlorhydria on β-carotene ab-sorption was investigated.16 The authors foundthat serum β-carotene concentrations were sig-nificantly lower at a higher gastric pH of6.4+0.3 (with omeprazole) than at a gastric pHof 1.3+0.1 (without omeprazole). Lipid mi-celles containing carotenoids, formed in theduodenum as a result of fat digestion, releasecarotenoids into mucosal cells of the duode-num by passive diffusion, determined by theconcentration gradients between the two.10 The
authors of the omeprazole study theorized thata higher gastric pH increased the negative sur-face charges of the carotenoid-containing mi-celle and the intestinal lumen, inhibiting pas-sive diffusion.16 Saturation of these uptakemechanisms are estimated to occur only at in-takes below 100 mg (166,000 IU),10 althoughabsorption studies discussed later in this ar-ticle appear to reveal significant problems withβ-carotene absorption at dosage levels muchlower than 100 mg.
The digestion of carotene complexesin the duodenum occurs as a result of the ac-tion of pancreatic lipase and bile salts,10 andabsorption depends on the efficiency of lipiddigestion; non-digested lipids interfere withcarotenoid absorption.17 Similarly, bile acidsequestrant drugs, like cholestyramine, reducecarotenoid absorption as do other situationsthat interfere with micelle formation: malab-sorption, intestinal parasites, and steatorrheaor fat malabsorption syndromes from pancre-atic or gall bladder disorders.18 Certain formsof dietary fiber also appear to inhibit caro-tenoid absorption: when 12 grams of citruspectin was added to a meal with 25 mg β-caro-tene, plasma β-carotene levels were signifi-cantly reduced.19
The Effect of Dietary FatDietary fat is a factor in carotenoid
absorption. High-fat diets (18-24 g fat withbreakfast, 45 g fat with midday meal) producedbetter β-carotene absorption than low fat diets(no fat for breakfast and 6 g for midday meal)in test meals when subjects were given 45 mgβ-carotene for five days.20 Although the dif-ference in absorption between the two groupswas significant, the low-fat diet group still hada measurable and sustained rise in β-carotenelevels, apparent after 13-15 days of treatment.Levels in the low-fat diet group, however,dropped back to baseline more quickly aftertreatment was discontinued (7-23 days vs 21-41 days post-discontinuation). Adding 18 golive oil to a low-fat diet (7% of total calories)

Page 532 Alternative Medicine Review ◆ Volume 5, Number 6 ◆ 2000
Copyright©2000 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
improved carotene absorption from 5 to 25percent in young African males.21 Absorptionstudies with low-fat diets have shown a mini-mum of 3-5 g per meal is necessary for anycarotenoid absorption to occur.22
IntestinalAbsorption ofBeta-carotene
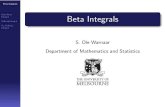
In the smalli n t e s t i n a lenterocyte, β-caro-tene can be trans-formed into vitaminA mainly as retinylester (20-75%)through cleavage ofthe β-carotene mol-ecule. The majorityof conversion to vi-tamin A takes place,not in the liver, butin the intestinal mu-cosa (Figure 1).23
This cleavage de-pends on the vita-min A content of themeal and the vita-min A status of theindividual.24 In vita-min A-depleted sub-jects, synthetic β-carotene had 50 per-cent of the potencyof retinol; in otherwords, 2 mg β-caro-tene was equivalentto 1 mg vitamin A.25
However, β-caro-tene has not beenshown to precipitatevitamin A toxicity,and it has been dem-
onstrated in several species that, when dietaryβ-carotene increases, the regulatory mecha-nisms limit vitamin A production from caro-tenoids.18 β-carotene not converted to vitaminA is absorbed by the lymphatics, having beenincorporated into chylomicrons as intact β-carotene or other non-vitamin A products ofβ-carotene cleavage.26 The entire family of
Chylomicron9 cBC
trans BCtrans RE
9 cRAtRA
Lymph
trans retinyl ester
trans retinol
trans retinoic acid
trans-retinal
9 c retinoic acid
9 c retinal
9 cBC trans BC
9 cBC trans BC
Duodenum9 cBC = 9-cis-β-carotenetrans BC = trans-β-carotene9 cRA = 9-cis-retinoic acidtRA = trans retinoic acid
mucosa
Figure 1: Proposed Absorption Mechanism for Beta-caroteneand Conversion to Vitamin A in Intestinal Mucosa.

Beta C
arotene
Alternative Medicine Review ◆ Volume 5, Number 6 ◆ 2000 Page 533
Copyright©2000 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
carotenoids is found in the bloodstream, in-corporated into either chylomicrons or lipo-proteins: very low density lipoproteins(VLDL), low density lipoproteins (LDL), orhigh density lipoproteins (HDL) – the major-ity being transported in LDLs.27 Actual absorp-tion levels of β-carotene have dramatic indi-vidual and inter-individual variation with re-ports in the literature varying from 10-90 per-cent.28 Three- to four-fold variations in plasmaβ-carotene levels among individuals have beenseen after a single dose of 30 mg (50,000 IU).29
These results have been confirmed in studiesthat control for fat malabsorption, smoking,alcoholism, gastrointestinal disorders, and fatcontent of the test meals.26 Absorption appearsto be linear up to doses of 20-30 mg (33,000-50,000 IU) and then begins to become lim-ited.10
Absorption studies exploring indi-vidual isomers are difficult given that some β-carotene is converted to vitamin A in the in-testinal lumen and some is unabsorbed and lostin the feces as intestinal enterocytes aresloughed off.10 β-carotene isomers also appearto have a biphasic appearance in the plasma,possibly as a result of re-secretion of VLDLfrom the liver or storage in the intestinal epi-thelium; levels have remained high for threedays after an oral dose of 120 mg (200,000IU) or have risen 12 hours after a single dose(of 120 mg) and then again three or four dayslater.26 The body also appears to have a mecha-nism for maintaining significant β-carotenereserves. When healthy males were fed low β-carotene diets they maintained normal bloodβ-carotene levels for 17 weeks.30
Mechanisms of absorption in specifictissues are not well understood. High levels ofcarotenoids are found in the liver, adrenals,kidneys, ovaries, adipose tissue, and themacula of the eye.31 Significant correlationshave been found between serum and breast tis-sue levels of retinoids, tocopherol, and eightcarotenoids including β-carotene.32 Significantamounts of carotenoids have also been found
in the pineal gland and the corpus luteum ofcattle.10 The accumulation in the adrenals, liver,testes, and ovaries may follow uptake of lipo-proteins (LDL/HDL) but accumulation in othertissues, like the macula of the eye, appears tofollow selective tissue uptake pathways whichare still unknown.33
Competitive Inhibition AmongCarotenoids for Absorption
One difference between synthetic β-carotene and natural-source β-carotene in-volves the inclusion of other naturally-occur-ring carotenoids: lutein, canthaxanthin, lyco-pene, α-carotene, zeaxanthin, and cryptoxan-thin in Dunaliella species, the algal form ofcommercially available mixed carotenes.34
These carotenoids have immune modulatingactivities of their own and the possibility thatfeeding high doses of purified β-carotene mayinhibit absorption of other carotenoids hasbeen investigated.
The studies examining competitive in-hibition among carotenoids, however, haveshown conflicting results. In a long-term study,the ATBC trial, commonly known as the Finn-ish Smokers Study, a 6.7-year supplementa-tion with 20 mg (33,000 IU) synthetic all-transβ-carotene resulted in a significant decrease(≅ 11%) in serum lutein levels.35 Other stud-ies have not shown evidence of competitiveinhibition. The Physicians’ Health Study, a 12-year treatment with 50 mg (83,000 IU) all-transβ-carotene dosed every other day did not showchanges in any other serum or plasma caro-tenoid levels.36 Two polyp-prevention trials,one with 25 mg (42,000 IU) synthetic β-caro-tene for four years37 and the other supplement-ing 20 mg (33,000 IU) synthetic β-carotenefor two years38 found different results: the four-year study showed no effect of β-carotenesupplementation on other carotenoid levelswhile the two-year study found increases inserum lycopene and α-carotene levels as a re-sult of β-carotene supplementation. Another

Page 534 Alternative Medicine Review ◆ Volume 5, Number 6 ◆ 2000
Copyright©2000 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
long-term β-carotene study, employing dosesof 50 mg (83,000 IU) for five years, found nosignificant effect on plasma carotenoid levels,with the expected exception of the α- and β-carotene found in the supplement.39
The only negative carotenoid interac-tions have been found in short-term studieswhere varying levels of lutein and β-carotenehave been fed simultaneously. When lutein wasthe predominant carotenoid, β-carotene ab-sorption from a 22.5 mg (37,000 IU) β-caro-tene meal was inhibited.40 β-carotene also ap-pears to inhibit lutein absorption, although atinsignificant levels, in intervention35 and insingle-feeding41 trials. Although these nega-tive interactions have not been borne out inthe majority of long-term supplementationstudies with β-carotene, they are important toinvestigate due to the role lutein plays in macu-lar function and the provitamin activity of β-carotene in retinoid metabolism.40
Isomers of Beta-carotene: 9-cisVersus All-trans and Differences inAbsorption
Isomers of β-carotene are found invarying forms in nature; each double-bond inthe carbon chain of a carotenoid can exist ineither the trans or the cis configuration, thecis configuration being less stable than thetrans (Figure 2). Cis isomers are more polar,less crystallized, and more soluble in oil thanthe trans isomers.42,43 The all-trans, 9-cis, 13-cis, and 15-cis isomers have been identified inboth food sources and human plasma in vary-ing amounts depending on the source. Rawcarrots, tomatoes, and sweet potatoes appearto be devoid of the cis isomer;44 98 percent ofthe β-carotene in raw carrots is in the trans-form.45 The 9-cis-carotenoid isomers in foodsappear to increase with processing and heat-ing but multiple studies indicate the 9-cis-caro-tenoids are not absorbed as easily or are ab-sorbed through different mechanisms than theall-trans isomers.13
The majority of carotenoids in natureoccur in the all-trans form, which is
All-trans-β-carotene
9-cis-β-carotene
Figure 2: Cis and Trans Isomers of Beta-Carotene.

Beta C
arotene
Alternative Medicine Review ◆ Volume 5, Number 6 ◆ 2000 Page 535
Copyright©2000 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
molecularly identical to synthetically producedall-trans-β-carotene.1 All-trans β-carotene canisomerize under exposure to heat and withoxidation1 and multiple studies addressed inthis article document the isomerization of thecis-β-carotenes (in algal β-carotene) to thetrans form in the human intestine.
The cis-isomers have been reported toaccount for less than five percent of humanplasma β-carotene but a larger proportion (10-25%) of the total carotenoid content of humantissue; 9-cis-β-carotene makes up 25 percentof the total β-carotene content of the liver and10 percent in the adrenals. Cis-isomers werealso found in significant amounts in the kid-neys, testes, ovaries, and fat tissue.31 The trans-isomer is the most common form in humantissue, comprising up to 60 percent of the to-tal β-carotene content.31 However, significantlyhigher levels of the 9-cis isomer were foundin the breast adipose of women with a historyof benign breast lesions when compared towomen with a history of breast cancer.32
The debate over the differences be-tween synthetic and food-source (or naturally-derived commercial – from the algaeDunaliella species) β-carotene centers aroundthe role of the cis-isomers, which are absentfrom synthetic all-trans β-carotene. The im-portance of the 9-cis isomer has been linkedto the fact that it is a direct precursor in theintestinal enterocyte to 9-cis retinoic acid.46
Retinoic acid acts as a hormone in signalingprocesses where it binds to nuclear receptorsand controls normal reproduction and main-tenance of epithelial tissue.47 Retinoids are alsoinvolved in preventing carcinogenesis, inhib-iting squamous metaplasia, acting as achemopreventive agent in epithelial carcino-genesis, and as a differentiating agent in acutepromyelocytic leukemia.47 Specifically, 9-cisretinoic acid binds to human nuclear retinoicacid receptor (RAR) and retinoid X receptor(RXR-α) and plays a significant role in theexpression of normal epithelial and squamoustissue growth. The 9-cis retinoic acid isomer
has been studied as an antitumor agent in com-bination studies with either tamoxifen48 orraloxifene49 in experimental mammary car-cinogenesis; both studies found significantinhibition of mammary tumor growth whencompared to the anti-estrogens alone. Signifi-cant inhibitory effects on head and neck squa-mous cell carcinoma cell lines have also beenfound with 9-cis retinoic acid.50
9-cis retinoic acid is formed only from9-cis β-carotene, while all-trans β-carotene hasbeen shown to be transformed into only all-trans retinoic acid.51 The 9-cis isomer of β-carotene appears to be isomerized in the in-testinal mucosa to the all-trans isomer52 andtheoretically, all-trans retinoic acid can bemetabolized into 9-cis retinoic acid. Althoughthis has been demonstrated both in vivo and invitro, this pathway is not well understood andhas not been demonstrated in the human gut.46
In vitro, algal extracts of Dunaliellacontaining relatively equal mixtures of cis andtrans isomers had a greater ability to preventmethyl-linoleate peroxidation than the syn-thetic all-trans β-carotene.53 The ability of thetrans and cis isomers of β-carotene to preventlipid peroxidation has also been studied in ananimal model.54 Rats were fed 1g/kg β-caro-tene either in a Dunaliella extract of 75-per-cent 9-cis β-carotene or a synthetic all-transisomer, and both groups were fed oxidized soyoil. Both carotenoid isomers prevented lipidperoxidation to the same extent; however, thetrans isomer resulted in a significant depletionof hepatic carotene stores while the 9-cis iso-mer conserved liver carotene stores compa-rable to the levels in rats fed fresh soy oil.
As a result of the conflicting data be-tween the cancer-protective effect of dietarycarotenoid consumption and the subsequentnegative results of supplementation trials us-ing all-trans isomers of β-carotene, interest inthe absorption and biochemistry of the β-caro-tene isomers has increased. Research has cen-tered on the absorption and utilization of thethree main isomers found in natural sources:

Page 536 Alternative Medicine Review ◆ Volume 5, Number 6 ◆ 2000
Copyright©2000 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
all trans, 9-cis, and 13-cis β-carotene.Data from absorption studies show
clear differences in absorption among the iso-meric forms. Multiple studies have comparedhuman absorption of synthetic all-trans β-caro-tene with a natural isomeric mix of all-transand 9-cis β-carotene from algal sources(Dunaliella species). The ratios of all-trans to9-cis carotenoids in the different species ofDunaliella vary from 40:60 to 54:37.13 Con-sistently in the studies evaluated in Table 1,the levels of serum and plasma all-trans and9-cis β-carotenoids were greater after feedingeither synthetic all-trans β-carotene or, in thestudy by Jensen,45 raw carrots containing atleast 98-percent all-trans β-carotene comparedto an algal extract.
Jensen gave either 207 g raw carrot (24mg β-carotene) containing 98-percent all-transβ-carotene or an algal-source β-carotene (24mg from Dunaliella) to 16 healthy adults andserum levels of all-trans and cis β-carotenewere compared after seven days. Theabsorption of β-carotene from the raw carrotwas greater than from the algae and the rise inserum cis β-carotene was significantly greaterin those fed carrots than those who receivedalgal carotene capsules. Despite the 50:50trans-to-cis ratio of the algal carotenes, theabsorption rate of cis-carotenes in the serumwas only 9.6 percent of the rise in total serumβ-carotene level, only slightly more than therise in the serum level of cis β-carotene (7.1%)with raw carrot. There was a constant serumtrans:cis ratio of 11:1 after Dunaliella-derivedβ-carotene ingestion indicating what other
Gaziano, et al. 56
Jensen, et al. 45
Johnson, et al. 57
You, et al. 52
Tamai, et al. 58
24 adult M + F for 6 days 100 mg synthetic vs. 66 or 100 mg algal source (trans/cis ratio=50:50)
16 adult M and F for 7 days 24 mg β-carotene algal source:(trans/cis ratio=40:60)24 mg β-carotene raw carrot:(98% all-trans)
15 M single dose of 120 mgβ-carotene containing either all-trans βC or 80% 9-cis βC/20% all-trans
3 adult M and F single dose 1 mg β-carotene (99.4% cis)-radioactively labeled (13C)
30 adult M 60 mg of either: algal β-carotene(trans/9-cis ratio=50:50) vs. all trans or placebo – 44 weeks
160% increase in plasma β-carotene with synthetic, all trans form.87% increase in plasma β-carotene with natural algal form
algal source: serum cis-carotenoid increase 9.6% of total serum β-carotene carrot source: serum cis- carotenoid: 7.1% total serum β-carotene
all-trans βC well absorbed in 7 of 15no increase in all-trans βC with mixture
>95% of 13 Cβ-carotene in plasma found as trans isomer (14-52%) and retinol
Levels of both cis (77%) and trans (116%) isomers significantly higher with all-trans β-carotene
Study Data β-carotene absorption
Table 1: Studies of Beta-Carotene Absorption.

Beta C
arotene
Alternative Medicine Review ◆ Volume 5, Number 6 ◆ 2000 Page 537
Copyright©2000 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
researchers have found, a higher ratio of transto cis isomers in the serum, plasma, andchylomicrons after feeding algal-source β-carotene.55 In chylomicrons, the ratio of trans
to cis isomers has been shown to bebetween 10:1 and 50:1 afterconsumption of 5.6 mmol/kg naturalβ-carotene consisting of 54-percentall-trans β-carotene and 37-percent 9-cis β-carotene.46
A study by Gaziano et al56 ex-amining the difference in absorptionbetween all-trans β-carotene and al-gal β-carotene from Dunaliella salina(50:50 trans:cis ratio) found syntheticβ-carotene produced a higher plasmalevel of all-trans β-carotene and a five-fold increase in 9-cis β-carotene, whilethe natural algal form produced onlya 3.7-fold increase in 9-cis isomer. Asa result of the significant increase inlevels of the plasma trans-isomers inthe synthetic β-carotene group, how-ever, the trans to cis isomer ratio wasmuch higher than was normally seen:15.1 compared to a baseline of 10.3.The natural source or algal β-carotenedid not alter the plasma isomer ratios.After 23 additional days on an alter-nate daily dosing of 50 mg syntheticβ-carotene or a daily dosing of either66 mg or 100 mg algal-derived β-caro-tene, there were no real changes in theisomeric ratios or the total plasma β-carotene ratios of those given the al-gal source. Total β-carotene plasmalevels in subjects given synthetic β-carotene were higher during the entire30 days of the trial. It is also interest-ing to note there were no differencesin the plasma levels of β-caroteneachieved with either 66 mg (110,000IU) or 100 mg (166,600 IU) of thenatural β-carotene.
Johnson57 studied the absorp-tion of a “natural” algal carotene mix-
ture containing 80-percent 9-cis β-caroteneand equal amounts of all-trans β-carotene, α-carotene, and 13-cis β-carotene versus a mix-ture containing 93-percent all-trans β-carotene
1500
1200
900
600
300
0
150
120
90
60
30
0
0 11 22 33 44
0 11 22 33 44
All-trans β-carotene
9-cis β-carotene
Week
Week
All-
tran
s β-
caro
tene
µg/
mL
9-ci
s β-
caro
tene
µg/
mL
Synthesized (60 mg/day)
Dunaliella (60 mg/day)
Placebo
Synthesized (60 mg/day)
Dunaliella (60 mg/day)
Placebo
From: Tamai H, Morinobu T, Murata T, et al. Lipids 1995; 30: 493-498. copyright ©, 1995 Lipids. All rights reserved.
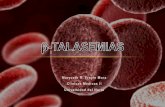
Figure 3: Changes in Plasma Levels of Beta-carotene Isomers with Synthetic vs Naturally-derived Beta-carotene.

Page 538 Alternative Medicine Review ◆ Volume 5, Number 6 ◆ 2000
Copyright©2000 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
and 7-percent α-carotene, 9-cis and 13-ciscarotenes. The two mixtures were given to 15male volunteers in single doses one week apart.Serum levels in the group given the 9-cis β-carotene mixture did not show appreciablechanges in the all-trans isomer and the levelsof 9-cis β-carotene were significantly raisedat only one point during the 24 hours of mea-surements. The serum levels following the 93-percent all-trans mixture were significantlyhigher for the all-trans isomer and showed noincrease in the 9-cis isomer.
Tamai58 gave 38 male volunteers either60 mg synthetic all-trans β-carotene or 60 mgalgal β-carotene (trans-to-cis ratio 50:50) for44 weeks. His group found the levels of all-trans β-carotene in the plasma of those whohad taken the synthetic form were twice as highas for those who had taken the natural form.Surprisingly, he also found the synthetic β-carotene group had a significantly higher levelof plasma 9-cis β-carotene, even though therewere no 9-cis β-carotene isomers in the syn-thetic form (100% all-trans β-carotene) (Fig-ure 3). The authors concluded that isomeriza-tion from the all-trans to the 9-cis form prob-ably takes place in the body during or afterabsorption and that the 9-cis form accumulatesin tissue as a result.
A study was published one year afterTamai’s work that appears to solve the all-transand 9-cis isomerization question. A group atCornell University52 gave three healthy adultsa 1 mg (1666 IU) single dose of 99-percentcis β-carotene labeled with a radioactive tracer(13C) and found over 95 percent of the cis iso-mers had been isomerized to trans β-caroteneor transformed into retinol prior to enteringthe bloodstream. Using calculations the au-thors admit “may be underestimates” theyspeculated that 14-52 percent of the cis β-caro-tene had been isomerized to the all-trans form.
They also compared the absorption ofthe labeled cis β-carotene by giving a singledose of unlabeled cis β-carotene eight monthslater.52 As a result of the comparison data, they
produced three provocative points. First, thiswas the first definitive proof that cis β-caro-tene is isomerized in the intestinal lining tothe trans isomer before absorption. Second, theauthors suggest that greater amounts of all-trans β-carotene are absorbed and secreted intochylomicrons after cis β-carotene dosing thanoccurred after an equivalent dose of all-transβ-carotene, alluding to the fact that (unlikeother researchers’ findings) the cis isomer mayactually be better absorbed. Third, most of theradioactively-labeled retinol produced by thestudy subjects was made from the labeledtrans-isomer rather than being produced di-rectly from the labeled cis-isomeric form ofβ-carotene, pointing out a more efficientmechanism for retinol production by trans-forms of β-carotene. They concluded theisomerization process could serve as a controlmechanism for the production of 9-cis retinol.Because this study used a very small dose ofβ-carotene (1666 IU), absorption mechanismsmay not be reproducible with higher doses.
The results of this study point out thegaps in our knowledge about cis β-caroteneand its relationship to β-carotenoid absorptionand metabolism. They also provide an expla-nation for the previous dosing studies in which9-cis β-carotene blood levels were alwayslower than dosing levels, a result of the isomer-ization of the cis isomer to the trans isomer inthe intestine.
Although 9-cis β-carotene (along withthe 13-cis and 15-cis isomers found in foodand naturally-occurring substances) may servean important function in human physiologythat cannot be replaced by synthetic β-caro-tene, the consequences of using all-trans syn-thetic β-carotenes are at this point unknown.There is evidence that 13-cis β-carotene canbe produced from all-trans β-carotene in sig-nificant quantities: as much as 10 percent oftotal β-carotene intake.59 Certainly, using theβ-carotene carotenoid exclusively may beproblematic as there appears to be a possiblecompetitive inhibition between β-carotene and

Beta C
arotene
Alternative Medicine Review ◆ Volume 5, Number 6 ◆ 2000 Page 539
Copyright©2000 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
lutein. However, as discussed previously, long-term β-carotene studies have not found suchcompetition. Whether or not the lower luteinlevels seen in the Finnish Smokers Study arerelevant is unknown.1
Beta-Carotene TrialsIntervention studies with β-carotene
have not shown the efficacy predicted by ob-servational and animal studies. The well-pub-licized intervention trials with β-carotene, theAlpha-Tocopherol Beta-Carotene Cancer Pre-vention Study (ATBC)60 and the Beta-Caro-tene Retinol Efficacy Trial (CARET),61 weredesigned to assess the effects of tocopherol,β-carotene, and retinol in populations at highrisk for lung cancer – former and presentsmokers and asbestos-exposed workers.
The ATBC trial (Finnish SmokersStudy) looked at the effect of supplementa-tion of alpha-tocopherol (50 mg) and β-caro-tene (20 mg), alone or in combination, in29,133 smokers for 5-8 years. At the con-clusion of the study, those receiving β-caro-tene, alone or in combination with toco-pherol, had a 16-percent increased inci-dence of lung cancer compared to thosereceiving tocopherol alone or placebo. Theelevation of risk was restricted only to thosewho were smoking at least one pack ofcigarettes daily; those smoking less thanone pack daily had no increase in lung can-cer risk and β-carotene had no effect onother types of cancers (prostate, bladder,stomach, colorectal).
The CARET study evaluated the ef-fect of 30 mg β-carotene and 25,000 IUretinyl palmitate versus placebo in 18,314men and women.61 Twenty-two percent ofthe study population were occupationallyasbestos-exposed, 39 percent were formersmokers, and 60 percent were currentsmokers. The trial was ended two yearsearly, after approximately four years, whenthe incidence of lung cancer in the inter-vention group was found to be 28-percent
higher and the incidence of mortality 17-per-cent higher than the placebo group. Those whowere smoking during the study had an evenhigher risk of lung cancer: a relative risk of1.42 (42-percent increase in incidence). In theparticipants who had stopped smoking at leasttwo years prior to entry, the combination of β-carotene and retinol had a protective effect thatdid not reach statistical significance – a rela-tive risk of 0.80 for diagnosis of lung cancerduring the study period.
A third study, the Physicians’ HealthStudy (PHS), assessed the effect of 50 mg β-carotene every other day and 325 mg aspirinalone or in combination for 12 years against aplacebo group in a population of 22,071 phy-sicians.62 The endpoints in this study were can-cer and cardiovascular disease incidence andmortality. Although the population of currentsmokers in this study was smaller (11%), thepopulation of former smokers (39%) was sub-stantial. There was no increased incidence of
Table 2: Treatment Groups in LinxianStudy.63
Treatment Group
1
2
3
4
Treatment group combinations:
Treatment (daily dosage)
retinol 5,000 IUzinc 22.5 mg
riboflavin 3.2 mg niacin 40 mg
ascorbic acid 120 mgmolybdenum 30 mcg
β-carotene 15 mgselenium 50 mcgα tocopherol 30 mg
1+2, 1+3, 1+4, 2+3, 2+4, 3+4, 1+2+3+4, placebo

Page 540 Alternative Medicine Review ◆ Volume 5, Number 6 ◆ 2000
Copyright©2000 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
mortality or cancer diagnosis in the β-caro-tene population, and only those in the lowestquartile for baseline plasma β-carotene expe-rienced a protective effect of β-carotene forprostate cancer.
A fourth study, from Linxian, China ,compared the cancer-protective effects of foursupplemental vitamin and mineral combina-tions.63 The study included 29,584 adults di-vided into eight groups: either placebo or com-binations of retinol, zinc, riboflavin, niacin,ascorbic acid, molybdenum, β-carotene, sele-nium, and α-tocopherol, in a complex 2 x 2 x2 x 2 factorial design that included all pos-sible combinations of the four groups in pairedsequences (Table 2).
The study was conducted for fiveyears. At the conclusion the group taking 50mcg selenium, 30 mg α-tocopherol, and 15mg β-carotene, when compared to the otherintervention groups and placebo, had areduction in cancer risk of 13 percent,primarily due to a decrease in the incidence ofgastric cancer.
Comparisons of these trials are usefuleven though they involved different treatmentprotocols, patient populations, and endpoints(Table 3).
The Linxian study used the smallestdosage of β-carotene (15 mg) and resulted inthe lowest mean level of plasma β-carotene(0.86 mcg/mL). The incidence of lung cancerwas reduced by 55 percent although, becausethere were only 31 total deaths from lung can-cer in the study, the statistical power of lungcancer incidence was low.63 The number ofpatients in this trial who were “ever smokers”(current or former smokers) was 30 percent,compared to 50 percent in the PHS trial, 100percent in the ATBC trial, and 80 percent inthe CARET trial.60-63
The ATBC study, providing 20 mg β-carotene/day, resulted in the highest meanplasma levels of 3.0 mcg/mL, a level 18-timeshigher than the mean baseline. Higher plasmalevels of β-carotene in this study, however, hadno relationship, positive or negative, to lungcancer incidence.60 In all three interventionstudies where the incidence of smoking washighest (ATBC, PHS, CARET), the overallmortality and the incidence of cancer wereinversely correlated with the baseline levelsof β-carotene, independent of treatment pro-tocol.1 The implications of the ATBC andCARET studies – that ß-carotene acts as a co-carcinogen – have been criticized because the
Study
treatment
% former plus current smokers at initiation
Plasma β-carotene levels after intervention (micrograms/ml)
PHS 62
*Aspirin 325 mg*β-carotene 50 mg q other day*combination*placebo
50%
1.2
CARET 61
*retinol (25,000 IU) plus β-carotene (30 mg)*placebo
80%
2.1
Linxian 63
∗β-carotene (15 mg)*selenium (50 mcg)*α tocopherol (30 mg)
30%
0.86
ATBC 60
*α-tocopherol (50 mg)*β-carotene (20 mg)*combination*placebo
100%
3.0
Table 3: Comparisons of Intervention Trials with Beta-Carotene and OtherAntioxidants.

Beta C
arotene
Alternative Medicine Review ◆ Volume 5, Number 6 ◆ 2000 Page 541
Copyright©2000 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
smokers in the studies had been smoking formany years (36-pack-year history was the av-erage in the ATBC study) prior to study entry.The critical stages of initiation and promotionof tumors, stages that antioxidants have beenshown to inhibit,64 may have already been by-passed at the initiation of the trials.1
Carotenoids as Pro-oxidantsCarotenoids, as a class, are particularly
vulnerable to free radical attack due to theirlong chains of conjugated double bonds.65 Apro-oxidant effect has been seen in in vitro andanimal studies, both in high concentrations andin the presence of tocopherol deficiencies.66
The gas phase of cigarette smoke contains highlevels of oxidants (nitric oxide) that have beenshown to interact with lipid membranes to in-duce lipid peroxidation and protein oxidationto form protein-bound carbonyl groups.67 Theprotein-carbonyl groups result in the inactiva-tion of crucial enzymes such as creatine ki-nase and lecithin-cholesterol acyltransferase.67
Carotenoids interact with cigarettesmoke-containing oxidants. Depletion of caro-tenoids and tocopherol, particularly trans-β-carotene, alpha-tocopherol, and lycopene, hasbeen demonstrated in cigarette smoke-exposedhuman plasma.68 As β-carotene acts as a scav-enger of nitrogen oxides in cigarette smoke,β-apo-carotenals and other carotene oxidationproducts are created that, if not effectivelyneutralized by other antioxidants (specificallytocopherol and ascorbate), may initiate celldamage that could lead to neoplasm.65 Mul-tiple studies have substantiated that toco-pherols (both alpha and gamma) protect caro-tenoids from auto-oxidation.69,70 Ascorbate alsoacts to protect both tocopherol and β-carotenefrom oxidative damage and has been shownto preserve β-carotene in oxidized humanLDL.71,72
The theory that β-carotene becomes anoxidant in the plasma and possibly tissues ofsmokers appears to be probable given the lowantioxidant levels of smokers’ blood.68
Whether or not these carotenoid radicals caninitiate cancer is, however, disputed. Baker73
and colleagues examined a model of liposomesexposed to cigarette smoke. They found thatβ-carotene neither enhanced lipid peroxidationin membranes nor contributed to the depletionof other antioxidants. They concluded, “Thedata strongly suggest that, although β-caroteneis readily oxidized by smoke, pro-oxidant ef-fects are unlikely to account for the apparentenhancement of lung cancer in smokers tak-ing this supplement.”
One actual benefit of β-carotene’s pro-oxidant effect may be its action in tumor cells.Carotenoids as a class appear to act as oxidiz-ing agents selectively in tumor cells by increas-ing the production of heat shock proteinswhich ultimately enhance tumor cytotoxicity.74
ConclusionThe issues of absorption and metabo-
lism of carotenoids are full of unansweredquestions. The significant inter-individual andintra-individual variations in absorption of β-carotene indicate the possible effect of medi-cations, individual variations in gut pH, sub-clinical fat malabsorption, and intestinaldysbiosis that exist outside of overt fat malab-sorption and gastrointestinal disease.
Competitive inhibition of differentcarotenoids appears to occur in single-dosingstudies but only bears out in long-term humanstudies that involve smoking populations. It isnot clear whether there is an interaction be-tween synthetic β-carotene and cigarettesmoke that may have caused lower lutein lev-els in the Finnish Smokers Study.
The efficient uptake of synthetic all-trans β-carotene and isomerization in the gutto 9-cis β-carotene appears to make thesynthetic form more desirable for effectiveabsorption. But the tendency of synthetic β-carotene to alter normal serum trans/cis ratiosin favor of the trans isomer may not be abeneficial effect. If, as theorized by You et al,

Page 542 Alternative Medicine Review ◆ Volume 5, Number 6 ◆ 2000
Copyright©2000 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
the preferred absorption of all-trans isomersis a mechanism to control the production of 9-cis retinoic acid by the 9-cis β-carotenoidisomer, then artificial down-regulation of thisimportant chemopreventive growth-regulatormay not be wise.
Clearly, more research is needed tofully understand the antioxidant mechanismsin β-carotenoid physiology. The isomerizationof all-trans ß-carotene in the gut lumen to 9-cis ß-carotene is not a thermodynamically fa-vored reaction and may be catalyzed enzymati-cally.75 The 9-cis ß-carotenoids do appear tohave an advantage as antioxidants in prevent-ing depletion of hepatic ß-carotene stores inthe rat model; however; whether or not cis β-carotenoids act as antioxidants at the humangut surface is unclear.
The transport mechanisms of 9-cis ß-carotenoids may be different than those de-fined for all-trans ß-carotenoids and may ex-plain their appearance in tissues at greater lev-els than those found in plasma. Again, if all-trans ß-carotene is re-isomerized in the tissuesto the 9-cis form, unknown enzymes may cata-lyze these reactions and we have little if anyinformation about them.
The possibility that β-carotene acts asa pro-oxidant and co-carcinogen in the lungtissue of smokers who smoke more than onepack per day has not been ruled out and theuse of β-carotene (natural or synthetic) inheavy smokers or those exposed to significantamounts of airborne nitric oxides must bequestioned, as we do not have enough infor-mation about the antioxidant deficiencies in-herent in this population.
References1. Woutersen R, Wolterbeek APM, Appel MJ, et
al. Safety evaluation of synthetic beta-carotene. Crit Rev Toxicol 1999;29:515-542.
2. Faure H, Fayol V, Galabert C, et al. Caro-tenoids: 1. Metabolism and physiology. AnnBiol Clin 1999;57:169-183.
3. Wang XD, Russell RM. Procarcinogenic andanticarcinogenic effects of beta-carotene. NutrRev 1999;57:263-272.
4. Palozza P. Prooxidant actions of carotenoids inbiologic systems. Nutr Rev 1998;56(9):257-265.
5. Edes TE, Thornton W, Shah J. Beta-caroteneand aryl hydrocarbon hydroxylase in the rat:an effect of beta-carotene independent ofvitamin A activity. J Nutr 1989;119:796-799.
6. Tavani A, La Vechia C. Beta-carotene and riskof coronary heart disease. A review of observa-tional and intervention studies. BiomedPharmacother 1999;53:409-416.
7. Van Poppel G, Goldbohm RA. Epidemiologi-cal evidence for beta-carotene and cancerprevention. Am J Clin Nutr 1995;62:1393S-1402S.
8. Ziegler RG, Mayne ST, Swanson CA. Nutri-tion and lung cancer. Cancer Causes Control1996;7:157-177.
9. De Flora S, Bagnasco M, Vainio H. Modula-tion of genotoxic and related effects bycarotenoids and vitamin A in experimentalmodels: mechanistic issues. Mutagenesis1999;14:153-172.
10. Parker RS. Absorption, metabolism, andtransport of carotenoids. FASEB J1996;10:542-551.
11. Stahl W, Sies H. Uptake of lycopene and itsgeometrical isomers is greater from heat-processed than from unprocessed tomato juicein humans. J Nutr 1992;122:2161-2166.
12. Henderson CT, Mobarhan S, Bowen P, et al.Normal serum response to oral beta-carotenein humans. J Am Coll Nutr 1989;8:625-635.
13. Castenmiller JJ, West CE. Bioavailability andbioconversion of carotenoids. Annu Rev Nutr1998;18:19-38.
14. Hartz SC, Rosenburg IH, Russell RM. Nutri-tion in the Elderly. The Boston NutritionalStatus Survey. London, England: Smith-Gordon Publishers; 1992:80-84.
15. Krasinski SD, Russell RM, Samloff IM, et al.Fundic atrophic gastritis in an elderly popula-tion. Effect on hemoglobin and several serumnutritional indicators. J Am Geriatr Soc1986;34:800-806.
16. Tang G, Serfaty-Lacrosniere C, Camilo ME,Russell R. Gastric acidity influences the bloodresponse to a beta-carotene dose in humans.Am J Clin Nutr 1996;64:622-626.

Beta C
arotene
Alternative Medicine Review ◆ Volume 5, Number 6 ◆ 2000 Page 543
Copyright©2000 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
17. Westrate JA, van het Hof KH. Sucrose polyes-ter and plasma carotenoid concentrations inhealthy subjects. Am J Clin Nutr 1995;62:591-597.
18. Erdman JW, Bierer TL, Gugger ET. Absorp-tion and transport of carotenoids. Ann NY AcadSci 1993;691:76-85.
19. Rock CL, Swendseid ME. Plasma beta-carotene response in humans after mealssupplemented with dietary pectin. Am J ClinNutr 1992;55:96-99.
20. Dimitrov NV, Meyer C, Ullrey DE, et al.Bioavailability of beta-carotene in humans. AmJ Clin Nutr 1988;48:298-304.
21. Roels OA, Trout ME, Dujaquier R. Carotenebalances in boys in Ruanda where vitamin Adeficiency is prevalent. J Nutr 1958;65:115-127.
22. van het Hof KH, West CE, Westrate JA,Hautvast JG. Dietary factors that affect thebioavailability of carotenoids. J Nutr2000;130:503-506.
23. Gronowska-Senger A, Wolf G. Effect ofdietary protein on the enzyme from rat andhuman intestine which converts beta-caroteneto retinal. J Nutr 1970;100:300-308.
24. Blomstrand R, Werner B. Studies on theintestinal absorption of radioactive beta-carotene and vitamin A in man. Conversion ofbeta-carotene into vitamin A. Scand J Clin LabInvest 1967;19:339-345.
25. Suberlich HE, Hodges RE, Wallace DL, et al.Vitamin A metabolism and requirements in thehuman studied with the use of labeled retinol.Vit Horm 1974;32:251-275.
26. Johnson EJ, Russell R. Distribution of orallyadministered beta-carotene among lipoproteinsin healthy men. Am J Clin Nutr 1992;56:128-135.
27. Krinsky NI, Cornwell DG, Oncley JL. Thetransport of vitamin A and carotenoids inhuman plasma. Arch Biochem Biophys1958;73:233-246.
28. Heywood R, Palmer AK, Gregson R, HimmlerH. The toxicity of beta-carotene. Toxicology1985;36:91-100.
29. Brown ED, Micozzi MS, Craft NE, et al.Plasma carotenoids in normal men after asingle ingestion of vegetables or purified beta-carotene. Am J Clin Nutr 1989;49:1258-1265.
30. Mangels AR, Block G, Levander OA, et al.Differences in plasma beta-carotene (P-BC)maintained despite similar dietary beta-carotene. FASEB J 1991;5:A1322. (Abstract)
31. Stahl W, Schwarz W, Sundquist AR, Sies H.Cis-trans isomers of lycopene and beta-carotene in human serum and tissues. ArchBiochem Biophys 1992;294:173-177.
32. Yeum KJ, Ahn SH, Rupp de Paiva SA, et al.Correlation between carotenoid concentrationsin serum and normal breast adipose tissue ofwomen with benign breast tumor or breastcancer. J Nutr 1998;128:1920-1926.
33. Van der Berg H. Carotenoid interactions. NutrRev 1999;57:1-10.
34. Internal document– Cognis Inc. Description ofBetatene 7.5%.
35. Albanes D, Virtamo J, Taylor PR, et al. Effectsof supplemental beta-carotene, cigarettesmoking, and alcohol consumption on serumcarotenoids in the ATBC study. Am J Clin Nutr1997;66:366-372.
36. Fotouhi N, Meydani M, Santos MS, et al.Carotenoid and tocopherol concentrations inplasma, peripheral blood mononuclear cells,and red blood cells after long-term beta-carotene supplementation in men. Am J ClinNutr 1996;63:553-558.
37. Neirenberg DW, Bradley JD, Mott LA, et al.Effect of 4 years of oral supplementation withbeta-carotene on serum concentrations ofretinol, tocopherol, and five carotenoids. Am JClin Nutr 1997;66:315-319.
38. Wahlquist ML, Wattanapenpailboon N, MacraeFL, et al. Changes in serum carotenoids insubjects with colorectal adenomas after 24months of beta-carotene supplementation. AmJ Clin Nutr 1994;60:936-943.
39. Mayne ST, Cartmel B, Silva F, et al. Effect ofsupplemental beta-carotene on plasma concen-trations of carotenoids, retinol, and alpha-tocopherol in humans. Am J Clin Nutr1998;68:642-647.
40. Van den Berg H. Effect of lutein on beta-carotene absorption and cleavage. Int J VitNutr Res 1998;68:360-365.
41. Kostic D, White WS, Olson JA. Intestinalabsorption, serum clearance, and interactionsbetween lutein and beta-carotene whenadministered to human adults in separate orcombined oral doses. Am J Clin Nutr1995;62:604-610.

Page 544 Alternative Medicine Review ◆ Volume 5, Number 6 ◆ 2000
Copyright©2000 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
42. Chandler LA, Schwartz SJ. HPLC separationof cis-trans carotene isomers in fresh andprocessed fruits and vegetables. J Food Sci1987;52:669-672.
43. Krinsky NI, Russett MD, Handelman GJ, et al.Structural and geometrical isomers of caro-tenoids in human plasma. J Nutr1990;120:1654-1661.
44. Wang XD, Krinsky N, Benotti P. Biosynthesisof 9-cis-retinoic acid from 9-cis-beta-carotenein human intestinal mucosa in vitro. ArchBiochem Biophys 1994;313:150-155.
45. Jensen CD, Howes TW, Spiller GA, et al.Observations on the effects of ingesting cis-and trans-beta-carotene isomers on humanserum concentrations. Nutr Rep Int1987;35:413-422.
46. Nagao A, Olson JA. Enzymatic formation of 9-cis, 13-cis, and all-trans retinals from isomersof beta-carotene. FASEB J 1994;8:968-973.
47. Hansen LA, Sigman CC, Andreola F, et al.Retinoids in chemoprevention and differentia-tion therapy. Carcinogenesis 2000;2:1271-1279.
48. Anzano MA, Byers SW, Smith JM, et al.Prevention of breast cancer in the rat with 9-cis-retinoic acid as a single agent and incombination with tamoxifen. Can Res1994;54;4614-4617.
49. Anzano MA, Peer CW, Smith JM, et al.Chemoprevention of mammary carcinogenesisin the rat: combined use of raloxifene and 9-cis-retinoic acid. J Natl Cancer Inst1996;88;123-125.
50. Sun SY, Yue P, Mao L, et al. Identification ofreceptor-selective retinoids that are potentinhibitors of the growth of human head andneck squamous cell carcinoma cells. Clin CanRes 2000;6:1563-1573.
51. Wang XD, Krinsky NI, Benotti PN, Russell R.Biosynthesis of 9-cis-retinoic acid from 9-cis-beta-carotene in human intestinal mucosa invitro. Arch Biochem Biophys 1994;313:150-155.
52. You CS, Parker R, Goodman KJ, et al.Evidence of cis-trans isomerization of 9-cis-beta-carotene during absorption in humans. AmJ Clin Nutr 1996;64:177-183.
53. Levin G, Mokady S. Antioxidant activity of 9-cis compared to all-trans beta-carotene in vitro.Free Rad Biol Med 1994;17:77-82.
54. Levin G, Yeshrun M, Mokady S. In vivoantiperoxidative effect of 9-cis beta-carotenecompared with that of the all-trans isomer.Nutr Cancer 1997;27:293-297.
55. Stahl W, Schwartz W, von Laar J. All-transbeta-carotene preferentially accumulates inhuman chylomicrons and very low densitylipoproteins compared with the 9-cis isomer. JNutr 1995;125:2128-2133.
56. Gaziano JM, Johnson EJ, Russell RM, et al.Discrimination in absorption or transport ofbeta-carotene isomers after oral supplementa-tion with either all-trans or 9-cis-beta-carotene.Am J Clin Nutr 1995;61:1248-1252.
57. Johnson E, Krinsky N, Russell R. Serumresponse of all-trans and 9-cis isomers of beta-carotene in humans. J Am Coll Nutr1996;15:620-624.
58. Tamai H, Morinobu T, Takuji M, et al. 9-cisbeta-carotene in human plasma and blood cellsafter ingestion of beta-carotene. Lipids1995;30:493-498.
59. Von Laar J, Stahl W, Bozen K, et al. Beta-carotene serum levels in patients with erythro-poietic protoporphyria on treatment with thesynthetic all-trans isomer or a natural isomericmixture of beta-carotene. J PhotochemPhotobiol B 1996;33:157-162.
60. Albanes D, Heinonen OP, Taylor PR, et al.Alpha-tocopherol and beta-carotene supple-ments and lung cancer incidence in the Alpha-Tocopherol, Beta-Carotene Cancer PreventionStudy: effects of baseline characteristics andstudy compliance. J Natl Cancer Inst1996;88:1560-1570.
61. Omen GS, Goodman G, Thornquist M, et al.The Beta-Carotene and Retinol Efficacy Trial(CARET) for chemoprevention of lung cancerin high risk populations: smokers and asbestos-exposed workers. Cancer Res 1994;54:2038-2043.
62. Cook N, Lee IM, Manson J, et al. Effects of 12years of beta-carotene supplementation oncancer incidence in the Physician’s HealthStudy (PHS). Am J Epidemiol 1999;149:270-279.
63. Blot WJ, Li JY, Taylor PR, et al. Nutritionalintervention trials in Linxian, China: supple-mentation with specific vitamin/mineralcombinations, cancer incidence, and diseasespecific mortality in the general population. JNatl Cancer Inst 1993;85:1483-1492.

Beta C
arotene
Alternative Medicine Review ◆ Volume 5, Number 6 ◆ 2000 Page 545
Copyright©2000 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
64. Pryor WA. The involvement of free radicals inchemical carcinogenesis. In: Cerutti PA,Nygaard OF, Simic MG, eds.Anticarcinogenesis and Radiation Protection.New York: Plenum Press; 1987:1-9.
65. Palozza P. Prooxidant actions of carotenoids inbiologic systems. Nutr Rev 1998;56:257-265.
66. Lomnitski L, Bergman M, Schon I, GrossmanS. The effect of dietary vitamin E and beta-carotene on oxidation processes in rat testis.Biochim Biophys Acta 1991;1082:101-107.
67. Eiserich JP, van der Vliet A, Handelman GJ, etal. Dietary antioxidants and cigarette smoke-induced biomolecular damage: a complex interac-tion. Am J Clin Nutr 1995;62:1490S-1500S.
68. Handelman GJ, Cross C, Packer L. Oxidationof tocopherols and carotenoids in humanplasma by gas-phase cigarette smoke. FASEB J1995;9:A443. (Abstract).
69. Kennedy TA, Liebler DC. Peroxyl radicalscavenging of beta-carotene in lipid bilayers:effect of oxygen partial pressure. J Biol Chem1992;267:4658-4663.
70. Palozza P, Krinsky NI. Beta-carotene andalpha-tocopherol are synergistic antioxidants.Arch Biochem Biophys 1992;297:184-187.
71. Packer L. Antioxidant action of carotenoids invitro and in vivo and protection againstoxidation of human low density lipoproteins.Ann N Y Acad Sci 1993;691:48-60.
72. Reaven PD, Ferguson E, Navab M, Powell FL.Susceptibility of human LDL to oxidativemodifications: effects of variations in beta-carotene concentration and oxygen tension.Arterioscler Thromb Vasc Biol 1994;14:1162-1169.
73. Baker DL, Krol ES, Jacobsen N, Liebler DC.Reactions of β-carotene with cigarette smokeoxidants. Identification of carotenoid oxidationproducts and evaluation of the prooxidant/antioxidant effect. Chem Res Toxicol1999;12:535-543.
74. Schwartz JL, Singh RP, Teicher B, et al.Induction of a 70 kD protein associated withthe selective cytotoxicity of beta-carotene inhuman epidermal carcinoma. Biochem BiophysRes Comm 1990;169:941-946.
75. Doering WE, Sotirou-Leventis C, Roth WR.Thermal interconversion among 15-cis, 13-cis,and all-trans-beta-carotene: kinetics, Arrheiusparameters, thermochemistry, and potentialrelevance to anticarcinogenicity of all-trans-beta-carotene. J Am Chem Soc 1995;117:2747-2757.