2018 ESC Guidelines for the management of cardiovascular ... › services › hcs › userfiles ›...
40
2018 ESC Guidelines for the management of cardiovascular diseases during pregnancy Μπουγιακλή Μαρία Ειδικευόμενη Καρδιολογίας ΓΝΘ- Γ. ΠΑΠΑΝΙΚΟΛΑΟΥ
Transcript of 2018 ESC Guidelines for the management of cardiovascular ... › services › hcs › userfiles ›...

2018 ESC Guidelines for the management of cardiovascular diseases during pregnancy
Μπουγιακλή Μαρία Ειδικευόμενη ΚαρδιολογίαςΓΝΘ- Γ. ΠΑΠΑΝΙΚΟΛΑΟΥ

Ποια η σημασία των Guidelines?
2018 ESC Guidelines for the management of cardiovascular diseases duringpregnancyEuropean Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340
• 1-4% κυήσεων περιπλέκεται με μητρική νοσηρότητα .
• H καρδιαγγειακή νόσος είναι η πιο συχνή αιτία μητρικού θανάτου στην
Ευρώπη.
•Η αρτηριακή υπέρταση επηρεάζει το 5 - 10% του συνόλου των εγκύων.
Μείζονος σημασίας η γνώση και η αντιμετώπιση των κινδύνων που
σχετίζονται με καρδιαγγειακή νόσο κατά τη διάρκεια της εγκυμοσύνης με
σκοπό την κατάλληλη συμβουλευτική των γονέων πριν αλλά και κατά τη
διάρκεια της εγκυμοσύνης.
Ωστόσο:
• Πολύ μικρός αριθμός περιστατικών ώστε ο κάθε θεράπων ιατρός να
βασιστεί στην εμπειρία του.
• Πολύ μικρός αριθμός τυχαιοποιημένων μελετών. Οι περισσότερες συστάσεις
είναι level C.

2018 ESC Guidelines for the management of cardiovascular diseases duringpregnancyEuropean Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340

2018 ESC Guidelines for the management of cardiovascular diseases during pregnancy European Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340
Έγκυοι με καρδιακή νόσο:
ΑΥΞΗΜΕΝΟΣ ΚΙΝΔΥΝΟΣ ΕΠΙΠΛΟΚΩΝ
ΥπερπηκτικότηταΑυξημένος Όγκος πλάσματος /
CO 40-50%
Μείωση περιφερικών αντιστάσεων
Λευκωματίνη

Έγκυοι με καρδιακή νόσο:
ΑΥΞΗΜΕΝΟΣ ΚΙΝΔΥΝΟΣ ΕΠΙΠΛΟΚΩΝ
Recommendations Class Level
Pre-pregnancy risk assessment and counselling is indicated in all women with known or suspected congenital or acquired cardiovascular and aortic disease.
I C
Αξιολόγηση του κινδύνου και συμβουλευτική:
- Πληροφορημένη λήψη αποφάσεων
- Αλλαγές της φαρμακευτικής αγωγής ανά στάδιο κύησης.
- Σχεδιασμός παρακολούθησης κατά τη διάρκεια της εγκυμοσύνης (τόπος, χρόνος)

2018 ESC Guidelines for the management of cardiovascular diseases during pregnancy European Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340
www.escardio.org/guidelines
II-III

www.escardio.org/guidelines 2018 ESC Guidelines for the management of cardiovascular diseases during pregnancyEuropean Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340
II-III

II-III
Συχνότητα Καρδιαγγειακών επεισοδίων
Counselling
Care during pregnancy
Minimal follow up visits during pregnancy
www.escardio.org/guidelinesCare during delivery 2018 ESC Guidelines for the management of cardiovascular diseases during pregnancy European Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340

II-III
Συμβουλευτική
Care during pregnancy
Minimal follow up visits during pregnancy
www.escardio.org/guidelinesCare during delivery 2018 ESC Guidelines for the management of cardiovascular diseases during pregnancy European Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340
Συχνότητα Καρδιαγγειακών επεισοδίων

2018 ESC Guidelines for the management of cardiovascular diseases duringpregnancy
ΨΑII-III
Συμβουλευτική
Φροντίδα κατά την εγκυμοσύνη
Minimal follow up επισκέψεις κατά τη διάρκεια της εγκυμοσύνης
Τοκετός
European Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340
Συχνότητα Καρδιαγγειακών επεισοδίων

Nέες έννοιες?
2018 ESC Guidelines for the management of cardiovascular diseases duringpregnancyEuropean Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340

Pregnancy Heart Team
cardiologist
obstetrician anesthetist
geneticist CT surgeon
pediatric cardiologist
neonatologist
nurse specialist
hematologist
pulmonary specialist
2018 ESC Guidelines for the management of cardiovascular diseases duringpregnancyEuropean Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340

www.escardio.org/guidelines 2018 ESC Guidelines for the management of cardiovascular diseases during pregnancyEuropean Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340
II-III
Δεν βασίζεται στην ανά ασθένεια κατηγοριοποίηση

Αξιολόγηση κινδύνου- Διάγνωση
• Ηλεκτροκαρδιογράφημα
• Υπερηχοκαρδιογράφημα
• Σε περιπτώσεις παθήσεων αορτής, MRI/ CT scan εάν κρίνεται απαραίτητο
•Διενέργεια εργομετρίας ή δοκιμασίας κόπωσης. Η μέγιστη πρόσληψη Ο₂ > 80% συνδέεται με θετική έκβαση της κύησης.

uidelines for the management of cardiovascular diseases during pregnancyEuropean Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340
ww.escardio.org/guidelines 2018 ESCGw
Πίνακας 4 Προγνωστικοί παράγοντες καρδιαγγειακών συμβάντων
Predictors of maternal cardiovascular events
Prior cardiac event (heart failure, transient ischaemic attack, stroke, arrhythmia)
Pulmonary arterial hypertension
NYHA class III/IV Cardiac medication before pregnancy
Left heart obstruction (moderate to severe) Cyanosis (O2 <90%)
Reduced systemic ventricular systolic function (ejection fraction <40%)
Natriuretic peptide levels (NT-proBNP>128 pg/mL at 20 weeks predictive of event later in pregnancy)
Reduced subpulmonary ventricular function (TAPSE <16 mm)
Smoking history
Systemic atrioventricular valve regurgitation (moderate to severe)
Mechanical valve prosthesis
Pulmonary atrioventricular valve regurgitation (moderate to severe)
Repaired or unrepaired cyanotic heart disease

2018 ESC Guidelines for the management of cardiovascular diseases during pregnancyEuropean Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340
Αυξημένος κίνδυνος νεογνικών συμβάντων

uidelines for the management of cardiovascular diseases during pregnancyEuropean Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340
ww.escardio.org/guidelines 2018 ESCG
Predictors of maternal cardiovascular eventsPulmonary arterial hypertension
Cardiac medication before pregnancy
Cyanosis (O2 <90%)
Natriuretic peptide levels (NT-proBNP>128 pg/mL at 20 weeks predictive of event later in pregnancy)
Smoking history
Mechanical valve prosthesis
Predictors of maternal cardiovascular events
Prior cardiac event (heart failure, transient ischaemic attack, stroke, arrhythmia)
NYHA class III/IV
Left heart obstruction (moderate to severe)
Reduced systemic ventricular systolic function (ejection fraction <40%)
Reduced subpulmonary ventricular function (TAPSE <16 mm)
Systemic atrioventricular valve regurgitation (moderate to severe)
Pulmonary atrioventricular valvew regurgitation (moderate to severe)
Repaired or unrepaired cyanotic heart disease

Mηχανική Βαλβίδα
ROPAC registry: θρόμβωση βαλβίδας 4.7% & 20% θνητότητα
UK study: Έγκυοι με μηχανική βαλβίδα 9% θάνατος & 28% θετική έκβαση κύησης
www.escardio.org/guidelineswww.escardio.org/guidelines 2018 ESC Guidelines for the management of cardiovascular diseases during pregnancy2
7 European Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy 340
Van Hagen Circ 2015
Vause BJOG 2017

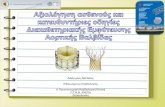
Flowchart on anticoagulation in mechanical valves and high-dose VKA
Woman with mechanical valve and HIGH dose VKA(wafarin >5 mg/day or phenprocoumon >3 mg/day or acenocoumarol >2 mg/day)
who contemplates pregnancy: Pre-pregnancy counselling – Continue VKA antagonist until pregnant
PREGNANT
In-hospital change to i.v. UFH (aPTT ≥2x control) (l)or in-hospital change to LMWH 2-daily or continue LMWH, close monitoring b(l)
i.v. UFH (aPTT ≥2x control) (l)
Stop UFH 4-6 hours before delivery and restart 4-6 hours after delivery if no bleeding
Continue VKA, monitor INR at least 2-weekly (llb)
Continue VKA, monitor INR at least 2-weekly (lla)
Continue LMWH 2-daily close monitoring (llb)°
In-hospital change from LMWH/UFH to VKA (lIa).
When on target INR monitor INR at least 2-weekly
1st trim.
2nd/3rd
trim.
36weeks
36 hrs before planned delivery
Delivery
In-hospital changeOR to i.v. UFH aPTT ≥2x control OR
(lla)a
In-hospital change toLMWH 2-daily, closemonitoring (lla)a, b
2018 ESC Guidelines for the management of cardiovascular diseases duringpregnancyEuropean Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340

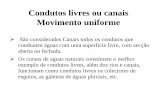
Flowchart on anticoagulation in mechanical valves and low-dose VKA
Woman with mechanical valve and LOW dose VKA(wafarin <5 mg/day or phenprocoumon <3 mg/day or acenocoumarol <2 mg/day)
who contemplates pregnancy: Pre-pregnancy counselling – Continue VKA antagonist until pregnant
PREGNANT
In-hospital change to i.v. UFH (aPTT ≥2x control) (l)or in-hospital change to LMWH 2-daily or continue LMWH, close monitoring b(l)
i.v. UFH (aPTT ≥2x control) (l)
Stop UFH 4-6 hours before delivery and restart 4-6 hours after delivery if no bleeding
Continue VKA, monitor INR at least 2-weekly (lla)
In-hospital changeto LMWH 2-daily,monitoring (llb)a,b
Continue VKA, monitor INR at least 2-weekly (l)
In-hospital change from UFH to VKA (l).
When on target INR monitor INR at least 2-weekly
In-hospital change from LMWH to VKA (l).
When on target INR monitor INR at least 2-weekly
1st trim.
2nd/3rd
trim.
36weeks
36 hrs before planned delivery
Delivery
ORIn-hospital change to i.v.
OR UFH (aPTT ≥2x control)(llb)b
2018 ESC Guidelines for the management of cardiovascular diseases duringpregnancyEuropean Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340

2018 ESC Guidelines for the management of cardiovascular diseases duringpregnancyEuropean Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340
Συγγενείς Καρδιοπάθειες
2/3 όλων των καρδιακών παθήσεων κατά τη διάρκεια της εγκυμοσύνης
Σπάνιο αίτιο μητρικής θνητότητας στην εγκυμοσύνη

Sub-classification No. of deaths
Ischaemic deaths 34
Valve disease/endocarditis 11
Sudden death (normal heart) 47
Essential hypertension 6
Myocardial disease/cardiomyopathy 27
Aortic dissection 21
Pulmonary Hypertension 6
Undetermined CV disease 1
Total 153
2012-2014
2018 ESC Guidelines for the management of cardiovascular diseases duringpregnancyEuropean Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340

Sub-classification No. of deaths
Ischaemic deaths 34
Valve disease/endocarditis 11 (4)
Sudden death (normal heart) 47
Essential hypertension 6
Myocardial disease/cardiomyopathy 27
Aortic dissection 21 (5)
Pulmonary Hypertension 6 (2)
Undetermined CV disease 1
Total 153
2012-2014
<10%Θάνατοι
λόγω συγγενών παθήσεων
2018 ESC Guidelines for the management of cardiovascular diseases duringpregnancyEuropean Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340

Πνευμονική Υπέρταση
2018 ESC Guidelines for the management of cardiovascular diseases duringpregnancyEuropean Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340
Recommendations Class Level
Right heart catheterization is recommended to confirm the diagnosis of PAH (group 1). This can be performed during pregnancy but with very strict indications.
l C
Treatment dose LMWH is recommended in pregnant patients with chronic thromboembolic pulmonary hypertension.
l C
If a PAH patient conceives on targeted PH therapies, consideration should be given to withdrawing embryotoxic drugs, taking into account the risks of withdrawal.
lla C
In treatment-naive pregnant PAH patients, initiating treatment should be considered.
lla C
Pregnancy is not recommended in patients with PAH. lll B

Παρακολούθηση κατά τη διάρκεια της εγκυμοσύνης
2018 ESC Guidelines for the management of cardiovascular diseases duringpregnancyEuropean Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340
Όλες οι γυναίκες με συγγενή καρδιοπάθεια ή άλλες γενετικές καρδιακές παθήσεις πρέπει να υποβάλλονται σε εμβρυικό υπέρηχο καρδιάς στις 19-22 εβδομάδες της κύησης.
Συνίσταται υπερηχοκαρδιογραφικός έλεγχος (20 εβδομάδες) στις εγκύους με γνωστή καρδιακή νόσο ή εκδήλωση ανεξήγητων ή νέων καρδιαγγειακών σημείων και συμπτωμάτων
Στις 20-30 εβδομάδες κύησης θα πρέπει να σχεδιαστεί λεπτομερές πλάνο που περιλμβάνει την επαγωγή και τη διαχείρηση του τοκετού καθώς και την παρακολούθηση κατά τη λοχεία.
Αναγκαιότητα αντιπηκτικής αγωγής: H ηπαρίνη Χ.Μ.Β μπορεί να χρησιμοποιηθεί μόνο σε διαθεσιμότητα εβδομαδιαίας παρακολούθησης επιπέδων anti-Xa.

Tοκετός
2018 ESC Guidelines for the management of cardiovascular diseases duringpregnancyEuropean Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340
Η επαγωγή του τοκετού θα πρέπει να πραγματοποιηθεί στις 40 εβδομάδες κύησης, σε όλες τις γυναίκες με καρδιακή νόσο.
Ο Κολπικός τοκετός πρέπει να αποτελεί την πρώτη επιλογή για την πλειοψηφία των ασθενών.
Eνδείξεις Καισαρικής Τομής:‒Πρόωρος τοκετός σε ασθενείς υπό OACs,‒Επείγουσα παθολογία αορτής‒Οξεία Καρδιακή Ανεπάρκεια ‒Σοβαρές μορφές πνευμονικής υπέρτασης ( σύνδρομο Eisenmenger’s ).
Προφυλακτική αντιβιοτική αγωγή για ενδοκαρδίτιδα ΔΕΝ συνίσταται

Αντενδείξεις εγκυμοσύνης (mWHO 4)
he following patients should be counsell ned against preg ancy:
u
‒ Fontan oparrhythmi
‒ pulmonar‒ severe sys‒ severe (re‒ systemic r
eration and aas, or valve rey arterial hype temic ventric-)coarctation ight ventricle
ditional cogurgitation)rtensionlar dysfuncti
with modera e
orbidities (vent
on (EF <30% or
te or severely d
ricular dysfunctio
NYHA class III–IV)
creased ventricu
n,
lar function
‒ Σοβαρή διάταση αορτής ή ιστορικό διαχωρισμού αορτής‒ Σοβαρή ΜS (ακόμη και ασυμτωματική)‒ Ασθενείς με σοβαρού βαθμού AS και συμπτωματολογία ή χωρίς
συμπτωματολογία με επηρεασμένη λειτουργικότητα αριστερής κολίας ή παθολογική δοκιμασία κόπωσης.
‒ Μη βελτίωση Κλάσματος Εξώθησης σε ασθενείς με παλαιότερη PPCM
Marfan
2018 ESC Guidelines for the management of cardiovascular diseases duringpregnancyEuropean Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340
Bicuspid LoeysDietz Turner aortic valve
Vascular Ehlers-Danlos
become pregnant
Advise not to Ascendingaorta >45 mm (or >40 mm in family history of dissection or sudden death)
aorta>50 mm
Ascending Ascending aorta>45 mm (or>40mm in family history of dissection or sudden death)
ASI >25 mm/m2 All patients

Στεφανιαία Νόσος
2018 ESC Guidelines for the management of cardiovascular diseases duringpregnancyEuropean Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340
Recommendations Class Level
ECG and measurement of troponin levels are recom-mended when a pregnant woman has chest pain.
l C
Primary PCI is recommended as the preferred reperfusion therapy for STEMI during pregnancy.
l C
An invasive management strategy should be considered for NSTE-ACS with risk criteria.
lla C
Conservative management should be considered for stable NSTEMI/NSTE-ACS with low risk criteria.
lla C
Follow-up should be considered over at least the next 3 months.
lla C
Breastfeeding is not recommended in mothers who take anti-platelet agents other than low-dose aspirin due to a lack of data.
lll C
Παρότι τα ΟΣΣ συμβαίνουν σπάνια κατά τη διάρκεια τη εγκυμοσύνης
(~ 5 /100 000), εντούτοις η ΣΝ είναι υπεύθυνη για > 20% όλων τον μητρικών καρδιακών θανάτων.
Στις περισσότερες περιπτώσεις ΟΣΣ απουσία αθηροσκληρωτικών μηχανισμών •Αυτόματος διαχωρισμός στεφανιαίων αγγείων(43%),•Φυσιολογικές στεφανιαίες αρτηρίες αγγειογραφικά (18%)•Θρόμβωση στεφανιαίων(17%).

Μυοκαρδιοπάθεις και Καρδιακή Ανεπάρκεια
2018 ESC Guidelines for the management of cardiovascular diseases duringpregnancyEuropean Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340
Η Περιγεννητική Μυοκαρδιοπάθεια (PPCM), τοξική, υπερτοφική (HCM), διατατική(DCM), Takotsubo cardiomyopathy (TTC) είναι σπάνιες αλλά μπορούν να προκαλέσουν σοβαρές επιπλοκές στην εγκυμοσύνη.
PPCM παρουσιάζεται με συμπτώματα ΚΑ λόγω συστολικής δυσλειτουργίας ΑΚ στο τέλος της κύησης και τους πρώτους μήνες μετά τον τοκετό. Συνηθέστερα ΚΕ < 45 %, με θνητότητα από 2.0% στη Γερμανία έως 24 % στην Τουρκία.
Θεραπεία παρόμοια με μη-εγκύους και ΚΑ, χωρίς τα εμβρυοτοξικά φάρμακα(ACE inhibitors, ARB, ARNI, MRA).
Bromocriptine αποτελεί νέα οδηγία με απαραίτητη τη συνοδεία αντιπηκτικής αγωγής.
Αυξημένος κίνδυνος επιδείνωσης σε επόμενη κύηση γυναίκες με ιστορικό PPCM καιDCM, εάν δεν ομαλοποιηθεί το ΚΕ.

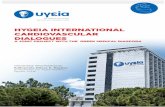
Management of acute heart failure during/after pregnancy
Assess heart failure severitySBP <90 mmHg; HR >130/min or <45/min
RR <25/min; SpO2 <90%Lactate >20 mmol/L; ScvO2 <60%
Altered mental state; cold skin; oliguria
Confirm diagnosisECG
Blood tests incl. natriuretic peptides Echocardiography, consider lung ultrasound,
Consider additional tests to exclude differential diagnosis
Initial
evaluation
Stabilized AHF
Antepartum
HF therapy Hydralazine
Nitrates Beta-blocker
Consider diuretics
Consider delivery (vaginal delivery
with PDA)
Postpartum
HF therapy ACE-I (or ARB)Beta-blocker
MR antagonist Diuretics
Consider Ivabradine
Consider bromocriptine
in patients with PPCM
Consider WCD therapyif LVEF ≤35%
Continue HF therapy
Severe AHF/Cardiogenic Shock
Optimize preloadVolume vs diuretics; vasodilators if SBP >110 mmHg
Optimize oxygenationConsider NIV, invasive ventilation if SpO2 <95%
Add inotropes and/or vasopressorsConsider levosimendan 0.1 mcg/kg/min during 24 h
Urgent delivery (caesarean section)
Consider bromocriptine in patients with PPCM
Consider mechanical circulatory support (MCS)plan delivery strategy to have access to
MCS if necessary
Recovery?
Transplantation Weaning
2018 ESC Guidelines for the management of cardiovascular diseases duringpregnancyEuropean Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340
www.escardio.org/guidelines

Αρρυθμίες
Risk for arrhythmia .. at delivery
Surveillance at delivery
Classb Levelc
Low risk PSVT, AF, idiopathic VT, low-risk LQTS, WPW 1 l C
syndrome
Medium risk Unstable SVT, VT, ICD carriers, VT and structural 2 l C
heart disease, Brugada syndrome; moderate risk:
LQTS, catecholaminergic polymorphic VT
High risk for life threatening Unstable VT in structural heart disease/congenital 3 l C
arrhythmia heart disease, unstable VT/TdP in high-risk LQTS
patients, short QT syndrome, high-risk
catecholaminergic polymorphic VT
2018 ESC Guidelines for the management of cardiovascular diseases duringpregnancyEuropean Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340
AF και PSVT είναι οι πιο συχνές αρρυθμίες. Συνήθως καλοήθεις και διαχειρίσιμες.
Οι απειλητικές για τη ζωή κοιλιακή ταχυκαρδία (VT) και κοιλιακή μαρμαρυγή (VF)
όπως και οι διαταραχές αγωγής είναι εξαιρετικά σπάνιες.

Διαχείριση αρρυθμιών
5
Recommendations Class Level
Acute management (iv admin of drugs) of SVT and AF
Vagal manoeuvres, followed by adenosine if these fail, are recommended for acute conversion of PSVT.
l C
Immediate electrical cardioversion is recommended for any tachycardia with haemodynamic instability and for pre-excited AF.
l C
Adenosin• Δεν διαπερνά τον πλακούντα• Δεν εισέρχεται στο μητρικό γάλα• Δεν έχουν αναφερθεί παρενέργειες στο
έμβρυο
Πίνακας Drug and safety data
www.escardio.org/guidelines

Διαχείριση αρρυθμιών
Recommendations Class Level
Acute management (iv admin of drugs) of SVT and AF
Vagal manoeuvres, followed by adenosine if these fail, are recommended for acute conversion of PSVT.
l C
Immediate electrical cardioversion is recommended for any tachycardia with haemodynamic instability and for pre-excited AF.
l C
Hλεκτρική Ανάταξη• Δεν διαταράσει εμβρυική κυκλοφορία• Μικρός κίνδυνος πρόκλησης αρρυθμιών στο έμβρυο ή πρόωρο
τοκετό• Θα πρέπει να ελέγχεται το έμβρυο μετά

Διαχείριση αρρυθμιών
Recommendations Class Level
Acute management (iv admin of drugs) of SVT and AF
Beta-1-selective blockers should be considered for acute conversion of PSVT.
lla C
Ibutilide or flecainide may be considered for termination of atrial flutter and AF in stable patients with structurally normal hearts.c
llb C
Ibutilide or flecainideCase reports (limitedhuman data)
2018 ESC Guidelines for the management of cardiovascular diseases duringpregnancyEuropean Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340

Διαχείριση αρρυθμιών
Recommendations Class Level
Long-term management (oral administration of drugs) of SVT and AF (cont’d)
Beta-selective blockers are recommended for rate control of AT or AF.
l C
Flecainidee, propafenone,e or sotalolf should be considered to prevent SVT, AT, and AF if AV nodal blocking agents fail.
lla C
2018 ESC Guidelines for the management of cardiovascular diseases duringpregnancyEuropean Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340
Flecainide & sotalol:
Έπιτρέπεται η γαλουχία εάν η
μητέρα λαμβάνει το φάρμακο.

Υπέρταση- Σημαντικά μηνύματα
2018 ESC Guidelines for the management of cardiovascular diseases duringpregnancyEuropean Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340
Χορήγηση αντιυπερτασικής αγωγής συνίσταται σε όλες τις γυναίκες με BP ≥150/95 mmHg και >140/90 mmHg σε γυναίκες με:
‒Υπέρταση κύησης (με ή χωρίς πρωτεïνουρία),
‒Προϋπάρχουσα υπέρταση
‒Υπέρταση με υποκλινική βλάβη οργάνων-στόχων κατά τη διάρκεια της εγκυμοσύνης.
Γυναίκες μετρίου- υψηλού κινδύνου για προεκλαμψία συνίσταται να λαμβάνουν 100-150 mg ασπιρίνης ημερησίως από τη 12η έως τη 36-37η εβδομάδα συμπληρωματικά με την αντιυπερτασική αγωγή.
Φάρμακα που ενδείκνυνται για τη θεραπεία της υπέρτασης κύησης είναι η λαβεταλόλη, η μεθυλντόπα και οι ανταγωνιστές ασβεστίου (κυρίως νιφεδιπίνη)

Διαχείριση της Υπέρτασης
2018 ESC Guidelines for the management of cardiovascular diseases duringpregnancyEuropean Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340
Recommendations Class Level
In women with gestational hypertension or mild pre-eclampsia, delivery is recommended at 37 weeks.
l B
It is recommended to expedite delivery in pre-eclampsia and with adverse conditions such as visual disturbances or haemostatic disorders.
l C
In pre-eclampsia associated with pulmonary oedema, nitroglycerin given as an intravenous infusion is recommended.
l C
In severe hypertension, drug treatment with intravenous labetalol, or oral methyldopa or nifedipine, is recommended.
l C
Weight gain, limited to <6.8 kg for obese pregnant women, should be considered.
lla C
ACE inhibitors, ARBs, or direct renin inhibitors are not recommended. llI C

Φλεβική θρομβοεμβολή (VTE)
2018 ESC Guidelines for the management of cardiovascular diseases duringpregnancyEuropean Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340
Οι Η.Χ.Μ.Β είναι οι παράγοντες εκλογής για την πρόληψη και θεραπεία VTE.
Για τις γυναίκες υψηλού κινδύνου, συνίσταται η προφυλακτική χορήγηση Η.Χ.Μ.Β σχετιζόμενη με το βάρος (π.χ enoxaparin 0.5 mg/kg ημερησίως)
Aξιολόγηση παραγόντων κινδύνου για VTE στην αρχή της κύησης.
D Dimers αναξιόπιστα για τη διάγνωση.
Η θεραπευτική δόση της Η.Χ.Μ.Β θα πρέπει να εξαρτάται από το σωματικό βάρος.
Θρομβόλυση σε Πνευμονική Εμβολή ενδείκνται μόνο σε αιμοδυναμική αστάθεια

easesduring1093/eurhea
pregnancyrtj/ehy340
www.escardio.org/guidelineswww.escardio.org/guidelines 2018 ESC Guidelines for the management of cardiovascular dis European Heart Journal (2018) 00, 1–83- doi:10.
Drugs and safety data
Drugs Classification (Vaughan Williams for antiarrhythmic drugs)
Former
FDA
category
Placenta
permeable
Transfer to
breast milk (foetal dose)
Pre-clinical/
clinical safety data
The table on drugs an safety data can be found in the Full text of the Guidelines and it isavailable at: www.escardio.org/guidelines and on the European Heart Journal w(https://academic.oup.com/eurheartj/articlelookup/doi/10.1093/eurheartj/ehy
eb site340).
Recommendations Class Level
Before pharmacological treatment in pregnancy is started, it is recommended to check
Table 19 for clinical safety data.l C
In the absence of clinical safety data, it is recommended to check …for pre-clinical safety
data.l C
In the absence of adequate human safety data, decision-making should be based on
individual drug efficacy and safety profiles, and the available animal data, and the
decision must be made together with the patient.lla C
Decision-making based on former FDA categories alone is no longer recommended. llI C

2018 ESC Guidelines for the management of cardiovascular diseases during pregnancyEuropean Heart Journal (2018) 00, 1–83- doi:10.1093/eurheartj/ehy340
Ευχαριστώ για την προσοχή σας