BAIAE
49
CASE STUDY: Bronchial Asthma In Acute Exacerbation I. INTRODUCTION A. DEFINITION Asthma (from the Greek άσθμα, ásthma, "panting") is the common chronic inflammatory disease of the airways characterized by variable and recurring symptoms, reversible airflow obstruction, and bronchospasm. Symptoms include wheezing, coughing, chest tightness, and shortness of breath. Asthma is clinically classified according to the frequency of symptoms, forced expiratory volume in 1 second (FEV1), and peak expiratory flow rate. Asthma may also be classified as atopic (extrinsic) or non-atopic (intrinsic). It is thought to be caused by a combination of genetic and environmental factors. Treatment of acute symptoms is usually with an inhaled short-acting beta-2 agonist (such as salbutamol). Symptoms can be prevented by avoiding triggers, such as allergens and irritants, and by inhaling corticosteroids. Leukotriene antagonists are less effective than corticosteroids and thus less preferred. 1 | P a g e
-
Upload
mishiel-castillo -
Category
Documents
-
view
266 -
download
4
Transcript of BAIAE

CASE STUDY: Bronchial Asthma In Acute Exacerbation
I. INTRODUCTION
A. DEFINITION
Asthma (from the Greek άσθμα, ásthma, "panting") is the common chronic
inflammatory disease of the airways characterized by variable and recurring symptoms,
reversible airflow obstruction, and bronchospasm. Symptoms include wheezing, coughing,
chest tightness, and shortness of breath. Asthma is clinically classified according to the
frequency of symptoms, forced expiratory volume in 1 second (FEV1), and peak expiratory
flow rate. Asthma may also be classified as atopic (extrinsic) or non-atopic (intrinsic).
It is thought to be caused by a combination of genetic and environmental factors.
Treatment of acute symptoms is usually with an inhaled short-acting beta-2 agonist (such as
salbutamol). Symptoms can be prevented by avoiding triggers, such as allergens and irritants,
and by inhaling corticosteroids. Leukotriene antagonists are less effective than
corticosteroids and thus less preferred.
Its diagnosis is usually made based on the pattern of symptoms and/or response to
therapy over time. The prevalence of asthma has increased significantly since the 1970s. As
of 2010, 300 million people were affected worldwide. In 2009 asthma caused 250,000 deaths
globally. Despite this, with proper control of asthma with step down therapy, prognosis is
generally good.
ETIOLOGY:
Asthma commonly results from hyperresponsiveness of the trachea and bronchi to
irritants. Allergy influences both the persistence and the severity of asthma, and atopy or the
1 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
genetic predisposition for the development of an IgE-mediated response to common airborne
allergens is the most predisposing factor for the development of asthma.
CLASSIFICATION:
1. Extrinsic Asthma – called Atopic/allergic asthma. An “allergen” or an “antigen” is a
foreign particle which enters the body. Our immune system over-reacts to these often
harmless items, forming “antibodies” which are normally used to attack viruses or
bacteria. Mast cells release these antibodies as well as other chemicals to defend the
body.
Common irritants:
Cockroach particles
Cat hair and saliva
Dog hair and saliva
House dust mites
Mold or yeast spores
Metabisulfite, used as a preservative in many beverages and some foods
Pollen
2. Intrinsic asthma – called non-allergic asthma, is not allergy-related, in fact it is
caused by anything except an allergy. It may be caused by inhalation of chemicals such
as cigarette smoke or cleaning agents, taking aspirin, a chest infection, stress, laughter,
exercise, cold air, food preservatives or a myriad of other factors.
2 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
Smoke
Exercise
Gas, wood, coal, and kerosene heating units
Natural gas, propane, or kerosene used as cooking fuel
Fumes
Smog
Viral respiratory infections
Wood smoke
Weather changes
SIGNS AND SYMPTOMS:
1. Non Productive to Productive Cough
2. Dyspnea
3. Wheezing on expiration
4. Cyanosis
5. Mild apprehension and restlessness
6. Tachycardia and palpitation
7. Diaphoresis
CLINICAL MANIFESTATIONS:
1. Increased respiratory rate
2. Wheezing (intensifies as attack progresses)
3. Cough (productive)
3 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
4. Use of accessory muscles
5. Distant breath sounds
6. Fatigue
7. Moist skin
8. Anxiety and apprehension
9. Dyspnea
Bronchial asthma in Acute Exacerbation
Bronchial asthma acute exacerbation is actually another term for a chronic asthma
attack. During bronchial asthma acute exacerbation bronchial tubes tighten instantly and
make it very hard for the air to flow through them. This is a very difficult situation because a
person suffering from the attack cannot breathe, and can enter a stage of shock.
Many things are considered a trigger for a bronchial asthma acute exacerbation.
These things are allergens (pet hair, pollen, smoke, dust etc), air pollution and air toxins, hard
physical activity and stress and anxiety.
B. MORBIDITY AND MORTALITY
As of 2009, 300 million people worldwide were affected by asthma leading to
approximately 250,000 deaths per year.
4 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
It is estimated that asthma has a7-10% prevalence worldwide. As of 1998, there was a
great disparity in the prevalence of asthma across the world, with a trend toward more
developed and westernized countries having higher rates of asthma, with as high as a 20 to
60-fold difference. Westernization however does not explain the entire difference in asthma
prevalence between countries, and the disparities may also be affected by differences in
genetic, social and environmental risk factors. Mortality however is most common in low to
middle income countries, while symptoms were most prevalent (as much as 20%) in the
United Kingdom, Australia, New Zealand, and Republic of Ireland; they were lowest (as low
as 2–3%) in Eastern Europe, Indonesia, Greece, Uzbekistan, India, and Ethiopia.
Asthma affects approximately 7% of the population of the United States and 5% of
people in the United Kingdom. Asthma causes 4,210 deaths per year in the United States. In
2005 in the United States asthma affected more than 22 million people including 6 million
children. It accounted for nearly 1/2 million hospitalizations that same year. More boys have
asthma than girls, but more women have it than men. In England, an estimated 261,400
people were newly diagnosed with asthma in 2005; 5.7 million people had an asthma
diagnosis and were prescribed 32.6 million asthma-related prescriptions.
C. INCIDENCE AND PREVALENCE
There are no available nationwide data published on asthma prevalence. However, the
limited reports gathered showed a prevalence of 12% in children aged 13-14 years and 17-
22% in older age groups.
5 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
LOCAL PREVALENCE
Three thousand two hundred and seven children in Metro Manila aged 13-14 years
participated in the International Study of Asthma and Allergies in Children (ISAAC).
Participants accomplished a 12-month prevalence of self-reported asthma symptoms from
written questionnaires and from video questionnaires. The results showed that approximately
12% and 8% prevalence based on responses to the written questionnaires and to the video
questionnaires respectively. In a subsequent study, 12.3% of the same population reported
wheezing.
A local study estimating the prevalence of asthma and allergies in adults was
completed in Malolos, Bulacan in 1998. One thousand five (1,005) adults (ages 18-44 years)
were interviewed using a pre-tested questionnaire adapted from the European Community
Health Survey (ECHRS) and the ISAAC. The study showed a prevalence of 17.2% for
asthma and 49.9% for allergy among adults. Another study conducted at the Lung Center of
the Philippines reported a prevalence of 22% in adults.
D. REASONS FOR CHOOSING THE DISEASE
We choose Bronchial Asthma in Acute Exacerbation as our case to be studied because
we want each and all of us whether men and women, children and adult to be aware of the
possible causes of the disease and the prevention and management of patient with such
respiratory disease. Moreover, we are all at our teenage year and smoking as major causes of
BAIAE is very common addiction of most teenagers.
6 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
II. OBJECTIVES
A. GENERAL OBJECTIVES
Within 8 hours of exposure at World Citi Medical Center (WCMC) 7th floor ward,
we, BSN III-A Group 2 student nurses from World Citi Colleges (WCC) Antipolo campus
aim to use our knowledge, skills, and attitude to render holistic care to our client as well as
convey information with regards to the promotion and maintenance of health in order for our
client to achieve possible wellness state and carry out activities of daily living.
B. SPECIFIC OBJECTIVES
Knowledge
>To know how this respiratory disease affects patient’s life.
>To identify the problem of the patient
>To formulate exact and effective nursing care plan to the patient
>To review the normal anatomy and physiology of the respiratory system
>To discern the pathophysiology of the disease
Skills
>To improve our ability to handle respiratory disease and to enhance our skills to the
applications of our knowledge.
>To provide health teachings and nursing interventions
7 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
Attitude
>To establish good nurse-patient relationship with our client and to improve the level of our
communications to our patient and staff nurses.
>To build rapport with the patient
III. SIGNIFICANCE OF THE STUDY
To patient with Bronchial Asthma in Acute Exacerbation:
>To acquire necessary knowledge related to their health condition.
>To be able to manage them when pain and abnormalities related to the disease occurs.
>To be able to understand the treatment that the health care providers offer in their recovery
process.
>To promote prevention of the disease
To staff nurses:
>To properly indentify the needs of the patient
>To be able to render nursing care and information to the patient through the application of
the nursing skills.
>To apply their knowledge and skills when caring to patients with pelvic organ prolapsed.
8 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
To nursing students:
>To properly assess patients who are manifesting the disease.
>To be knowledgeable in the treatment they are providing them.
>To be able to provide more health teachings in the prevention of the disease.
IV. SCOPE AND DELIMITATIONS
We had our duty at World Citi Medical Center (WCMC) 7th floor, in Quezon City last
January 30, 2012. We were able to assess the patient’s condition but not that holistic due to
lack of time and chances and the irritable feelings of our patient due to her condition but
through keen observations, little participation of the client, patient’s chart and records. We
are able to gather certain information needed to formulate this case study. The study lasted
about 8 hours of exposure with the patient. Our client, Mrs. E.M. is suffering from Bronchial
Asthma in Acute Exacerbation (BAIAE) which we will be dealing with this study. This
includes its CAUSES and PREVENTION for the wellness of our patient.
9 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
V. NURSING HISTORY
Name : Ms. EM
Age : 36 y/o
Gender : Female
Birthday : Jan 1, 1976
Weight : 59 kg (129.8 lbs)
Height : 157 cm
Religion : Catholic
Nationality : Filipino
Address : Quezon City
Occupation : Plain Housewife
Status : Married
Hospitalization : (-)
Case Numver : 191944
Date of Admission : January 26, 2012
Chief Complain : fever and cough and colds
Attending Physician : Dr. Agustin
Admitting Diagnosis : Bronchial Asthma In Acute Exacerbation, Hypertension
Final Diagnosis : Bronchial Asthma In Acute Exacerbation, Hypertension
10 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
A. History of Present Illness
Patient is known asthmatic and was maintained on seretide and salbutamol
Turbohaler PRN, last attack was 1 year ago.
One week PTC, patient had on and off episode of fever; Temp is 39 C with
nonproductive cough and night time awakening, > 4x/week and shortness of breath. Patient
just took paracetamol and salbutamol but to no avail. This prompted consult.
B. Past Medical History
(+) Hypertension
(-) DM
(+) BA
C. Family History
(+) Hypertension (Father/Mother)
(+) Asthma (Father)
11 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
VI. 13 AREAS OF ASSESSMENT
Social Status
Mrs. E.M. 36 years old born on Jan 1, 1976 is a plain housewife. She resides at
Quezon City together with her husband and with her 3 kids. She’s the one who takes care of
her 2 daughters and her 1 son. She sometimes goes out of their house to talk with her
neighbors. She does not stay too long along the streets because she tends to have an attack
whenever she inhales street dust.
Mental Status
Mrs. E.M. is oriented to time, place, events and person. She is able to recall recent
and past events in her life. She is able to read and write and can speak in English and
Tagalog. She is responsive and answers to the questions being asked.
Emotional State
Mrs. E.M. says that she feels a little stressed because of her confinement. Also, she is
somewhat irritable because of her condition.
Sensory Perception
Vision Mrs. E.M. only uses reading glasses.
Hearing Mrs. E.M.’s hearing ability is okay because she is able to answers our
questions without us repeating it.
Smell N/A
12 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
Taste Mrs. E.M. claims that she can taste every food she is being offered.
Touch Mrs. E.M. responds to our touch.
Motor Ability
Mrs. E.M. is lethargic and a bit weak. She can move freely in her bed but she needs
help from her companion when sitting up and going to the bathroom.
Nutritional Status
Before Mrs. E.M. was admitted she states that she eats at least three times a day. She
is not picky with food. Her meal normally includes fish, pork, and vegetables. She is a
normal beverage drinker.
BMI = lbs. / inch 2 X 703 .
BMI = 130 lbs. / 61.81 inches2 x 703
= 130 lbs. / 3820.5 inches x 703
= 23. 92 (NORMAL)
Underweight Below 18.5
Normal 18.5 – 24.9
Overweight 25 – 29.9
Obese Above 30
13 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
Body Temperature
DATE TIME BODY
TEMPERATURE
(ºC)
Jan. 31, 2012 8:00 AM 37. 1 ºC
12: 00 PM 37.3 ºC
Feb. 1, 2012 8:00 AM 36. 2 ºC
12:00 PM 36.6ºC
Respiratory Status
DATE TIME RESPIRATORY RATE
(cpm)
Jan. 31, 2012 8:00 AM 21 cpm
12:00 PM 18 cpm
Feb. 1, 2012 8:00 AM 19 cpm
12:00 PM 17 cpm
Circulatory Status
14 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
DATE TIME BLOOD PRESSURE
(mmHg)
Jan. 31, 2012 8:00 AM 120/80 mmHg
12:00 PM 120/80 mmHg
Feb. 1, 2012 8:00 AM 120/80 mmHg
12:00 PM 120/80 mmHg
Elimination Pattern
DATE URINE STOOL
Jan. 31, 2012 3 1
Feb. 1, 2012 2 0
Reproductive Status
Mrs. E.M’s first menstrual period was when she was 10 years old. She got married at
the age of 24 years old. She has 3 children (2 girls/1 boy) with 2 years gap each. She is
sexually active.
Sleep Pattern
Mrs. E.M. stated that she normally sleeps 4-6 hours/day, after she was admitted she
has some difficulty in sleeping because of the nurses coming in and out of her room and
sometimes she has difficulty of breathing. She usually watches television at home during rest
hours and also during admission.
15 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
State of Skin and Appendages
Mrs. E.M. has fair skin. Her wavy hair is up to her shoulders. Her lips are not dried
and slightly brownish in color. Nails are trimmed.
VII. THEORETICAL FRAMEWORK
16 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
FLORENCE NIGHTINGALE: Environmental Theory
Florence Nightingale (1820-1910), considered the founder of educated and scientific
and widely known as "The Lady with the Lamp" wrote the first nursing notes that became the
basis of nursing practice and research. The notes, entitled Notes on Nursing: What it is, what
is not (1860), listed some of her theories that have served as foundations of nursing practice
in various settings, including the succeeding and in the field of Nursing. Nightingale is
considered the first nursing theorist. One of her theories was the Environmental Theory,
which incorporated the restoration of the usual health status of the nurse's clients into the
delivery of it is still practiced today.
Nightingale's theory was show to be applicable during the Crimean war along with
other nurses she had trained, took care of injured soldiers by attending to their immediate
needs, when communicable disease and rapid spread of disease were rampant in this early
period in the development of disease-capable medicines. The practice of environment
configuration according to patient's health or disease condition is still applied today, in such
cases as patients infected with suffering from who need minimal noise to calm them and a
quiet environment to prevent seizure-causing stimulus.
In environmental effects she stated in her nursing notes that nursing "is an act of
utilizing the environment of the patient to assist him in his recovery" (Nightingale
1860/1969) that it involves the nurse's initiative to configure environmental settings
appropriate for the gradual restoration of the patient's health, and that external factors
17 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
associated with the patient's surroundings affect life or biologic and physiologic processes,
and his development.
Major Concepts and Definitions
Environment - concepts of ventilation, warmth, light, diet, cleanliness and noise. She focus
o the physical aspect of environment.
She believed that "Healthy surroundings were necessary for proper nursing care."
5 essential components of healthy environment:
1. Pure air
2. Pure water
3. Efficient drainage
4. Cleanliness
5. Light
Concerns of Environmental Theory
1. Proper ventilation focus on the architectural aspect of the hospital.
2. Light has quite as real and tangible effects to the body. Her nursing intervention includes
direct exposure to sunlight.
3. Cleanliness and sanitation. She assumes that dirty environment was the source of infection
and rejected the "germ theory". Her nursing interventions focus on proper handling and
18 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
disposal of bodily secretions and sewage, frequent bathing for patients and nurses, clean
clothing and hand washing.
4. Warmth, quiet and diet environment. She introduces the manipulation of the environment
for patient's adaptation such as fire, opening the windows and repositioning the room
seasonally, etc.
5. Unnecessary noise is not healthy for recuperating patients.
6. Dietary intake.
7. Petty management proposed the avoidance of psychological harm, no upsetting news.
Strictly war issues and concerns should not be discussed inside the hospital. She includes the
use of small pets of psychological therapy.
Nursing Metaparadigm
Nursing
Nursing is very essential for everybody's well-being. Notes on nursing focus on the
implementation and rendering efficient and effective nursing care.
Person
The patient is the focus of the environmental theory. The nurse should perform the task for
the patient and control environment for easy recovery. She practices nurse-patient passive
relationship.
19 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
Health
Health is the being well and using every power that the person has to the fullest extent. A
healthy body can recuperate and undergo reparative process. Environmental control uplifts
maintenance of health.
Environment
People would benefit from the environment.
Importance of Environmental Theory
Practice
1. Disease control
2. Sanitation and water treatment
3. Utilized by modern architecture in the prevention of "sick building syndrome" applying
the principles of ventilation and good lighting.
4. Waste disposal
5. Control of room temperature.
6. Noise management.
Education
1. Principles of nursing training. Better practice result from better education.
2. Skills measurement through licensing by the use of testing methods, the case studies.
20 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
Research
1. Use of graphical representations like the polar diagrams.
2. Notes on nursing.
The Analysis
Simplicity: The theory is simply explained as the nurse, patient and environment interacts
with each other. There are dangers in the environment and benefits from the good
environment. The roles of environmental management to patient recovery are greatly
emphasized. Manipulating the environment to prevent diseases. Nurse-patient relationship
focuses on cooperation and collaboration. Her care focus on eating patterns and food
preferences of the patients, provision of comfort, protection from emotional distress and
conservation of energy.
Generality: The universality of the concepts provides general guidelines and is still
applicable and relevant today.
VIII. ANATOMY AND PHYSIOLOGY
21 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
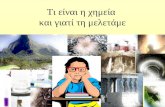
The Human Respiratory SystemThe Pathway
Air enters the nostrils
passes through the nasopharynx,
the oral pharynx
through the glottis
into the trachea
into the right and left bronchi, which branches and rebranches into
bronchioles, each of which terminates in a cluster of alveoli
22 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
Only in the alveoli does actual gas exchange takes place. There are some 300
million alveoli in two adult lungs. These provide a surface area of some 160
m2 (almost equal to the singles area of a tennis court and 80 times the area of our
skin!).
Breathing
In mammals, the diaphragm divides the body cavity into the
abdominal cavity, which contains the viscera (e.g., stomach and intestines)
and the
Thoracic cavity, which contains the heart and lungs.
The inner surface of the thoracic cavity and the outer surface of the lungs are
lined with pleural membranes which adhere to each other. If air is introduced
between them, the adhesion is broken and the natural elasticity of the lung causes
it to collapse. This can occur from trauma. And it is sometimes induced
deliberately to allow the lung to rest. In either case, reinflation occurs as the air is
gradually absorbed by the tissues.
Because of this adhesion, any action that increases the volume of the thoracic
cavity causes the lungs to expand, drawing air into them.
During inspiration (inhaling),
o The external intercostal muscles contract, lifting the ribs up and out.
23 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
o The diaphragm contracts, drawing it down.
During expiration (exhaling), these processes are reversed and the natural
elasticity of the lungs returns them to their normal volume. At rest, we
breathe 15–18 times a minute exchanging about 500 ml of air.
In more vigorous expiration,
o The internal intercostal muscles draw the ribs down and inward
o The wall of the abdomen contracts pushing the stomach and liver
upward.
Under these conditions, an average adult male can flush his lungs with
about 4 liters of air at each breath. This is called the vital capacity. Even with
maximum expiration, about 1200 ml of residual air remain.
The table shows what happens to the composition of air when it reaches the
alveoli. Some of the oxygen dissolves in the film of moisture covering the
epithelium of the alveoli. From here it diffuses into the blood in a nearby capillary.
It enters a red blood cell and combines with the hemoglobin therein.
At the same time, some of the carbon dioxide in the blood diffuses into the
alveoli from which it can be exhaled.
24 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
Composition of atmospheric air and expired air in a typical subject.
Note that only a fraction of the oxygen inhaled is taken up by the lungs.
Component Atmospheric Air (%) Expired Air (%)
N2 (plus inert gases) 78.62 74.9
O2 20.85 15.3
CO2 0.03 3.6
H2O 0.5 6.2
100.0% 100.0%
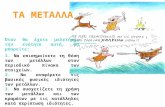
The ease with which oxygen and carbon
dioxide can pass between air and blood is clear
from this electron micrograph of two alveoli (Air)
and an adjacent capillary from the lung of a
laboratory mouse. Note the thinness of the
epithelial cells (EP) that line the alveoli and
capillary (except where the nucleus is located). At
the closest point, the surface of the red blood cell is
only 0.7 µm away from the air in the alveolus.
(Reproduced with permission from Keith R. Porter and Mary A. Bonneville, An
Introduction to the Fine Structure of Cells and Tissues, 4th. ed., Lea & Febiger,
1973.)
Central Control of Breathing
The rate of cellular respiration (and hence oxygen consumption and carbon
dioxide production) varies with level of activity. Vigorous exercise can increase by
25 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
20–25 times the demand of the tissues for oxygen. This is met by increasing the
rate and depth of breathing.
It is a rising concentration of carbon dioxide — not a declining
concentration of oxygen — that plays the major role in regulating the ventilation
of the lungs. Certain cells in the medulla oblongata are very sensitive to a drop
in pH. As the CO2 content of the blood rises above normal levels, the pH drops
[CO2 + H2O → HCO3− + H+],
and the medulla oblongata responds by increasing the number and rate of nerve
impulses that control the action of the intercostal muscles and diaphragm. This
produces an increase in the rate of lung ventilation, which quickly brings the
CO2 concentration of the alveolar air, and then of the blood, back to normal levels.
However, the carotid body in the carotid arteries does have receptors that
respond to a drop in oxygen. Their activation is important in situations (e.g., at
high altitude in the unpressurized cabin of an aircraft) where oxygen supply is
inadequate but there has been no increase in the production of CO2.
Local Control of Breathing
The smooth muscle in the walls of the bronchioles is very sensitive to the
concentration of carbon dioxide. A rising level of CO2 causes the bronchioles to
dilate. This lowers the resistance in the airways and thus increases the flow of air
in and out.
26 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
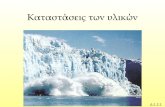
IX. PATHOPHYSIOLOGY
Bronchial Asthma In Acute Exacerbation
27 | P a g e
PREDISPOSING FACTORS
-Gender
-Age
-Family History
-Race
PRECIPITATING FACTORS
-Viral Respiratory Infections
-Allergen exposure (animal dander, dust, pollen, etc.)
-change in Weather
-Exercise
-Smoke ( fr. Vehichles, smokers ect.)
Release of eosinophils (to combat allergen)
Prostaglandins Histamine, Bradykinin, and other inflammatory mediators
Exposure to different pathogens
Entry of allergens
Release of Immunoglobulin E (IgE)
Release of different chemical mediators
Mast cell degranuation
Release of the different inflammatory chemical mediators
Leukotrienes
Opening of the mucosal Intracellular junction

CASE STUDY: Bronchial Asthma In Acute Exacerbation
F
28 | P a g e
Mucus Hypersecretion
Fatigue, Anxiety
Inflammatory Process
Mucus Production Increase Vascular Permeability
Direct stimulation of vagal efferents
Mucosal EdemaBronchoconstriction
Further edma
More release of other inflammatory
mediatorsEpithelial damage
Decrease Ciliary Function
Increase airway responsiveness
Wheezing, continuous coughing, feelings of chest tightness
Dyspnea, moist skin, tachypnea

CASE STUDY: Bronchial Asthma In Acute Exacerbation
PATHOPHYSIOLOGY
The bronchi and bronchioles are very responsive to irritants, leading to contraction of
the smooth muscles (bronchoconstriction), inflammation with edema (swelling), and
increased secretion of thick mucous. These changes can block the airways, totally or
partially, interfere with the air flow and oxygen supply. In extrinsic asthma, the allergic
reaction causes release of chemical mediators like histamine that causes the bronchospasms,
edema and increased mucous secretion. This reaction also stimulates tha vagus nerve,
causing a reflex bronchoconstriction. The second stage of the allergic reaction occurs a few
hours later. During this stage, the increased leukocytes (white blood cells) released additional
chemical mediators that cause tissue damage. Left untreated, frequented and prolonged attack
can lead to chronic asthma later in life. The mechanisms behind intrinsic attacks are not fully
understood.
Partial obstruction of the smaller airways results in air trapping with hyperinflation of
the lungs. Air passes into the areas distal to the obstruction (alveoli), but are only partially
exhaled. Since exhalation is a passive process, less force is available to move air out, and
forced expiration often collapses the bronchial wall, creating a further barrier to exhalation.
The residual volume (air left in the lungs after exhalation) increases and as a result. It
becomes harder to inhale fresh air or to cough to effectively remove the mucous. To better
understand the air trapping, try this experiment. Take several breaths and exhale only
partially before inhaling again. After a few breaths you will see how hard it is to inhale, or to
cough. This is what an asthma attack feels like.
29 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
Total obstruction of the airway results when mucous plugs completely block the
airflow in an already narrowed passage. This leads to atelectasis (collapse of the alveoli). The
air left in the alveoli diffuses out and is not replaced. This could lead to collapse of the lung.
Both a partial and total obstruction will lead to hypoxia. Oxygen levels are further depleted
by the increase demand by the muscles of respiration and by the stress of the individual
fighting for air. Hypoxemia causes vasoconstriction if the pulmonary blood vessels, slowing
blood flow and increasing the workload of the right side of the heart.
With repeated acute asthma attacks, irreversible damage occurs in the lungs. The
bronchial walls become thickened, and fibrous tissue resulting from the frequent infections
that follow attacks develops in atelectic areas. Because it is impossible to remove all of the
tiny mucous plugs in the small airways, complications are common following frequent
episodes of asthma.
30 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
X. NURSING MANAGEMENT
A. Laboratory Test
URINALYSIS
(January 27, 2012)
NORMAL RANGE
RESULT INTERPRETATION
Physical exam
Color Pale yellow to amber
yellow Normal
characteristic Clear to slightly hazy slightly turbid Normal
Chemical exam
Specific gravity 1.003 - 1.040 1.010 Normal
Protein Negative negative Normal
Sugar negative negative Normal
Microscopic exam
RBC 4 /HPF 4-6/HPF Normal
Pus cells 2 to 3 HPF 0-2/ HPF normal
31 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
HEMATOLOGY REPORT
(January 28, 2012)
REFERENCE
VALUE
RESULT INTERPRETATION
WBC Count 5 – 10 10^3/uL 8.7 Normal
Lymphocytes 0.25 – 0.50 0.22 Decreased.
RBC Count 3.80 – 5.8 10^6u/L 4.18 Normal
Hemoglobin 115.00-160.00 g/dL 132 Normal
Hematocrit 0.37 – 0.47 % .41% Normal
B. Nursing Care Plan
32 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
C. Drug Study
Name of Drug Action Indication/ContraindicationNursing Considerations and
Responsibilities
Levopront 15ml /
TID
The medication with drug
Levopront yet to materialize
Indicated with:
Symptomatic treatment of cough dry
unproductive cough with pharyngitis,
influenza, pneumonia, bronchial asthma,
emphysema lungs.
Contraindicated with:
hypersensitivity, the excess rate, expressed
violation of the liver
-Should be taken on an empty
stomach (Take between meals.)
-Instruct patient to increase oral
fluid intake
-instruct patient not to perform
tasks that require alertness
Name of Drug Action Indication/Contraindication Nursing Considerations and
33 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
Responsibilities
Nafarin A
1 Tab BID
The phenylpropanolamine HCl is a sympat
homimetic amine with achemical structure
and pharmacological actions similar to the
ephedrine, but with fewer central stimulant
effects. It is a vasoconstrictor with
decongestant action on the nose and upper
respiratory tract mucous membranes. It
directly and indirectly stimulates the a- and
b-adrenergic receptors. It exerts this last
action by allowing the norepinephrine
liberation (noradrenaline) from its storage
sites. Its action on the a-receptors in the
respiratory tract mucosa produces
vasoconstriction, which results in the
decrease of the mucosa edema and
the consequent increase of the nasal air
flow.
Indicated with:
Urinary incontinence, relive
symptoms of some allergic
disorders such as asthma and
have fever.
Contraindicated with:
Patients with high blood
pressure, over activity of the
thyroid gland, coronary heart
disease or diabetes, or who are
taking antidepressant drugs
-Administer the medication
with a full glass of water after a
meal or snack. The tablet can be
broken in half. However, the
whole or half tablet should be
swallowed whole.
-Assess for kidney disease,
heart disease, lung disease,
asthma, emphysema,
high blood pressure, an overa
ctive thyroid, diabetes, glaucom
a, prostatetrouble, depression,
any allergies of the patient.
-Caution patient not to exceed
recommended doses.
34 | P a g e

CASE STUDY: Bronchial Asthma In Acute Exacerbation
XI. DISCHARGE PLANNING/ PROGNOSIS
Medications:
Administer prescribed medications, such as bronchodilators, anti-inflammatory, and antibiotics
Give paracetamol if have fever
Exercise:
Patient will verbalize need importance of exercise and demonstrate proper initiation of appropriate exercise.
Advise the patient to exercise daily for good and healthy body.
Treatment:
Respiratory therapy
Combivent neb q6 T.I.D
Health Teaching:
Increase fluid intake Eat a balance healthy diet. Proper hygiene
Out – patient follow up:
Advised the patient to have a follow up check up based on the discharge plan of the doctor for him.
Diet:
It is recommended to eat hypoallergenic diet.
Spiritual:
Advise patient to pray so that God will help him in her daily life and bring forth more blessings.
35 | P a g e