Thyroid hormone effect and mechanism of action
37
Effects Of Thyroid Hormone and it’s Applied Physiology Dr Anwar H Siddiqui Senior Resident, Physiology
-
Upload
anwar-siddiqui -
Category
Health & Medicine
-
view
3.491 -
download
6
Transcript of Thyroid hormone effect and mechanism of action

Effects Of Thyroid
Hormone and it’s Applied
Physiology
Dr Anwar H SiddiquiSenior Resident, Physiology

Mechanism of Thyroid Hormone Action
O Acts by binding to a specific nuclear thyroid hormone receptor (TR).
O T3 has a 15-fold higher binding affinity for TRs than does T4.
O The hormone-receptor complex binds to DNA via zinc fingers and increases/decreases the expression of a variety of different genes that code for proteins that regulate cell function.
O In humans, there are two TR genes, α and β.O By alternative splicing, each forms at least
two different mRNAs and therefore two different receptor proteins.

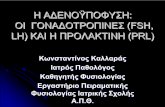
Schematic diagram of thyroid hormone mechanism of action.
The interaction of T3 with the TR that is bound as a heterodimer with retinoid X receptor (RXR) to the thyroid hormone response element (TRE), often in the 5′ flanking
region of a T3-responsive gene, causes either an increase or a decrease in the transcription of that gene.
coactivator proteins
corepressor proteins

O The active proteins are TRα1, TRβ1, TRβ2, and TRβ3.
O There are tissue-specific preferences in expression of the various TRs.O TRβ2 is found only in the brainO TRα, particularly TRα2, is thought to be
important in the hypothalamus and pituitary.O TRα1 is expressed in all tissues, although its
mRNA is especially highly expressed in the kidney, liver.
O TRβ3 mRNA is expressed at very low levels but is more abundant in the liver, kidneys, and lungs than in other tissues.

O Experiments with inactivation of TRα and TRβ have illuminated their different physiologic roles
O Feedback regulation of thyroid hormone effects and cochlear development are functions of TRβ.
O Cardiac function and energy metabolism are more likely to be regulated by TRα.
Resistance to thyroid hormone, a condition in which TRβ mutations markedly reduce the binding affinity of TRβ for T3. This binding defect produces a TRβ1 or TRβ2 protein that acts as a dominant negative inhibitor of the intact TRβ proteins encoded by the normal allele

Effects of Thyroid Hormone

Calorigenic ActionO T4 and T3 increase the O2 consumption of
almost all metabolically active tissues.O Some of the calorigenic effect of thyroid
hormones is due to metabolism of the fatty acids they mobilize.
O Thyroid hormones increase the activity of the membrane-bound Na, K ATPase in many tissues
O The resulting increased metabolic rate increases thermogenesis.
O Most of the effect of thyroid hormone are secondary to its calorigenic effects.

Effects Secondary to Calorigenesis
On Protein Metabolism
O Increase in metabolic rate by T4 and T3 in pharmacological dose increases N2 excretion; if food intake is not increased, endogenous protein and fat stores are catabolized and weight is lost.( Catabolic action)
O In small doses causes positive N2 balance and stimulate growth (Anabolic action).
O Excess catabolic effect along with marked creatinuria leads to muscle fatiguability (Thyrotoxic Myopathy)

O The potassium liberated during protein catabolism appears in the urine, and there is also an increase in urinary hexosamine and uric acid excretion
O Bone protein mobilization Osteoporosis, hypercalcemia and subsequent hypercalciuria.
O Hypothyroidism protein catabolism accumulation of osmotically active protein conjugates under skin/subcutaneous tissue coarse puffy skin (Myxoedema)

On vitaminsO Increased BMR increased use of
co-factors and vitamins Vitamin deficiency in hyperthyroid state.
O Thyroid hormone is necessary for hepatic conversion of β carotene to vitamin A.
O Decreased thyroid hormone increased accumulation of β carotene in blood (Carotenemia)
yellowish discoloration of skin.

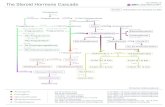
Typical appearance of patients with moderately severe primary hypothyroidism or myxedema.
Carotenemia versus
Jaundice

Lactation and GonadsO T4 is essential for maintenance of lactation.O Milk secretion is decreased in hypothyroidism
and stimulated by thyroid hormones.O Thyroid hormone is involved in gonadal
development and secondary sexual characteristics.
O In adult women, severe hypothyroidism may be associated with diminished libido and failure of ovulation.
O Secretion of progesterone is inadequate, and endometrial proliferation persists, resulting in excessive and irregular breakthrough menstrual bleeding.

O In hyperthyroidism menstrual flow is initially diminished and ultimately ceases reducing fertility.
O Likely mechanism for menstrual changes:O disruption in amplitude and frequency of
LH/FSH pulses caused by thyroid hormone influences on GnRH signaling..
O “spillover” of elevated TSH stimulating the luteinizing hormone (LH) receptor48 and elevated TRH initiating excess prolactin release.
O A significant fraction of men with hypothyroidism or hyperthyroidism have moderate to severe erectile dysfunction that improves with treatment of the thyroid disease

Effects on the Cardiovascular System

O Circulatory T3 enters the myocytes, combines with its receptors, and enters the nucleus, where it promotes the expression of some genes and inhibits the expression of others.
O Those that are enhanced include the genes for a -myosin heavy chain, sarcoplasmic reticulum Ca2+ ATPase, b-adrenergic receptors, G proteins, Na-K ATPase, and certain K+ channels.
O Those that are inhibited include the genes for b-myosin heavy chain, phospholamban, adenylyl cyclase, T3 nuclear receptors, and NCX, the Na+–Ca2+ exchanger.
O The net result is increased heart rate and force of contraction


O The myosin containing β-MHC has less ATPase activity than the myosin containing α -MHC.
O α -MHC predominates in the atria in adults, and its level is increased by treatment with thyroid hormone. This increases the speed of cardiac contraction.
O Conversely, expression of the α -MHC gene is depressed and that of the β -MHC gene is enhanced in hypothyroidism.

Effects on the Nervous SystemO Thyroid hormone is essential for the
development of the central nervous system.O T4 deficiency in fetus or in infants causes:
O Defective myelination of axons of cortical regionO Defective branching of dendrites leading to
defective synapsesO Marked reduction in vascularity of brainNet Result Infantile brain/mental retardation
O Thyroid hormone therapy must be given to a thyroid hormone-deficient child during the first few months of postnatal life to prevent mental retardation.(critical period- 1 year of life)

O The parts of the central nervous system (CNS) most affected are the cerebral cortex, the basal ganglia and the cochlea .(mental retardation, motor rigidity, and deafness).
O T4 deficiency in adults cause:O Loss of all intellectual functionO Memory lossO Decrease electrical activity of brainO Slow, delayed and husky voiceO Eventually Psychosis (Myxoedema
Madness)O T4 excess increases response to
catecholamines and stimulation of RAS anxiety, nervousness, irritability, insomnia , rythmic tremors etc

Effects on growth and development
O Thyroid hormone is essential for normal growth and maturation of the skeleton.
O Growth failure in thyroid deficiency is caused by impaired general protein synthesis, reduced growth hormone, and especially reduced insulin-like growth factor 1.
O A major way thyroid hormones promote normal body growth is by stimulating the expression of the gene for growth hormone (GH) in the somatotrophs of the anterior pituitary gland.

O Impairment of linear growth leads to dwarfism (cretinism) in which the limbs are disproportionately short in relation to the trunk but cartilage growth is unaffected.
O Children with prolonged hypothyroidism, even after adequate treatment, do not reach predicted height
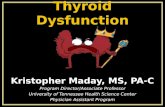
The consequences of untreated congenital hypothyroidism aredemonstrated in this 17-year-
old girl. Her tongue is enlarged, and
her extremities are inappropriately short in
relation to her trunk.

Effect on carbohydrate metabolism
O Dual and opposite effectsO Increases peripheral utilization of glucose
can cause hypoglycemiaO Can also cause hyperglycemia by :
O Increase absorption from GI tractO Increase glycogenolysis in the liverO Increase gluconeogenesis from pyruvateO Increase breakdown of insulinO Decrese secretion of insulin
O In hyperthyroidism, therefore, the plasma glucose level rises rapidly after a carbohydrate meal, sometimes exceeding the renal threshold.

Effects on lipid metabolismO Thyroid hormones lower circulating cholesterol
levels.O The decrease in plasma cholesterol
concentration is due to increased formation of low-density lipoprotein (LDL) receptors in the liver, resulting in increased hepatic removal of cholesterol from the circulation.
O Thyroid decreases the stores of triglycerides and phospholipids by increasing the activity of lipases i.e increasing lipolysis
O Dextro –thyroxine (D-T4) and TETRAC are used clinically as serum cholestrol lowering agents in atherosclerosis

Effects on Hematopoietic System
O T4 deficiency leads to anaemia due to:O In response to the diminished oxygen requirements
and decreased production of erythropoietin causing mild normocytic, normochromic anemia.
O Decreased absorption ov vitamin B12,Folate deficiency from malabsorption or dietary inadequacy may cause macrocytic anemia.
O The frequent menorrhagia and the defective absorption of iron resulting from achlorhydria may contribute to a microcytic, hypochromic anemia.
O T4 excess stimulates erythropoiesis,increase production of 2,3 DPG in RBC shifting O2 dissociation curve to right.
O A parallel increase in plasma volume also occurs, with the result that the hematocrit is normal.

Relation to CatecholaminesO The actions of thyroid hormones and the
catecholamines norepinephrine and epinephrine are intimately interrelated.
O The functional synergism observed between catecholamines and thyroid hormones,arises from the ability of thyroid hormones to increase expression of catecholamine receptors and the signaling effectors to which they are linked.
O The reduced adrenergic responsiveness associated with hypothyroidism has been linked to all steps of catecholamine signaling, including receptor and postreceptor actions, resulting in an impaired cAMP response.

Catecholamines T4
• Epinephrine and nor epinephrine increases BMR,stimulates CNS,increases heart rate and force of contraction
• T4 also has the same action but is prolonged and slow
• Cannot increase BMR in absence of T4
• T4 potentiate the action of catecholamine and in their presence increase in BMR by T4 is more
• Cause stimulation of Reticular Activating System
• Same effect but : T4 action on CNS and CVS can be decreased after sympathectomy or by β blockers

Applied Aspects

HypothyroidismO Reduced circulating levels of free T4 and T3.O The syndrome of adult hypothyroidism is
generally called myxedema.O Children who are hypothyroid from birth or
before are called cretins. O Hypothyroidism may be the end result of a
number of diseases of the thyroid gland, or it may be secondary to pituitary or hypothalamic failure.
O Treatment is almost always with levothyroxine

Causes of Hypothyroidism
Primary Hypothyroidism
Acquired• Hashimoto’s thyroiditis• Iodine deficiency (endemic goiter)• Drugs blocking synthesis or release of T4 (e.g., lithium, ethionamide, sulfonamides, iodide)• Goitrogens in foodstuffs or as endemic substances or pollutants• Cytokines (interferon-γ, interleukin-2)• Thyroid infiltration (amyloidosis, hemochromatosis, sarcoidosis, • Postablative thyroiditis due to 131I surgery or therapeutic irradiation for nonthyroidal malignancyCongenital• Maternal iodine deficiency • Fetal thyroid dysgenesis • Inborn errors of thyroid hormone synthesis • Maternal antithyroid antibodies that cross the placenta • Fetal hypopituitary hypothyroidism
Transient (Post-Thyroiditis) HypothyroidismFollowing subacute, painless, or postpartum thyroiditis
Consumptive HypothyroidismRapid destruction of thyroid hormone due to D3 expression in large hemangiomas or hemangioendotheliomas
Defects of Thyroxine-to-Triiodothyronine ConversionSelenocysteine insertion sequence–binding protein 2 (SBP2) defect
Drug-Induced Thyroid DestructionTyrosine kinase inhibitor (e.g., sunitinib)
Central HypothyroidismAcquiredPituitary origin (secondary) Hypothalamic disorders (tertiary)Bexarotene (retinoid X receptor agonist) Dopamine and/or severe illnessCongenital TSH deficiency or structural abnormalityTSH receptor defect
Resistance to Thyroid Hormone

Signs and Symptoms of Adult Hypothyroidism
Tiredness
Forgetfulness/Slower Thinking
Moodiness/ Irritability
Depression
Inability to Concentrate
Thinning Hair/Hair Loss
Loss of Body Hair
Dry, Patchy Skin
Weight Gain
Cold Intolerance
Elevated Cholesterol
Family History of Thyroid Disease or
Diabetes
Muscle Weakness/
Cramps
Constipation
Infertility
Menstrual Irregularities/
Heavy Period
Slower Heartbeat
Difficulty Swallowing
Persistent Dry or Sore Throat
Hoarseness/
Deepening of Voice
Enlarged Thyroid (Goiter)
Puffy Eyes

Various manifestations of Hypothyroidism

HyperthyroidismO It is the condition resulting from increased
circulating levels of free T4 and T3.O The term thyrotoxicosis, rather than
hyperthyroidism, should be used for this disorder because it need not be associated with hyperfunction of the thyroid gland. The term hyperthyroidism is reserved for disorders that result from sustained overproduction and release of hormone by the thyroid itself.
O It has various causes,the most common cause is Graves disease (Graves hyperthyroidism), which accounts for 60–80% of the cases

Causes of Hyperthyroidism
Sustained Hormone Overproduction (Hyperthyroidism)Graves’ disease (von Basedow’s disease)Toxic multinodular goiterToxic adenomaChorionic gonadotropin-induced Gestational hyperthyroidismPhysiologic hyperthyroidism of pregnancyFamilial gestational hyperthyroidism due to TSH receptor mutationsTrophoblastic tumorsAmiodarone-associated hyperthyroidism due to iodide releaseMetastatic functioning thyroid carcinomaTSH-secreting pituitary tumorsThyroid hormone resistance with pituitary predominance
Transient Hormone Excess (Thyrotoxicosis)ThyroiditisAutoimmuneLymphocytic thyroiditis (silent thyroiditis, painless thyroiditis,postpartum thyroiditis)Acute exacerbation of Hashimoto’s diseaseViral or postviralSubacute (granulomatous, painful, postviral) thyroiditisDrug-induced or associated thyroiditis (Amiodarone,Lithium, interferon-α, interleukin-2, GM-CSF)Infectious thyroiditisExogenous Thyroid HormoneIatrogenic overreplacementIngestion of natural products containing thyroid hormoneNatural foodstuffsThyromimetic compounds (e.g., tiratricol PLB)Occupational exposure to thyroid hormone (e.g., pill manufacturing,veterinary occupations

Nervousness/Tremor
Mental Disturbances/ Irritability
Difficulty Sleeping
Bulging Eyes/
Unblinking Stare/ Vision Changes
Enlarged Thyroid (Goiter)
Menstrual Irregularities/
Light Period
Frequent Bowel Movements
Warm, Moist Palms
First-Trimester Miscarriage/
Excessive Vomiting in Pregnancy
Persistent Dry or Sore Throat
Difficulty Swallowing
Palpitations/
Tachycardia
Impaired Fertility
Weight Loss or Gain
Heat Intolerance
Increased Sweating
Family History of
Thyroid Disease
or Diabetes
Sudden Paralysis
Hoarseness/
Deepening of Voice
Signs and Symptoms of Hyperthyroidism

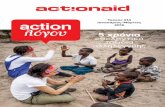
Computed tomographic scans of orbits in two patients with Graves’ orbitopathy.
Rare thyroid acropachy in a patient with Graves’disease.The hypermetabolic state leads to axial bone destruction

Test Hypothyroidism Hyperthyroidism
A. Based on metabolic Function
• BMR (Normal: ±10%) Decreases to – 30% to -40% Increases from +10% to +100%
• S.Creatinine (0.2 to 0.6 mg/dl) decreases increases
• Fasting blood sugar decreases increases
• S.Cholestrol (120-200mg/dl) increases decreases
B. Based on handling of Iodine• Total
S.T4(3-8µg/dl):S.T3( 0.15µg/dl)decreases increases
• Free S.T4(2ng/dl); S.T3(0.3ng/dl) decreases increases
• Protein bound Iodine (3.5-7.5µg/dl)
decreases increases
• RAI123 uptake (normal: 20-40%) decreases <20% Increases>60%
• Serum TSH level (normal 2.3 µU/ml)
• Primary hypothyroidism- decreases
• Secondary hypothyroidism- decreases
Decreases or undetectable
C.Urine Calcium Loss(normal 100mg/day
decreases increases
Thyro id Func t ion Test Compared

Thank You…………..