The Effect of Polymorphysm of The β-2 Adrenergic Receptor...
5
8 ORIGINAL ARTICLE ABSTRACT Aim: to discover the role of β2-adrenergic receptor (β2-AR) polymorphism on the response to beta-2 agonist, particularly in coding amino acid at sequences 16 and 27 as well as adjacent nucleotides. Methods: the study was conducted by nested case- control method with consecutive samples of asthma patients aged 15-60 years at the outpatient clinic, Department of Pulmonolgy in Dr. Wahidin Sudirohusodo General Hospital, Makassar. Twenty-eight patients were found irresponsive to terbutaline nebulation (increased FEV1 < 15%) and 56 patients were responsive (increased FEV1 > 15%). DNA extraction and amplication were performed by PCR as well as polymorphism detection, which was done by automatic sequencing machine. Results: the Arg 16 polymorphism did not have any effect on the response to terbutaline nebulation, but Gln 27 polymorphism did with OR 3.18. New polymorphism was found in nucleotide at 20 th order before the start codon, it was T/C –20, which also has an effect on the response to terbutaline nebulation with OR 4.53. When the three polymorphisms were combined, the effect were greater with OR 11.11. It was found that age, gender, obesity, onset and ethnicity had no effect on the response to terbutaline nebulation. Conclusion: polymorphism of the novel Gln 27 and T/C –20 (newly known) have an effect on the response to beta-2 agonist. Both combination and polymorphism of Arg 16 will bring greater effect on the response to beta-2 agonist. Key words: polymorphism, beta-2 agonist, beta-2 receptor. INTRODUCTION Asthma is defined as a chronic inflammatory disease of airways that is characterized by increased responsiveness of the tracheobronchial tree to a multiplicity of stimuli. It is manifested physiologically by a widespread narrowing of the air passages, which may be relieved spontaneously or as a result of therapy, and clinically by paroxysms of dyspnea. 1 The prevalence The Effect of Polymorphysm of The β-2 Adrenergic Receptor on The Response to β-2 Agonist in Bronchial Asthma Patients Syamsu, Irawan Yusuf, Budu, Ilhamjaya Patellongi Research Center of Hasanuddin University, Makassar of asthma in the general population is increasing and the economic costs of this disorder, i.e. morbidity, health care expenses, lost productivity and even mortality, are staggering. 2 The β2-adrenergic agonists are the most potent bronchodilators presently currently available for asthma treatment. Genetic factors controlling β2-adrenergic receptor ( β2-AR) function may be very important determinant of response to bronchodilator therapy and thus of severity and duration of asthmatic symptoms. 3 Polymorphisms of β2-AR can affect receptor regula- tion. Smaller studies examining the effects of such polymorphisms on the response to β2-agonist therapy have produced inconsistent results. 4 Over past several years, there has been considerable controversy about the role of inhaled β2-agonist in the asthma treatment. Studies using mutagenesis and recombinant expression in cells and transgenic mice as well as using airway smooth muscle cell, which are endogenously expressing these β2-AR variant, have shown that some forms of the β2-AR demonstrate distinct differences in signaling and/or regulation after exposure to β2-agonist. Study by Israel et al suggested that these polymorphisms may be associated with various asthma severity. 4 Furthermore, other studies have reported a relationship between these polymorphism and the degree of responsiveness or desensitization to the bronchodilator effect of β2- agonist. 5 In vitro studies have shown that common variant (polymorphisms) of the β 2-adrenoceptor involves amino-acid substitution at positions (codons) 16 and 27 of the receptor sequences resulting in conforma- tional changes that determine down regulation and desen- sitization in response to agonist stimulation. 6 Data of randomized, controlled trials have indicated that regular use of β2-agonist will cause tolerance in bronchodilat- ing and nonbronchodilating effect, increased airway inflammation, and increased asthma exacerbations. Tachyphylaxis against benecial effect of β2-agonist may contribute to correlation between these agents’, utilization and increased asthma mortality rates. 7,8
Transcript of The Effect of Polymorphysm of The β-2 Adrenergic Receptor...

8
ORIGINAL ARTICLE
ABSTRACTAim: to discover the role of β2-adrenergic receptor
(β2-AR) polymorphism on the response to beta-2 agonist, particularly in coding amino acid at sequences 16 and 27 as well as adjacent nucleotides.
Methods: the study was conducted by nested case-control method with consecutive samples of asthma patients aged 15-60 years at the outpatient clinic, Department of Pulmonolgy in Dr. Wahidin Sudirohusodo General Hospital, Makassar. Twenty-eight patients were found irresponsive to terbutaline nebulation (increased FEV1 < 15%) and 56 patients were responsive (increased FEV1 > 15%). DNA extraction and amplication were performed by PCR as well as polymorphism detection, which was done by automatic sequencing machine.
Results: the Arg 16 polymorphism did not have any effect on the response to terbutaline nebulation, but Gln 27 polymorphism did with OR 3.18. New polymorphism was found in nucleotide at 20th order before the start codon, it was T/C –20, which also has an effect on the response to terbutaline nebulation with OR 4.53. When the three polymorphisms were combined, the effect were greater with OR 11.11. It was found that age, gender, obesity, onset and ethnicity had no effect on the response to terbutaline nebulation.
Conclusion: polymorphism of the novel Gln 27 and T/C –20 (newly known) have an effect on the response to beta-2 agonist. Both combination and polymorphism of Arg 16 will bring greater effect on the response to beta-2 agonist.
Key words: polymorphism, beta-2 agonist, beta-2 receptor.
INTRODUCTIONAsthma is defined as a chronic inflammatory
disease of airways that is characterized by increased responsiveness of the tracheobronchial tree to a multiplicity of stimuli. It is manifested physiologically by a widespread narrowing of the air passages, which may be relieved spontaneously or as a result of therapy, and clinically by paroxysms of dyspnea.1 The prevalence
The Effect of Polymorphysm of The β-2 Adrenergic Receptor on The Response to β-2 Agonist in Bronchial Asthma PatientsSyamsu, Irawan Yusuf, Budu, Ilhamjaya Patellongi
Research Center of Hasanuddin University, Makassar
of asthma in the general population is increasing and the economic costs of this disorder, i.e. morbidity, health care expenses, lost productivity and even mortality, are staggering.2
The β2-adrenergic agonists are the most potent bronchodilators presently currently available for asthma treatment. Genetic factors controlling β2-adrenergic receptor (β2-AR) function may be very important determinant of response to bronchodilator therapy and thus of severity and duration of asthmatic symptoms.3 Polymorphisms of β2-AR can affect receptor regula-tion. Smaller studies examining the effects of such polymorphisms on the response to β2-agonist therapy have produced inconsistent results.4 Over past several years, there has been considerable controversy about the role of inhaled β2-agonist in the asthma treatment. Studies using mutagenesis and recombinant expression in cells and transgenic mice as well as using airway smooth muscle cell, which are endogenously expressing these β2-AR variant, have shown that some forms of the β2-AR demonstrate distinct differences in signaling and/or regulation after exposure to β2-agonist. Study by Israel et al suggested that these polymorphisms may be associated with various asthma severity.4 Furthermore, other studies have reported a relationship between these polymorphism and the degree of responsiveness or desensitization to the bronchodilator effect of β2-agonist.5 In vitro studies have shown that common variant (polymorphisms) of the β2-adrenoceptor involves amino-acid substitution at positions (codons) 16 and 27 of the receptor sequences resulting in conforma-tional changes that determine down regulation and desen-sitization in response to agonist stimulation.6 Data of randomized, controlled trials have indicated that regular use of β2-agonist will cause tolerance in bronchodilat-ing and nonbronchodilating effect, increased airway inflammation, and increased asthma exacerbations. Tachyphylaxis against benecial effect of β2-agonist may contribute to correlation between these agents’, utilization and increased asthma mortality rates.7,8

9
Vol 39 • Number 1 • January - March 2007 The Effect of Polymorphysm of The β-2 Adrenergic Receptor
Based on several studies, the effectiveness of β2-agonist is highly varied and it is reported to be related to increased asthma mortality rate. Such study has not been available yet in Indonesia, therefore we are interested in conducting the study.
The objective of this study is to discover the effect of polymorphism of β2-AR on the response to β2-agonist, especially the coder of amino acid at sequences 16 and 27 as well as nucleotide around it.
METHODSThe study was done with nested case controls
design and consecutive samples of asthma patients aged 15-60 years at the outpatient clinic, Department of Pulmonology in Dr. Wahidin Sudirohusodo General Hospital, Makassar. Subjects were stable asthma patients who were not in exacerbation state, did not have other concomitant diseases that might affect lung function, not in pregnancy, not smoking, and had no signs of thyrotoxicosis, gastroesophageal reux or aspergillosis. Patients were instructed to stop any utilization of systemic bronchodilator, corticosteroid and antihistamine 72 hours before bronchodilator test. Long acting beta-2 agonist inhalation was stopped 24 hours and short acting beta-2 agonist was stopped 12 hours before the test.
Specically, they were asked about their experiences of asthma episodes or wheezing including age of onset, frequency and severity of asthma attack, hospitalization, medication and complication, as well as family history of asthma or other atopic diseases. They were also asked about their asthma episodes occurring in previous months. Skin prick test against eight aeroallergens (D.pteronyssinus, D.farinae, Alternaria, cat fur, dog hair, cockroach, Candida albicans, latex) were performed during bronchodilator test. Subjects were considered as atopic patients when they had at least one positive skin test result, i.e. equal or larger wheal size compared to the control positive (histamine). In order to exclude another disease, we performed detailed history taking, systematic physical examination, chest x-ray, and electrocardiography.
Bronchodilator Responsiveness. To assess response to a bronchodilator, one respule terbutaline (0,5 mg) was administered using ultrasonic nebulizer Acoma N-15 Japan and measurement of lung function was performed before and 15 minutes after terbutaline nebulation by electronic spirometer H1 298, Chest Corporation Japan. We used the best of three spirometer-values and response to terbutaline was expressed as:
For the polymorphism of β2-AR 16 we used a primer.5’-CGCCTTCTTGCTGGCACCCAAT-3’ (sense)
5’-CCAACTACTTCATCACTTCACTGG-3’(anti-sense)
For the polymorphism of β2-AR 27 we used a primer.5’-GAATGAGGCTTCCAGGCGTC-3’ (sense)
5’-GGCCCATGACCAGATCAGCA-3’ (anti-sense)
We considered as responsive when the increasing of FEV1 was 15% or more and irresponsive when the increasing of FEV1 was less than 15%.
After a systematic selection, we found 86 patients. Twenty-eight patients were found irresponsive to terbutaline nebulation (the increase of FEV1 < 15%) and 58 patients were responsive to it (the increase of FEV1 > 15%). In order to simplify the analysis, two responsive patients were excluded randomly.
Molecular Methods. Genomic DNA was prepared from peripheral blood using standard techniques. Three milliliters of periphery blood was taken from cubital vein by venoject EDTA contained. This blood was collected and incubated at –200C xed temperature. After samples was enough, the blood was prepared for DNA extraction and amplication. The frozen blood was made liquid by incubating in 370C water-bathe. The extraction and amplication of DNA was done by PCR using Chelex-methods at Research Center of Hasanuddin University Makassar. Two hundred microliter of blood was add to 800 ul of saphonin solution and was incubated in 40C for 5 minutes. Then centrifuged at room temperature at 10.000 rpm for 10 minutes. We poured off the supernatant and add 500 ul PBS (for once). Centrifuged at room temperature of 4000 rpm for 5 minutes (for three times). We add Chelex solution 20% and dd-H2O 150 ul and heated in boiled water for 10 minutes then centrifuge at 10.000 rpm for 10 minutes. Put the supernatant into new tube as DNA material ready for amplication. For the amplication of DNA by PCR we used 2 pairs of primers (an upstream (5’) primer and a downstream (3’) primer.
The amplication procedures are as follows: for each sample in PCR tube add 100ug DNA genom in a PCR buffer (10 mM Tris HCl pH 8,3. 50 mM KCl, 1,5 MM MgCl 2 , 200 uM dNTP, 1.25 u enzyme DNA-poly-merase and 10 p mol primer pair). Sample in PCR tube is incubated in PCR machine at 940C for 2 minutes followed by 30 cycles of incubation at 940C for 30 seconds for denaturation of ds-DNA followed by annealing of primers to ssDNA template strands (for Arg-16 polymorphism by incubation at 550C for 30 seconds, for Gln-27 polymorphism by incubation at 600C for 30 seconds) and extension of nascent strands by DNA polymerase by incubation at 720C for one minute.
Postbronchodilator FEV1 – Prebronchodilator FEV1 x 100 % Prebronchodilator FEV1

10
Syamsu, et al Acta Med Indones-Indones J Intern Med
For detection of point polymorphism we used automatic sequencer machine ABI Prism USA. Start on purication of PCR product by Qiagen, sequencing reaction like in PCR amplication but only one direction (there are three major steps which are repeated for 30 cycles, denaturation at 960C for minutes, annealing at 500C for minutes and extention at 600C for minutes), after that the mixture of strands will be stained by dye blue dextran will be put into acrylamide gel electrophoresis and taken into sequencer machine, that will produce gel images. By computer program gel image is translated to electrophoregram and can be read by overlapping program.
was no difference in prevalence of polymorphism of β2-adrenoreceptor polymorphism between asthma and non-asthma subjects. However, the prevalence among ethnic groups was very variable.
In this study, we found 94% prevalence of Arg 16 polymorphism, 62% prevalence of Gln 27 polymorphism, and 62 % prevalence of the new T/C-20 polymorphism. From this study, we found that Arg-16 polymorphism had no effect on the response to beta-2 agonist; but the Gln-27 polymorphism did with Odds Ratio (OR) 3.18. New polymorphism was found in nucleotide at 20th order before the start codon, i.e. T/C-20 (Thymine changed by Cytosine), which also had an effect on the response to β2-agonist with OR 4.53. If these three polymorphisms are combined, the effect will be greater with OR 11.11. However, the polymorphism effect on asthma perpetua-tion was not found. (Table 2)
The responsiveness to terbutaline nebulation obviously also had association with pre-test-FEV1. However, it was statistically not signicant. Irresponsive patients indicated 41.5 % normal lung function (FEV1 > 80% predictive) and 19.4% abnormal lung function (FEV1 < 80% predictive). (Table 3).
DISCUSSIONThere are many reasons for evaluating the β2-AR
gene as a candidate gene in asthma. Clinical and labora-tory data show that β2-AR dysfunction is a hallmark of asthma. Previous genetic evaluation of β2-AR gene in patient with asthma identied several sequences that altered receptor activity.9 Mutation of Arg16 to Gly 16 leads to enhanced receptor down regulation, while mutation of Gln 27 to Glu 27 leads to a resistance to receptor down regulation. Previous attempts to correlate β2-AR polymorphism with the severity of asthma or responses to β2-agonist therapy have been inconclusive. Turki et al10 correlated the Gly 16 allele, which is associated with enhanced receptor down regulation with nocturnal asthma, and Martinez et al3 found that children who were homozygous for Arg 16 were more responsive to inhaled albuterol. The Gly 16 allele was found to be associated with steroid dependent11 and nocturnal asthma10 as well as with an increased degree of bronchodilator desensitization.5 An association of Gln 27 with elevated airway hyper-responsiveness and high level of total IgE among asthmatic have been described.12,13 In contrast, Lipworth et al6 demonstrated that the protection afforded by inhaled formoterol to subsequent metacholine challenge was not inuenced by the β2-AR genotype and Weir et al14 reported no polymorphism or haplotype was found
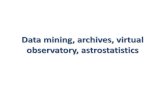
Figure 2. The base pair alteration T to C at -20 base-pair upstream from the initiation codon of RAB-2 gene
Statistical Analysis. Chi square test is used to analyze the association between nonparametric variable to other variables, such as age of onset, nutrition, atopic disease, gender, duration of asthma, pretest lung-function and bronchodilator responsiveness to terbutaline nebulation and perpetuation of asthma. Multivariate and logistic regression was used to adjust the effects of other variables on those of any given variable, such as the effect of genetic polymorphisms of β-AR, pretest-lung function, and atopic status on response to terbutaline nebulation and perpetuation of asthma. All data were analyzed by SPSS program.
RESULTSWe found no association of age, gender, obesity, age
of onset, and ethnicity and with response to terbutaline nebulation. (Table 1)
There was no relation between β2-adrenergic receptor polymorphism and asthma prevalence. There

11
Vol 39 • Number 1 • January - March 2007 The Effect of Polymorphysm of The β-2 Adrenergic Receptor

12
Syamsu, et al Acta Med Indones-Indones J Intern Med
to be associated with fatal/near-fatal asthma. Hancox et al15 reported that polymorphism of the β2-AR did not appear to determine the response to long-term inhaled β2-agonist treatment, and they did not nd relationship between the genotypes at either position 16 or 27 and any of the morning Peak Expiratory Flow Rate, diurnal variation in FEV1, additional bronchodilator use, bronchodilator response or asthma symptom scores.
In this study, we found no relationship between polymorphism of Arg 16 alone and the response to terbutaline nebulation. However, closed association with OR 4.53 can be found if it is combined with T/C-20 polymorphism. If it is also combined with Glu-27, the closed association increase with OR 11.11.
New polymorphism is found in nucleotide at 20th order, before the start codon (initiation codon) is T/C–20 (thymine changed by cytosine). Location of this polymorphism is known as a promoter region or up-stream base pairs. The nucleotide in this region does not directly set or regulate the sequencing of amino acids composed the protein or hormone. However, it was prepare or processing anything to facilitate the transcription process and translation of the gene, including activity of many enzymes in the beginning of reading the DNA strands, construct an RNA strand that compliment the DNA strand and then put together the amino acid chain. It may play an important role in the expression of the gene. In this study we found the association of polymorphism of T/C-20 and responsiveness to terbutaline nebulation with OR 4.53.
Similar to our preliminary study several years ago,16 we found the association between lung function (pre-test FEV1) and the response to terbutaline inhalation. However, it is not statistically signicant in this study. These phenomena may occur because bronchial lumen in normal lung function (FEV1 > 80%) cannot be dilated further by β2-agonist. The association of lung function and the response to β2 agonist was also found by Choudhry et al17 in Puerto Rican but not in Mexican, although they live in the same country and same environment. This phenomenon was related to the role of other genetic factors in ethnicity.
From various studies, it appears that genetics polymorphism of β2-agonist receptor is not only a single one factor which inuences the response to β2-agonist but also many other genetic factors, environmental variables and physiologic condition of host may be have a role.
CONCLUSIONThe polymorphism of Arg 16 has no effect on the
response to β2 agonist but the polymorphism of Gln 27 does with OR 3.18. New polymorphism is found in
nucleotide at 20th order before the start codon (up-stream), which also has an effect on the response to β2 agonist with OR 4.53. If the three polymorphisms are combined, the effect will be greater with OR 11.11.
REFERENCES 1. Mc Fadden, E.R . Asthma. In: Kasper DL, et al, eds. Harrison’s
principle of internal medicine. 16th edition. New York: McGraw-Hill Medical Publishing Division; 2005. p. 1508-16.
2. Sheffer AL, Bartal M, Bousquet J, Carrasco E, Chen YZ,Chuchalin AG, et al. The global initiative for asthma. Global strategy for asthma management and prevention. Bethesda: National Institutes of Health, NHBLI Publication. 2002;02-3659: 93-172.
3. Martinez FD, Graves PE, Baldini M, Solomon S and Erickson R. Association between genetic polymorphisms of the β2-adrenoceptor and response to albuterol in children with and without a history of wheezing. J Clin Invest. 1997;100:3184-8.
4. Israel E, Drazen JM, Liggett SB, Boushey HA, Cherniack RM, Chinchilli VM, et al. The effect of polymorphisms of the β2-adrenergic receptor on the response to regular use of albuterol in asthma. Am J Respir Crit Care Med. 2000;162:75-80.
5. Tan S, Hall IP, Dewar J, Dow E and Lipworth. Association between β2-adrenoceptor polymorphism and susceptibility to bronchodilator desensitization in moderately severe stable asthmatic. Lancet. 1997;350:995-9.
6. Lipworth BJ, Hall IP, Tan S, Azis I and Coutie W. Effect of genetic polymorphism on ex vivo and in vivo function of β2-adrenoceptors in asthma patients. Chest. 1999;115:324-8.
7. Spitzer WO, Suissa S, Ernst P, Horwitz RI, HabbickB, Cockroft D, et al. The use beta-agonists and the risk of death and near death from asthma. N Engl J Med. 1992;326:501-6.
8. Lanes SF, Rodriguez LA, Huerta C. Respiratory medication and risk of asthma death. Thorax. 2002;57:683-6.
9. Bai TR. Abnormalities in airway smooth muscle in fatal asthma. Am Rev Respir Dis. 1990;141:552-7.
10. Turki JJ, Pak J, Green SA, Martin RJ, Liggett SB. Polymorm-phisms of the beta 2-adrenergic receptor in nocturnal and nonnocturnal asthma. J Clin Invest. 1995;95:1635-41.
11. Reihsaus E, Innis M, MacIntyre N, Liggett SB. Mutations in the gene encoding for β2-adrenergic receptor in normal and asthmatic subjects. Am J Respir Cell Mol Biol. 1993;8:334-9.
12. Dewar JC, Wilkinson J, Wheatley A, Thomas NS, Doul I, Morton N, et al. The glutamine 27 β2-adrenoceptor polymorphism is associated with elevated IgE levels in asthmatic families. J Allergy Clin Immunol. 1997;100:261-5.
13. Hall IP, Wheatley A, Wilding P, Liggett SB. Association of glu-27 beta-2 adrenoceptor polymorphism with lower airway reactivity in asthmatic subjects. Lancet. 1995;345:1213-4.
14. Weir TD, Mallek N, Sandford AJ, Bai TR, Awadh N, Fitzgerald JM, et al. Beta-2-adrenergic receptor haplotypes in mild, moderate and fatal/near fatal asthma. Am J Repir Crit Care Med. 1998;158:787-91.
15. Hancox RJ, Sears MR, Taylor DR. Polymorphism of the β2-adrenoceptor and the response to longterm β2-agonist therapy in asthma. Eur Respir J. 1998;11:589-93.
16. Syamsu. Efek bronkodilatasi terbutalin aerosol pada penderita asma asimtomatis. KOPAPDI VII Makassar. 1987:111-8.
17. Choudhry S, Ung N, Avila PC, Nazario S, Casal J, Torres A, et al. Pharmacogenetic difference in response to albuterol between puerto Ricans and Mexicans with asthma. Am J Respir Crit Care Med. 2005;171:563-70.