Reproduced from CuttingEdge Volume 8 Issue 7 November 2018
8
Reproduced from CuttingEdge November 2018 Volume 8 Issue 7
Transcript of Reproduced from CuttingEdge Volume 8 Issue 7 November 2018

Reproduced from
CuttingEdgeNovember 2018Volume 8 Issue 7


November 2018 9Spinco Biotech
Hemoglobin (Hb) is a globular protein composed of four polypeptide subunits - two α-globin and two non-α-globin chains working in conjunction with heme to transport oxygen in the blood. Normal adult hemoglobin (HbA) is
designated α2β2. Variant hemoglobin is derived from genetic abnormalities affecting the α-globin genes (HbA1 or HbA2) or β-globin (HBB) structural genes (exons). More than a thousand hemoglobin variants have been identified relative to changes in the globin chains. Qualitative changes correspond to amino acid substitutions resulting in hemoglobinopathies.[1,2,3]
During 1950s, there was rapid progress towards understanding the structure and function of human hemoglobin. It was found that normal adults have a major hemoglobin called ‘Hb A’, comprising about 95-98% of the total, and a minor component, ‘Hb A2,’ which accounts for 2–3%. The main hemoglobin in infants is Hb F, only traces of which are found in normal adults. Earlier during development, there are three different embryonic hemoglobins. All these different hemoglobins were found to be tetramers of two pairs of unlike globin chains; adult and fetal hemoglobins have α chains combined with β (Hb A, α2β2), δ (Hb A2, α2δ2), or γ chains (Hb F, α2γ2).
[4]
India is an ethnically diverse country with marked regional variations. This diversity is reflected in the presence of different hemoglobin variants in different ethnic groups. Due to migration, there is constant mixing of people from different regions. Many of these abnormal variants are of little clinical significance in heterozygous state, but when combined with other variants they may give rise to several severe diseases. Therefore, there is always need for a screening method that can detect maximum variants. HPLC has the advantage of quantifying Hb F and Hb A2 along with the detection of other variants in a single screening test.
High Performance Liquid Chromatography (HPLC) has been used for low level quantitation of vitamins, nucleic acids, biogenic amines, TDM (Therapeutic Drug Monitoring) such as, immunosuppressants etc. HPLC-based methods will remain the gold standard in clinical testing for many of the current and future biomarkers. The main advantages of HPLC method over other techniques are their high selectivity, sensitivity, reliability and versatility with low cost operation. Its use in the clinical laboratory has steadily increased over the past decades as its unmatched analytical performance and versatility allow for testing of many different types of clinically relevant analytes.
- a true gold standard opens up
HPLC for Testing Hemoglobinopathies
Shailesh DamaleShimadzu Analytical (India) Pvt. Ltd.,
Bhaumik H. Trivedi
3
Figure 2. Prominence-i
Hemoglobin variants are most often inherited characteristics. First, abnormal beta gene can be inherited in an autosomal recessive fashion. This means that the person who inherits this will have two copies of the altered gene. Both of these genes can be passed to offspring. The next way they can be inherited is in a heterozygous fashion. This means that the person has one normal beta gene and one abnormal beta gene. This person is considered to be a carrier of whichever hemoglobin variant is inherited. Only the abnormal gene can be passed on to offspring in this case.
Along with lengthy list of common hemoglobin variants, there are some variants that are less common. These variants are considered silent, which means that they have no signs or symptoms. They usually affect the functionality and/or the stability of the hemoglobin molecule. With most of these variants are mutations in the alpha globin gene that result in an abnormally long alpha chain and an unstable hemoglobin molecule.
Thalassaemias are caused by impaired synthesis of one or more globin chains of the haemoglobin (consisting of 4 polypeptide chains), resulting in much less oxygen being bound to the haemoglobin molecules and transported through the body. Depending on which polypeptide chains are affected, the thalassaemias are named α, β, γ or δ thalassaemia. It is the β chain that is most frequently affected, so that this disorder is called β-thalassaemia. β-thalassaemia major is a homozygous form in which both partners are severely mutated so that β chain synthesis is stopped completely, whereas β-thalassaemia minor is a heterozygous form resulting in an approximately 20 % reduction of polypeptide synthesis. To compensate this reduction, more HbA2 and HbF are produced. In β-thalassaemia major it is more HbF, and in β-thalassaemia minor primarily HbA2. Depending on severity, patients may suffer from enlargement of the liver and spleen, growth disorders, severe inner organ damages and bone deformities. Further mutations are known that modify the peptide chains in other ways, leading to abnormal haemoglobin variants. The most common and clinically relevant variants are HbS, HbC and HbE. HbD also occurs relatively
i-Series HPLC

10 November 2018Spinco Biotech
4
often. Combinations of various thalassaemias with different genetically related haemoglobin variants are also possible.
Sickle cell anemia is an inherited form of anemia — a condition in which there aren't enough healthy red blood cells to carry adequate oxygen throughout your body. Normally, our red blood cells are flexible and round, moving easily through your blood vessels. In sickle cell anemia, the red blood cells become rigid and sticky and are shaped like sickles or crescent moons as shown in Figure 3. These irregularly shaped cells can get stuck in small blood vessels, which can slow or block blood flow and oxygen to parts of the body.
Figure 3. Sickle cell
As of 2015, about 4.4 million people have sickle cell disease, while an additional 43 million have sickle cell trait. About 80% of sickle cell disease cases are believed to occur in Sub-Saharan Africa. It also occurs relatively frequently in parts of India, the Arabian Peninsula and among people of African origin living in other parts of the world. In 2015, it resulted in about 114,800 deaths.
The primary purpose of new born screening for hemoglobinopathies is to identify infants with sickle cell disease (SCD), especially sickle cell anemia or clinically relevant thalassemia. The diagnosis can be confirmed within 2 months of age. However screening also identifies infants with other haemoglobin variants, many of which are clinically mild or insignificant.
Hemoglobin F is the primary hemoglobin produced by the fetus. Hemoglobin transports oxygen efficiently in a low oxygen environment. The hemoglobin production stops at birth and decreases to adult levels by the age of one or two. The levels can be normal to increased in beta thalassemia. Hemoglobin F frequently increases in individuals with sickle cell anemia and sickle cell-beta thalassemia. Individuals with sickle cell and increase of Hb F have a milder case of the disease. There are situations where the Hb F is increased. This rare condition is called Hereditary Persistence of Fetal Hemoglobin (HPFH). This is a group of disorders where the Hemoglobin F is increased without signs or clinical features of thalassemia. Some different ethnic groups have different mutations that cause HPFH. Hb F can also be increase by acquired conditions that involve the red blood cells. Elevated Hemoglobin F levels are also associated with Leukemia and myeloproliferative disorders.
6
Fig 4: G
Globin switcch during in utero and ppost-natal liffe
Fig. 2: Sickle cell
Fig. 3: Globin switch during in utero and post-natal life
HPLC for Testing Hemoglobinopathies
Besides HPLC, there are other analytical procedures used for detection of thalassemia and hemoglobinopathies such as alkaline and acid electrophoresis, Hb A2 quantification by ion-exchange column chromatography and Hb F quantification by alkali denaturation and radial immunodiffusion. Electrophoretic methods will not separate Hb E and O or D and G. False-positive diagnosis of sickle cell anemia and incorrect or unresolved diagnosis of hemoglobinopathies are sometimes encountered. It is recommended during
such screening programs that further tests should always be carried out to confirm the presumed identity of an abnormal variant. None of the above-mentioned methods can detect multiple hemoglobin fractions in a single step procedure. HPLC has many advantages over these methods and over the past decades it has evolved as an excellent and powerful diagnostic tool for identification of most of the clinically significant Hb variants especially the beta thalassemia trait owing to its quantitative power and automation. HPLC is sensitive, specific, reproducible, less time consuming and requires less manpower. Hence, it is ideal for a routine clinical laboratory with high workload.
The developed HPLC procedure detects major variants and has fast turnaround time. This technique accurately diagnoses even the variants that would have been missed by the traditional electrophoretic methods. The Shimadzu i-Series HPLC (LC-2030C), integrated system has ICM (Interactive Communication Mode) for freeing up operators from laboratory besides providing maximum reliability, stability and ultrafast injection cycle to reduce analysis times.
The Hb variants analysis was done based on the principle of cation exchange; HPLC column packed with silica and coated with polyaspartic acid was used. This column improves the elution time of hemoglobin analysis while maintaining high sensitivity and resolution necessary for both screening and confirmatory purposes. Buffers made using commonly available reagents were used for the method. A simple sample preparation work flow was developed for DBS (Dried Blood Spot) and whole blood. In case of whole blood 3 µL of sample was diluted in 1000 µL of mobile phase A as diluent. The same methodology can be used for New Born Screening (NBS); a 3 mm disc of DBS was taken and transferred in 1000 µL of diluent. The DBS and diluent was mixed till the DBS cleared. This mixture was centrifuged for 10 minutes and the supernatant was injected. DBS analysis is not possible with existing closed HPLC systems whereas open systems like i-Series HPLC can very well be used for both whole blood and DBS.
Hemoglobin variants are most often inherited characteristics. An abnormal beta gene can be inherited in an autosomal recessive fashion. This means that the person who inherits will have two
2
most of the clinically significant Hb variants especially to beta thalassemia trait owing to its quantitative power and automation. HPLC is sensitive, specific, reproducible, and less time consuming and requires less manpower. Hence, it is ideal for a routine clinical laboratory with high work load.
Figure 1. Hemoglobin
High-performance liquid chromatographic (HPLC) methods with high sensitivity and specificity have been developed for analysis of Hb variants. The analysis procedures have the sensitivity for detecting major variants and have fast turnaround time required for large numbers of samples. The techniques have produced accurate diagnoses that would have been missed by the traditional electrophoretic methods.
Using Shimadzu Prominence-i (LC-2030C), (Figure 2) which is an integrated system of Prominence-i series is a perfect system for a clinical diagnostic set up as it has ICM (Interactive Communication Mode) for freeing up operators from laboratory besides providing maximum reliability, stability and ultrafast injection cycle to reduce analysis time.
The analysis Hb variants is done based on the principle of cation exchange; we used HPLC column packed with silica and coated with polyaspartic acid. Such a column improves the elution time of hemoglobin analysis while maintaining the high sensitivity and resolution necessary for both screening and confirmatory purposes. Buffers compatible to column and analysis were used for the method. A simple sample preparation work flow was developed for DBS and whole blood. In case of whole blood 3 µL of sample was diluted in 1000 µL of mobile phase A as diluent. The same methodology can be used for NBS, a 3 mm disc of DBS (Dried Blood Spot) was taken and transferred in 1000 µL of diluent. The mixture of DBS and diluent is mixed till the DBS is cleared. This mixture is allowed to centrifuge for 10 minutes and the supernatant is injected. DBS analysis was not possible with existing closed HPLC systems whereas open systems like Prominence-i can very well be used for both whole blood and DBS.
Fig. 1: Hemoglobin

November 2018 11Spinco Biotech
copies of the altered gene. Both of these genes can be passed to the offspring. The other way they can be inherited is in a heterozygous fashion. This means that the person has one normal beta gene and one abnormal beta gene. The person is considered to be a carrier of whichever hemoglobin variant is inherited. Only the abnormal gene can be passed onto the offspring.
Among the lengthy list of common hemoglobin variants, there are some variants that are less common. These variants are considered silent, which means that they have no signs or symptoms. They usually affect the functionality and/or the stability of the hemoglobin molecule. Most of these variants arise due to mutations in the alpha globin gene resulting in an abnormally long alpha chain and an unstable hemoglobin molecule.
Thalassemia are caused by impaired synthesis of one or more globin chains of hemoglobin (consisting of 4 polypeptide chains), resulting in much less oxygen being bound to the hemoglobin molecules and transported through the body. Depending on which polypeptide chains are affected, the thalassemias are named α, β, γ or δ thalassemia. It is the β chain that is most frequently affected and hence this disorder is called β-thalassemia. β-thalassemia major is a homozygous form in which both partners are severely mutated so that β chain synthesis is stopped completely, whereas β-thalassemia minor is a heterozygous form resulting in an approximately 20% reduction of polypeptide synthesis. To compensate this reduction, more HbA2 and Hb F are produced. In β-thalassemia major it is more Hb F, and in β-thalassemia minor it is primarily HbA2.
Depending on severity, patients may suffer from enlargement of the liver and spleen, growth disorders, severe inner organ damages and bone deformities. Further mutations are known that modify the peptide chains in other ways, leading to abnormal hemoglobin variants. The most common and clinically relevant variants are Hb S, Hb C and Hb E. Hb D also occurs relatively often. Combinations of various thalassemias with different genetically related hemoglobin variants are also possible.
Sickle cell anemia is an inherited form of anemia - a condition in which there isn’t enough healthy red blood cells to carry adequate oxygen throughout the body. Normally, our red blood cells are flexible and round, moving easily through the blood vessels. In sickle cell anemia, the red blood cells become rigid, sticky and
are shaped like sickles or crescent moons as shown in Figure 2. These irregularly shaped cells can get stuck in small blood vessels, which can slow or block blood flow and oxygen to parts of the body.
As of 2015, about 4.4 million people have sickle cell disease, while an additional 43 million have sickle cell trait. About 80% of sickle cell disease cases are believed to occur in Sub-Saharan Africa. It also occurs relatively frequently in parts of India, the Arabian Peninsula and among people of African origin living in other parts of the world. In 2015, it resulted in about 114,800 deaths.
The primary purpose of NBS for hemoglobinopathies is to identify infants with Sickle Cell Disease (SCD), especially sickle cell anemia or clinically relevant thalassemia. The diagnosis can be confirmed within two months of age. However screening also identifies infants with other hemoglobin variants, many of which are clinically mild or insignificant.
Hemoglobin F is the primary hemoglobin produced by the fetus that transports oxygen efficiently in a low oxygen environment. The hemoglobin production stops at birth and decreases to adult levels by the age of one or two. The levels can be normal to increased in beta thalassemia. Individuals with sickle cell and increase of Hb F have a milder case of the disease. There are situations where the Hb F is increased. This rare condition is called Hereditary Persistence of Fetal Hemoglobin (HPFH). This is a group of disorder where the Hemoglobin F is increased without signs or clinical features of thalassemia. Some different ethnic groups have different mutations that cause HPFH. Hb F can also increase by acquired conditions that involve the red blood cells. Elevated Hemoglobin F levels are also associated with Leukemia and myeloproliferative disorders.
The most widely used method for hemoglobin analysis is cellulose acetate electrophoresis at alkaline pH. It is rapid, reproducible and capable of separating common hemoglobin variants such as S, F, A, and C, but Hb A2, C, O and E remain unresolved, as do Hb S, D, and G. Consequently, citrate agar electrophoresis at acidic pH is needed for the identification of the aforementioned Hb. Nevertheless, electrophoretic methods will not separate Hb E and O or D and G. False-positive diagnosis of sickle cell anemia and incorrect or unresolved diagnosis of hemoglobinopathies are sometimes encountered. HPLC with high sensitivity
HPLC for Testing Hemoglobinopathies

12 November 2018Spinco Biotech
7
0.0 2.5 5.0 min
0
10
20
30
40
50
60mV
Hb
FHb
A0
Hb
A2
Hb
Q
0.0 2.5 5.0 min
0
10
20
30
40
50
mV
Hb
FHb
A0
Hb
E
0.0 2.5 5.0 min
0
10
20
30
40
mV
Hb
FHb
A0
Hb
D
0.0 2.5 5.0 min
0
5
10
15
20
25
30
35mV
Hb
FHb
A0
Hb
A2
0.0 2.5 5.0 min
0.0
2.5
5.0
7.5
10.0
12.5
15.0
17.5
20.0mV
Hb
FHb
A0
Hb
A2
Hb
S
0.0 2.5 5.0 min
0
10
20
30
40
50
60
70mV
Hb
FHb
A0
Hb
Lapo
reHb
A2
0.0 2.5 5.0 min
0
10
20
30
40
50
mV
Hb
FHb
JHb
A0
Hb
A2
0.0 2.5 5.0 min
0
5
10
15
20
25
30
35
mV
Hb
FHb
A0
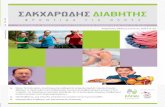
Figure 5a. Hemoglobin variants F, A0 and A2
Figure 5b. Hemoglobin variants F, A0, A2 and S
Figure 5c. Hemoglobin variants F, A0 and D
Figure 5e. Hemoglobin variants F, A0, A2 and Q-India
Figure 5f. Hemoglobin variants F, A0, Lapore and A2
Figure 5g. Hemoglobin variants F, J, A0 and A2
Figure 5d. Hemoglobin variants F, A0 and E Figure 5h. Hemoglobin variants F and A0 of Newborn DBS
and specificity have recently been developed for both screening and confirmation of hemoglobinopathies in new-borns and adults. The procedures have the sensitivity for detecting major variants and have fast turnaround time (8 min/sample) required for large numbers of samples. The method is capable of resolving Hb F, Hb A0, Hb A2, Hb S, Hb D, Hb E, Hb Q-India, Hb Lepore, Hb C, Hb J (practically checked) eluting at different retention times.
7
0.0 2.5 5.0 min
0
10
20
30
40
50
60mV
Hb
FHb
A0
Hb
A2
Hb
Q
0.0 2.5 5.0 min
0
10
20
30
40
50
mV
Hb
FHb
A0
Hb
E
0.0 2.5 5.0 min
0
10
20
30
40
mV
Hb
FHb
A0
Hb
D
0.0 2.5 5.0 min
0
5
10
15
20
25
30
35mV
Hb
FHb
A0
Hb
A2
0.0 2.5 5.0 min
0.0
2.5
5.0
7.5
10.0
12.5
15.0
17.5
20.0mV
Hb
FHb
A0
Hb
A2
Hb
S
0.0 2.5 5.0 min
0
10
20
30
40
50
60
70mV
Hb
FHb
A0
Hb
Lapo
reHb
A2
0.0 2.5 5.0 min
0
10
20
30
40
50
mV
Hb
FHb
JHb
A0
Hb
A2
0.0 2.5 5.0 min
0
5
10
15
20
25
30
35
mV
Hb
FHb
A0
Figure 5a. Hemoglobin variants F, A0 and A2
Figure 5b. Hemoglobin variants F, A0, A2 and S
Figure 5c. Hemoglobin variants F, A0 and D
Figure 5e. Hemoglobin variants F, A0, A2 and Q-India
Figure 5f. Hemoglobin variants F, A0, Lapore and A2
Figure 5g. Hemoglobin variants F, J, A0 and A2
Figure 5d. Hemoglobin variants F, A0 and E Figure 5h. Hemoglobin variants F and A0 of Newborn DBS
7
0.0 2.5 5.0 min
0
10
20
30
40
50
60mV
Hb
FHb
A0
Hb
A2
Hb
Q
0.0 2.5 5.0 min
0
10
20
30
40
50
mV
Hb
FHb
A0
Hb
E
0.0 2.5 5.0 min
0
10
20
30
40
mV
Hb
FHb
A0
Hb
D
0.0 2.5 5.0 min
0
5
10
15
20
25
30
35mV
Hb
FHb
A0
Hb
A2
0.0 2.5 5.0 min
0.0
2.5
5.0
7.5
10.0
12.5
15.0
17.5
20.0mV
Hb
FHb
A0
Hb
A2
Hb
S
0.0 2.5 5.0 min
0
10
20
30
40
50
60
70mV
Hb
FHb
A0
Hb
Lapo
reHb
A2
0.0 2.5 5.0 min
0
10
20
30
40
50
mV
Hb
FHb
JHb
A0
Hb
A2
0.0 2.5 5.0 min
0
5
10
15
20
25
30
35
mV
Hb
FHb
A0
Figure 5a. Hemoglobin variants F, A0 and A2
Figure 5b. Hemoglobin variants F, A0, A2 and S
Figure 5c. Hemoglobin variants F, A0 and D
Figure 5e. Hemoglobin variants F, A0, A2 and Q-India
Figure 5f. Hemoglobin variants F, A0, Lapore and A2
Figure 5g. Hemoglobin variants F, J, A0 and A2
Figure 5d. Hemoglobin variants F, A0 and E Figure 5h. Hemoglobin variants F and A0 of Newborn DBS
7
0.0 2.5 5.0 min
0
10
20
30
40
50
60mV
Hb
FHb
A0
Hb
A2
Hb
Q
0.0 2.5 5.0 min
0
10
20
30
40
50
mV
Hb
FHb
A0
Hb
E
0.0 2.5 5.0 min
0
10
20
30
40
mV
Hb
FHb
A0
Hb
D
0.0 2.5 5.0 min
0
5
10
15
20
25
30
35mV
Hb
FHb
A0
Hb
A2
0.0 2.5 5.0 min
0.0
2.5
5.0
7.5
10.0
12.5
15.0
17.5
20.0mV
Hb
FHb
A0
Hb
A2
Hb
S
0.0 2.5 5.0 min
0
10
20
30
40
50
60
70mV
Hb
FHb
A0
Hb
Lapo
reHb
A2
0.0 2.5 5.0 min
0
10
20
30
40
50
mV
Hb
FHb
JHb
A0
Hb
A2
0.0 2.5 5.0 min
0
5
10
15
20
25
30
35
mV
Hb
FHb
A0
Figure 5a. Hemoglobin variants F, A0 and A2
Figure 5b. Hemoglobin variants F, A0, A2 and S
Figure 5c. Hemoglobin variants F, A0 and D
Figure 5e. Hemoglobin variants F, A0, A2 and Q-India
Figure 5f. Hemoglobin variants F, A0, Lapore and A2
Figure 5g. Hemoglobin variants F, J, A0 and A2
Figure 5d. Hemoglobin variants F, A0 and E Figure 5h. Hemoglobin variants F and A0 of Newborn DBS
7
0.0 2.5 5.0 min
0
10
20
30
40
50
60mV
Hb
FHb
A0
Hb
A2
Hb
Q
0.0 2.5 5.0 min
0
10
20
30
40
50
mV
Hb
FHb
A0
Hb
E
0.0 2.5 5.0 min
0
10
20
30
40
mV
Hb
FHb
A0
Hb
D
0.0 2.5 5.0 min
0
5
10
15
20
25
30
35mV
Hb
FHb
A0
Hb
A2
0.0 2.5 5.0 min
0.0
2.5
5.0
7.5
10.0
12.5
15.0
17.5
20.0mV
Hb
FHb
A0
Hb
A2
Hb
S
0.0 2.5 5.0 min
0
10
20
30
40
50
60
70mV
Hb
FHb
A0
Hb
Lapo
reHb
A2
0.0 2.5 5.0 min
0
10
20
30
40
50
mV
Hb
FHb
JHb
A0
Hb
A2
0.0 2.5 5.0 min
0
5
10
15
20
25
30
35
mV
Hb
FHb
A0
Figure 5a. Hemoglobin variants F, A0 and A2
Figure 5b. Hemoglobin variants F, A0, A2 and S
Figure 5c. Hemoglobin variants F, A0 and D
Figure 5e. Hemoglobin variants F, A0, A2 and Q-India
Figure 5f. Hemoglobin variants F, A0, Lapore and A2
Figure 5g. Hemoglobin variants F, J, A0 and A2
Figure 5d. Hemoglobin variants F, A0 and E Figure 5h. Hemoglobin variants F and A0 of Newborn DBS
7
0.0 2.5 5.0 min
0
10
20
30
40
50
60mV
Hb
FHb
A0
Hb
A2
Hb
Q
0.0 2.5 5.0 min
0
10
20
30
40
50
mV
Hb
FHb
A0
Hb
E
0.0 2.5 5.0 min
0
10
20
30
40
mV
Hb
FHb
A0
Hb
D
0.0 2.5 5.0 min
0
5
10
15
20
25
30
35mV
Hb
FHb
A0
Hb
A2
0.0 2.5 5.0 min
0.0
2.5
5.0
7.5
10.0
12.5
15.0
17.5
20.0mV
Hb
FHb
A0
Hb
A2
Hb
S
0.0 2.5 5.0 min
0
10
20
30
40
50
60
70mV
Hb
FHb
A0
Hb
Lapo
reHb
A2
0.0 2.5 5.0 min
0
10
20
30
40
50
mV
Hb
FHb
JHb
A0
Hb
A2
0.0 2.5 5.0 min
0
5
10
15
20
25
30
35
mV
Hb
FHb
A0
Figure 5a. Hemoglobin variants F, A0 and A2
Figure 5b. Hemoglobin variants F, A0, A2 and S
Figure 5c. Hemoglobin variants F, A0 and D
Figure 5e. Hemoglobin variants F, A0, A2 and Q-India
Figure 5f. Hemoglobin variants F, A0, Lapore and A2
Figure 5g. Hemoglobin variants F, J, A0 and A2
Figure 5d. Hemoglobin variants F, A0 and E Figure 5h. Hemoglobin variants F and A0 of Newborn DBS
7
0.0 2.5 5.0 min
0
10
20
30
40
50
60mV
Hb
FHb
A0
Hb
A2
Hb
Q
0.0 2.5 5.0 min
0
10
20
30
40
50
mV
Hb
FHb
A0
Hb
E
0.0 2.5 5.0 min
0
10
20
30
40
mV
Hb
FHb
A0
Hb
D
0.0 2.5 5.0 min
0
5
10
15
20
25
30
35mV
Hb
FHb
A0
Hb
A2
0.0 2.5 5.0 min
0.0
2.5
5.0
7.5
10.0
12.5
15.0
17.5
20.0mV
Hb
FHb
A0
Hb
A2
Hb
S
0.0 2.5 5.0 min
0
10
20
30
40
50
60
70mV
Hb
FHb
A0
Hb
Lapo
reHb
A2
0.0 2.5 5.0 min
0
10
20
30
40
50
mV
Hb
FHb
JHb
A0
Hb
A2
0.0 2.5 5.0 min
0
5
10
15
20
25
30
35
mV
Hb
FHb
A0
Figure 5a. Hemoglobin variants F, A0 and A2
Figure 5b. Hemoglobin variants F, A0, A2 and S
Figure 5c. Hemoglobin variants F, A0 and D
Figure 5e. Hemoglobin variants F, A0, A2 and Q-India
Figure 5f. Hemoglobin variants F, A0, Lapore and A2
Figure 5g. Hemoglobin variants F, J, A0 and A2
Figure 5d. Hemoglobin variants F, A0 and E Figure 5h. Hemoglobin variants F and A0 of Newborn DBS
7
0.0 2.5 5.0 min
0
10
20
30
40
50
60mV
Hb
FHb
A0
Hb
A2
Hb
Q
0.0 2.5 5.0 min
0
10
20
30
40
50
mV
Hb
FHb
A0
Hb
E
0.0 2.5 5.0 min
0
10
20
30
40
mV
Hb
FHb
A0
Hb
D
0.0 2.5 5.0 min
0
5
10
15
20
25
30
35mV
Hb
FHb
A0
Hb
A2
0.0 2.5 5.0 min
0.0
2.5
5.0
7.5
10.0
12.5
15.0
17.5
20.0mV
Hb
FHb
A0
Hb
A2
Hb
S
0.0 2.5 5.0 min
0
10
20
30
40
50
60
70mV
Hb
FHb
A0
Hb
Lapo
reHb
A2
0.0 2.5 5.0 min
0
10
20
30
40
50
mV
Hb
FHb
JHb
A0
Hb
A2
0.0 2.5 5.0 min
0
5
10
15
20
25
30
35
mV
Hb
FHb
A0
Figure 5a. Hemoglobin variants F, A0 and A2
Figure 5b. Hemoglobin variants F, A0, A2 and S
Figure 5c. Hemoglobin variants F, A0 and D
Figure 5e. Hemoglobin variants F, A0, A2 and Q-India
Figure 5f. Hemoglobin variants F, A0, Lapore and A2
Figure 5g. Hemoglobin variants F, J, A0 and A2
Figure 5d. Hemoglobin variants F, A0 and E Figure 5h. Hemoglobin variants F and A0 of Newborn DBS
Fig. 4a: Hemoglobin variants F, A0 and A2
Fig. 4b: Hemoglobin variants F, A0, A2 and S
Fig. 4c: Hemoglobin variants F, A0 and D
Fig. 4d: Hemoglobin variants F, A0 and E Fig. 4h: Hemoglobin variants F and A0 of Newborn DBS
Fig. 4g: Hemoglobin variants F, J, A0 and A2
Fig. 4f: Hemoglobin variants F, A0, Lapore and A2
Fig. 4e: Hemoglobin variants F, A0, A2 and Q-India
HPLC for Testing Hemoglobinopathies

November 2018 13Spinco Biotech
The confirmatory techniques have produced accurate diagnoses that would have been missed by the traditional electrophoretic methods. The system is capable to perform DBS and liquid whole blood is used for screening and/or confirmation of children (greater than one year of age) and adults. There are changes in hemoglobin types and quantities through the first year of life, but after a year of age the hemoglobin types of an individual are going to remain the same. The changes occur in relative proportions of globin chains at various stages of embryonic, fetal and post-natal life [5]. Table 1 lists the percentages of normal and variant haemoglobin seen in new-borns and older children. Figure 3. shows how the globin synthesis (globin-switch) happens during in-utero and post-natal life.
The chromatograms shown in Figure 4 are of the hemoglobin samples analysed on Shimadzu i-Series (LC-2030C). These unusual hemoglobins are most common among people whose ancestors originate from former and current malaria zones of the world; for example, Africa, Asia, the Middle and Far East, Mediterranean islands, and South America. Because of migration and intermarriage, it is also seen in people who did not originate from malaria zones of the world.
In Figure 4b, there is existence of Hb S. Its presence is due to a genetic condition in which the quality of hemoglobin is defective. This condition can cause abnormal hemoglobin that result in abnormally-shaped (sickled) red blood cells (see illustration). These abnormal red blood cells cannot easily pass through small blood vessels leading to inadequate oxygen to the tissues. Sickle cells also have a shorter life span than normal red blood cells
(10 to 20 days compared to 120 days). This rapid turnover may result in inadequate time to replace the red blood cells and may result in anemia. In sickle cell anemia, one defective hemoglobin gene is inherited from each parent. If only one gene is inherited from one parent, then the condition is milder and referred to as sickle cell trait. Symptoms of sickle cell anemia vary depending on its severity. Patients with sickle cell trait may experience mild, if any, symptoms at all. In sickle cell disease, symptoms are more significant, especially in episodes of acute crisis.
In Figure 4c, there is presence of Hb D or hemoglobin D-Punjab, also known as hemoglobin D-Los Angeles, one of the most common hemoglobin variants worldwide. It is derived from a point mutation in the beta-globin gene prevalent in the Punjab region, Northwestern India. Hemoglobin D-Punjab can be inherited in heterozygosis with hemoglobin A causing no clinical or hematological alterations, or in homozygosis, the rarest form of inheritance, a condition that is commonly not related to clinical symptomatology. Moreover, this variant can exist in association with other hemoglobinopathies, such as thalassemias; the most noticeable clinical alterations occur when hemoglobin D-Punjab is associated to hemoglobin S. The clinical manifestations of this association can be similar to homozygosis for hemoglobin S. Although hemoglobin D-Punjab is a common variant globally with clinical importance especially in cases of double heterozygosis, hemoglobin S/D-Punjab is still understudied.
In Figure 4d, the Hemoglobin E (Hb E) is also an abnormal hemoglobin with a single point mutation in the β chain. At position 26 there is a change in the amino acid, from glutamic acid to lysine (E26K).
Hemoglobin Structure Level at birth Level in adults Comments
A α2β2 20-25% 97% Reaches adult levels by 1 year of age
A2 α2δ2 0.50% 2.50% Elevated in β thalassemia
F α2γ2 75-80% < 1% Reaches adult levels by 1 year of age
HbH Β415-20% in HbH
disease NA HbH produces Heinz bodies in erythrocytes and hemolysis
Hb Bart γ4100% in hydrops
fetalis 15-20 in HbH disease
NA Increased in carriers of α-thalassemia trait at birth
Table 1: Percentage of Hemoglobin.
HPLC for Testing Hemoglobinopathies

14 November 2018Spinco Biotech
Hemoglobin E is very common among people of Southeast Asia, Northeast India, Sri Lanka and Bangladeshi descent.
In Figure 4e, Hemoglobin (HbQ) or Hb Q-India is a clinically silent hemoglobinopathy that results from modification of alpha 1 globin gene (AAG>GAG) substituting arginine for histidine. HbQ was first described in association with alpha thalassemia in a Chinese patient. Three variations have been described namely India, Thailand and Iran based on the involved codon (64, 74 and 75 respectively). This infrequent disorder has been detected in the homozygous and heterozygous states in association with alpha and beta thalassemia. The first case of Hb Q-India was reported in 1972 in a Sindhi family with associated beta thalassemia. Hb Q-India is usually seen in the heterozygous form which is clinically silent not having deleterious phenotypic effect. The major clinical significance of Hb Q is its correct diagnosis. The identification of hemoglobin variants by conventional techniques is often presumptive.
In Figure 4f, Hemoglobin Lepore is an unusual hemoglobin molecule composed of two alpha chains and two delta-beta chains as a result of the fusion of delta and beta genes. The delta-beta chains have the first 87 amino acids of the delta chain and 32 amino acids of the beta chain. There are three common variants of hemoglobin Lepore: Hb Lepore Washington (also known as Hb Lepore Boston), Hb Lepore Baltimore and Hb Lepore Hollandia. Hemoglobin Lepore is seen in individuals of Mediterranean descent. Individuals with Hb A/Hb Lepore are asymptomatic, with Hb Lepore representing 5-15% of haemoglobin and slightly elevated Hb F (2–3%). However, homozygous Lepore individuals suffer from severe anemia similar to patients with beta-thalassemia intermedia, with Hb Lepore representing 8-30% of hemoglobin and the remaining hemoglobin as Hb F. Patients with Hb Lepore/beta-thalassemia experience severe disease complications similar to patients with beta-thalassemia major.
In Figure 4g, Hemoglobin J (Hb J) an abnormal hemoglobin with an alpha globin gene variant is prevalent in various geographic locations. It was first reported in a black American family in 1956.
Later on, it has been further reported from Indonesia, India, and other parts of the world. Hemoglobin J reported from Meerut India shows the mutation of 120th alanine to glutamic acid on alpha chain.
Conclusions
HPLC has played a significant role in the clinical diagnostic laboratory over the years. Though it is a gold standard technique for Hb variants and the availability of many closed HPLC systems have addressed many applications, they always had some drawbacks one of which is their inability to perform analysis using DBS. Earlier the demands on Hb variants analysis in NBS using DBS was fulfilled by performing the test using traditional techniques. The home-brewed reagent system in Hb variant analysis using Shimadzu’s i-Series HPLC (LC-2030C) makes it possible to perform the analysis using DBS (Figure 4h) and further reduces the dependency on kits in turn making it more productive and cost effective. The chromatographic conditions developed provide excellent resolution of more than 9 frequently encountered human hemoglobins and thus leads to an accurate diagnosis of hemoglobinopathies in the clinical laboratory. This makes it an excellent method for the screening of high-risk new-born populations and the preliminary diagnosis for adults for hemoglobinopathies. The turnaround time for each specimen is 8 minutes on HPLC system. These conditions make Shimadzu’s i-Series HPLC (LC-2030C) a perfect tool in the clinical diagnostic laboratory for performing Hb variant analysis.
References1. A.D.A.M. Medical Encyclopedia [Internet]. Atlanta (GA):
A.D.A.M., Inc.; ©2005 Thalassemia; updated 2014 Feb 24; cited 2015 Apr 10]. Available from: http://www.nlm.nih.gov/ medlineplus/ency/article/000587.htm
2. Tietz: Fundamentals of Clinical Chemistry, (6th Edition). Burtis, C. A., Ashwood, E. R., Bruns, D.E. (Eds.). (2008).Haryana, India: Elsevier.
3. National Library of Medicine. (2009) HBB. Retrieved from http://ghr.nlm.nih.gov/gene/HBB
4. Pagana, Kathleen Deska. Mosby's Manual of Diagnostic and Laboratory Tests. St. Louis: Mosby, Inc., 1998.
5. William Joseph William: Williams Hematology, Volume 487-Sixth Edition, 2001.
C E
HPLC for Testing Hemoglobinopathies