Pancreatic Transplantation · AngelikA C. gruessner, rAjA kAndAswAmy, khAlid m. khAn, dAvid e. r....
14
840 CHAPTER 73 Pancreatic Transplantation ANGELIKA C. GRUESSNER, RAJA KANDASWAMY, KHALID M. KHAN, DAVID E. R. SUTHERLAND, and RAINER W. GRUESSNER INTRODUCTION The treatment options for insulin-dependent diabetes mellitus are either exogenous insulin administration or β-cell replace- ment by pancreas or islet transplantation. Exogenous insulin administration is burdensome to the patient and gives imper- fect glycemic control, predisposing to secondary complica- tions of the eyes, nerves, kidneys, and other systems. On the other hand, β-cell replacement, when successful, establishes a constant euglycemic state but requires major surgery (a pan- creas transplant) and immunosuppression to prevent rejection, predisposing to complications, often compounded by comor- bidities from pre-existing diabetes. The Diabetes Control and Complications Trial (1) showed that intensive insulin therapy (multiple injections per day with dose adjusted by frequent blood sugar determinations) decreased (although rarely normalized) glycosylated hemoglobin (HgbA 1c ) levels and reduced the rate of secondary complications (2). The threshold for totally eliminating the risks of secondary diabetic complications is perfect glycemic control, an objective that can be achieved by the most sophisticated exogenous insulin deliv- ery devices unfortunately at the cost of frequent hypoglycemic episodes. This may change in the future with real-time glucose monitoring systems combined with insulin pumps (3,4). Pan- creas transplantation induces insulin independence in diabetic recipients without the risk of hypoglycemia and can ameliorate secondary complications. With major advances in the manage- ment of pancreas transplantation, the success rate of pancreas transplants has progressively increased during the past two decades (5,6). Today’s recipients have a high probability of being insulin independent for years, if not indefinitely. Historically, islet transplants have been less successful for a variety of reasons. In the late 1990s at the University of Alberta, insulin independence was achieved in several consec- utive recipients by sequential grafting of islets from multiple donors and the use of a steroid-free nondiabetogenic immuno- suppressive regimen (7). In another series from the University of Minnesota with a similar regimen, single-donor islet trans- plants induced insulin independence (8). In the Minnesota series, the donors had a high body mass index and the recipi- ents had a low body mass index. Thus, the net number of islets transplanted per unit weight was similar in the Alberta and Minnesota series. Islet transplants can succeed with stringent donor and recipient selections, but is not yet able to supersede pancreas transplants as the mainstay of β-cell replacement. Until islet transplants can consistently succeed from a single donor, regardless of size or recipient insulin requirements, an integrated approach is preferable (9): low-risk patients should undergo a surgically more challenging pancreas transplant, high-risk patients an islet transplant. Although short-term islet graft survival appears promis- ing (even with single donors) (10), long-term graft function after islet transplants (even with multiple donors) continues to be a major impediment to rapid progress. In the University of Alberta series, only 10% of islet transplant recipients were insulin independent at 5 years posttransplant (11). The main tradeoff for recipients of β-cell allografts is the need for immunosuppression. A successful graft makes the recipient euglycemic and normalizes HgbA 1c levels (11,12), but the combined risks of immunosuppression and pancreas trans- plant surgery must be weighed against the long-term risks of imperfect glycemic control and of development of secondary complications with exogenous insulin. A randomized prospec- tive trial has not been done to weigh these risks. The burden of day-to-day management of diabetes, with need for multiple needlesticks to inject insulin and monitor blood sugar levels tilts the balance in favor of a transplant for many diabetic patients. Furthermore, antirejection strategies are continually being developed to decrease the side effects of immunosup- pression. Nevertheless, only a few institutions perform pan- creas transplants soon after the onset of the disease (13). The main indications for a pancreas transplant in patients with normal kidney function has been labile diabetes with frequent insulin reactions and hypoglycemic unawareness, a syndrome that may emerge years after the onset of diabe- tes, particularly in patients with autonomic neuropathy (14). However, even for nonlabile diabetic patients who attempt tight control by intensive glucose monitoring, literature shows a high rate of secondary complications that are just as mor- bid as (15), if not more so than, chronic immunosuppressive complications in organ allograft recipients (16,17). Thus, for a patient who wishes to avoid a lifetime of insulin injections and glucose monitoring and who prefers the risks of immu- nosuppressive complications to the secondary complications of diabetes, a pancreas transplant can be performed with good results (18). This also applies to type 2 diabetics who are obligatory insulin dependent. About 5% of pancreas trans- plants are performed in selected type 2 diabetics (19). In the past, most pancreas transplant candidates had advanced diabetic nephropathy and required a kidney trans- plant also. As the risks of immunosuppression are assumed because of the kidney transplant, a simultaneous or sequential pancreas transplant does not pose any additional risks other than surgery (13). Indeed, pancreas transplants have been done in renal allograft recipients who meet the criteria for type 2 dia- betes with elimination of the need for exogenous insulin (20). RECIPIENT CATEGORIES Diabetic pancreas transplant candidates are divided into three categories: uremic (need a kidney transplant), posturemic (have a functioning kidney transplant), and nonuremic (do not need a kidney transplant). For candidates who are uremic, the options LWBK1580_C73_p840-853.indd 840 31/07/17 5:40 PM
Transcript of Pancreatic Transplantation · AngelikA C. gruessner, rAjA kAndAswAmy, khAlid m. khAn, dAvid e. r....

840
Chapter
73Pancreatic TransplantationAngelikA C. gruessner, rAjA kAndAswAmy, khAlid m. khAn, dAvid e. r. sutherlAnd, and rAiner w. gruessner
InTroducTIon
The treatment options for insulin-dependent diabetes mellitus are either exogenous insulin administration or β-cell replace-ment by pancreas or islet transplantation. Exogenous insulin administration is burdensome to the patient and gives imper-fect glycemic control, predisposing to secondary complica-tions of the eyes, nerves, kidneys, and other systems. On the other hand, β-cell replacement, when successful, establishes a constant euglycemic state but requires major surgery (a pan-creas transplant) and immunosuppression to prevent rejection, predisposing to complications, often compounded by comor-bidities from pre-existing diabetes.
The Diabetes Control and Complications Trial (1) showed that intensive insulin therapy (multiple injections per day with dose adjusted by frequent blood sugar determinations) decreased (although rarely normalized) glycosylated hemoglobin (HgbA1c) levels and reduced the rate of secondary complications (2). The threshold for totally eliminating the risks of secondary diabetic complications is perfect glycemic control, an objective that can be achieved by the most sophisticated exogenous insulin deliv-ery devices unfortunately at the cost of frequent hypoglycemic episodes. This may change in the future with real-time glucose monitoring systems combined with insulin pumps (3,4). Pan-creas transplantation induces insulin independence in diabetic recipients without the risk of hypoglycemia and can ameliorate secondary complications. With major advances in the manage-ment of pancreas transplantation, the success rate of pancreas transplants has progressively increased during the past two decades (5,6). Today’s recipients have a high probability of being insulin independent for years, if not indefinitely.
Historically, islet transplants have been less successful for a variety of reasons. In the late 1990s at the University of Alberta, insulin independence was achieved in several consec-utive recipients by sequential grafting of islets from multiple donors and the use of a steroid-free nondiabetogenic immuno-suppressive regimen (7). In another series from the University of Minnesota with a similar regimen, single-donor islet trans-plants induced insulin independence (8). In the Minnesota series, the donors had a high body mass index and the recipi-ents had a low body mass index. Thus, the net number of islets transplanted per unit weight was similar in the Alberta and Minnesota series. Islet transplants can succeed with stringent donor and recipient selections, but is not yet able to supersede pancreas transplants as the mainstay of β-cell replacement. Until islet transplants can consistently succeed from a single donor, regardless of size or recipient insulin requirements, an integrated approach is preferable (9): low-risk patients should undergo a surgically more challenging pancreas transplant, high-risk patients an islet transplant.
Although short-term islet graft survival appears promis-ing (even with single donors) (10), long-term graft function
after islet transplants (even with multiple donors) continues to be a major impediment to rapid progress. In the University of Alberta series, only 10% of islet transplant recipients were insulin independent at 5 years posttransplant (11).
The main tradeoff for recipients of β-cell allografts is the need for immunosuppression. A successful graft makes the recipient euglycemic and normalizes HgbA1c levels (11,12), but the combined risks of immunosuppression and pancreas trans-plant surgery must be weighed against the long-term risks of imperfect glycemic control and of development of secondary complications with exogenous insulin. A randomized prospec-tive trial has not been done to weigh these risks. The burden of day-to-day management of diabetes, with need for multiple needlesticks to inject insulin and monitor blood sugar levels tilts the balance in favor of a transplant for many diabetic patients. Furthermore, antirejection strategies are continually being developed to decrease the side effects of immunosup-pression. Nevertheless, only a few institutions perform pan-creas transplants soon after the onset of the disease (13).
The main indications for a pancreas transplant in patients with normal kidney function has been labile diabetes with frequent insulin reactions and hypoglycemic unawareness, a syndrome that may emerge years after the onset of diabe-tes, particularly in patients with autonomic neuropathy (14). However, even for nonlabile diabetic patients who attempt tight control by intensive glucose monitoring, literature shows a high rate of secondary complications that are just as mor-bid as (15), if not more so than, chronic immunosuppressive complications in organ allograft recipients (16,17). Thus, for a patient who wishes to avoid a lifetime of insulin injections and glucose monitoring and who prefers the risks of immu-nosuppressive complications to the secondary complications of diabetes, a pancreas transplant can be performed with good results (18). This also applies to type 2 diabetics who are obligatory insulin dependent. About 5% of pancreas trans-plants are performed in selected type 2 diabetics (19).
In the past, most pancreas transplant candidates had advanced diabetic nephropathy and required a kidney trans-plant also. As the risks of immunosuppression are assumed because of the kidney transplant, a simultaneous or sequential pancreas transplant does not pose any additional risks other than surgery (13). Indeed, pancreas transplants have been done in renal allograft recipients who meet the criteria for type 2 dia-betes with elimination of the need for exogenous insulin (20).
recIPIenT caTegorIes
Diabetic pancreas transplant candidates are divided into three categories: uremic (need a kidney transplant), posturemic (have a functioning kidney transplant), and nonuremic (do not need a kidney transplant). For candidates who are uremic, the options
LWBK1580_C73_p840-853.indd 840 31/07/17 5:40 PM

Chapter 73 Pancreatic transplantation 841
are to receive kidney and pancreas transplants either simultane-ously in one operation or sequentially in separate operations. The decision as to which option to take is usually based on the availability and suitability of living and cadaveric donors for one or both organs (5). Accordingly, there are three broad cat-egories of recipients: simultaneous pancreas–kidney (SPK), pan-creas after kidney (PAK), and pancreas transplants alone (PTA).
PK Transplants
Most SPK transplants have been done with both organs com-ing from the same cadaveric donor. Because a large number of patients are waiting for a kidney, unless priority is given to SPK candidates, waiting times tend to be long (years). Thus, to avoid two operations and a long wait, a simultaneous kidney and segmental pancreas transplant from a living donor can be done (20–22). Only a few centers offer this option (23,24). There has been a report from Japan of a successful islet transplantation from a live donor (25). Therefore, a simultaneous living-donor islet kidney transplant may become a viable option in the future (26,27). If a living donor is suitable for or only willing to give a kidney, another option is a simultaneous living-donor kidney and cadaveric pancreas transplant (23,24). For these options, the living kidney donor usually must be available on a moment’s notice (the same as for the recipient), as the cadaveric pancreas must be transplanted soon after procurement. Alter-natively, a recipient of a scheduled living-donor kidney trans-plant could also receive a cadaveric pancreas simultaneously if one became available fortuitously. If not, and only a kidney is transplanted, the recipient becomes a PAK candidate.
PAK Transplants
For nephropathic diabetic patients who have already under-gone a kidney transplant from a living or a cadaveric donor, a PAK transplant can be performed. Most PAK transplants today are done in patients who previously received a living-donor kidney because suitable uremic diabetic patients without a living donor will undergo a cadaveric pancreas transplant. Although a PAK means a uremic diabetic patient requires two operations to achieve both a dialysis-free and insulin-independent state, the two transplants done separately are smaller procedures than a combined transplant. The interval between the living-donor kidney and cadaveric pancreas trans-plant depends on several factors, including recipient recovery from the kidney transplant and donor availability, but the out-come is similar for all intervals more than 1 month. PAK is the largest pancreas transplant category at the University of Minnesota (28,29).
PTA Transplants
For recipients with adequate kidney function, a solitary pan-creas transplant can be performed from either a living or a cadaveric donor. Because the waiting time for a cadaveric pancreas is relatively short at the present time, living-donor pancreas transplants are done infrequently, but are particu-larly indicated if a candidate has a high panel-reactive anti-body and a negative cross-match to a living donor. Most PTA candidates have problems with glycemic control, hypoglyce-mic unawareness, and frequent insulin reactions. A successful PTA not only obviates these problems, but also improves the
quality of life, and may ameliorate secondary complications, thus increasing the applicability of PTA (28–30).
evoluTIon and ImProvemenTs
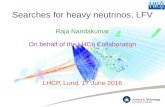
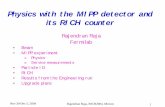
The first clinical pancreas transplant was performed at the Uni-versity of Minnesota in 1966 (31). The number of transplants remained low during the 1970s, but progressively increased in the 1980s, following the introduction of cyclosporine. By the end of 2014, almost 50,000 pancreas transplants had been performed in 55 countries around the world (Fig. 73.1), including almost 30,000 in the United States (Fig. 73.2) (6).
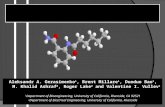
The history of pancreas transplants involves many different techniques and eras (32). The first series of pancreas trans-plants at the University of Minnesota used enteric drainage (ED) (32). Urinary drainage was first done into the ureter by Gliedman in the early 1970s (33,34), then via duct injection by Dubernard et al. (35) in 1974, and then via direct blad-der drainage (BD) by Sollinger et al. (36) in 1982. During the 1980s, BD became the predominant technique (Fig. 73.3) with good results (37). ED was still used (38), although spar-ingly, but since the late 1990s it has become the most frequent (Fig. 73.4) technique, especially in SPK transplants.
Venous drainage of the pancreas has also evolved over the years. Portal drainage was used with segmental grafts in the 1980s (32,39–42). For whole-organ pancreas transplants, systemic drainage was the norm until the 1990s, when por-tal drainage gained popularity, especially with ED (43,44), as opposed to BD (45). Between 1996 and 2000, about one-fifth of all SPKs used portal drainage, by anastomosis either to the recipient splenic vein (40) or, more commonly, to the superior mesenteric vein (Fig. 73.5) (46). Over the past decade, sys-temic drainage has reestablished itself as the most common technique (5,6).
Before techniques were developed to procure both liver and pancreas grafts with intact blood supply (47,48), seg-mental pancreas grafts were commonly used. Since the early 1990s, whole-organ pancreaticoduodenal grafts predominate (49), although segmental grafts are still used for living-donor pancreas transplants (28). The first living-donor pancreas transplant was performed at the University of Minnesota in 1979 (50). The early series of living-donor pancreas trans-plants consisted of solitary pancreases because the rejection rate of cadaveric pancreases was high (23). In the 1990s, living-donor pancreas transplants were predominantly per-formed in combination with a kidney from the same donor (Fig. 73.6) (22,51–53). Living-donor segmental pancreatec-tomy are now performed laparoscopically (54). Another approach, as previously mentioned, is to perform a living-donor kidney transplant simultaneously with a cadaveric pancreas transplant (24).
Immunosuppressive regimens have made great strides over the years. Today, there are more than 100 pancreas transplant centers in the United States (55). Some centers have reported extensive experience. For example, more than 1,000 SPK transplants have been performed at the University of Wiscon-sin (UW) (56), and more than 2,000 pancreas transplants of all categories have been performed at the University of Min-nesota (28). The International Pancreas Transplant Registry, formed in 1980, collects data from all centers in the world (57) and is the best resource for outcome analysis.
LWBK1580_C73_p840-853.indd 841 31/07/17 5:40 PM

842 SeCtion 7 OrgAn trAnsPlAntAtiOn
resulTs
Outcomes after pancreas transplants have consistently improved over the years (5,6). The latest report from the International Pancreas Transplant Registry (6) outlined recent results, focusing on U.S. transplants from 2009 through 2013, including more than 3,900 SPK, more than 500 PAK, and 389 PTA cases. Patient survival rates for all three categories was more than 95% at 1 year posttransplant (Fig. 73.7). Pri-mary pancreas graft survival rates at 1 year posttransplant were higher for SPK (88.9%) than for PAK (84.4%) and PTA
(81.5%) recipients (Fig. 73.8). Graft loss from rejection was low at 1 year in all three categories (1.7% SPK, 4.4% PAK, 5.5% PTA). In the majority of all transplants, ED was used for duct management, and of the ED transplants, portal venous drainage was used in about 20% of SPK and 10% of solitary transplants. Although overall graft function did not vary with ED or BD, the PTA group had a higher immunologic graft loss rate in ED versus BD cases. BD may result in earlier diagnosis of rejection because of the ability to monitor for a decline in urine amylase activity as a marker (28). Nevertheless, the late rejection rate is higher in the PTA than in other categories.
1,600
0
200
400
600
800
1,000
1,200
1,400
Transplant Year
USA n = 28,173
Non USA n = 19,164
pre 78
1981
1979
1983
1985
1987
1989
1991
1993
1995
1997
1999
2001
2003
2005
2007
2009
2011
2013
FIgure 73.1 number of pancreas transplants worldwide tabulated by the international Pancreas transplant registry from 1966 to 2013.
Cen
ters
0
200
400
600
800
1,000
1,200
1,400
1,600
0
20
40
60
80
100
120
140
160
Transplant Year
# Centers
# of Txs
Tran
splan
ts
19881990199219941996199820002002200420062008201020122014 FIgure 73.2 number of us transplant centers tab-
ulated by the international Pancreas transplant registry from 1966 to 2014. tx, transplant.
LWBK1580_C73_p840-853.indd 842 31/07/17 5:40 PM

Chapter 73 Pancreatic transplantation 843
who have developed secondary complications of diabetes. The progression of complications is halted by a functioning pan-creas graft. In fact, even an improvement in neuropathy has been documented (5,22,34,59,60). In addition to improve-ment in glomerular architecture, a recent study shows that interstitial expansion is reversible, and atrophic tubules can be reabsorbed (61). Advanced retinopathy and vascular dis-ease, however, are unaffected (62). Atherosclerotic risk factors decrease and endothelial function improves posttransplant (63). A pancreas transplant should be offered early, before the onset of complications of diabetes, to interested patients
Pancreas(graft)
Iliacartery(graft)
Iliacarteryandvein Bladder
Duodenum(graft)
Pancreasvessels
Iliacartery
FIgure 73.3 Bladder-drained (Bd) pancreaticoduodenal transplant alone (PtA) from a cadaver donor.
Recipientintestine
Entericanastamosis
Pancreas andduodenum
(graft)
Ureter
Kidneygraft
FIgure 73.5 enteric drainage (ed) simultaneous pancreas and kidney (sPk) transplants with portal venous drainage of the pancreas graft via the superior mesenteric vein.
FIgure 73.4 enteric-drained (ed) simultaneous pan-creas and kidney (sPk) transplant from a cadaver donor with systemic venous drainage.
IndIcaTIons and conTraIndIcaTIons
The indications for a pancreas transplant have evolved and expanded over the years as the results have improved. The position statement of the American Diabetes Association (58) on indications for a pancreas transplant (Table 73.1) is con-servative. A pancreas transplant is also indicated for patients
LWBK1580_C73_p840-853.indd 843 31/07/17 5:40 PM

844 SeCtion 7 OrgAn trAnsPlAntAtiOn
who understand the risk of immunosuppression versus the benefit of insulin independence and freedom from diabetic complications.
Contraindications include those for any other transplant, such as malignancy, active infections, noncompliance, serious psychosocial problems, and prohibitive cardiovascular risk. Candidates with advanced vascular disease have an increased risk of surgical complications, yet those who do well post-transplant greatly benefit from stabilization of their cardio-vascular risk.
Although it was clear that insulin-dependent recipients with renal failure benefited from a pancreas transplant in addition to the kidney, the survival benefit for pancreas trans-plant in patients with preserved renal function was questioned by at least one study (64). However, a more comprehensive reanalysis revealed that there was no increased mortality for solitary pancreas transplant recipients over wait-listed patients (65,66).
Tail of pancreas
Pancreatic duct
FIgure 73.6 simultaneous segmental pancreas and kidney transplant from a living donor (ld). either bladder drainage (Bd) or enteric drain-age (ed) can be used, but the Bd technique has a lower complication rate and is illustrated.
60
70
80
90
100
Transplant Year
1982
/83
1984
/85
1986
/87
1988
/89
1990
/91
1992
/93
1994
/95
1996
/97
1998
/99
2000
/01
2002
/03
2004
/05
2006
/07
2008
/09
2010
/11
2012
/13
PAK
PTA
SPK
%
Transplant Year
1982
/83
1980
/81
1984
/85
1986
/87
1988
/89
1990
/91
1992
/93
1994
/95
1996
/97
1998
/99
2000
/01
2002
/03
2004
/05
2006
/07
2008
/09
2010
/11
2012
/13
%
20
30
40
50
60
70
80
90
100
PAK
PTA
SPK Px
SPK Kd FIgure 73.8 Pancreas graft survival after primary deceased donor pancreas transplants in the united states from 1980 to 2013 by international Pancreas transplant registry. PAk, pancreas after kidney; PtA, pancreas transplant alone; sPk, simultaneous pancreas–kidney.
FIgure 73.7 Patient survival after primary deceased donor pancreas transplants in the united states from 1980 to 2013 by the international Pancreas transplant registry. PAk, pancreas after kidney; PtA, pancreas transplant alone; sPk, simultaneous pancreas–kidney.
LWBK1580_C73_p840-853.indd 844 31/07/17 5:40 PM

Chapter 73 Pancreatic transplantation 845
PreTransPlanT evaluaTIon
The pretransplant workup should include a detailed medical and psychosocial evaluation. Cardiac risk assessment is man-datory because diabetes is a major risk factor for coronary artery disease (CAD). Cardiologists vary on the type of test to screen for CAD in pretransplant diabetic patients. Coronary angiograms are performed in most candidates. Noninvasive tests are not very sensitive for CAD and poorly predictive for subsequent postoperative events in long-standing diabetic patients (67,68). With the use of iso-osmolar radio contrast, there does not seem to be an increased risk of contrast-induced nephropathy in patients with chronic kidney disease (69). In selected patients (i.e., young, healthy patients with short- duration diabetes), dobutamine stress echocardiograms are used for cardiac evaluation with good results (70). Once sig-nificant CAD is detected, aggressive treatment by revascular-ization, angioplasty, or stenting is recommended. In one study, revascularized transplant candidates had significantly fewer postoperative cardiac events, as compared with those who received medical therapy alone (71).
A detailed vascular examination must be done to rule out significant vascular insufficiency. If such insufficiency is found, it may need correction pretransplant because the transplant surgery, involving an anastomosis to the iliac artery, may fur-ther diminish lower-extremity blood flow. Pulmonary func-tion tests are indicated in chronic smokers and patients with a history of chronic pulmonary disease. Postoperative intensive care unit monitoring and perioperative bronchodilator therapy may be indicated in some patients. Liver function tests should be done to rule out hepatic insufficiency and viral hepatitis. The diagnosis of viral hepatitis (either B or C) is associated with worse long-term outcome after extrahepatic transplanta-tion (72). Abnormal liver function tests or the diagnosis of viral hepatitis should be followed up with a liver biopsy to rule out cirrhosis. The presence of cirrhosis is a contraindication for pancreas transplant. A gastrointestinal evaluation must be done to rule out autonomic dysfunction. Some immunosup-pressive medications may worsen gastrointestinal dysfunction. A prokinetic agent may be indicated to treat gastroparesis. A urologic examination is especially important for BD recipients because bladder dysfunction predisposes to graft pancreatitis.
deceased donor selecTIon
Pancreas donor selection criteria are not standardized, but instead vary from center to center. Absolute contraindica-tions are the obvious ones applied to most solid organs: active
hepatitis B, C, and non A–non B; human immunodeficiency virus; non–central nervous system (CNS) malignancy; surgi-cal or traumatic damage to the pancreas; history of diabetes mellitus; pancreatitis; and extremes of age (younger than 10 or older than 60 years). Prolonged intensive care unit stay and duration of brain death have been associated with an increased risk of graft failure (73). Other studies have shown that donor age is important; even middle-aged donors (older than 40 years) are associated with increased complications and graft failure (73–75). However, the so-called marginal donor organs are associated with good outcome if the pancreas, on inspec-tion, is found to be “healthy” in appearance (76,77).
Donors after cardiac death (DCD) are being used increas-ingly to expand the donor pool. However, there may be a higher rate of early organ dysfunction with these donors (78). A recent survey showed equivalent patient and graft survival at 1, 3, and 5 years in SPK transplant recipients from DCD compared with donors after brain death (78).
Pancreas PreservaTIon
UW solution was first used for pancreas preservation in a preclinical model in 1987 (79). As with most solid organs, in vivo flush followed by simple storage in cold UW solu-tion is the standard for pancreas preservation. In the original model, pancreases were preserved for up to 96 hours (80). In clinical transplantation, pancreas cold preservation exceeding 24 hours has been associated with increased graft dysfunction (81). Even when there is less than 24 hours, it has been shown that the longer the cold ischemia time, the greater the technical complication rate (82). Therefore, every effort should be made to minimize the cold ischemia time in order to optimize graft function and to lower complication rates. Recent data suggest a new method of preservation that may be advantageous: the two-layer method using UW solution and perfluorochemical (83). This method allows for longer preservation time while providing a mechanism for repair of ischemic damage due to cold storage (84–86). More clinical trials are needed before the two-layer method becomes routine.
Recently, histidine-tryptophan ketoglutarate solution has been increasingly used in pancreas transplantation (87). Advan-tages include lower viscosity, less potassium, and lower cost. Early outcome studies do not show inferiority compared to the more expensive UW solution (88,89).
Human leukocyTe anTIgen maTcHIng
The impact of human leukocyte antigen (HLA) matching on outcome varies. It is generally accepted that HLA matching has little effect on graft outcome for the SPK category (90,91), although higher rejection rates have been reported with poor matches (92–94). For solitary pancreas transplants (PAK and PTA), the data are mixed, ranging from studies show-ing no impact (95) to registry data showing that HLA A and B matches have a significant impact (91). At the University of Minnesota, SPKs are done regardless of HLA match; for PAKs, generally at least one antigen in the B locus matches, and for PTAs, at least one antigen in each of the A, B, and DR loci matches.
TABLE 73.1 Summary of American Diabetes Association (ADA) Recommendations for Indications for Pancreas Transplants
1. established end-stage renal disease (esrd) in patients who have had, or plan to have, a kidney transplant.
2. history of frequent, acute, and severe metabolic complications (e.g., hypoglycemia, hyperglycemia, ketoacidosis).
3. incapacitating clinical and emotional problems with exogenous insulin prescription.
4. Consistent failure of insulin-based management to prevent acute complications.
LWBK1580_C73_p840-853.indd 845 31/07/17 5:40 PM

846 SeCtion 7 OrgAn trAnsPlAntAtiOn
anesTHeTIc consIderaTIons
A patient with brittle diabetes and secondary complications (e.g., CAD, autonomic neuropathy) can pose special prob-lems for the anesthesiologist. Dysautonomic response to drugs or hypoxia can lead to significant morbidity and even death (96). It has also been documented that long-standing diabe-tes poses a challenge to the anesthesiologist during intubation (97). Awareness of these risks and employment of an expe-rienced anesthesiology team might help decrease the risks or morbidity. A major operation such as a pancreas transplant or combined kidney–pancreas transplant is often prolonged and can be associated with significant blood loss. Prompt replacement with blood or colloids should be instituted to avoid hypoperfusion after significant blood loss. Before and after revascularization of the pancreas, careful blood glucose monitoring, along with continuous intravenous (IV) insulin therapy to maintain tight control of blood glucose levels, is essential. Perioperative β-blockade should be considered for long-standing diabetic patients with a cardiac history.
Back-TaBle PreParaTIon oF THe donor Pancreas
Once the donor pancreas has been opened in the recipient operating room, some back-table work is necessary to prepare it for the transplant, including these steps (98):
1. Donor splenectomy (taking care to avoid injury to the pancreatic tail)
2. Trimming down of the donor duodenum to the shortest length without damage to the main or accessory duct (especially important with BD to minimize bicarbonate loss)
3. Oversewing or individual vessel ligation of the meso-colic and mesenteric stumps on the anterior aspect of the pancreas
4. Excision of lymphatic and ganglionic tissue in the peri-portal area
5. Reconstruction of the splenic and superior mesenteric arteries with a Y graft of the donor iliac A bifurca-tion (to provide for a single arterial anastomosis in the recipient).
recIPIenT oPeraTIon
Several techniques have been described for the recipient opera-tion (32,99). The techniques vary based on whether a solitary pancreas transplant (PTA, PAK) or a combined transplant (SPK) is done.
Solitary Pancreas Transplant
Choice of Exocrine Secretion of the Pancreas—Drainage of Bowel or Bladder?
Currently, for pancreas transplants in the United States, 86% of PAK, 79% of PTA, and 87% of SPK transplants are drained enterically (5,6). ED is more physiologic and does away with the complications of BD (e.g., acidosis, pancreatitis, urinary
infections, hematuria). Between 10% and 20% of BD recipi-ents are ultimately converted to ED because of such complica-tions once they are 6 to 12 months posttransplant and their rejection risk is lower. BD, however, allows for direct measure-ment of urinary amylase as a marker of exocrine function. A decrease in urine amylase is sensitive, but not very specific, for acute rejection of the pancreas (100,101). Hyperglycemia is a late event in the rejection, and a decrease in urine amy-lase occurs early. Thus, rejection episodes are detected early with BD, and the rejection loss rate is lower with BD than with other techniques (55). In clinical practice, the choice of exocrine drainage varies. Some groups always use ED, while some always use BD (101,102). Others base it on the indi-vidual recipient’s immunologic risk versus the risk of urologic complications (28). The surgical risks and short-term outcome with both techniques are comparable (74,103). ED is likely to predominate as the major technique in the future as immuno-logic strategies to eliminate rejection are developed (102).
Choice of Venous Drainage—Portal or Systemic?
Currently in the United States, of all ED transplants, 20% of SPK, 10% of PAK, and 12% of PTA cases are drained to the por-tal vein (5,6). Portal drainage is more physiologic than systemic drainage (104,105). Theoretically, portal drainage preserves the first-pass metabolism of insulin in the liver. Therefore, portally drained recipients will have lower systemic insulin levels (106). However, there is no evidence of any detrimental effect on lipid levels (107) or on risk of vascular disease (62) as seen in de novo hyperinsulinemia (syndrome X). Portal venous drainage is difficult to perform with exocrine BD (45). Portal drainage had gained in popularity after initial reports that rejection rates are lower in this category (103,108). It appears, however, based on registry data (5,6) that the immunologic advantage is much smaller than initially found. Recent modifications include a retroperitoneal portal-ED technique (109).
Transplantation Portion—Whole Organ or a Segment?
Almost all cadaveric pancreas transplants performed today use whole-organ grafts. Segmental grafts have little role to play in this group, except when a rare anatomic abnormality is noted such that the head of the pancreas cannot be used. A rare instance of a split cadaveric pancreas transplanted into two different recipients has been described (110). All living-donor pancreas transplants use segmental grafts (body and tail); doing so maintains normoglycemia in the recipient (12).
Simultaneous Pancreas–Kidney
SPK transplants have a lower rejection rate than do solitary pancreases. Further, rejection episodes are rarely isolated to the pancreas alone. Most pancreas rejection episodes can be indirectly detected by monitoring serum creatinine as a marker for kidney rejection. Therefore, most SPK transplants are done using ED, as advocated by the Stockholm group (111) (Fig. 73.5). With ED, the risk of acute technical complications is slightly higher, but the chronic complication rate is lower (112). Choice of venous drainage varies by center. Because ED is the choice for exocrine drainage, there is no impediment to performing portal venous drainage.
LWBK1580_C73_p840-853.indd 846 31/07/17 5:40 PM

Chapter 73 Pancreatic transplantation 847
PosToPeraTIve care
After an uncomplicated pancreas transplant, the recipient is transferred to the postanesthesia care unit (PACU) or the surgical intensive care unit (SICU). Centers that have a spe-cialized monitored transplant unit (with central venous and arterial monitoring capabilities) transition the postoperative recipients through the PACU to the transplant unit. Others transfer directly to the SICU for the first 24 to 48 hours. Care during the first few hours after transplant is similar to care after any major operative procedure. Careful monitoring of vital signs, central venous pressure, oxygen saturation, and hematologic and laboratory parameters is crucial. The fac-tors below are unique to pancreas recipients and should be attended to.
Blood Glucose Levels
Any sudden, unexplained increase in glucose levels should raise the suspicion of graft thrombosis. An immediate ultra-sound examination must be done to assess blood flow to the graft. Maintenance of tight glucose control (<150 mg/dL) using an IV insulin drip is important to “rest” the pancreas in the early postoperative period.
Intravascular Volume
Because the pancreas is a “low-flow” organ, intravascular volume must be maintained to provide adequate perfusion to the graft. Central venous pressure monitoring is used to monitor intravascular volume status. In some cases, such as patients with depressed cardiac function, pulmonary artery catheter monitoring may be required during the first 24 to 48 hours. If the hypovolemia is associated with low hemo-globin levels, then washed packed red blood cell transfusions should be given. Otherwise, colloid or crystalloid replacement can be used.
Maintenance IV Fluid Therapy
The choice of IV fluid is usually 5% dextrose in 0.45% saline solution. The use of dextrose is not contraindicated and may be of benefit, as long as IV insulin is used to maintain good blood glucose control. In SPK recipients, whose IV rate is based on urine output, dextrose should be eliminated if the urine output is high (>500 mL/hr). Maintenance solution for BD recipients should include 10 mEq of HCO3 added to each liter to account for the excess HCO3 loss (113,114); sodium lactate can be used as an alternative (115).
Antibiotic Therapy
Broad-spectrum antibiotic therapy (with strong gram-negative coverage) and antifungal therapy are instituted before the inci-sion is made in the operating room, then continued for 3 (for antibiotics) and 7 days (for antifungal). At the University of Minnesota, since the introduction of this protocol, we have noted a decrease in postoperative abdominal infections (74). Cytomegalovirus (CMV) and antiviral prophylaxis are similar to that for other solid organs.
Octreotide
The use of octreotide in pancreas recipients helps reduce the incidence of technical complications (116). This benefit should be weighed against evidence from rat studies that shows decreased pancreatic islet blood flow with octreotide use (117), although clinically no detrimental effects of octreotide use have been documented. A dose of 100 to 150 μg IV or sub-cutaneously three times a day is administered for 5 days post-transplant. Dose adjustments may be made for nausea, which is the predominant side effect.
Anticoagulation
The use of low-dose heparin in the early postoperative period (days 0 to 5) decreases the risk of graft thrombosis (118). An intraoperative dose of 70 units/kg is given, followed by an IV infusion of 3 units/kg started at 4 hours postoperatively and gradually increased up to 7 units/kg (depending on hemody-namic stability and hemoglobin levels). Enteric-coated aspi-rin (80 mg) is started on day 1 and continued for 6 months. At the University of Minnesota, this protocol decreased the thrombosis rate from about 12% to 6%, but increased the relaparotomy rate due to bleeding from 4% to 6%. Segmen-tal pancreas transplants (as in living-donor transplants) have a higher thrombosis risk and therefore therapeutic heparin-ization (with a target-activated partial thromboplastin time [aPTT] of 50 seconds) for 5 days and Coumadin therapy (with a target international normalized ratio [INR] of 2 to 2.5) are recommended for 6 months. The higher risk of thrombosis is due to the smaller vessels in a segmental graft (119,120).
ImmunosuPPressIon
Immunosuppression is essential to thwart rejection in all allo-transplant recipients (17). Before the advent of cyclosporine in the early 1980s (121), azathioprine and prednisone were the mainstays of immunosuppression. From the early 1980s to the mid-1990s, cyclosporine was added to the mix and resulted in significant improvement in immunologic outcomes (122). Since the mid-1990s, tacrolimus and mycophenolate mofetil have replaced cyclosporine and azathioprine as the main drugs, resulting in even better pancreas graft survival rates (122–124). In addition, steroids have been successfully with-drawn from some pancreas recipients (125) and, in some cases, avoided (126). With a recently introduced drug, rapamycin, used in combination with tacrolimus, steroids have been suc-cessfully avoided in some pancreas recipients (127,128).
Anti–T-cell therapy has always remained a part of the induc-tion protocol for pancreas recipients. With the recent emphasis on steroid withdrawal or avoidance, anti–T-cell therapy has taken on added importance to avoid rejection. Anti-CD25 antibodies are also used frequently as induction therapy (129). Avoidance of calcineurin inhibitors has been attempted in pan-creas transplantation. When combined with steroid avoidance, this required prolonged anti–T-cell therapy, which increases the risk of infection without adequately controlling rejection (130). Table 73.2 presents the immunosuppressive protocol for pan-creas transplant recipients at the University of Minnesota.
For PTA recipients, whose rejection rates are the high-est of all categories, pretransplant immunosuppression has decreased rejection rates and graft loss from rejection (31).
LWBK1580_C73_p840-853.indd 847 31/07/17 5:40 PM

848 SeCtion 7 OrgAn trAnsPlAntAtiOn
Heavy use of immunosuppression may increase the infection rate, but effective antimicrobial prophylaxis has helped ame-liorate this problem (131,132).
InTravenous ImmunogloBulIn and PlasmaPHeresIs
IV immunoglobulin has many applications in transplantation. It has been used successfully to decrease anti-HLA antibod-ies in transplant recipients on the waiting list and to shorten their waiting times (133,134). It can also be used to control acute humoral rejection in kidney and heart allograft recipi-ents (135). Plasmapheresis has been used to decrease humoral antibody titers in ABO-incompatible liver and kidney recipi-ents (136,137). It has also been used to control hyperacute and accelerated acute rejection in positive cross-match kidney recip-ients (138,139) and lung (140) recipients. At the University of Minnesota, for ABO-incompatible (A2 to O, B, or AB) or posi-tive cross-match (T-cell) pancreas recipients, the treatment pro-tocol consists of intraoperative IV immunoglobulin (0.5 mg/kg) followed by a course of 5 to 7 days in combination with daily plasmapheresis. For B-cell positive cross-match recipients, IV immunoglobulin may be used without plasmapheresis.
surgIcal comPlIcaTIons
Bleeding
Postoperative bleeding is a frequent reason for early relaparot-omy in pancreas recipients. The incidence ranges from 6% to 8% (74,141). This risk is increased by the use of anticoagulation
in the immediate postoperative period. Frequent physical examinations and monitoring of hemoglobin help detect bleed-ing early. Heparin may be temporarily suspended to stabilize the patient. If bleeding continues, early operative intervention is indicated. If bleeding stops or slows down, heparin should be restarted at a lower rate and judiciously increased as tolerated.
Thrombosis
The incidence of thrombosis posttransplant ranges from 5% to 13% (118,141). The risk is increased after segmental pancreas transplants because of the small caliber of vessels (51). Most thromboses are due to technical reasons. A short portal vein (requiring an extension graft) or atherosclerotic arteries in the pancreas graft increases the risk for thrombosis. In the recipient, a narrow pelvic inlet with a deeply placed iliac vein, atheroscle-rotic disease of the iliac artery, a technically difficult vascular anastomosis, kinking of the vein by the pancreas graft, signifi-cant hematoma formation around the vascular anastomosis, and a hypercoagulable state are some of the factors that increase the risk for thrombosis. The most common form of hypercoagulable state is factor V Leiden mutation in the Western population. The incidence ranges from 2% to 5% but may be as high as 50% to 60% in patients with a history (self or family) of thrombosis (142). Other causes of hypercoagulable state include antithrom-bin deficiency, protein C or S deficiency, activated protein C resistance, and anticardiolipin antibodies (143).
Duodenal Leaks
The incidence of duodenal leaks ranges from 4% to 6% (74,141). A leak from the anastomosis of the duodenum to the bowel almost always leads to a relaparotomy. Gross
TABLE 73.2 University of Minnesota Standard Immunosuppression Pancreas Program
SPK PAK and SPLK PTA Rejection
Antithymocyte globulin1.25 mg/kga5 dosesFirst dose intraoperativegive methylprednisolone 500 mg,
250 mg, and 100 mg before first, second, and third doses, respectively
Antithymocyte globulin1.25 mg/kga7 dosesFirst dose intraoperativegive methylprednisolone
500 mg, 250 mg, and 100 mg before first, second, and third doses, respectively
Antithymocyte globulin1.25 mg/kga7–10 dosesFirst dose intraoperativegive methylprednisolone
500 mg, 250 mg, and 100 mg before first, second, and third doses, respectively
Methylprednisoloneday #0: 500 mg ivday #1: 250 mg ivday #2: 125 mg iv
Antithymocyte globulin1.25 mg/kg iva × 5–7 dgive premedicationmonitor AlC
Resistant rejection
Tacrolimus2 mg orally, twice dailystart when creatinine less than
3 mg/dl or postoperative day #5, whichever is later
if tacrolimus is delayed continue tmg until tacrolimus levels are therapeutic
levels 8–10 ng/ml for 3 mo, then 5–8 ng/ml
Tacrolimus2 mg orally, twice dailystart postoperativeif tacrolimus is delayed con-
tinue tmg until tacrolimus levels are therapeutic
levels 8–10 ng/ml for 3 mo, then 5–8 ng/ml
Tacrolimus2 mg orally, twice dailystart postoperativeif tacrolimus is delayed con-
tinue tmg until tacrolimus levels are therapeutic
levels 8–10 ng/ml for 3 mo, then 5–8 ng/ml
Mycophenolatestart postoperative1 g orally, twice daily
Mycophenolatestart postoperative1 g orally, twice daily
Mycophenolatestart postoperative1 g orally, twice daily
Note: kidney rejections on the kidney steroid avoidance study should be treated with Alg, Atg, or other antibody preparations
sPk, simultaneous pancreas kidney; PAk, pancreas after kidney; sPlk, simultaneous cadaver pancreas living-donor kidney; tmg, antithymocyte globulin; AlC, absolute lymphocyte count; mo, month.
around up antithymocyte globulin dose to the nearest 25.ALC levels: if zero, hold antithymocyte globulin; if 0.1 give half-dose antithymocyte globulin; if 0.2 or above give full dose.Antithymocyte globulin and other antibody preparations require “premedication.”
LWBK1580_C73_p840-853.indd 848 31/07/17 5:40 PM

Chapter 73 Pancreatic transplantation 849
peritoneal contamination due to an enteric leak necessitates a graft pancreatectomy. The diagnosis is made by elevated pan-creatic enzymes associated with acute abdomen. The differ-ential diagnosis is pancreatitis, abdominal infection, or acute severe rejection. A Roux-en-Y anastomosis to the pancreatic duodenum may be preferred if the risk of leak is thought to be increased during intraoperative inspection of the pancreas. Other novel techniques such as a venting jejunostomy (Roux-en-Y) have been used in selected recipients (144). Duodenal leaks in BD recipients are usually managed nonoperatively with prolonged catheter decompression of the urinary blad-der. The diagnosis is made using plain or computed tomogra-phy (CT) cystography. The size and extent of the leak cannot always be assessed by the imaging studies. Large leaks may require operative intervention, such as a repair or enteric conversion (145).
Major Intra-Abdominal Infections
The incidence of intra-abdominal infections requiring reopera-tion ranges from 4% to 10% (74,141). Opening the duodenal segment intraoperatively, with associated contamination, pre-disposes to this high rate; fungal and gram-negative infections predominate. With the advent of advanced interventional radiologic procedures to drain intra-abdominal abscesses, the incidence of reoperations is fast decreasing. If the infec-tion is uncontrolled or widespread, then graft pancreatectomy followed by frequent washouts may be necessary.
Renal Pedicle Torsion
Torsion of the kidney has been reported after the SPK trans-plants (146,147). The intraperitoneal location of the kidney (allowing for more mobility) predisposes to this complication. Additional risk factors are a long renal pedicle (>5 cm) and a marked discrepancy between the length of artery and vein. Prophylactic nephropexy to the anterior or lateral abdominal wall is recommended in intraperitoneal transplants to avoid this problem.
Others
Other surgical complications that may require laparotomy also decreased from 9% to 1%. Improved anti-infective prophylaxis, surgical techniques, immunosuppression, and advances in interventional radiology have all contributed to this disease (74).
nonsurgIcal comPlIcaTIons
Pancreatitis
The incidence of posttransplant pancreatitis varies based on the type of exocrine drainage. BD recipients with abnormal bladder function are at increased risk secondary to incomplete bladder emptying or urine retention causing resistance to the flow of pancreatic exocrine secretions. Other causes of pancre-atitis include drugs (corticosteroids, azathioprine, cyclospo-rine), hypercalcemia, viral infections (CMV or hepatitis C), and reperfusion injury after prolonged ischemia. Pancreatitis is usually manifested by an increase in serum amylase and lipase
with or without local signs of inflammation. The treatment usually consists of catheter decompression of the bladder for a period of 2 to 6 weeks, depending on the severity. In addi-tion, octreotide therapy may be used to decrease pancreatic secretions. The underlying urologic problem, if any, should be treated. If repeated episodes of pancreatitis occur, an enteric conversion of exocrine drainage may be indicated (148–150).
Rejection
The incidence of rejection is discussed in the Results section earlier in this chapter. The diagnosis is usually based on an increase in serum amylase and lipase and a decrease in urine amylase in BD recipients. A sustained significant drop in uri-nary amylase from baseline should prompt a pancreas biopsy to rule out rejection (151). In ED recipients, one has to rely on serum amylase and lipase only. A rise in serum lipase has recently shown to correlate well with acute pancreas rejec-tion (149). Other signs and symptoms include tenderness over the graft, unexplained fever, and hyperglycemia (usually a late finding). Diagnosis can be confirmed by a percutaneous pancreas biopsy (152–154). In cases in which percutaneous biopsy is not possible due to technical reasons, empiric ther-apy may be started. Rarely, open biopsy is indicated. Transcys-toscopic biopsy, which was used in the past, has been largely abandoned.
Others
Other findings include infectious complications such as CMV, hepatitis C, extra-abdominal bacterial or fungal infections, posttransplant malignancy such as posttransplant lympho-proliferative disorder, and other rare complications such as graft-versus-host disease that occur in pancreas transplanta-tion. The diagnosis and management of these complications are similar to those of other solid-organ transplants.
FuTure dIrecTIons
In diabetic patients with kidney dysfunction, SPK or PAK trans-plant is the standard of care. A PTA, however, is less common because the long-term risks of diabetes are pitted against the long-term risks of immunosuppression. A successful transplant can improve existing neuropathy (62) in diabetic recipients, and the survival after a solitary pancreas transplant is better than remaining on the waiting list (65). As the risks of immunosup-pression decrease with novel methods of tolerance and immu-nomodulation (102), the balance will tilt in favor of an early transplant. The limiting factor will then be the organ shortage, which could be alleviated if xenotransplantation is able to over-come its current barrier of hyperacute rejection (155).
The application of islet transplants is rapidly growing. Recent successes (7,8) suggest that islet transplants can pro-vide all the benefits of pancreas transplants without the risks of major surgery. Xenotransplantation of islets may be more readily achievable using encapsulation (156) than with other organs. Prolonged diabetes reversal after intraportal xenotrans-plant in primates has been documented (157) and may pave the way for human xenotransplant trials. Also, stem cells that are manipulated to differentiate into islets may provide a rich sup-ply for transplantation (158). Islet transplants can be combined
LWBK1580_C73_p840-853.indd 849 31/07/17 5:40 PM

850 SeCtion 7 OrgAn trAnsPlAntAtiOn
with immunomodulation and tolerogenic strategies to minimize or avoid immunosuppression (159). This combination would provide for minimally invasive cellular (islet) transplants for all type 1 diabetic patients without the need for long-term immu-nosuppression. But unless the results of clinical islet transplanta-tion continue to substantially improve, pancreas transplantation remains the best treatment option long-term for (labile) type 1 diabetic patients with or without uremia.
14. Gruessner RW, Sutherland DE, Najarian JS, et al. Solitary pancreas trans-plantation for nonuremic patients with labile insulin-dependent diabetes mellitus. Transplantation. 1997;64:1572–1577.
15. Krolewski AS, Warram JH, Freire MB. Epidemiology of late diabetic com-plications: a basis for the development and evaluation of preventive pro-grams. Endocrinol Metab Clin North Am. 1996;25:217–242.
16. Syndman DR. Infection in solid organ transplantation. Transplant Infect Dis. 1999;1:21–28.
17. First MR. Immunosuppressive agents and their actions. Transplant Proc. 2002;34:1369–1371.
18. Gruessner RW, Sutherland DE, Kandaswamy R, Gruessner AC. Over 500 solitary pancreas transplants in nonuremic patients with brittle diabetes mellitus. Transplantation. 2008;85:42–47.
19. Nath DS, Gruessner AC, Kandaswamy R, et al. Outcomes of pancreas transplants for patients with type 2 diabetes mellitus. Clin Transplant. 2005;19:792–797.
20. Light JA, Sasaki TM, Currier CB, Barhyte DY. Successful long-term kid-ney-pancreas transplants regardless of C-peptide status or race. Transplan-tation. 2001;71:152–154.
21. Benedetti E, Dunn T, Massad MG, et al. Successful living related simulta-neous pancreas-kidney transplant between identical twins. Transplanta-tion. 1999;67:915–918.
22. Gruessner RW, Kendall DM, Drangstveit MB, et al. Simultaneous pan-creas-kidney transplantation from live donors. Ann Surg. 1997;226:471–480 discussion 480–482.
23. Sutherland DE, Gores PF, Farney AC, et al. Evolution of kidney, pancreas, and islet transplantation for patients with diabetes at the University of Minnesota. Am J Surg. 1993;166:456–491.
24. Farney AC, Cho E, Schweitzer EJ, et al. Simultaneous cadaver pancreas living-donor kidney transplantation: a new approach for the type 1 dia-betic uremic patient. Ann Surg. 2000;232:696–703.
25. Matsumoto S, Okitsu T, Iwanaga Y, et al. Insulin independence after living-donor distal pancreatectomy and islet allotransplantation. Lancet. 2005;365:1642–1644.
26. Matsumoto S, Okitsu T, Iwanaga Y, et al. Follow-up study of the first successful living donor islet transplantation. Transplantation. 2006;82: 1629–1633.
27. Iwanaga Y, Matsumoto S, Okitsu T, et al. Living donor islet transplanta-tion, the alternative approach to overcome the obstacles limiting trans-plant. Ann N Y Acad Sci. 2006;1079:335–339.
28. Sutherland DE, Gruessner RW, Dunn DL, et al. Lessons learned from more than 1,000 pancreas transplants at a single institution. Ann Surg. 2001;233:463–501.
29. Gruessner AC, Sutherland DE, Dunn DL, et al. Pancreas after kidney transplants in posturemic patients with type I diabetes mellitus. J Am Soc Nephrol. 2001;12:2490–2499.
30. Gruessner RW, Gruessner AC. Pancreas transplant alone: a procedure coming of age. Diabetes Care. 2013;36:2440–2447.
31. Kelly WD, Lillehei RC, Merkel FK, et al. Allotransplantation of the pancreas and duodenum along with the kidney in diabetic nephropathy. Surgery. 1967;61:827–837.
32. Gruessner RWG. Recipient procedures. In: Gruessner RW, Sutherland DE, eds. Transplantation of the Pancreas. New York: Springer-Verlag; 2004:150–178.
33. Gold M, Whittaker JR, Veith FJ, Gliedman ML. Evaluation of ureteral drainage for pancreatic exocrine secretion. Surg Forum. 1972;23:375–377.
34. Gliedman ML, Natale DL, Riflan H, et al. Clinical segmental pancreatic transplantation with ureter-to-pancreatic duct anastomosis for exocrine drainage. Bull Soc Int Chir. 1975;34:15–20.
35. Dubernard JM, Traeger J, Neyra P, et al. A new method of preparation of segmental pancreatic grafts for transplantation: trials in dogs and in man. Surgery. 1978;84:633–639.
36. Sollinger HW, Cook K, Kamps D, et al. Clinical and experimental experi-ence with pancreaticocystostomy for exocrine pancreatic drainage in pan-creas transplantation. Transplant Proc. 1984;16:749–751.
37. Nghiem DD, Corry RJ. Technique of simultaneous renal pancreatoduo-denal transplantation with urinary drainage of pancreatic secretion. Am J Surg. 1987;153:405–406.
38. Groth CG, Collste H, Lundgren G, et al. Successful outcome of segmen-tal human pancreatic transplantation with enteric exocrine diversion after modifications in technique. Lancet. 1982;2:522–524.
39. Calne RY. Paratopic segmental pancreas grafting: a technique with portal venous drainage. Lancet. 1984;1:595–597.
40. Gil-Vernet JM, Fernandez-Cruz L, Caralps A, et al. Whole organ and pancreaticoureterostomy in clinical pancreas transplantation. Transplant Proc. 1985;17:2019–2022.
1. Pancreas transplantation remains the most reliable treatment option for insulin-dependent patients with diabetes that offers freedom from insulin administra-tion long-term and achieves normoglycemia.
2. Pancreas transplantation can hold or even reverse some of the secondary complications of diabetes mellitus.
3. Pancreas transplants can be performed in (a) nonuremic, brittle diabetic patients, (b) uremic diabetic patients, and (c) posturemic diabetic patients who underwent a previ-ous kidney transplant.
4. One-year patient survival rates after pancreas trans-plantation are over 95%, graft survival rates are above 80%.
5. Quality of life is markedly improved in previously dia-betic patients after successful pancreas transplantation.
6. Graft loss from technical or immunologic complica-tions is less than 5% each at 1 year.
key Points
References 1. The effect of intensive treatment of diabetes on the development and pro-
gression of long-term complications in insulin-dependent diabetes melli-tus. The Diabetes Control and Complications Trial Research Group. N Engl J Med. 1993;329:977–986.
2. Lifetime benefits and costs of intensive therapy as practiced in the diabetes control and complications trial. The Diabetes Control and Complications Trial Research Group. JAMA. 1997;277:372.
3. Diabetes Research in Children Network (DirecNet) Study Group, Buck-ingham B, Beck RW, et al. Continuous glucose monitoring in children with type 1 diabetes. J Pediatr. 2007;151:388–393.
4. Cobry E, Chase HP, Burdick P, et al. Use of CoZmonitor in youth with type 1 diabetes. Pediatr Diabetes. 2008;9:148–151.
5. Gruessner RW, Gruessner AC. The current state of pancreas transplanta-tion. Nat Rev Endocrinol. 2013;9:555–562.
6. Gruessner AC, Gruessner RW. Pancreas transplant outcomes for United Stated and non United States cases as reported to the United Network for Organ Sharing and the International Pancreas Transplant Registry as of December 2011. Clin Transpl. 2012:23–40.
7. Shapiro AM, Lakey JR, Ryan EA, et al. Islet transplantation in seven patients with type 1 diabetes mellitus using a glucocorticoid-free immuno-suppressive regimen. N Engl J Med. 2000;343:230–238.
8. Hering BJ, Kandaswamy R, Harmon J. Insulin independence after single-donor islet transplantation in type I diabetes with hOKT3–1 (ala-ala), siro-limus, and tacrolimus therapy. Am J Transplant. 2001;1:180.
9. Gruessner RW, Gruessner AC. What defines success in pancreas and islet transplantation:insulin independence or prevention of hypoglycemia. Transplant Proc. 2014;46:1898–1899.
10. Hering BJ, Kandaswamy R, Ansite JD, et al. Single-donor, marginal-dose islet transplantation in patients with type 1 diabetes. JAMA. 2005; 293:830–835.
11. Ryan EA, Paty BW, Senior PA, et al. Five-year follow-up after clinical islet transplantation. Diabetes. 2005;54:2060–2069.
12. Gruessner AC, Sutherland DE, Gruessner RW. Long-term outcome after pancreas transplantation. Curr Opin Organ Transplant. 2012;17:100–105.
13. Sutherland DE, Stratta RJ, Gruessner AC. Pancreas transplant outcome by recipient category: single pancreas versus combined kidney-pancreas. Curr Opin Organ Transplant. 1998;3:231–241.
LWBK1580_C73_p840-853.indd 850 31/07/17 5:40 PM

Chapter 73 Pancreatic transplantation 851
41. Sutherland DE, Goetz FC, Moudry KC, et al. Use of recipient mesenteric vessels for revascularization of segmental pancreas grafts: technical and metabolic considerations. Transplant Proc. 1987;19:2300–2304.
42. Tyden G, Lundgren G, Ostman J. Grafted pancreas with portal venous drainage. Lancet. 1984;1:964–965.
43. Rosenlof LK, Earnhardt RC, Pruett TL, et al. Pancreas transplantation. An initial experience with systemic and portal drainage of pancreatic allografts. Ann Surg. 1992;215:586–595; discussion 596–597.
44. Shokouh-Amiri MH, Gaber AO, Gaber LW, et al. Pancreas transplanta-tion with portal venous drainage and enteric exocrine diversion: a new technique. Transplant Proc. 1992;24:776–777.
45. Muhlbacher F, Gnant MF, Auinger M, et al. Pancreatic venous drainage to the portal vein: a new method in human pancreas transplantation. Trans-plant Proc. 1990;22:636–637.
46. Gaber AO, Shokouh-Amiri MH, Hathaway DK, et al. Results of pan-creas transplantation with portal venous and enteric drainage. Ann Surg. 1995;221:613–622; discussion 622–624.
47. Marsh CL, Perkins JD, Sutherland DE, et al. Combined hepatic and pan-creaticoduodenal procurement for transplantation. Surg Gynecol Obstet. 1989;168:254–258.
48. Delmonico FL, Jenkins RL, Auchincloss H Jr, et al. Procurement of a whole pancreas and liver from the same cadaveric donor. Surgery. 1989; 105:718–723.
49. Stratta RJ, Taylor RJ, Gill IS. Pancreas transplantation: a managed cure approach to diabetes. Curr Probl Surg. 1996;33:709–808.
50. Sutherland DE, Goetz FC, Najarian JS. Living-related donor segmental pancreatectomy for transplantation. Transplant Proc. 1980;12:19–25.
51. Gruessner RW, Sutherland DE. Simultaneous kidney and segmental pan-creas transplants from living related donors: the first two successful cases. Transplantation. 1996;61:1265–1268.
52. Sutherland DE, Najarian JS, Gruessner R. Living versus cadaver donor pancreas transplants. Transplant Proc. 1998;30:2264–2266.
53. Gruessner RW, Sutherland DE, Drangstveit MB, et al. Pancreas trans-plants from living donors: short- and long-term outcome. Transplant Proc. 2001;33:819–820.
54. Gruessner RW, Kandaswamy R, Denny R. Laparoscopic simultaneous nephrectomy and distal pancreatectomy from a live donor. J Am Coll Surg. 2001;193:333–337.
55. Gruessner AC, Sutherland DE. Pancreas transplant outcomes for United States (US) and non-US cases as reported to the United Network for Organ Sharing (UNOS) and the International Pancreas Transplant Reg-istry (IPTR) as of October 2002. In: Cecka JM, Terasaki PI, eds. Clinical Transplants 2002. Los Angeles: UCLA Immunogenetics Center; 2003.
56. Sollinger HW, Odorico JS, Knechtle SJ, et al. Experience with 500 simulta-neous pancreas-kidney transplants. Ann Surg. 1998;228:284–296.
57. Sutherland DE. International human pancreas and islet transplant registry. Transplant Proc. 1980;12(4 Suppl 2):229–236.
58. Pancreas transplantation for patients with type 1 diabetes: American Dia-betes Association. Diabetes Care. 2000;23:117.
59. Kennedy WR, Navarro X, Goetz FC, et al. Effects of pancreatic transplan-tation on diabetic neuropathy. N Engl J Med. 1990;322:1031–1037.
60. Solders G, Tyden G, Persson A, Groth CG. Improvement of nerve con-duction in diabetic neuropathy: a follow-up study 4 yr after combined pancreatic and renal transplantation. Diabetes. 1992;41:946–951.
61. Fioretto P, Sutherland DE, Najafian B, Mauer M. Remodeling of renal interstitial and tubular lesions in pancreas transplant recipients. Kidney Int. 2006;69:907–912.
62. Stratta RJ. Impact of pancreas transplantation on complications of diabe-tes. Curr Opin Organ Transplant. 1998;3:258–273.
63. Fiorina P, La Rocca E, Venturini M, et al. Effects of kidney-pancreas transplantation on atherosclerotic risk factors and endothelial function in patients with uremia and type 1 diabetes. Diabetes. 2001;50:496–501.
64. Venstrom JM, McBride MA, Rother KI, et al. Survival after pancreas transplantation in patients with diabetes and preserved kidney function. JAMA. 2003;290:2817–2823.
65. Gruessner RW, Sutherland DE, Gruessner AC. Mortality assessment for pancreas transplants. Am J Transplant. 2004;4:2018–2026.
66. Gruessner RW, Sutherland DE, Gruessner AC. Survival after pancreas transplantation. JAMA. 2005;293:675; author reply 675–676.
67. Vandenberg BF, Rossen JD, Grover-McKay M, et al. Evaluation of diabetic patients for renal and pancreas transplantation: noninvasive screening for coronary artery disease using radionuclide methods. Transplantation. 1996;62:1230–1235.
68. Herzog CA, Marwick TH, Pheley AM, et al. Dobutamine stress echocar-diography for the detection of significant coronary artery disease in renal transplant candidates. Am J Kidney Dis. 1999;33:1080–1090.
69. Tadros GM, Malik JA, Manske CL, et al. Iso-osmolar radio contrast iodixanol in patients with chronic kidney disease. J Invasive Cardiol. 2005;17:211–215.
70. Bates JR, Sawada SG, Segar DS, et al. Evaluation using dobutamine stress echocardiography in patients with insulin-dependent diabetes mellitus before kidney and/or pancreas transplantation. Am J Cardiol. 1996;77:175–179.
71. Manske CL, Wang Y, Rector T, et al. Coronary revascularisation in insulindependent diabetic patients with chronic renal failure. Lancet. 1992;340:998–1002.
72. Legendre C, Garrigue V, Le Bihan C, et al. Harmful long-term impact of hepatitis C virus infection in kidney transplant recipients. Transplantation. 1998;65:667–670.
73. Douzdjian V, Gugliuzza KG, Fish JC. Multivariate analysis of donor risk factors for pancreas allograft failure after simultaneous pancreas-kidney transplantation. Surgery. 1995;118:73–81.
74. Humar A, Kandaswamy R, Granger D, et al. Decreased surgical risks of pancreas transplantation in the modern era. Ann Surg. 2000;231:269–275.
75. Humar A, Harmon J, Gruessner A, et al. Surgical complications requir-ing early relaparotomy after pancreas transplantation: comparison of the cyclosporine and FK 506 eras. Transplant Proc. 1999;31:606–607.
76. Kapur S, Bonham CA, Dodson SF, et al. Strategies to expand the donor pool for pancreas transplantation. Transplantation. 1999;67:284–290.
77. Bonham CA, Kapur S, Dodson SF, et al. Potential use of marginal donors for pancreas transplantation. Transplant Proc. 1999;31:612–613.
78. Salvalaggio PR, Davies DB, Fernandez LA, Kaufman DB. Outcomes of pancreas transplantation in the United States using cardiac-death donors. Am J Transplant. 2006;6:1059–1065.
79. Wahlberg JA, Love R, Landegaard L, et al. 72-hour preservation of the canine pancreas. Transplantation. 1987;43:5–8.
80. Kin S, Stephanian E, Gores P, et al. Successful 96-Hr cold-storage preserva-tion of canine pancreas with UW solution containing the thromboxane A2 synthesis inhibitor OKY046. J Surg Res. 1992;52:577–582.
81. D’Alessandro AM, Kalayoglu M, Sollinger HW, et al. Current status of organ preservation with University of Wisconsin solution. Arch Pathol Lab Med. 1991;115:306–310.
82. Humar A, Kandaswamy R, Drangstveit MB, et al. Surgical risks and out-come of pancreas retransplants. Surgery. 2000;127:634–640.
83. Matsumoto S, Kandaswamy R, Sutherland DE, et al. Clinical application of the two-layer (University of Wisconsin solution/perfluorochemical plus O2) method of pancreas preservation before transplantation. Transplantation. 2000;70:771–774.
84. Kuroda Y, Kawamura T, Suzuki Y, et al. A new, simple method for cold storage of the pancreas using perfluorochemical. Transplantation. 1988;46:457–460.
85. Fujita H, Kuroda Y, Saitoh Y. The mechanism of action of the two-layer cold storage method in canine pancreas preservation–protection of pancre-atic microvascular endothelium. Kobe J Med Sci. 1995;41:47–61.
86. Tanioka Y, Kuroda Y, Saitoh Y. Amelioration of rewarming ischemic injury of the pancreas graft during vascular anastomosis by increasing tissue ATP contents during preservation by the two-layer cold storage method. Kobe J Med Sci. 1994;40:175–189.
87. Agarwal A, Murdock P, Pescovitz MD, et al. Follow-up experience using histidine-tryptophan ketoglutarate solution in clinical pancreas transplan-tation. Transplant Proc. 2005;37:3523–3526.
88. Englesbe MJ, Moyer A, Kim DY, et al. Early pancreas transplant outcomes with histidine-tryptophan-ketoglutarate preservation: a multicenter study. Transplantation. 2006;82:136–139.
89. Becker T, Ringe B, Nyibata M, et al. Pancreas transplantation with histi-dine-tryptophan-ketoglutarate (HTK) solution and University of Wiscon-sin (UW) solution: is there a difference? JOP. 2007;8:304–311.
90. Mancini MJ, Connors AF Jr, Wang XQ, et al. HLA matching for simul-taneous pancreas-kidney transplantation in the United States: a multivari-able analysis of the UNOS data. Clin Nephrol. 2002;57:27–37.
91. Gruessner AC, Sutherland DE, Gruessner RW. Matching in pancreas trans-plantation—a registry analysis. Transplant Proc. 2001;33:1665–1666.
92. Malaise J, Berney T, Morel P, et al; EUROSPK Study Group. Effect of HLA matching in simultaneous pancreas-kidney transplantation. Trans-plant Proc. 2005;37:2846–2847.
93. Lo A, Stratta RJ, Alloway RR, Hodge EE; PIVOT Study Group. A mul-ticenter analysis of the significance of HLA matching on outcomes after kidney-pancreas transplantation. Transplant Proc. 2005;37:1289–1290.
94. Berney T, Malaise J, Morel P; Euro-SPK Study Group. Impact of HLA matching on the outcome of simultaneous pancreas-kidney transplanta-tion. Nephrol Dial Transplant. 2005;20(Suppl 2):ii48–53, ii62.
95. Gruber SA, Katz S, Kaplan B, et al. Initial results of solitary pancreas transplants performed without regard to donor/recipient HLA mismatch-ing. Transplantation. 2000;70:388–391.
LWBK1580_C73_p840-853.indd 851 31/07/17 5:40 PM

852 SeCtion 7 OrgAn trAnsPlAntAtiOn
96. Page MM, Watkins PJ. Cardiorespiratory arrest and diabetic autonomic neuropathy. Lancet. 1978;1:14–16.
97. Hogan K, Rusy D, Springman SR. Difficult laryngoscopy and diabetes mellitus. Anesth Analg. 1988;67:1162–1165.
98. Gruessner RW. Donor procedures. In: Gruessner RW, Sutherland DE, eds. Transplantation of the Pancreas. New York, NY: Springer-Verlag; 2004:126–142.
99. Krishnamurthi V, Philosophe B, Bartlett ST. Pancreas transplantation: con-temporary surgical techniques. Urol Clin North Am. 2001;28:833–838.
100. Gruessner RW, Sutherland DE: Clinical diagnosis in pancreas allograft rejection. In: Solez K, Racusen LC, Billingham ME, eds. Solid Organ Transplant Rejection: Mechanisms, Pathology and Diagnosis. New York, NY: Marcel Dekker; 1996:455–499.
101. Benedetti E, Najarian JS, Gruessner AC, et al. Correlation between cys-toscopic biopsy results and hypoamylasuria in bladder-drained pancreas transplants. Surgery. 1995;118:864–872.
102. Kirk AD. Immunosuppression without immunosuppression? How to be a tol-erant individual in a dangerous world. Transplant Infect Dis. 1999;1:65–75.
103. Stratta RJ, Shokouh-Amiri MH, Egidi MF, et al. A prospective compari-son of simultaneous kidney-pancreas transplantation with systemic-enteric versus portal-enteric drainage. Ann Surg. 2001;233:740–751.
104. Bagdade JD, Ritter MC, Kitabchi AE, et al. Differing effects of pancreas-kid-ney transplantation with systemic versus portal venous drainage on choles-teryl ester transfer in IDDM subjects. Diabetes Care. 1996;19:1108–1112.
105. Carpentier A, Patterson BW, Uffelman KD, et al. The effect of systemic versus portal insulin delivery in pancreas transplantation on insulin action and VLDL metabolism. Diabetes. 2001;50:1402–1413.
106. Diem P, Abid M, Redmon JB, et al. Systemic venous drainage of pan-creas allografts as independent cause of hyperinsulinemia in type I diabetic recipients. Diabetes. 1990;39:534–540.
107. Konigsrainer A, Foger BH, Miesenbock G, et al. Pancreas transplantation with systemic endocrine drainage leads to improvement in lipid metabo-lism. Transplant Proc. 1994;26:501–502.
108. Philosophe B, Farney AC, Schweitzer EJ, et al. Superiority of portal venous drainage over systemic venous drainage in pancreas transplantation: a ret-rospective study. Ann Surg. 2001;234:689–696.
109. Boggi U, Vistoli F, Signori S, et al. A technique for retroperitoneal pancreas trans-plantation with portal-enteric drainage. Transplantation. 2005;79:1137–1142.
110. Sutherland DE, Morel P, Gruessner RW. Transplantation of two diabetic patients with one divided cadaver donor pancreas. Transplant Proc. 1990;22:585.
111. Tyden G, Tibell A, Sandberg J. Improved results with a simplified tech-nique for pancreaticoduodenal transplantation with enteric exocrine drainage. Clin Transplant. 1996;10:306.
112. Becker YT, Collins BH, Sollinger HW. Technical complications of pancreas transplantation. Curr Opin Organ Transplant. 1998;3:253.
113. Elkhammas EA, Henry ML, Tesi RJ, et al. Control of metabolic acido-sis after pancreas transplantation using acetazolamide. Transplant Proc. 1991;23:1623–1624.
114. Schang T, Timmermann W, Thiede A, et al. Detrimental effects of fluid and electrolyte loss from duodenum in bladder-drained pancreas transplants. Transplant Proc. 1991;23:1617–1618.
115. Peltenburg HG, Mutsaerts KJ, Hardy EL, van Hooff JP. Sodium lactate as an alternative to sodium bicarbonate in the management of metabolic aci-dosis after pancreas transplantation. Transplantation. 1992;53:225–226.
116. Benedetti E, Coady NT, Asolati M, et al. A prospective randomized clinical trial of perioperative treatment with octreotide in pancreas transplanta-tion. Am J Surg. 1998;175:14–17.
117. Carlsson PO, Jansson L. The long-acting somatostatin analogue octreotide decreases pancreatic islet blood flow in rats. Pancreas. 1994;9:361–364.
118. Kandaswamy R, Humar A, Gruessner AC, et al. Vascular graft thrombosis after pancreas transplantation: comparison of the FK 506 and cyclospo-rine eras. Transplant Proc. 1999;31:602–603.
119. Humar A, Gruessner RW, Sutherland DE. Living related donor pancreas and pancreas-kidney transplantation. Br Med Bull. 1997;53:879–891.
120. Benedetti E, Rastellini C, Sileri P, et al. Successful simultaneous pancreas-kidney transplantation from well-matched living-related donors. Trans-plant Proc. 2001;33:1689.
121. Calne RY, Rolles K, White DJ, et al. Cyclosporin A initially as the only immunosuppressant in 34 recipients of cadaveric organs: 32 kidneys, 2 pancreases, and 2 livers. Lancet. 1979;2:1033–1036.
122. Stratta RJ. Simultaneous use of tacrolimus and mycophenolate mofetil in combined pancreas-kidney transplant recipients: a multi-center report. The FK/MMF Multi-Center Study Group.Transplant Proc. 1997;29:654–655.
123. Gruessner AC, Sutherland DE. Analysis of United States (US) and non-US pancreas transplants as reported to the International Pancreas Transplant
Registry (IPTR) and to the United Network for Organ Sharing (UNOS). Clin Transpl. 1998;53–73.
124. Gruessner RW, Sutherland DE, Drangstveit MB, et al. Mycophenolate mofetil and tacrolimus for induction and maintenance therapy after pan-creas transplantation. Transplant Proc. 1998;30:518–520.
125. Gruessner RW, Sutherland DE, Parr E, et al. A prospective, randomized, open-label study of steroid withdrawal in pancreas transplantation-a prelimi-nary report with 6-month follow-up. Transplant Proc. 2001;33:1663–1664.
126. Kaufman DB, Leventhal JR, Gallon LG. Pancreas transplantation in the prednisone-free era. Am J Transplant. 2003;3:322.
127. Salazar A, McAlister VC, Kiberd BA, et al. Sirolimus-tacrolimus combina-tion for combined kidney-pancreas transplantation: effect on renal func-tion. Transplant Proc. 2001;33:1038–1039.
128. Kaufman DB, Leventhal JR, Koffron AJ, et al. A prospective study of rapid corticosteroid elimination in simultaneous pancreas-kidney transplantation: comparison of two maintenance immunosuppression protocols: tacroli-mus/mycophenolate mofetil versus tacrolimus/sirolimus. Transplantation. 2002;73:169–177.
129. Stratta RJ, Alloway RR, Lo A, Hodge E. A multicenter trial of two daclizumab dosing strategies versus no antibody induction in simultaneous kidney-pan-creas transplantation: interim analysis. Transplant Proc. 2001;33:1692–1693.
130. Gruessner RW, Kandaswamy R, Humar A, et al. Calcineurin inhibitor- and steroid-free immunosuppression in pancreas-kidney and solitary pan-creas transplantation. Transplantation. 2005;79:1184–1189.
131. Rubin RH. A new beginning. Transplant Infect Dis. 1999;1:1. 132. Villacian JS, Paya CV. Prevention of infections in solid organ transplant
recipients. Transplant Infect Dis. 1999;1:50–64. 133. Tyan DB, Li VA, Czer L, et al. Intravenous immunoglobulin suppression of
HLA alloantibody in highly sensitized transplant candidates and transplan-tation with a histoincompatible organ. Transplantation. 1994;57:553–562.
134. Glotz D, Haymann JP, Niaudet P, et al. Successful kidney transplantation of immunized patients after desensitization with normal human polyclonal immunoglobulins. Transplant Proc. 1995;27:1038–1039.
135. Jordan SC, Quartel AW, Czer LS, et al. Posttransplant therapy using high-dose human immunoglobulin (intravenous gammaglobulin) to control acute humoral rejection in renal and cardiac allograft recipients and poten-tial mechanism of action. Transplantation. 1998;66:800–805.
136. Watanabe H, Misu K, Kobayashi T, et al. ABO-incompatible auxiliary partial orthotopic liver transplant for late-onset familial amyloid polyneu-ropathy. J Neurol Sci. 2002;195:63–66.
137. Shishido S, Asanuma H, Tajima E, et al. ABO-incompatible living-donor kidney transplantation in children. Transplantation. 2001;72:1037–1042.
138. Montgomery RA, Zachary AA, Racusen LC, et al. Plasmapheresis and intravenous immune globulin provides effective rescue therapy for refrac-tory humoral rejection and allows kidneys to be successfully transplanted into cross-match-positive recipients. Transplantation. 2000;70:887–895.
139. Takeda A, Uchida K, Haba T, et al. Acute humoral rejection of kidney allografts in patients with a positive flow cytometry crossmatch (FCXM). Clin Transplant. 2000;14(Suppl 3):15–20.
140. Bittner HB, Dunitz J, Hertz M, et al. Hyperacute rejection in single lung trans-plantation–case report of successful management by means of plasmapheresis and antithymocyte globulin treatment. Transplantation. 2001;71:649–651.
141. Reddy KS, Stratta RJ, Shokouh-Amiri MH, et al. Surgical complications after pancreas transplantation with portal-enteric drainage. J Am Coll Surg. 1999;189:305–313.
142. Wuthrich RP. Factor V Leiden mutation: potential thrombogenic role in renal vein, dialysis graft and transplant vascular thrombosis. Curr Opin Nephrol Hypertens. 2001;10:409–414.
143. Friedman GS, Meier-Kriesche HU, Kaplan B, et al. Hypercoagulable states in renal transplant candidates: impact of anticoagulation upon incidence of renal allograft thrombosis. Transplantation. 2001;72:1073–1078.
144. Zibari GB, Aultman DF, Abreo KD, et al. Roux-en-Y venting jejunostomy in pancreatic transplantation: a novel approach to monitor rejection and prevent anastomotic leak. Clin Transplant. 2000;14:380–385.
145. Eckhoff DE, Ploeg RJ, Wilson MA, et al. Efficacy of 99mTc voiding cys-tourethrogram for detection of duodenal leaks after pancreas transplanta-tion. Transplant Proc. 1994;26:462–463.
146. Roza AM, Johnson CP, Adams M. Acute torsion of the renal transplant after combined kidney-pancreas transplant. Transplantation. 1999;67:486–488.
147. West MS, Stevens RB, Metrakos P, et al. Renal pedicle torsion after simulta-neous kidney-pancreas transplantation. J Am Coll Surg. 1998;187:80–87.
148. Del Pizzo JJ, Jacobs SC, Bartlett ST, Sklar GN. Urological complications of bladder-drained pancreatic allografts. Br J Urol. 1998;81:543–547.
149. Kaplan AJ, Valente JF, First MR, et al. Early operative intervention for urologic complications of kidney-pancreas transplantation. World J Surg. 1998;22:890–894.
LWBK1580_C73_p840-853.indd 852 31/07/17 5:40 PM

Chapter 73 Pancreatic transplantation 853
150. Troppmann C, Gruessner AC, Dunn DL, et al. Surgical complications requiring early relaparotomy after pancreas transplantation: a multivariate risk factor and economic impact analysis of the cyclosporine era. Ann Surg. 1998;227:255–268.
151. Gruessner RW. Immunobiology, diagnosis, and treatment of pancreas graft rejection. In: Gruessner RW, Sutherland DE, eds. Transplantation of the Pancreas. New York, NY: Springer-Verlag; 2004:349–380.
152. Papadimitriou JC, Drachenberg CB, Wiland A, et al. Histologic grading of acute allograft rejection in pancreas needle biopsy: correlation to serum enzymes, glycemia, and response to immunosuppressive treatment. Trans-plantation. 1998;66:1741–1745.
153. Klassen DK, Weir MR, Cangro CB, et al. Pancreas allograft biopsy: safety of percutaneous biopsy-results of a large experience. Transplantation. 2002;73:553–555.
154. Malek SK, Potdar S, Martin JA, et al. Percutaneous ultrasound-guided pan-creas allograft biopsy: a single-center experience. Transplant Proc. 2005; 37:4436–4437.
155. Auchincloss H Jr, Sachs DH. Xenogeneic transplantation. Ann Rev Immu-nol. 1998;16:433–470.
156. Lanza RP, Chick WL. Transplantation of encapsulated cells and tissues. Surgery. 1997;121:1–9.
157. Hering BJ, Wijkstrom M, Graham ML, et al. Prolonged diabetes reversal after intraportal xenotransplantation of wild-type porcine islets in immu-nosuppressed nonhuman primates. Nat Med. 2006;12:301–303.
158. Shapiro AM, Lakey JR. Future trends in islet cell transplantation. Diabetes Technol Ther. 2000 Autumn;2:449–452.
159. Cooke A, Phillips JM, Parish NM. Tolerogenic strategies to halt or prevent type 1 diabetes. Nat Immunol. 2001;2:810–815.
LWBK1580_C73_p840-853.indd 853 31/07/17 5:40 PM