New PMMA Membrane for Better Quality of Life...As for several KoAs (the product of overall mass...
8
New PMMA Membrane for Better Quality of Life Hollow Fiber Dialyzer Filtryzer BG-U Series
Transcript of New PMMA Membrane for Better Quality of Life...As for several KoAs (the product of overall mass...

New PMMA Membrane for Better Quality of Life
Hollow Fiber Dialyzer
Filtryzer BG-U Series

New Membrane Structure by “Sophisticated Pore Control Technology”
iso-PMMA
syn-PMMA
CH3
O
C
200 2 5 10 50
200
500
Pure water permeability λ Lp (cm3 • sec/g)
Pore
size
r(Å)
Pore
dens
ity∝
∆H•T
p2(°
C•c
al•g
–1)
100
50
20
200
100
50
20
B2 B1 B1-U BG BK-F
“FILTRYZER” is Polymethylmethacrylate membrane (PMMA) and TORAY is the only manufacturer which succeeded in developing it as dialysis membrane. FILTRYZER was intro-duced in 1977 and it has enjoyed a good reputation all over the world due to high biocompatibility, high removal performance, wide range of UFR, and unique adsorption characteristics for various proteins.
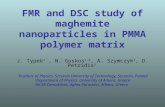
PMMA is synthetic membrane by mixing 2 kinds of poly-mer, isotactic PMMA (Iso-PMMA) and syndiotactic PMMA (Syn-PMMA). These polymers form the stereocomplex structure as shown in the picture. The pore structure in the membrane can be widely adjusted by controlling the process condi-tions including the chemical structure, the composition of the PMMAs (i.e., ratio of Iso-PMMA to Syn-PMMA), the concen-tration, cooling speed of dope solution, and the heat setting.
With this wide range of pore structure, FILTRYZER has met the new targets of physicians and has been used in many clinical studies for more than 20 years.
PMMA has established excellent reliability in its long his-tory based on many kinds of clinical data and accumulated technology. For further improvement of the patients’ quality of life, TORAY has been investigating the potential of PMMA through reserch and trials.
Our “Sophisticated Pore Control Technology”, which combines the process conditions and copolymerization, made it possible to create brand new PMMA membrane “FILTRYZER BG-U series”. This new PMMA membrane has obtained both the controlled pore size around 70Å and uniform distribution of pore size.
At the same time, this membrane has higher porosity and unprecedented adsorption capability.
This structure can improve both UFR and permeability or adsorption performance of not only small molecules but also low molecular weight proteins like β2-microglobulin.
Relationship of pore size, pore density and water permeability of PMMA membranes

As shown in the figure, BG membrane is designed by homogenizing the pore size and increasing the number of pores, resulting in the improvement of the re-moval through small molecules to low molecular weight proteins such as β2-MG.
1,000
800
600
400
200
0
Creatinine
Uric acid
Phosphate
Vitamin B12
BG-1.6UBK-1.6PBK-1.6U
(ml/min)
BUN
Diff
usive
perm
eabi
lity
(KoA
)
755
809
839
484
504
515
387
401
408
361
361
423
178
183
189
Internal data
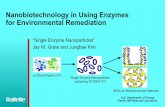
Structure of new PMMA membrane BGPore structure SEM observation
Inside Center Outside
PMMA(BK)
NewPMMA
BG
Improved diffusive permeability (KoA)
As for several KoAs (the product of overall mass transfer coefficient and area) for small molecules, Filtryzer BG has an improving per-formance compared with the other types of high-flux PMMA membranes, BK-U and BK-P.

Proven Biocompatibility
Comparison of removal for several cytokines (in vitro)
Rem
oval
(pg/
3hr)
1,2001,000
800
600
400
200
0
BS-U
PS-UW
BK-F
PAN-SFBG-U
TNF-α(MW: 17,000 + α2-MG)
Polysulfone
PMMA
Rem
oval
(pg/
3hr)
3,000
2,500
2,000
1,500
1,000
500
0
BS-U
PS-UW
PAN-SF
BK-F
BG-U
IL-6(MW: 21,000)
Polysulfone
PMMA
The time course of complement fragment C3a, white blood cell count and platelet count.
Removal amount; pg/3hr
Filtration amount
adsorption amount
QP: 1.15mL/minQF: 0.15mL/minmembrane area; 25cm2
perfusion; 3 hours
primary concentrationTNF-α: 65 pg/mLIL-6: 320 pg/mL
Kawanishi H. Intensive & Critical Care Medicine 12, S7–S8, proceedings 2000
Higher adsorptive removal for cytokinesRemoval of cytokines with BG-U membrane and others
were investigated in an in vitro perfusion test. The removal of cytokines with BG-U is mainly conducted by adsorption as shown in the graph: the green bar was the major portion of total removed amount with BG-U. As for removal of IL-6, the adsorbed amount with BG-U exceeded the total amounts with both polysulfone membranes.
Excwllent quality know as biocompatible membrane
Touma studied on the biocompatibility of BG-U membrane based upon the time course of WBC count, Platelet count and Complement fragment C3a in comparison with Cellulose Tri-acetate membrane, FB, and the previous PMMA membrane, BK-U.
As shown with blue line, the changes on these biocompatibility parameters of BG-U were more stable than that of FB and almost the same as BK-U. So the biocompatibility of BG-U membrane is judged as the superior level as previous PMMA membrane which has obtained a reputation by its excellent biocompatibility in a long period of its history.
Modified from Touma S, Kidney & Dialysis, Suppl.,132-134, 1997
n=4, crossover
n=4, crossover
n=4, crossover
BGFBBKU
700
600
500
400
300
200
100
0
C3a
(ng/
mL)
8,000
6,000
4,000
2,000
WBC
(/mm
3 )
30
25
20
15
10
Plat
.(10
4 /mm
3 )
pre 15min 30min post

Unique Adsorption of Proteins
Adsorption of 125I-labeled plasma proteins on the various membranes
For the 6 kinds of dialyzers, Birk et al., conducted the adsorption experiment of plasma protein in vitro with radio-isotope labelling. The PMMA membrane showed the maxi-mum amount of protein adsorption per unit surface area.
Furthermore, as a result of analyzing the molecular weight of the adsorbed proteins, compared with other mem-brane materials, PMMA adsorbed higher molecular weight proteins (HMW proteins) than albumin, shown in blue bars. When the PMMA membrane was used, the removability by adsorption tended to increase for proteins with higher mo-lecular weights.
Adsorption of plasma proteins with mini-module
The below figure shows the internal data for adsorption of plasma proteins with mini-module with 3 kinds of synthetic membranes. On the X axis, plasma proteins in the order of iso-electric point are shown. For example, the adsorptive ratio of β2-MG on BK and BG membranes are in the high level. But towards the target proteins with more cationic iso-electric point, BG membrane adsorbed more of them than BK membrane such as PF-4, lysozyme and somatostatin. So these data suggest the adsorption of cationic proteins are enhanced by the electric interaction with the BG membrane.
PMMA BG PMMA BK
PS
100
80
60
40
20
0
Adso
ptive
Rat
io (%
)
Retinol
Binding
Fibrin
ogen
(5.8)
α1-micr
oglob
lin(5.
89)
β2-micr
oglob
lin(6.
07)
IgG (6
.5)
Factor
D (7)
PF-4 (8
.65)
β-throm
boglo
blin(8.
93)
Protein
(5.14
)
lysozy
me (9.0
5)
somato
statin
(9.16
)
C3a (9.
92)
Birk, H-W. et al., Artificial Organs,19(5),411-415, 1995
HMW proteins>65kDLMW proteins<65kD

The possibility in removal of HCV particles in HD patients over hemodialysis therapy
In worldwide HD patients, the positive rate of anti-HCV antibody seems to be high. But the number of HCV RNA in blood is lower and the liver disorder is slight. It is due to extracorporial treatment through dialyzer use every 2 days. Kuramochi reported that the viral particles reduced in the blood through dialyzer, above all, through PMMA mem-brane. The viral particles were not detected in the filtrate or dialysate, and were rather thought to be adsorbed on the dialyzer membrane surface.
600
400
200
0
HC
V R
NA
(KU
/mL)
PS
EVAL
PAN
PMMA
CDA
CTA
Kuramochi and Shima J Artif Organs 4 ; 146-149, 2001
Kato A. et.al., Artificial Organs 25(6);441-447, 2001*p=0.047 as compared to scores at the beginning, §p=0.049 as compared to scores at 2 months
An Example of QOL Improvement
Excellent Clinical Benefits to Renal Failure Patients
3.5
3.0
2.5
2.0
1.5
1.0
Cross over
Pre 1M 2M 3M 4M 5M 6M
Itchin
g sc
ales
Group 2 (n=8)PMMA membrane Conventional membrane
PMMA membraneGroup 1 (n=9)
Conventional membrane *§
120
100
80
60
40
20
0
Chan
ge o
f % h
istam
ine
rele
ase
Pre
Post
With Polysulfone
With BG
Fraction from
patients was solely
incubated
Yamada S. et al., Kidney and Dialysis,suppl,; 167-171, 2003
*
**
Inlet of dialyzer
Outlet of dialyzer
* P<0.05
** P<0.01
Pre: Before incubationPost: After incubation without fibers
Efficacy in amelioration of renal itching in hemodialysis patients (cross over study)
In group 1, one month after changing to BG membrane, the pruritus score was decreased to 1.9 ±0.4 which is sig-nificantly lower compared to those at 2 months when the conventional membranes were used (§p=0.049).
In group 2, the BG membrane gradually and significantly reduced pruritus score from 2.8 ±0.2 to 1.9 ±0.4 3 months later (*p=0.047). The degree of pruritus did not worsen dur-ing the next 3 months despite returning to the conventional dialyzers.
Confirmation of removal of pruritus generating substances assayed with mast cells
This shows the results when the fraction from patients’ blood which has activity for histamine release from mast cells was coincubated with hollow fibers for 3 hours.
With BG membrane the activity was massively reduced compared with that of polysulfone membrane.
These data suggest the adsorption of the sustances gen-erating pruritus and correspond well to the observation of clinical amelioration in pruritus with BG membrane.

Advanced Technical Data
BG-U Series
Type BG-1.3U BG-1.6U BG-1.8U BG-2.1U
Housing Material Polystyrene
Fibers Material Poly (methylmethacrylate), PMMA
Inner diameter (µm) 200
Membrane thickness (µm) 30
Effective surface area (m2) 1.3 1.6 1.8 2.1
Potting Material Polyurethane
Sterilization Gamma-ray Irradiation
Blood Volume (mL) 76 94 112 126
Clearance in vitro (mL/min)*
Urea 184 189 191 192
Creatinine 182 188 188 191
Phosphate 154 165 172 179
Vitamin B12 106 118 123 133
Inulin 60 67 72 81
UFR in vitro {mL/hr, at 13.3kPa (100mmHg)}** 2,600 3,200 3,600 4,100
Max. TMP {kPa (mmHg)} 66 (500)
* Clearances were measured with aqueous solution. QB: 200mL/min, QD: 500mL/min, QF: 10mL/min, Temp.: 37°C** UFRs were measured data with bovine blood. (Ht 30 ±2%, TP 6g/dL) QB: 200mL/min, TMP: 13.3kPa (100mmHg), Temp.: 37°C Allowable ranges: Blood volume; ±13%. Clearances, Urea; ±6%, Creat.; ±6%, Others; ±13%, UFR in vitro; ±15%“Instructions for Use” should be read thoroughly prior to the use of these medical devices.Specifications and designs are subject to change without notice for improvements.
ClearanceBG-1.3UQB 300 400 500UR; Urea 234 267 289CR; Creatinine 228 253 269PO4; Phosphate 186 206 216VB12; Vitamin B12 119 123 129IN; Inulin 63 63 64
BG-1.6UQB 300 400 500UR; Urea 249 283 310CR; Creatinine 247 276 298PO4; Phosphate 202 221 236VB12; Vitamin B12 134 140 146IN; Inulin 73 74 79
BG-1.8UQB 300 400 500UR; Urea 258 301 321CR; Creatinine 250 285 300PO4; Phosphate 217 236 253VB12; Vitamin B12 142 152 155IN; Inulin 80 83 86
350
300
250
200
150
100
50
0200 400
350
300
250
200
150
100
50
0200 400
350
300
250
200
150
100
50
0200 400
350
300
250
200
150
100
50
0200 400
BG-2.1UQB 300 400 500UR; Urea 265 312 335CR; Creatinine 262 300 318PO4; Phosphate 223 248 268VB12; Vitamin B12 155 169 172IN; Inulin 86 90 99
BG-1.3U BG-1.6U BG-1.8U BG-2.1U
UFR
Measured data with aqueous solution
BG-1.3U BG-1.6 BG-1.8U BG-2.1U

Printed in Japan 0501 G
EU Representative:Toray Europe Ltd.Medical Department7, Old Park Lane, London W1K 1AD, U. K.TEL: 44-20 7663 7749 / FAX: 44-20 7663 7714
Exporter:Toray Medical Co., Ltd.International Business DivisionARCA Central 21F., 2-1, Kinshi 1-chome, Sumida-ku, Tokyo 130-0013, JAPANTEL: (03)5610-6535 / FAX: (03)5610-6545 / E-MAIL: [email protected]
Manufacturer:Toray Industries, Inc.2-1, Nihonbashi-Muromachi 2-chome, Chuo-ku, Tokyo 103-8666, JAPANTEL: (03)3245-5111 / FAX: (03)3245-5555