![&Z Ì ] & } u dZ /E/E'](https://static.fdocument.org/doc/165x107/629d9bc2687b3969ab0e8d75/ampz-amp-u-dz-ee.jpg)
Jaundice, E. Ngadaya
35
-
Upload
emmanuel-ngadaya -
Category
Health & Medicine
-
view
87 -
download
1
Transcript of Jaundice, E. Ngadaya
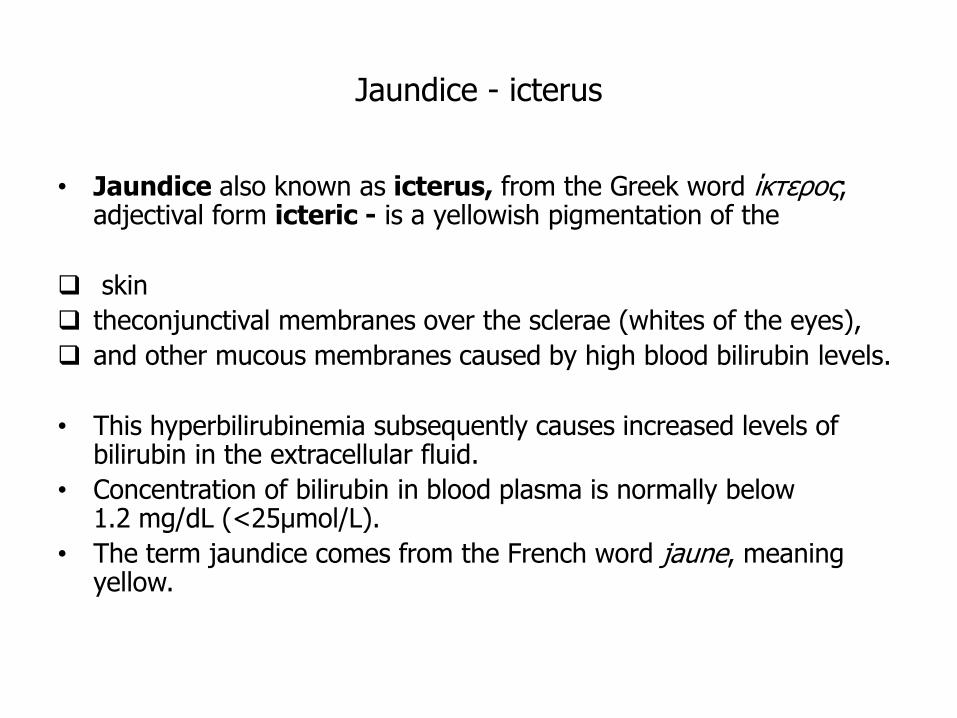
Jaundice - icterus
• Jaundice also known as icterus, from the Greek word ίκτερος; adjectival form icteric - is a yellowish pigmentation of the
skin
theconjunctival membranes over the sclerae (whites of the eyes),
and other mucous membranes caused by high blood bilirubin levels.
• This hyperbilirubinemia subsequently causes increased levels of bilirubin in the extracellular fluid.
• Concentration of bilirubin in blood plasma is normally below 1.2 mg/dL (<25µmol/L).
• The term jaundice comes from the French word jaune, meaning yellow.
Jaundice
Bilirubin is a yellow pigment which causes discolorationof the skin and when serum levels exceed 35-40 µmol/L.
Concentrations may increase for three reasons:
- the production rate of bilirubin is increased, exceeding the excretory capacity of the liver (prehepatic jaundice);
- conjugating and / or excretory functions are reduced, (hepatic
or hepatocellular jaundice);
- biliary obstruction interferes with the flow of bile and thus bilirubin excretion (posthepatic, obstructive or cholestatic jaundice).
3
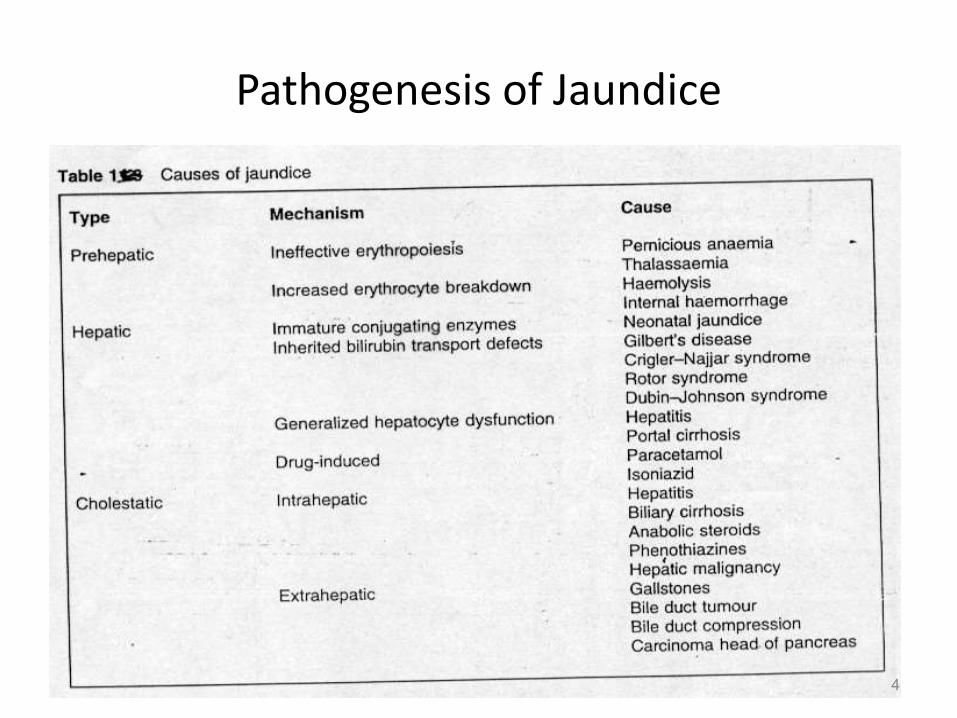
Pathogenesis of Jaundice
4
1.Pre hepatic jaundice
6
Prehepatic Jaundice
• Prehepatic jaundice is caused by increased destruction of erythrocytes either:
- mature cells or - precursors (ineffective erythropoiesis).
• The breakdown of mature cells can be caused by:
- haemolysis, or - as a result of the metabolism of blood following internal haemorrhage, e.g. into a soft tissue injury or fracture.
7
Prehepatic Jaundice
• Ineffective erythropoiesis occurs in conditions such as:
- pernicious anaemia, where the
maturation of red cells is impaired, or
- thalassaemia, where the structure
of haemoglobin is abnormal.
• Hyperbilirubinaemia in prehepatic jaundice results from
the accumulation of unconjugated bilirubin; this is not excreted by the kidney.
8
Prehepatic Jaundice
• Jaundice occurs because the conjugating capacity of the liver is saturated,
- the capacity of the liver for conjugation is
greater than the normal rate of bilirubin production.
• Increased fluxes of bilirubin through the liver into the gut
• Greater amounts of urobilinogen are produced, with
- increased urobilinogen excretion in urine.
9
2.Hepatic Jaundice
10
Hepatic Jaundice
• Congenital disorders of bilirubin transport lead to jaundice because of:
- defective uptake, reduced conjugation
or impaired excretion of bilirubin.
• Generalized hepatocellular dysfunction may occur in hepatitis and hepatic cirrhosis.
• Drugs may cause hepatocellular damage, either due to dose-dependent hepatoxicity (e.g. paracetamol).
11
Hepatic Jaundice
• The pathogenesis of jaundice in these conditions is complex,
- reduced hepatic uptake,
- decreased conjugation and,
- impaired intracellular transport
of bilirubin, all contributing.
12
Hepatic Jaundice
• When hyperbilirubinaemia is caused by impaired conjugation of bilirubin;
- unconjugated bilirubin, and no
increased fluxes of bilirubin through the liver,
- bilirubinuria does not occur and
- urinary urobilinogen is not increased.
13
Hepatic Jaundice
• Serum bilirubin may be unconjugated or conjugated, as UDP glucuronyl transferase and intracellular transport may be defective.
• If the rate of conjugation exceeds excretory capacity;
- conjugated hyperbilirubinaemia will
occur and bilirubin may be excreted,in urine,
- this is sometimes seen in recovery from acute
viral hepatitis.
14
3.Cholestatic Jaundice
15
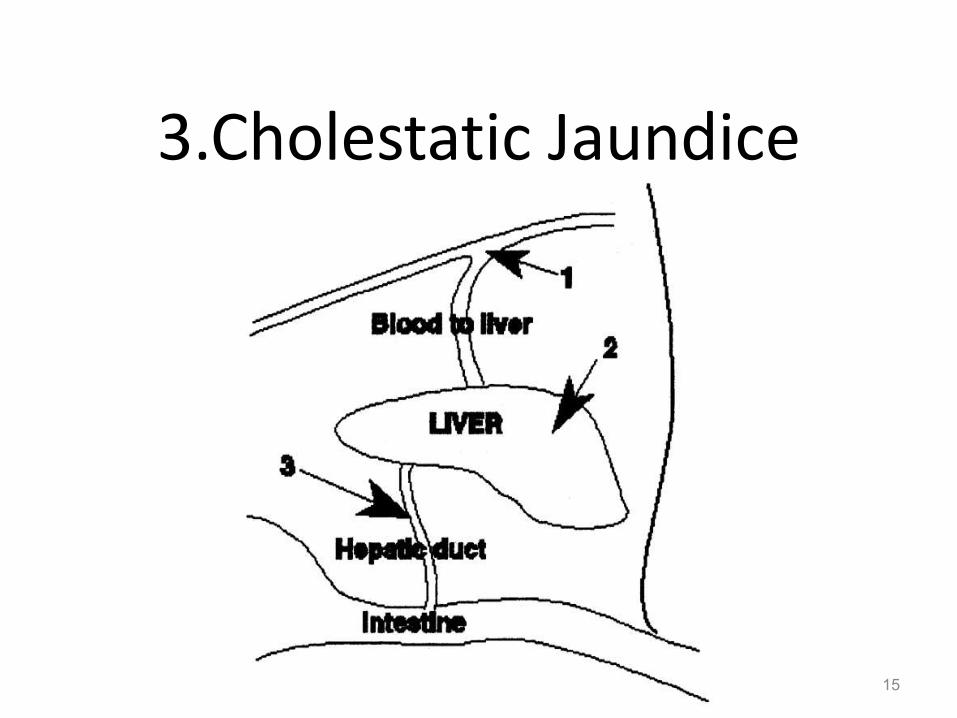
Cholestatic Jaundice
• Cholestatic jaundice results from interference to biliary flow between the sites of secretion by the hepatocyte and drainage into the duodenum.
• It may be caused by lesions;
- within the liver (intrahepatic cholestasis), or in the biliary tree or head of the pancreas (extrahepatic cholestasis);
- the term cholestatic is preferable to post-hepatic to describe this pattern of jaundice.
16
Cholestatic Jaundice
• Intra- and extra-hepatic cholestasis can be differentiated by;
- ultrasound examination or
- liver biopsy, but not by liver function tests.
• Intrahepatic cholestasis may result from generalized hepatocellular dysfunction, such as occurs in;
- Hepatitis,
- Hepatic cirrhosis
• Hepatic malignancies may block branches of the biliary tree.
17
Cholestatic Jaundice
• Some drugs may cause intrahepatic cholestasis such as:
- anabolic steroids, and
- phenothiazines
• Extrahepatic obstruction may be due to tumours in:
- major branches of the biliary tract,
- head of pancreas.
• Gallstones may obstruct biliary flow.
18
Cholestatic Jaundice
• Jaundice is due to impaired excretion and accumulation of conjugated bilirubin which can be filtered by the kidney and appear in urine.
• If obstruction is complete bilirubin does not reach the gut, therefore urobilinogen:
- is not produced, and
- is absent in urine.
• Under such circumstances the stools are pale.
19
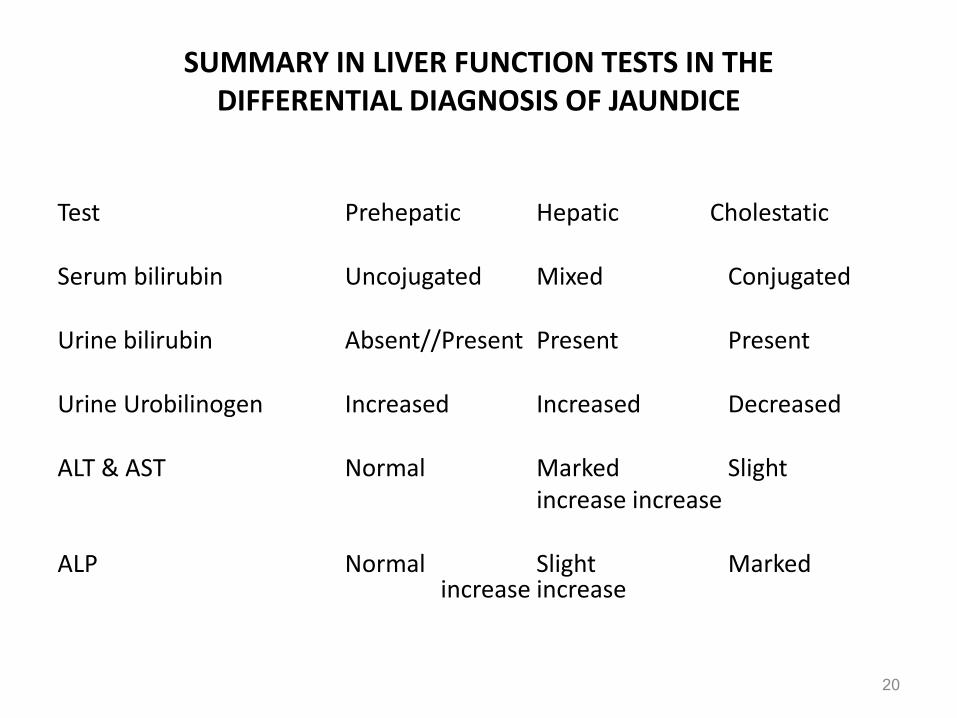
SUMMARY IN LIVER FUNCTION TESTS IN THE DIFFERENTIAL DIAGNOSIS OF JAUNDICE
Test Prehepatic Hepatic Cholestatic
Serum bilirubin Uncojugated Mixed Conjugated
Urine bilirubin Absent//Present Present Present
Urine Urobilinogen Increased Increased Decreased
ALT & AST Normal Marked Slight increase increase
ALP Normal Slight Marked increase increase
20
NEONATAL JAUNDICE
Neonatal jaundice
• is usually harmless
• this condition is often seen in infants around the second day after birth, lasting until day 8 in normal births, or to around day 14 inpremature births.
• Typical causes for neonatal jaundice include normal physiologic jaundice, jaundice due to formula supplementation, and hemolytic disorders that includehereditary spherocytosis, glucose-6-phosphate dehydrogenase deficiency, pyruvate kinase deficiency, ABO/Rhblood type auto antibodies, or infantile pyknocytosis.
• Serum bilirubin normally drops to a low level without any intervention required.
Neonatal jaundice
• In cases where bilirubin rises higher, a brain-damaging condition known as kernicterus can occur, leading to significant disability.
• This condition has been rising in recent years due to less time spent outdoors. A Bili light is often the tool used for early treatment, which often consists of exposing the baby to intensive phototherapy.
• Sunbathing is effective treatment, and has the advantage of ultra-violet-B, which promotes Vitamin D production. Bilirubin count is lowered through bowel movements and urination, so frequent and effective feedings are especially important
Hemolytic jaundice
• Congenital: Known also as hereditary spherocytosis (HS), this is a genetic disorder of the red blood cell membrane clinically characterized by anemia, jaundice (yellowing) and splenomegaly (enlargement of the spleen).
• It is also condition which is characterized by jaundice due to an increased production of bilirubin from degradation of red blood cells.
The risk factors for developing jaundice
• Certain individuals with hereditary conditions (for example, thalassemia or hereditary spherocytosis) jaundice from hemolysis.
• Individuals who consume alcohol heavily are at an increased risk of developing alcoholic hepatitis, pancreatitis, and cirrhosis leading to jaundice.
• exposure to the different types of viral hepatitis (for example, hepatitis B and hepatitis C) are also at risk of developing jaundice at the time of infection or subsequently if liver disease occurs or if liver cancer develops later.
What problems does jaundice cause?
1. Skin and sclerae - yellow2. Stool - light colour, clay coloured3. Dark urine4. Pain in abdomen5. Itching6. Trouble with sleeping7. Fatigue8. Swelling9. Ascites10. Mental confusion11. Coma12. Bleeding
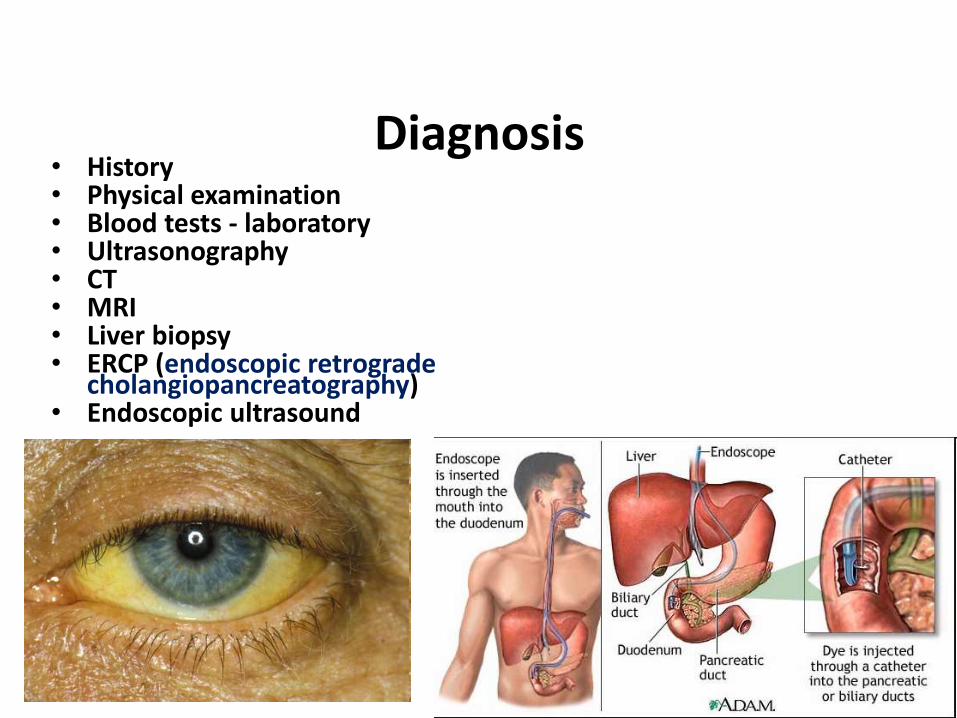
• History• Physical examination• Blood tests - laboratory• Ultrasonography• CT• MRI• Liver biopsy• ERCP (endoscopic retrograde
cholangiopancreatography)• Endoscopic ultrasound
Diagnosis
Laboratory Tests
• Bilirubin level in serum (total and direct)
• Aminotransferase
• Alkaline phosphatase
• U/A for bilirubin and urobilogen
Complete blood count
Prothrombin time
Other laboratory testspertinent to history
Coombs test
Electrophoresis of hemoglobin
Viral hepatitis panel
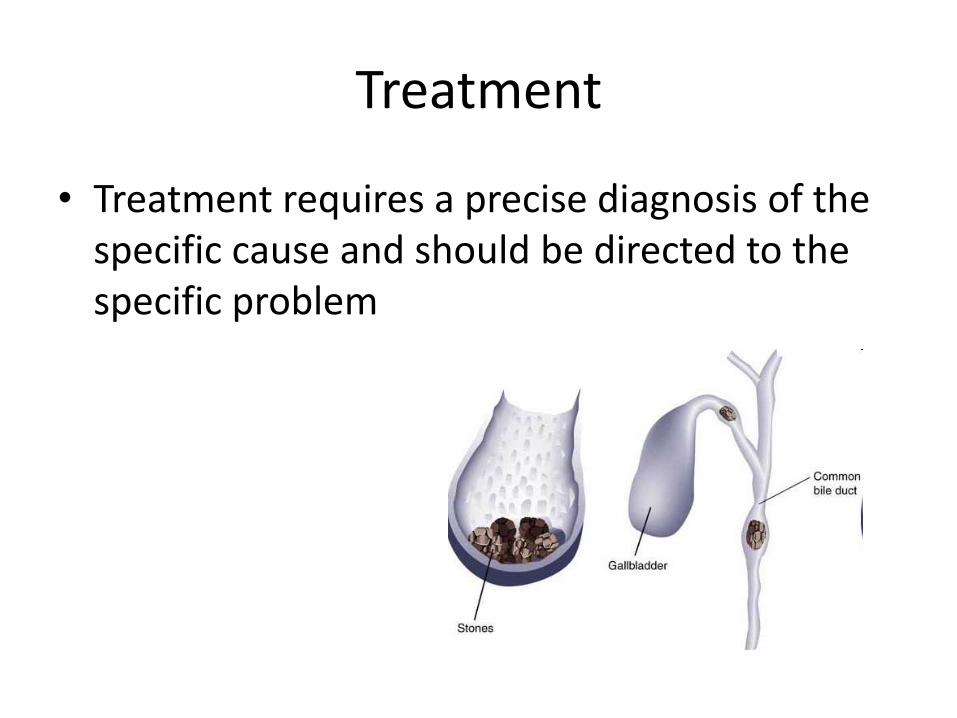
Treatment
• Treatment requires a precise diagnosis of the specific cause and should be directed to the specific problem
Treatment• In certain individuals with jaundice, the treatment will consist
of supportive care and can be managed at home. For example, most cases of mild viral hepatitis can be managed at home with watchful waiting and close monitoring by your doctor (expectant management).
• Alcohol cessation is necessary in patients with cirrhosis, alcoholic hepatitis, or acute pancreatitis secondary to alcohol use.
• Jaundice caused by drugs/medications/toxins requires discontinuation of the offending agent. In cases of intentional or unintentional acetaminophen (Tylenol) overdose, the antidote N-acetylcysteine (Mucomyst) may be required.
• Various medications may be used to treat the conditions leading to jaundice, such as steroids in the treatment of some autoimmune disorders. Certain patients with cirrhosis, for example, may require treatment with diuretics and lactulose.
Treatment
• Antibiotics may be required for infectious causes of jaundice, or for the complications associated with certain conditions leading to jaundice (for example, cholangitis).
• Blood transfusions may be required in individuals with anemia from hemolysis or as a result of bleeding.
• Individuals with cancer leading to jaundice will require consultation with an oncologist, and the treatment will vary depending on the type and extent (staging) of the cancer.
• Surgery and various invasive procedures may be required for certain patients with jaundice. For example, certain patients with gallstones may require surgery. Other individuals with liver failure/cirrhosis may require a liver transplant
Treatment
• Antihistamines may be used for the symptomatic treatment of pruritus, particularly as a sedative at night. Their effectiveness is modest. Endogenous opioidshave been suggested as possibly playing a role in the development of pruritus of cholestasis. Treatment with parentally administered naloxone and, more recently, nalmefene, has improved pruritus in some patients.
THE NEED FOR SURGICAL INTERVENTION DEPENDS ON THE CAUSE OF BILIARY OBSTRUCTION.
• Cholecystectomy is the recommended treatment in cases of symptomatic cholelithiasis because these patients have an increased risk of developing complications.Open cholecystectomy is relatively safe, with a mortality rate of 0.1-0.5 %.
• Laparoscopic cholecystectomy remains the treatment of choice for symptomatic gallstones, partially because of the shorter recovery period (return to work in an average of 7 d), decreased postoperative discomfort, and improved cosmetic result.
• Approximately 5% of laparoscopic cases are converted to an open procedure secondary to difficulty visualizing the anatomy or a complication.
RESECTABILITY OF NEOPLASTIC CAUSES OF BILIARY OBSTRUCTION
• Varies with respect to the location and extent of the disease. Photodynamic therapy (PDT) has been shown to have good results in the palliative treatment of advanced biliary tract malignancies, particularly when used in conjunction with a biliary stenting procedure.
• PDT produces localized tissue necrosis by applying a photosensitizing agent, which preferentially accumulates in the tumor tissue, and then exposing the area to laser light, which activates the medication and results in destruction of tumor cells.
• Liver transplantation may be considered in appropriate patients.

THANK YOU