Innovation in Cardiovascular Interventions New DES...
42
Innovation in Cardiovascular Interventions New DES, Scaffolds and other Devices Have Angioplasty Results Improved Alexandra Lansky, MD Yale University School of Medicine University College of London
Transcript of Innovation in Cardiovascular Interventions New DES...

Innovation in Cardiovascular Interventions
New DES, Scaffolds and other Devices
Have Angioplasty Results Improved
Alexandra Lansky, MD
Yale University School of Medicine
University College of London

3rd
Generation
2nd
Generation 1st
Generation
0.140 μm
(0.0055” )
Cypher®
Stent
0.091 μm
(0.0036”)
Endeavor®
Stent
TAXUS®
Liberté®
Stent
0.096 μm
(0.0038”)
TAXUS®
Express®
Stent
0.132 μm
(0.0052”)
ION™ /
TAXUS®
Element™
Stent
0.081 μm
(0.0032”)
4th
Generation
SYNERGY™ Stent
0.074 μm
(0.0029”)
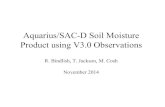
DES Evolution to Thinner Strut Thickness
Stainless Steel Cobalt Alloys Platinum Chromium
Reported strut thicknesses are for 3.0mm diameter
PROMUS
Element™
Stent
0.081 μm
(0.0032”)
Xience V®
and
Xience
Prime®
Stents
0.081 μm
(0.0032”)
current benchmark for lowest strut thickness
Coating Thickness:
12.6 µm 19.6 µm 4.8 µm 7.8 µm

Drug-eluting Stents: 2nd Generation
Drug Polymer
Xie
nce V
VDF + HFP copolymer Everolimus Vision
O
O
O O HO
O
O
O O H O
O O
N O
H O
Stent
Pro
mu
s
Ele
men
t
VDF + HFP copolymer Everolimus Element (Ion)
O
O
O O HO
O
O
O O H O
O O
N O
H O

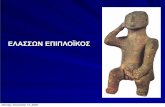
SPIRIT II, III, IV and COMPARE trials
Pooled database analysis (n=6,789)
MACE (Cardiac Death, MI, ID-TLR)
P<0.001
HR: 0.64 [0.54, 0.75] EES (n=4,247)
PES (n=2,542)
4247 4086 3942 3291
2542 2363 2269 1944
Number at risk
XIENCE
TAXUS
11.1%
Card
iac D
eath
, M
I,
Isc
he
mic
TL
R (
%)
0
15
Time in Months
0 3 6 9 12 15 18 21 24
3820
2193
7.3%
10
5
7.6%
4.4%
Kereiakes DJ et al. EuroIntervention 2011:7:74-83

SPIRIT II, III, IV and COMPARE trials
Pooled database analysis (n=6,789)
Stent thrombosis (ARC definite/probable)
4247 4177 4082 3479
2542 2463 2408 2110
Number at risk
XIENCE
TAXUS
2.3%
Ste
nt
thro
mb
osis
AR
C d
ef
or
pro
b (
%)
0
1
2
3
Time in Months
0 3 6 9 12 15 18 21 24
3998
2350
0.7%
p<0.001
HR: 0.30 [0.19, 0.47]
EES (n=4,247) PES (n=2,542)
Kereiakes DJ et al. EuroIntervention 2011:7:74-83

EXAMINATION Trial
0 1 2 3
Xience V
Vision
Acute Subacute Late
p = 0.01
1504 pts with STEMI undergoing PCI within 48 (85% primary PCI
within 12) were randomized to Xience V EES vs. Vision BMS
Stent thrombosis (Def/prob) within 1 year
2.6%
0.9%
Definite ST was reduced with Xience V from 1.9% to 0.5%, p=0.01
Sabate M et al. Lancet 2012

PLATINUM: Target Lesion Failure
Months Since Index Procedure
CoCr-EES
PtCr-EES
No. at risk
4-Year Follow-up (Primary Endpoint at 1 Year)
749 738 735 715 701 683 656 473
758 747 745 727 715 702 687 480
CoCr-EES (N=749)
PtCr-EES (N=758)
TL
F (
%) 8.5%
7.4%
Treatment Group PROMUS Element 0-4YPROMUS 0-4Y
Primary Endpoint
HR [95% CI] =
0.86 [0.60, 1.24]
P = 0.43
Kereiakes DJ et al. JACC 2014;63 (12):2905-4

Reso
lute
BioLinx Zotarolimus Driver
Drug Polymer Stent
Drug-eluting Stents: 2nd Generation
Hydrophilic
Hydrophobic
En
deav
or
Phosphorylcholine Zotarolimus Driver

Endeavor II Trial
Fajadet J et al. Circulation. 2006;114:798-806
1197 pts randomized to E-ZES vs. BMS
9 month
outcomes
E-ZES
(n=592)
BMS
(n=591) P
TVF (1 EP) 7.9% 15.1% 0.0001
- Death 1,2% 0.5% 0.34
- MI 2.7% 3.9% 0.26
- TLR 4.6% 11.8% 0.0001
- TVR 5.6% 12.5% <0.0001
Stent
thrombosis 0.5% 1.2% 0.22
In-segment binary restenosis
E-ZES: 13.2%
BMS: 35.0% P<0.0001
mm

Endeavor ZES
PROTECT Study Design
Largest RCT and first powered for ST
Cypher SES
6mo 4yr 3yr 30mo 18mo 24mo 12mo Clinical endpoints
5yr 30d
Real-world patients – N=8709 Single and multiple coronary artery lesions No limitations on number of lesions/vessels
1:1 Randomization
196 sites world wide in 5 continents
3-12 months of aspirin and clopidogrel
Primary endpoint: ARC definite or probable ST at 3 years
Powered for a 40% reduction with ZES
Camenzind E et al. Lancet 2012

Definite or probable stent thrombosis to 3 years
Patients at Risk
E-ZES 4357 4347 4222 4119
C-SES 4352 4344 4211 4100
PROTECT Primary Endpoint
Time After Initial Procedure (Years)
AR
C D
efi
nit
e / P
rob
ab
le S
T
0%
0 1 3
5%
2%
2
1%
Endeavor ZES (N = 4357)
Cypher SES (N = 4352)
1.42%
1.79%
3%
4%
Camenzind E et al. Lancet 2012
HR [95%CI =
0.81 [0.58-1.14]
P=0.22

Definite or probable stent thrombosis to 3 years
PROTECT Primary Endpoint
Camenzind E et al. Lancet 2012
Cypher SES (n = 4159) Endeavor ZES (n = 4181)
Late
(1 -12 months)
Early
(0-30 days)
Very late
(1-3 years)
P = 0.60
P = 0.02
P<0.001

P = 0.76 P = 0.21 P<0.0001
P = 0.03
Ra
te (
%)
Cypher SES (n = 4159) Endeavor ZES (n = 4181)
MI TVR Death TLR
PROTECT Secondary Endpoints - 3 years -
Camenzind E et al. Lancet 2012

Days after Initial Procedure
Cu
mu
lati
ve
In
cid
en
ce
of
Ev
en
ts
11.2% 10.7%
0%
0 180 360 540 720
20%
5%
15%
10%
EES (n=1,152)
R-ZES (n=1,140)
95% CI = 0.6% [-2.0%, 3.2%]
P = 0.73
RESOLUTE All-Comers: TLF (Cardiac Death, TV-MI or clinically-driven TLR)
Silber S et al. Lancet. 2011;377:1241-7

TWENTE (n=1,387)
Target Vessel Failure at 2-Year Follow-up
Tandjung K et al. J Am Coll Cardiol 2013;61:2406–16
0 60 120 180 240 300 360 420 480 540 600 660 720
TV
F (
%)
Follow-up (days)
0
5
10
15
20
25
30
Xience V (n=692)
Resolute (n=695)
P = 0.67
11.6%
10.9%

Stent Thrombosis Network Meta-analysis ARC Definite ST at 30 days
49 RCTs, 50,844 pts
Odds Ratio [95%] 30-day definite stent thrombosis*
CoCr-EES vs BMS
CoCr-EES vs PES
CoCr-EES vs SES
CoCr-EES vs End-ZES
CoCr-EES vs Res-ZES
PtCr-EES vs BMS
PtCr-EES vs PES
PtCr-EES vs End-ZES
PtCr-EES vs Res-ZES
SES vs BMS
0.21 (0.11-0.42)
0.27 (0.14-0.51)
0.40 (0.21-0.79)
0.22 (0.09-0.54)
0.07 (0.00-0.46)
0.06 (0.00-0.68)
0.07 (0.00-0.83)
0.06 (0.00-0.73)
0.02 (0.00-0.43)
0.54 (0.30-0.90)
Favors Stent 1
10 1 0.1 0.01
Favors Stent 2
Palmerini T et al. Lancet 2012:On-line

Stent Thrombosis Network Meta-analysis ARC Definite ST at 1 year
49 RCTs, 50,844 pts
Odds Ratio
[95%] 1-year definite stent thrombosis*
CoCr-EES vs BMS
CoCr-EES vs PES
CoCr-EES vs SES
CoCr-EES vs Res-ZES
CoCr-EES vs End-ZES
SES vs BMS
End-ZES vs SES
0.23 (0.13-0.41)
0.28 (0.16-0.48)
0.41 (0.24-0.70)
0.14 (0.03-0.47)
0.21 (0.10-0.44)
0.57 (0.36-0.88)
1.92 (1.07-3.90)
Favors Stent 1 Favors Stent 2
10 1 0.1 0.01
Palmerini T et al. Lancet 2012:On-line

Number at risk
XIENCE V 669 646 616 601 582 571 565 548 537 529 521
TAXUS 332 310 288 274 269 262 255 248 243 231 223
Months
SPIRIT III: Target Lesion Failure @5 years T
LF
(%
)
1-year HR
0.56 [0.34, 0.90]
p=0.01
5-year HR
0.64 [0.46, 0.89]
p=0.008
9.2%
5.4%
Δ3.8%
19.0%
12.7%
Δ6.3%
TLF = cardiac death, target vessel MI, or ischemic-driven TLR
0%
5%
10%
15%
20%
25%
30%
0 6 12 18 24 30 36 42 48 54 60
TAXUS Express (n=332) XIENCE V (n=669)
Stone GW et al. JACC 2011
~1.8%/yr event rate after year 1

Number at risk
XIENCE V 2458 2390 2364 2323 2281 2238 2212 2187 2162 2132 2116 2095 2074
TAXUS 1229 1166 1138 1119 1095 1069 1060 1049 1029 1019 1008 994 979
Ta
rge
t le
sio
n f
ail
ure
(%
)
Months
XIENCE V (n=2,458)
TAXUS Express (n=1,229)
p=0.02
HR [95%CI] =
0.78 [0.63, 0.97]
6.7%
4.0%
p=0.001
HR [95%CI] =
0.61 [0.46, 0.81]
Δ 2.7%
0
5
10
15
20
25
0 3 6 9 12 15 18 21 24 27 30 33 36
11.7%
9.2%
Δ 2.5%
p=0.004
HR [95%CI] =
0.71 [0.56, 0.90]
TLF = cardiac death, target vessel MI, or ischemic-driven TLR
Stone GW et al. JACC 2011
~2.6%/yr event rate after year 1
SPIRIT IV: Target Lesion Failure @3 years

Etiology of metallic stent events beyond 1 yr
Very late thrombosis and restenosis
Possible causes
1.Uncovered stent struts (thrombosis)
2.Persistent stimulation of SMCs, from adherent fibrin and/or
loss of normal vessel curvature
3.Abnormal shear stress from protruding struts and/or loss
of cyclic strain relief (compliance mismatch)
4.Chronic inflammation due to late foreign body reactions
and polymer hypersensitivity
5.Positive remodeling with strut malapposition
6.Strut fracture
7.Neoatherosclerosis

6-mo Taxus
%NC 8%
%DC 2%
9-mo Taxus
%NC 28%
%DC 8%
22-mo Taxus
%NC 39%
%DC 20%
48-mo BMS
%NC 40%
%DC 25%
57-mo BMS
%NC 57%
%DC 15%
Neoatherosclerosis: Transformation of Neointimal
Hyperplasia to Necrotic Core in BMS and DES
Kang SJ et al. AJC 2010;106:1561-1565

TCFA Development in Neointimal Hyperplasia
Is More Common with DES than BMS, occurs earlier,
and can rupture causing stent thrombosis and occlusion
Nakazawa G et al. J Am Coll Cardiol 2011;57:1314–22

Three Approaches to Improve Late
DES Outcomes
1. Metallic DES with bioabsorbable polymers
2. Metallic DES, polymer-free
3. Bioresorbable scaffolds (BRS)

Stefanini GG et al. EHJ 2012;33:1214–22
Ste
nt
thro
mb
osis
(%
)
2
0
0
3
4
5
HR (95% CI) DP BP
ISAR-TEST 3 1/202 2/202
ISAR-TEST 4 9/1299 10/652
LEADERS 20/857 32/850
Overall 30/2358
0.47 (0.04, 5.04)
0.45 (0.18, 1.12)
0.62 (0.35, 1.08)
44/1704 0.56 (0.35, 0.90)
0.1
Favors BP HR
10
Favors DP
0.22 [0.08, 0.61]
P=0.004
0.02 [0.47, 1.38]
P=0.43
1 2 3 4
1
Ste
nt
thro
mb
osis
(%
)
Years
2
0
0
3
4
5
HR [95%CI] = 0.56 [0.35, 0.90]
P=0.015
1 2 3 4
1
Biodegradable polymer Durable polymer
Years
Test for heterogeneity P=0.84
Test for inconsistency 12=0%
Test for overall effect z2=2.43 (P=0.015)
Meta-analysis of Bioresorbable Polymer DES:
ISAR-TEST 3, ISAR-TEST 4, and LEADERS at 4 yrs
4,062 randomized pts assigned to bioresorbable polymer
eluting sirolimus or biolimus A (2,388) or Cypher (1,704)
Definite Stent Thrombosis
1.3%
2.8%

Abluminal Bioabsorbable Polymer
SYNERGY Stent (BSC)
Abluminal
bioabsorbable
polymer (PLGA)
3-4 um thick
Thin PtCr stent
(74 – 81 um)
PLGA bioabsorbable
polymer + everolimus on
abluminal side of stent
Coating weight on 16
mm stent ~200 µg (vs
~685 µg for Xience /
Promus)
Everolimus elutes
over ~3 months
(similar to Xience /
Promus)
PLG undetectable by
~4 months, leaving
behind a BMS

291 Pts Randomized to
Promus Element vs. Synergy vs Synergy ½ dose Primary Endpoints
Meredith I et al. JACC 2012;59:1362–70
P=0.19
Late Loss at 6 Months TLF at 30 Days
Late
lo
ss, m
m
0.0
0.5
0.6
PROMUS
Element
SYNERGY SYNERGY
½ Dose
P=0.56
0.4
0.3
0.2
0.1
0.15 0.10 0.13
P=0.49
Targ
et
lesio
n f
ailu
re, %
0.0
8.0
10.0
PROMUS
Element
SYNERGY
P=0.25
6.0
4.0
2.0
0
1.1
3.1
SYNERGY
½ Dose

EVOLVE II Study Design SYNERGY Stent Pivotal Trial
Randomized cohort (RCT)
SYNERGY
N=842
PROMUS Element
N=842
RCT Design
Multicenter noninferiority trial
Single-blind, 1:1 randomization
Primary Endpoint: TLF at 12 mo
Follow-up: 30d, 6m, 12m, 18m and annual 2-5 yrs
2,006 pts with native coronary lesions ≤34 mm in length, RVD ≥2.25 mm - ≤4.0, %DS ≥50%
Up to 3 lesions in 2 vessels
(excludes LM disease, CTO, ISR, STEMI)
SYNERGY
N=250-292
SYNERGY
N=20-30
Diabetes
Substudy
PK
Substudy
Up to 160 global sites
Enrollment Complete

Selectively micro-structured surface
holds drug in abluminal surface
structures
BioFreedom Stent (Biosensors) Hypothesis: Polymer-free drug
release via porous-eluting
stents may reduce late events
caused by polymer stent
coatings.
Potential advantages
• Avoid long term late adverse
effects that might be
attributable to the polymer
• Improved surface integrity
since there is no polymer to be
sheared or pealed away from
the stent struts
• Possible shorter need of dual
antiplatelet therapy
Biolimus A9 - lipophilic

DFS: Drug Filled Stent (Medtronic)
Drug elution controlled by diffusion physics
Elution Holes

Bioresorbable Vascular Scaffold
A new paradigm providing temporary vessel support and then allow the
physiology to recover and evolve naturally.

BioResorbable Scaffolds
Scaffold Compromise is thicker struts (>130 μm )
150-220 μm
130 μm
157 μm
150 μm

Late Lumen Enlargement
Potentials of Fully Bioresorbable Coronary Scaffolds
Ormiston J et al. Circ Cardiovasc Interv 2012;5:620-32

Long-term Mechanical Differences between
Scaffolds and Metallic Stent Metallic Stent Scaffold
• Restoration of vascular physiology
• Restoration of cellular response
• Restoration of vasomotion and positive
remodeling
• “Caging” inhibits natural vessel
movement and remodeling
Baseline
1 year At 1 year, the
vessel is no longer
mechanically
constrained
At 6 months scaffold
begins to resorb

Cu
mu
lati
ve f
req
uen
cy d
istr
ibu
tio
n (
mm
)
Late loss (mm)
Late Loss with Absorb Cohort B vs. Xience V
6 month (SPIRIT II): 0.17 ± 0.32 mm (N=97)
24 month (SPIRIT II): 0.33 ± 0.37 mm (N=97)
6 month (Cohort B): 0.19 ± 0.18 mm (N=42)
24 month (Cohort B): 0.27 ± 0.20 mm (N=38)
Claessen BE et al. Circ CV Int. 2009;2:339-47
Serruys PW. ESC 2012

ABSORB II 1-Year Patient Flowchart
Intent To Treat N=501
Absorb BVS
N=335
N=334
N=331
N=329
(98.2%)
Xience N=166
N=166
N=165
N=164
(98.8%)
1 subject consent withdrawn
3 subjects consent withdrawn
2 subjects consent withdrawn
1 subject died
Baseline
30-day
180-day
1-year
1 subject consent withdrawn

Cumulative incidence in percentage Absorb 335 pts
Xience 166 pts
p value
Target Lesion Failure 4.8 % 3.0 % 0.35
Cardiac death 0 % 0 % 1.00
Target vessel MI 4.2 % 1.2 % 0.07
Clinically indicated TLR 1.2 % 1.8 % 0.69
All TLR 1.2 % 1.8 % 0.69
MACE 7.3 % 9.1 %
All death 0 % 0.6 %
All MI 4.5 % 1.2 %
All revascularization 3.6 % 7.3 %
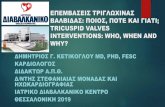
ABSORB II: Clinical Outcomes

Cumulative incidence in percentage Absorb 335 pts
Xience 166 pts
p value
Definite scaffold/stent thrombosis
Acute (0-1 day) 0.3 (1pt) 0.0 NS
Sub-acute (2–30 days) 0.3 (1pt) 0.0 NS
Late (31–365 days) 0.0 0.0 NS
Probable scaffold/stent thrombosis
Acute (0-1 day) 0.0 0.0 NS
Sub-acute (2–30 days) 0.0 0.0 NS
Late (31–365 days) 0.3 (1pt) 0.0 NS
ABSORB II: Definite scaffold/stent thrombosis

GHOST Registry Centers
Ferrarotto Hospital,
Catania
C. Tamburino (PI)
D. Capodanno (co-PI)
P. Capranzano
S. G. Di Dio Hospital, Agrigento
G. Caramanno
S. Geraci
San Raffaele Hospital and
Emocolumbus Clinic, Milan
A. Colombo
A. Lateeb
Klinikum Großhadern,
Munich
J. Mehilli
Medizinische Klinik, Mainz
T. Gori
ElisabethKrankenhaus, Essen
C. Naber
S. Pyxaras
Uniwersytet Medyczny, Poznan
M. Lesiak
A. Araszkiewicz
Royal Brompton Hospital,
London
C. Di Mario
A. Mattesini
University of Giessen, Giessen
H. Nef

*Compared to ABSORB II eligibility (Diletti et al. Am Heart J. 2012;164:654-63)
Clin
ical
An
gio
gra
ph
ic
GHOST: All Comers

CV Death All Death TV MI Any MI ID TLR ID TVR
Ghost: 6-Month Outcomes*
TLF** TVF ST
defin/prob

GHOST: Scaffold Thrombosis
1.5%
• There were 20 cases of angiographically confirmed ST and three of probable ST.
• 70% occurred in the first month after PCI, at a median of 5 days, suggesting the need for scrupulous lesion selection
and PCI techniques when using BVS
• Intravascular imaging was performed in only 9 of 23 patients who experienced ST
• 20 of 23 patients were on DAPT at the time of ST
• ST rates were numerically higher when more experience was accumulated and more complex patients were treated

Conclusions: Current and future
directions in stenting
• Current DES have improved safety and efficacy profiles
in ACS and stable CAD compared to first generation
devices
• By limiting polymer, polymer-free systems, or fully
bioresorbable scaffolds, will likely further reduce stent
thrombosis and improve late outcomes
• If BRS reduce very late events from 1-5 years and/or
stabilize or regress plaque, this will be transformative