High hepatic γ-glutamyltransferase (γ-GT) activity with normal serum γ-GT in children with...
4
High hepatic y-glutamyltransferase (y-GT) activity with normal serum y-GT in children with progressive idbpathic cholestasis Summary y-Glutamyl transferase o+-GT) was assayed in the serum and liver cii+iss ot children affected with either pro- gressive idiopathic cholestasis (PK. Bykr’s diseanr:. i)r other types of cholestatic (biliary atresia, cholestasis of various origins) and non-cholcstatic dicedses. The mean liver y-GT activity wtts increased significantly only in PIC and biliary are&+. In mntrost, the serum y-GT activity. raised in children with evident damage to the msin hilt ciucrs or to rhe interlobular bile ducts, was normal in children with PK. Although rhe mechanism for such a discrepancy between high liver and normal serum y-GT actir ties in PIC is still speculative, this peculiarity could prove 10 be of use in leading to a better cnderstandingof the disease. lntmduction Progressive idiopathic cholestaris (Byler‘s disease) is a probably heterogenous group of cholestatic dis- eases of childhood of unknown origin resubing in death dw to liver failure at ages ranging from infancy to adolescence (I]. It is likely lo be familial m origin in most instances and transmitted as an autosomal re- cessive trait. but it is poorly characterized since there are no absolute histological or biochemical criteria. Recently it was reported that, contrary to all other known causes of cholestasis in early infancy, a group of infants, affected with progressive idiopathic chole- stasis. were remarkable due to their nomml level of serum y-glutamyltransferase (?-CT) activity [2]; it was suggested that this peculiarity could be of use in the early iuentification of such children. Understand- ing the mechanism(s) responsible for the lack of in- crease of serum y-CT activity in spite of severe chole- stasis might also lead 10 progross in the understand-
Transcript of High hepatic γ-glutamyltransferase (γ-GT) activity with normal serum γ-GT in children with...

High hepatic y-glutamyltransferase (y-GT) activity with normal serum y-GT in children with progressive idbpathic cholestasis
Summary
y-Glutamyl transferase o+-GT) was assayed in the serum and liver cii+iss ot children affected with either pro-
gressive idiopathic cholestasis (PK. Bykr’s diseanr:. i)r other types of cholestatic (biliary atresia, cholestasis of
various origins) and non-cholcstatic dicedses. The mean liver y-GT activity wtts increased significantly only in
PIC and biliary are&+. In mntrost, the serum y-GT activity. raised in children with evident damage to the msin
hilt ciucrs or to rhe interlobular bile ducts, was normal in children with PK. Although rhe mechanism for such a
discrepancy between high liver and normal serum y-GT actir ties in PIC is still speculative, this peculiarity could prove 10 be of use in leading to a better cnderstandingof the disease.
lntmduction
Progressive idiopathic cholestaris (Byler‘s disease)
is a probably heterogenous group of cholestatic dis-
eases of childhood of unknown origin resubing in
death dw to liver failure at ages ranging from infancy
to adolescence (I]. It is likely lo be familial m origin
in most instances and transmitted as an autosomal re-
cessive trait. but it is poorly characterized since there
are no absolute histological or biochemical criteria.
Recently it was reported that, contrary to all other
known causes of cholestasis in early infancy, a group
of infants, affected with progressive idiopathic chole-
stasis. were remarkable due to their nomml level of
serum y-glutamyltransferase (?-CT) activity [2]; it
was suggested that this peculiarity could be of use in
the early iuentification of such children. Understand-
ing the mechanism(s) responsible for the lack of in-
crease of serum y-CT activity in spite of severe chole-
stasis might also lead 10 progross in the understand-

23
ing of the disease. In d first attempt in this direction,
we assayed y-CT activity in liver biopsy samples of
these children and compared them with liver :/-CT
activity of children with other types of cholesta!nc or
nonchokstatic diseases.
The liver biopsies of 21 childlen were studied.
These children were divided into four groups:
Group I (control group): 5 children aged 2 months
to 9 years. with histologically normal liver and nor-
mal liver function tests including serum ptiT activi-
ty. There were 3 children with portal vein obstruc-
tion. one brother of a child with Wilson’s disease in
whom liver histology was normal and one 2-mouth-
old infant who underwent liver needle biopsy for at-
say of giucuronrltransferzse activity because ol pro-
longed neonatal unconjugnted hyperbilirubbemia.
Group II: 5 children aged 2 months to 2 ? yezrx
with prur;resnve idtopalhlc cholestasis who exhibited
persistently normal serum y-CT activity.
Group III: 5 children with biliary atresia aged 2 to
4 months. Group IV: 6 children aged I month to I4 years with
cholestnsis of various origins: 2 had benign idiopnthic
neonatal cholrstasis (‘neonatal hepatitis’), 3 had sclc-
rosingcholangitis and one syndromic paucity of inter-
lobular bile ducts.
Methods
Needle or wedge liver biopsies were immediately
frozen and stored m liquid nitrogen until use. 2.5-10
mg of liver were homogenized in ice-cold 50 mM Tris
pH 7.4 with a 2 ml capacity Dounce homogenizer at a
tinal concmtratio:1 of 6-16 mg of tissue/ml. y-Glut,,-
myl transferase activity in homogenates was deter-
mined as previously described [3]. according to the
method of Orlowski and Meister I.!]. using L-gluta-
myl-p-nitroanilide as substrate ano glycylglycine as
receptor. The assay mixture was filtered (Whatma?
GWF) in order toclarify the solution before measure-
mem of absorbance at 405 nm. Proteins were esti-
mated by the procedure of Lowry et al. [S]. For each
homogenate. assays were done in triplicate. Enzyme
activity WBS expressed as mU/mg protein: I mU of
enzyme ccrrcs~nds to 1 nmol of product formed per
mm. Serum y-GT activity was meawred using an au-
toma’ed OLLI-KONE apparatus and rcsolts were
expressed in lU& normal levels are below 35 IlJ/I.
Differences between the groups were tested using
the fiat-parametric Mann-Whitney test (P < O.(iS
wns considered significant).
Results
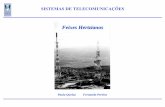
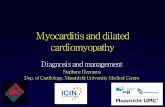
Eesults of serum arid liver y-GT measurements are
indicated in Fig. 1. Serum y-CT activity (panel ,I$)
was wi:hm normal limits in all children of group :
(mean 13.8 llJ/I) and group II (mean 22 IU/I); it was
raised in groups III (mean 727 IUil) and IV (mean
342 !t_‘!l). Menn liver y-CT activity (pex! 91 yi;s i3
mU/mg of protein in group 1. 37.6 mU/mg in group
II, 31 mU/mg in group 111 and 21.2 mU/mg in group
IV. The dlfterences between liver y-CT in group ti
(progressive Idiopathic cholestasis) and 111 (biliary
at&a) on the one hand and l+~er ?-CT in group I
(control) on the other hand are stetistically sipnifi-
cant (P < 0.008). The differences between liver y-
GT in group IV and liver y-CT in group I are not sta-
tistically ripnificant.
No correlation could be found between the levels
of serum aad liver y-GT activities in children of
groups II I and IV (data not shown).
These results indicate that the liver T-CT activity is
significantly raised in two groups of children with se-
vere. cholestatic diseases: progressive idiopathic
cholestasis and biliary atresia (groups II and III).
This increase may be secondary to the activation of
transcription or translation of the y-GT gene(s) in
liver cells, secondary to cholestasis, as has been sug-
gested for alkaline phosphatase [6]. However, the

24 M.-N. CHOBERT et at.
A
* .
I II lu m Ftg. 1. Sewn (A) and twer (8) r.GTartivities in 21 childrex. I: contr”t group: It. childrun wth progressive idiopathic chote- sm=.ix 111: chddren wh biliary mesia: IV. children with vari-
PUS other cholestnte disorders.
discrepancy ohserved in children with progressive
idiopathic cholestasis between high liver p-GT activi-
ty and the normal serum activity is unique. Such a dis-
crepancy has not heen reported in adult patients with
liver diseases [i’] and was not observed in the children
with other types of rholestaric diseases reported
here. In fact. liver and serum PGT activities are not
necessarily related and similar observations have
been made using experimental models: in one hepa-
toma cell line (C2). where y-CT activity is induced 2.
fold by ethanol. there is B concomitant release of y-
2 Me$piorc G. Bernard 0. Ricty C. Hadchouel M. Lcmon- nicr A. Atagitte U. N0rm.d serum gmnmu-gtulamyttrans. Ierase ncurity idcnutier pruupr <rt inlvnls with idiopathac
GT into the medium, while in another (Fao). where
y-CT is increased by glucocorticcids. there is no re-
lease of y-GT into the culture medium, although in
bothcasesthe viability of thecetlsisnot altered [8,9].
Two hypotheses may be advanced to account for
the discrepancy between high liver and normal serum
y-CT activities in children with progressive idiopa-
thic chotestasis. The first hypothesis would imply that
the increased ]-GT activity in the serum is related to
biliary epithelium damage [IO]. This would explain
why serum y-CT activity is raised in children where
damage to the main bale ducts (e.g. hiliarj atresie,
group Ill) or to interlobular bile ducts (e.g. bile duct
paucity, group IV) is evident. but is not raised in the
group of children witlr progressive idiopathic chole-
stasis studied here who do not exhibit iw.tological
signs of bile duct damage [2]. Accorditgly this hy-
pothesis would point to a hepatocytic r:tther than
ductular disorder in adult patients with benign recur-
rent intrahepatic cholestasis in whom serum y-CT ac-
tivity remains within normal limm [II]. The other
hypothesis would favor a genetic difference. between
progressive idiopathic cholestasis and other types of
cholestasis, concerning the intracellular transport.
the anchoring to the cell membrane. or the transport
in the serum of the pGT molecule. Such alterations
in the procassing of y-GT have been reported in both
rat and human hepatoma cell lines [12,131. The re-
cent availability of a human DNA probe specific for
Y-CT will now be used for further investigation of this
condition 1141.
Acknowledgment
We thank Mme M. Grelirr for help with the prepa-
ration of the manu.cript.
chotestais with pax tvogw~;~ ! %diatr 19X7: t It. 251-252.
3 Bsrouki R. Chohert M-N. Billon M.C. Finidura J. Tsapis R. Hrnoune 1. Gtucocorticoid hormones increase the act@ orgnmma-stut3myltmnrlerare in P highly differcnliated he- patomacct, tme. Blochim Bwphys Acta ,!X,?:??!: ,!-?I.
4 Orlawrki M. Mcisrcr A. tsotatiua ol panlma-gtutamyttnns-

CGT AND BYLER‘S DlSEASE
peptidare from hog kidney J Bml Chem 19fS: 240: 338-347.
5 Lowry OH. Rosebrough NJ. Fan AL. RIndall RJ. Pratem measuremem wh ohs Folin phenol reagent. J Bial Chem ,951: 193: 2hS-27.5.
h Seetharam S. Sussman N. Ko~wda 7. Alpcrr DH. The mechanism of elevared alkdlinc phosphr?tase acbvity afrcr bile dw ligation an the rat. Hepatoiogy 1986; 6: 374-380.
7 Selingxr HJ. Mi,Boff “S. Kaplan MM. Gamma-gl”tamyi-
8 Barouki R, Chabert M-N. Fm,dori J. Agpchreck K. Nalpx B. H~noune J. Ethanol elfcc,s in a rat hep.,,oma ce:l line: mdwwn of gamma-glutamyltranrlerase. HepaloioSy
1983;3: 323-329.





![Nandaana tamil pan · PDF file · 2012-03-07q>V ºvkV vx› Ø> qÔvDs›v\V¸´BD I q¤™V¨i¶ >V>V´D qº√Vº>Õ]´ zÚD √º¤ II q•¬y ¤VÈvN>D q¤≤º\V> ÔVˆ™D I](https://static.fdocument.org/doc/165x107/5aba1bd97f8b9a297f8b4830/nandaana-tamil-pan-vkv-vx-qvdsvvbd-i-qvi-vvd-qv-zd-ii-qy-vvnd.jpg)