Surgical Anatomy of the Liver : Ηepatectomies - Dimitris P. Korkolis
Upload
konstantinCategory
view
214download
0
ECc
IAa
b
c
a
ARRA
KLLMTQ
1
arnttcap
h0
European Journal of Radiology 83 (2014) 900–904
Contents lists available at ScienceDirect
European Journal of Radiology
j ourna l h o mepage: www.elsev ier .com/ locate /e j rad
valuation of T1� as a potential MR biomarker for liver cirrhosis:omparison of healthy control subjects and patients with liverirrhosis
sabel Rauschera,∗, Matthias Eibera, Carl Gantera, Petros Martirosianb, Wajima Safic,ndreas Umgelterc, Ernst J. Rummenya, Konstantin Holzapfela
Department of Diagnostic and Interventional Radiology, Technical University Munich, Ismaninger Str. 22, 81675 Munich, GermanySection on Experimental Radiology, University Tübingen, Hoppe-Seyler-Str. 3, 72076 Tübingen, Germany2nd Medical Department, Technical University Munich, Ismaninger Straße 22, 81675 Munich, Germany
r t i c l e i n f o
rticle history:eceived 29 November 2013eceived in revised form 15 February 2014ccepted 18 February 2014
eywords:iver cirrhosisiverRI
1rhouantification
a b s t r a c t
Objectives: The purpose of this study was to compare mean liver T1� values in patients with liver cirrhosisand healthy control subjects in order to evaluate T1� as a potential MR biomarker for liver cirrhosis.Materials and methods: Ten healthy control subjects (mean age 42.7 years; 6 female, 4 male) and 21patients with clinically diagnosed liver cirrhosis (mean age 56.5 years; 5 female, 16 male) were exam-ined at 1.5 T (Magnetom Avanto, Siemens). T1�-weighted images were acquired using a 2D TurboFLASHsequence (TR/TE 3/1.31 ms, FA 8◦, FoV 309 × 380 mm, resolution 2 × 2 × 6 mm, acquisition time 15 s, slicethickness 6 mm) with spin-lock preparation. T1� maps were calculated from five breath-hold measure-ments, performed with different spin-lock times (4, 8, 16, 32 and 48 ms). Mean liver T1� values of healthycontrol subjects and patients with liver cirrhosis were calculated and compared using Student t-test. Inaddition, a receiver operating characteristic (ROC) curve analysis was performed to evaluate the utilityof mean liver T1� values for the prediction of liver cirrhosis.Results: Mean liver T1� values in patients with liver cirrhosis (57.4 ± 7.4 ms) were significantly higher than
those of healthy subjects (47.8 ± 4.2 ms; p = 0.0007). According to the ROC analysis at a threshold value of50.1 ms the sensitivity and specificity of mean liver T1� in predicting liver cirrhosis were 90.5% and 90%,respectively. The area under the ROC curve was 0.90.Conclusion: Mean liver T1� values in patients with liver cirrhosis were significantly higher than those inhealthy subjects suggesting a potential role of liver T1� as a MR biomarker for liver cirrhosis.© 2014 Elsevier Ireland Ltd. All rights reserved.
. Introduction
Progressive hepatic fibrosis with the development of cirrhosis is feature of almost all chronic liver diseases. It is characterized byeplacement of liver tissue by fibrosis, scar tissue and regenerativeodules leading to loss of liver function, and ultimately progresso liver cirrhosis. In Europe, alcohol abuse and chronic viral infec-ions of the liver (hepatitis types B and C) are the most commonauses of liver cirrhosis. Originally, hepatic fibrosis was considered
s irreversible but is now regarded as a dynamic process with theotential for regression [1,2].∗ Corresponding author. Tel.: +49 89/4140 2621; fax: +49 89/4140 4834.E-mail address: [email protected] (I. Rauscher).
ttp://dx.doi.org/10.1016/j.ejrad.2014.02.017720-048X/© 2014 Elsevier Ireland Ltd. All rights reserved.
The diagnosis of cirrhosis is usually based on physical exami-nation, blood tests, and imaging techniques such as ultrasound, CT(computed tomography) and MRI (magnetic resonance imaging).Liver biopsy is currently considered the gold standard for diagnos-ing liver cirrhosis. In practice, limited sampling locations, bleeding,and the possibility of infection are the main disadvantages of aninvasive biopsy. Biopsy has been determined to have morbidityand mortality rates of 3% and 0.03%, respectively [3]. Identifyingcirrhotic tissue is difficult because only 1/50,000 of liver tissue issampled in a biopsy. Therefore, the rate of false-negative diagnosesof liver cirrhosis is artificially increased [4].
T1� describes the spin-lattice relaxation in the rotating frame
and reflects the interactions between motionally restricted watermolecules and their local macromolecular environment [5].Changes in the extracellular matrix, such as proteoglycan or col-lagen loss, may be reflected in measurements of T1�. First studies
I. Rauscher et al. / European Journal o
Table 1Patient characteristics of each patient with liver cirrhosis with age, child-pugh-score(CPS) and origin of liver cirrhosis (hepatitis B, C or alcohol-related).
Patient no. Age in years Origin of liver cirrhosis CPS
1 44 Alcoholism B2 52 Alcoholism B3 45 Hepatitis B A4 23 Alcoholism B5 63 Alcoholism B6 67 Hepatitis B C7 54 Hepatitis C A8 61 Alcoholism B9 51 Alcoholism A
10 63 Alcoholism A11 66 Alcoholism A12 55 Hepatitis C B13 49 Hepatitis C B14 61 Hepatitis B A15 63 Alcoholism B16 49 Alcoholism C17 48 Alcoholism A18 69 Hepatitis C A19 80 Hepatitis C B20 70 Alcoholism B21 53 Hepatitis C B
hgd[cocwmdpppmspola
2
2
rs(25dNajpaic
vessels were excluded visually through an upper threshold. Addi-tionally, a circular ROI was placed in the erector spinae muscle toserve as a control region independent from the presence of liver
ave used the spin-lock technique in the evaluation of neurode-enerative changes in patients with Alzheimer’s disease [6] oregeneration in articular cartilage and in the intervertebral disc7–10]. Histopathologic studies have shown that liver cirrhosis isharacterised by an accumulation of collagens, proteoglycans, andther macromolecules in the extracellular matrix. Therefore, T1�
ould be a valuable tool not only for the early diagnosis of fibrosishen it’s still reversible but also for therapeutic monitoring as itay allow sensitive detection of structural and functional changes
uring the early stages of liver cirrhosis. Recent studies have shownromising results of T1� MR imaging to reveal changes in the com-osition of the liver tissue. Wang et al. [11] showed that T1� becamerolonged after bile duct ligation- induced liver injury in an animalodel and that T1� values increased with the severity of liver fibro-
is. To our knowledge, T1� measurements of the liver have only beenerformed in healthy human subjects [12]. Therefore, the purposef this study was to compare mean liver T1� values in patients withiver cirrhosis and healthy control subjects in order to evaluate T1�
s a potential MR biomarker for liver cirrhosis.
. Materials and methods
.1. Subjects and clinical assessment
The study was performed in accordance with the rules andegulations of the local ethics committee. Written informed con-ent was obtained from all subjects. Ten healthy control subjectsn = 6 female, n = 4 male; mean age 42.7 ± 12.4 years; age range7–65 years) and 21 patients (n = 5 female, n = 16 male; mean age6.5 ± 12.1 years; age range 23–80 years) with clinically/laboratoryiagnosed liver cirrhosis were recruited from January 2012 toovember 2012. n = 8 patients had a Child-Pugh score (CPS) A, n = 11
CPS B and n = 2 a CPS C. Inclusion criteria for all healthy sub-ects and patients were good health according to medical history,hysical examination, and clinical laboratory data as well as thebsence of contraindications to MR imaging. Control subjects werencluded if they had no clinical evidence of liver disease. Patient
haracteristics are shown in Table 1.f Radiology 83 (2014) 900–904 901
2.2. Imaging techniques
All 31 subjects were examined at 1.5 T (Magnetom Avanto,Siemens Healthcare, Erlangen, Germany). Measurement of the liverwas performed head first in supine position using a combinationof body and spine matrix coils for signal reception. T1� measure-ments were performed just on one plane and not volumetric.T1�-weighted images were acquired using a spin-lock (SL) pre-pared sequence. The longitudinal magnetization was prepared bya non-selective RF pulse train 90◦
x - SLy - 90◦−x with a SL pulseamplitude of 400 Hz (∼9.4 �T). After the spoiling of the resid-ual transverse magnetization, the SL-prepared magnetization wasimaged using a 2D single-shot FLASH sequence (TR/TE 3/1.31 ms, FA8◦, FoV 309 mm × 380 mm, resolution 2 mm × 2 mm × 6 mm, acqui-sition time 15 s, slice thickness 6 mm). T1� maps were calculatedfrom five breath-hold measurements in expiration, performed withdifferent SL times (TSL = 4, 8, 16, 32 and 48 ms). To increase signal-to-noise ratio (SNR), the average signal of five identical SL-scans(separated by 3 s) was obtained in each breath-hold. To reduceundesired effects due to B0 inhomogeneity, the measured slice wasplaced in the isocenter of the magnet, followed by a 3D volumeshim.
2.3. T1� quantification
A sufficiently long time between consecutive spin-lock pulses(3 s) was chosen to allow for an essentially complete repolarizationof longitudinal magnetization of liver tissue at 1.5 T. Immedi-ately after SL-preparation, a centric k-space sampling scheme wasemployed in phase encoding direction. Taking both together, theacquired signal is in good approximation proportional to the avail-able longitudinal magnetization, which can be simply expressedas:
ST1� (TSL) ≈ S0 exp
(−TSL
T1�
)+ noise (1)
For largest TSL (48 ms), SNR was still high enough (>5) todescribe the noise term by zero mean Gaussian distribution, withsome constant variance �2. For a time-efficient maximum likeli-hood (ML) estimation of T1�, the linear pre-factor S0 was eliminatedanalytically with the variable-projection technique [13], and theremaining one-dimensional problem was solved numerically withthe golden section search (GSS) algorithm [14].
2.4. Image post-processing
Magnitude data were exported and T1� maps were calculatedoffline (Matlab 8.0, Natwick, MA) via self-written software. In theTSL = 4 ms image, a region of interest (ROI) was selected per handwithin the liver and copied to all other TSL images. To reduce pos-sible B0 effects to the spin-lock preparation, the ROI was restrictedto the right liver lobe. Based on the TSL = 48 ms image, hyperin-tense vessels were separated from normal liver tissue and excludedfrom the analysis. The acquisitions were measured in expirationand showed little relative displacement. Moreover, the T1� mapswere essentially constant within the liver. Therefore no image reg-istration was performed. After calculating T1� maps pixel-by-pixel,
cirrhosis.

9 rnal of Radiology 83 (2014) 900–904
2
7umwttpfbTro
3
(ssTtp
AtwcpTw
tcc
wp
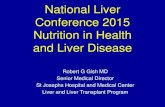
Fig. 1. Graph (box plots) shows mean liver T1� values of healthy subjects andpatients with liver cirrhosis. The horizontal line is the median (50th percentile)of the measured values, the top and bottom of the box represent 25th and 75thpercentiles, respectively, and whiskers indicate the range from the largest to thesmallest observed data point within 1.5 interquartile presented by the box. Notethat T values of patients with liver cirrhosis (57.5 ms ± 7.4 ms) are significantly
Fl
02 I. Rauscher et al. / European Jou
.5. Statistical analysis
Statistical analysis was performed using MedCalc Version.2.0.2. software package for windows. Descriptive statistical eval-ation was performed, and differences in liver and erector spinaeuscle T1� values between healthy control subjects and patientsith liver cirrhosis were compared by using two-sample Student’s
test. Differences were deemed to be significant at p < 0.05. In addi-ion, a receiver operating characteristic (ROC) curve analysis waserformed to assess the diagnostic performance of mean liver T1�
or the prediction of liver cirrhosis and its ability to differentiateetween subjects with and without liver cirrhosis [15]. In addition,1� values of healthy subjects were correlated with subject age (cor-elation coefficient r and p-value) to evaluate a possible influencef age on mean liver T1� values.
. Results
Mean liver T1� values in patients with liver cirrhosis57.4 ms ± 7.4 ms) were significantly higher than those of healthyubjects (47.8 ms ± 4.2 ms; p = 0.0007). The results of each healthyubject and patient with liver cirrhosis are summarized in Fig. 1.here was no significant difference (p = 0.23) between mean erec-or spinae muscle T1� values in healthy subjects (30.7 ± 2.8 ms) andatients with liver cirrhosis (33.7 ± 3.9 ms).
Separating the patients with liver cirrhosis into those with CPS and CPS B, both revealed a significant difference compared to
he healthy control group, although the difference for patientsith CPS B compared to healthy control subjects was more signifi-
ant (p = 0.001 compared to p = 0.01). Due to limited sample size ofatients with CPS C (n = 2) a statistical comparison was not possible.here was no significant difference in T1� values between patientsith CPS A and patients with CPS B.
According to the ROC analysis at a threshold value of 50.1 mshe sensitivity and specificity of mean liver T1� in predicting liverirrhosis were 90.5% and 90%, respectively. The area under the ROC
urve was 0.90.There was no significant correlation of subject age comparedith mean liver T1� within the healthy control group (r = 0.33;
= 0.35).
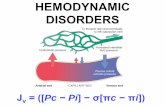
ig. 2. Representative T1�-weighted images of a healthy subject (28 years, T1� = 46.0 ms)iver inside a hand segmented ROI (C) and with excluded liver vessels (D) are shown as co
1�
higher than those of healthy subjects (47.8 ms ± 4.2 ms; p = 0.0007) with a smalloverlap.
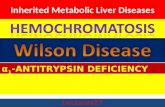
In Fig. 2, representative T1�-weighted images of a healthy sub-ject are shown with a TSL of 4 ms (A) and 48 ms (B). As colouredoverlays, Figs. 2C and D show the calculated T1� maps of the seg-mented liver tissue and the segmented liver with excluded vessels,respectively. Fig. 3 demonstrates an example of the T1� map of ahealthy control subject (A) and a patient with liver cirrhosis CPS A(B). T1� value of the healthy subject was 49.1 ms and T1� value ofthe patient with liver cirrhosis was 55.7 ms.
4. Discussion
In this study we showed that T1� can serve as an imagingbiomarker for identifying patients with liver cirrhosis. We founda significant difference in mean liver T1� values between healthy
with a spin-lock time of 4 ms (A) and 48 ms (B). In the lower part, T1� maps of theloured overlays. Colour bar shows T1� values in ms.

I. Rauscher et al. / European Journal o
Fig. 3. Segmented T1� map of a 28-year old healthy control subject (A) and a 45-year old patient with liver cirrhosis Child-Pugh score A (B). T1� value of the healthysC
srsTsb
lvohrf4oIhddIp
tedsawa
ubject was 49.1 ms and T1� value of the patient with liver cirrhosis was 55.7 ms.olour bar shows T1� values in ms.
ubjects and patients with liver cirrhosis. This difference most likelyeflects fibrosis within the liver matrix as indicated in previoustudies [11,16]. However, although the comparison of mean liver1� values between healthy subjects and patients with liver cirrho-is was significantly different, individual data show some overlapetween T1� values, so on a per patient basis this could be different.
To our knowledge, there has been no study of MR-based T1�
iver measurements on patients with liver cirrhosis published pre-iously. Deng et al. [12] were the first performing T1� MR imagingf the liver at 1.5 T to demonstrate the T1� dispersion of the liver inealthy human subjects. In his study, mean T1� values of the liveranged from 38.6 to 48.3 ms with no significant difference in theasting status and in the post meal status, the mean T1� value was3.0 ± 2.2 ms. Our study revealed slightly higher mean T1� valuesf the liver in healthy subjects (47.8 ± 4.2 ms; range 41.7–56.1 ms).n an experimental study with a rat biliary duct ligation model [11]istopathologic analysis revealed the highest content of collagen onay 24 after surgery. Corresponding mean T1� values of the liver onay 24 showed a 23.5% higher mean liver T1� than in control rats.
n terms of our study, we found a 20.1% higher mean liver T1� inatients with liver cirrhosis than those of healthy human subjects.
Several MR imaging-based techniques have been used inhe assessment of liver fibrosis including conventional contrast-nhanced MRI, double contrast-enhances MRI, MR elastography,iffusion-weighted MR imaging, MR perfusion imaging, and MR
pectroscopy [17]. In conventional MRI, morphologic signs ofdvanced cirrhosis can be observed such as surface nodularity,idening of fissures, expansion of the gallbladder fossa, notchingnd atrophy of the right lobe, and relative enlargement of the left
f Radiology 83 (2014) 900–904 903
lobe and caudate lobe [18]. MR elastography quantifies the stiff-ness of the liver by analyzing the propagation of mechanical wavesthrough tissue [19] whereas MR perfusion imaging utilizes the factthat liver fibrosis gradually obliterates normal intrahepatic vesselsand sinusoids and slows passage of blood through the parenchyma[20]. The central hypothesis behind the use of diffusion-weightedimaging for the imaging of liver fibrosis is the purpose that fibrosisrestricts water diffusion [21]. The advantage of T1� compared to allthese methods is that it is supposed to measure the biochemicalcomposition and therefore liver fibrosis itself rather than imagingsecondary signs of fibrosis.
To evaluate whether T1� can serve as a MR biomarker for livercirrhosis we used a 2D technique in this pilot-study as we onlywanted to analyse one representative section of the liver. This hasthe advantage that T1� as a 2D technique offers short acquisitiontime and low SAR.
A potential problem in T1�-weighted imaging in high mag-netic fields is the specific absorption rate (SAR). The addition ofthe SL pulse cluster significantly increases the SAR, and with theincreasing prevalence of high field (3 T and more) scanners, SARbecomes more of a concern due to the quadratic dependenceof SAR on the Larmor frequency [22]. Here, the 2D single-shotFLASH sequence offers the great advantage that the complete k-space is acquired after solely single spin-lock preparation pulse[23].
It is possible that there are confounding factors such as degree ofsteatosis or the presence of iron load that yield to increase the localmagnetic field inhomogeneity and thereby could affect T1� mea-surements. Fat suppression and using of strong SL radiofrequencypulses could help to reduce the influence of these undesired effects.Here further evaluation is needed.
Our experience with breath-hold T1� measurements in expira-tion produced reliable positions within the liver because in general,the variation in normal subjects is low. Nevertheless in the future,better results could be expected with navigator-controlled acqui-sition.
Our study has some limitations: Due to practical and partic-ularly ethical reasons no histologic correlation was obtained. Inour clinical routine the diagnosis of liver cirrhosis is usually basedon clinical and laboratory results and only in a minority of casesa histological confirmation is necessary. Here, further studies arerequired to evaluate the relationship between histopathology ofpatients with liver cirrhosis and T1� measurements. Furthermore,clinical evaluation of T1� measurements including correlation withlaboratory data, different levels of liver cirrhosis (CPS, MELD score)and results of other imaging modalities (e.g. elastography, ultra-sound, MRI) is needed as well as reproducibility testing. In ourstudy, we focused on patients with early levels of disease (CPS Aor B, except of two patients with CPS C) because the main advan-tage of T1� as a biomarker could be the evaluation of early signsof cirrhosis. The clinical symptoms of patients with CPS C includeascites and hepatic encephalopathy therefore diagnosis is simpleand the patients are often too sick to undergo a MR examinationwith multiple breath-holds.
In the future, one important clinical goal would be to assess andpossibly identify not only cirrhosis with T1� measurements but alsoearly stages of fibrosis and to differentiate these stages since fibrosisis still reversible. Here further studies are warranted and promisingsince the current study can only provide an outlook and is not basedon actual data.
We cannot completely exclude that in our study age is an con-founding factor as the healthy control group (42.7 ± 12.4 years) was
slightly younger than the patients with liver cirrhosis (56.5 ± 12.1years). Therefore furthers study should also focus on the evaluationof the influence of age on T1� measurements, although our initalresults did not show a significant correlation with subject age.
9 rnal o
5
iTtmttaf
R
[
[
[
[
[
[[
[
[
[
[
[
04 I. Rauscher et al. / European Jou
. Conclusion
Our study suggests that liver cirrhosis is associated with anncreased T1� compared to healthy human subjects and therefore1� may serve as a MR biomarker for liver cirrhosis. With furtherechnical development and clinical evaluation of T1�, this technique
ay play an important role in the early detection of liver cirrhosis,he assignment of the grade of liver fibrosis and the evaluation ofreatment. Consequently, larger prospective studies are promisingnd warranted to further evaluate the role of T1� relaxation timeor assessing liver cirrhosis.
eferences
[1] Arthur MJ. Reversibility of liver fibrosis and cirrhosis following treatment forhepatitis C. Gastroenterology 2002;122:1525–8.
[2] Gieling RG, Burt AD, Mann DA. Fibrosis and cirrhosis reversibility - molecularmechanisms. Clin Liver Dis 2008;12:915–37, xi.
[3] Janes CH, Lindor KD. Outcome of patients hospitalized for complications afteroutpatient liver biopsy. Ann Intern Med 1993;118:96–8.
[4] Regev A, Berho M, Jeffers LJ, et al. Sampling error and intraobserver varia-tion in liver biopsy in patients with chronic HCV infection. Am J Gastroenterol2002;97:2614–8.
[5] Becker EDFT. Pulse and Fourier Transform NMR: Introduction to Theory andMethods 1971.
[6] Borthakur A, Sochor M, Davatzikos C, et al. T1rho MRI of Alzheimer’s disease.Neuroimage 2008;41:1199–205.
[7] Regatte RR, Akella SV, Lonner JH, et al. T1rho relaxation mapping in humanosteoarthritis (OA) cartilage: comparison of T1rho with T2. J Magn Reson Imag-ing 2006;23:547–53.
[8] Wang L, Chang G, Xu J, et al. T1rho MRI of menisci and cartilage in patients withosteoarthritis at 3 T. Eur J Radiol 2012;81:2329–36.
[
[
f Radiology 83 (2014) 900–904
[9] Wang YX, Zhao F, Griffith JF, et al. T1rho and T2 relaxation times for lumbardisc degeneration: an in vivo comparative study at 3.0-Tesla MRI. Eur Radiol2012;23:228–34.
10] Zobel BB, Vadala G, Del Vescovo R, et al. T1rho magnetic resonance imag-ing quantification of early lumbar intervertebral disc degeneration in healthyyoung adults. Spine (Phila Pa 1976) 2012;37:1224–30.
11] Wang YX, Yuan J, Chu ES, et al. T1rho MR imaging is sensitive to evaluate liverfibrosis: an experimental study in a rat biliary duct ligation model. Radiology2011;259:712–9.
12] Deng M, Zhao F, Yuan J, et al. Liver T1rho MRI measurement in healthy humansubjects at 3 T: a preliminary study with a two-dimensional fast-field echosequence. Br J Radiol 2012;85:e590–5.
13] Golub GH, Pereyra V. Differentiation of pseudo-inverses and nonlinearleast-squares problems whose variables separate. Siam J Numer Anal1973;10:413–32.
14] Kiefer J. Sequential minimax search for a maximum. P Am Math Soc1953;4:502–6.
15] Metz CE. Basic principles of ROC analysis. Semin Nucl Med 1978;8:283–98.16] Zhao F, Wang YX, Yuan J, et al. MR T1rho as an imaging biomarker for monitoring
liver injury progression and regression: an experimental study in rats withcarbon tetrachloride intoxication. Eur Radiol 2012;22:1709–16.
17] Faria SC, Ganesan K, Mwangi I, et al. MR imaging of liver fibrosis: current stateof the art. Radiographics 2009;29:1615–35.
18] Dodd 3rd GD, Baron RL, Oliver 3rd JH, et al. Spectrum of imaging findings of theliver in end-stage cirrhosis: part, I., gross morphology and diffuse, abnormali-ties. AJR, Am J Roentgenol 1999;173:1031–6.
19] Asbach P, Klatt D, Schlosser B, et al. Viscoelasticity-based staging of hepaticfibrosis with multifrequency MR elastography. Radiology 2010;257:80–6.
20] Kanematsu M, Goshima S, Watanabe H, et al. Diffusion/perfusion MR imag-ing of the liver: practice, challenges, and future. Magn Reson Med Sci2012;11:151–61.
21] Bakan AA, Inci E, Bakan S, et al. Utility of diffusion-weighted imaging in the
evaluation of liver fibrosis. Eur Radiol 2012;22:682–7.22] Koskinen SK, Niemi PT, Kajander SA, et al. T1rho Dispersion profile of rat tissuesin vitro at very low locking fields. Magn Reson Imaging 2006;24:295–9.
23] Haase A, Matthaei D, Bartkowski R, et al. Inversion recovery snapshot FLASHMR imaging. J Comput Assist Tomogr 1989;13:1036–40.