
Clinical Evidence, Practice Guidelines, and β-Blocker...
12
558 F or over 3 decades, cardiac complications have been responsible for significant morbidity and mortality after noncardiac surgery. 1–3 Largely on the basis of 2 randomized, controlled trials (RCT) published in the 1990s, 4,5 perioperative β-blockade was quickly embraced by proponents of patient safety as a simple intervention to help prevent these impor- tant complications. 6–9 Practice guidelines were also influ- enced such that, in 2002, the American College of Cardiology (ACC) and American Heart Association (AHA) recommended prophylactic β-blockade for many intermediate- to high-risk surgical patients. 10 However, subsequent clinical evidence cast doubts on the appropriateness of these recommendations. Earlier findings of reduced cardiac complications with β-blockade were not con- firmed in 3 subsequent RCTs published in 2005 and 2006. 11–13 In addition, Lindenauer et al 14 published a large cohort study in 2005 that showed perioperative β-blockade to be associated with reduced mortality among individuals with 2 or more clinical risk factors for postoperative cardiac events, but with increased mortality among patients with 1 or fewer risk factors. Based on these newer data, the 2006 ACC/AHA guidelines recommended a somewhat more selective use of perioperative β-blockade. 15 Received February 7, 2012; accepted May 18, 2012. From the Keenan Research Centre of the Li Ka Shing Knowledge Institute, St. Michael’s Hospital, Toronto, Ontario, Canada (D.N.W., M.M., A.L.); the Department of Anesthesia, Toronto General Hospital and University of Toronto, Toronto, Ontario, Canada (D.N.W., W.S.B.); Institute for Clinical Evaluative Sciences, Toronto, Ontario, Canada (D.N.W., M.M., A.L.); Institute of Health Policy Management and Evaluation, University of Toronto, Toronto, Ontario, Canada (D.N.W., M.M., A.L., S.R.J.); Leslie Dan Faculty of Pharmacy, University of Toronto, Toronto, Ontario, Canada (M.M.); College of Medicine, King Saud University, Riyadh, Saudi Arabia (M.M.); the Department of Medicine, St. Michael’s Hospital and University of Toronto, Toronto, Ontario, Canada (A.L.); the Department of Anesthesiology and Critical Care, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA (L.A.F., M.D.N.); the Division of Rheumatology, Department of Medicine; Toronto Western Hospital, Mount Sinai Hospital, and University of Toronto; Toronto, Ontario, Canada (S.R.J.); Leonard Davis Institute for Health Economics, University of Pennsylvania, Philadelphia, PA (L.A.F., J.K., M.D.N.); and Wharton School, University of Pennsylvania, Philadelphia, PA (J.K.). These results were presented in part as an oral presentation at the 2011 Scientific Sessions of the American Heart Association in Orlando, FL (November 16, 2011). The online-only Data Supplement is available with this article at http://circoutcomes.ahajournals.org/lookup/suppl/doi:10.1161/CIRCOUTCOMES.112.965632/-/DC1. Correspondence to Duminda N. Wijeysundera, MD, PhD, FRCPC, Li Ka Shing Knowledge Institute, St. Michael’s Hospital, 30 Bond St, Toronto, Ontario, Canada M5B 1W8. E-mail [email protected] Clinical Evidence, Practice Guidelines, and β-Blocker Utilization Before Major Noncardiac Surgery Duminda N. Wijeysundera, MD, PhD; Muhammad Mamdani, PharmD, MA, MPH; Andreas Laupacis, MD, MSc; Lee A. Fleisher, MD; W. Scott Beattie, MD, PhD; Sindhu R. Johnson, MD; Jonathan Kolstad, PhD; Mark D. Neuman, MD, MSc Background—Largely on the basis of 2 randomized trials published in the 1990s, β-blockers were initially promoted as an evidence-based intervention for preventing cardiac complications of noncardiac surgery. However, subsequent studies raised concerns about a widespread use of perioperative β-blockade. Little is known regarding how this changing evidence influenced the use of perioperative β-blockers in clinical practice. Methods and Results—We conducted a population-based, time-series analysis (April 1999 to March 2010) among residents of Ontario, Canada (age 66 years and older), to evaluate the influence of research publications and practice guidelines on rates of new β-blocker prescriptions before major elective noncardiac surgery. In an analysis of 249 828 procedures, the rate of new β-blocker prescriptions increased from 26.3 per 1000 procedures in April 1999 to 62.7 per 1000 procedures in the first quarter of 2005, after which it decreased to 19.7 per 1000 procedures by March 2010. We observed a marked decrease in prescriptions (P=0.004) during early 2005, without any preceding publications that raised concerns about perioperative β-blockade. There was no change (P=0.98) in prescription rates after the May 2008 publication of a multicenter, randomized trial that showed increased mortality from perioperative β-blockade. Prescribing trends remain unchanged after revisions of related practice guidelines in 2002 (P=0.28) and 2006 (P=0.53). Conclusions—After a period characterized by increasing adoption of preoperative β-blockade between 1999 and 2005, prescriptions rates subsequently fell from 2005 to 2010. Further research is needed to understand the basis for these changes, which are only partially explained by evidence of potential harm. (Circ Cardiovasc Qual Outcomes. 2012; 5:558-565.) Key Words: surgery ◼ β-blockers ◼ coronary artery disease ◼ health services research © 2012 American Heart Association, Inc. Circ Cardiovasc Qual Outcomes is available at http://circoutcomes.ahajournals.org DOI: 10.1161/CIRCOUTCOMES.112.965632 by guest on October 20, 2017 http://circoutcomes.ahajournals.org/ Downloaded from by guest on October 20, 2017 http://circoutcomes.ahajournals.org/ Downloaded from by guest on October 20, 2017 http://circoutcomes.ahajournals.org/ Downloaded from by guest on October 20, 2017 http://circoutcomes.ahajournals.org/ Downloaded from by guest on October 20, 2017 http://circoutcomes.ahajournals.org/ Downloaded from
Transcript of Clinical Evidence, Practice Guidelines, and β-Blocker...

558
For over 3 decades, cardiac complications have been responsible for significant morbidity and mortality after
noncardiac surgery.1–3 Largely on the basis of 2 randomized, controlled trials (RCT) published in the 1990s,4,5 perioperative β-blockade was quickly embraced by proponents of patient safety as a simple intervention to help prevent these impor-tant complications.6–9 Practice guidelines were also influ-enced such that, in 2002, the American College of Cardiology (ACC) and American Heart Association (AHA) recommended prophylactic β-blockade for many intermediate- to high-risk surgical patients.10
However, subsequent clinical evidence cast doubts on the appropriateness of these recommendations. Earlier findings of reduced cardiac complications with β-blockade were not con-firmed in 3 subsequent RCTs published in 2005 and 2006.11–13 In addition, Lindenauer et al14 published a large cohort study in 2005 that showed perioperative β-blockade to be associated with reduced mortality among individuals with 2 or more clinical risk factors for postoperative cardiac events, but with increased mortality among patients with 1 or fewer risk factors. Based on these newer data, the 2006 ACC/AHA guidelines recommended a somewhat more selective use of perioperative β-blockade.15
Received February 7, 2012; accepted May 18, 2012. From the Keenan Research Centre of the Li Ka Shing Knowledge Institute, St. Michael’s Hospital, Toronto, Ontario, Canada (D.N.W., M.M., A.L.);
the Department of Anesthesia, Toronto General Hospital and University of Toronto, Toronto, Ontario, Canada (D.N.W., W.S.B.); Institute for Clinical Evaluative Sciences, Toronto, Ontario, Canada (D.N.W., M.M., A.L.); Institute of Health Policy Management and Evaluation, University of Toronto, Toronto, Ontario, Canada (D.N.W., M.M., A.L., S.R.J.); Leslie Dan Faculty of Pharmacy, University of Toronto, Toronto, Ontario, Canada (M.M.); College of Medicine, King Saud University, Riyadh, Saudi Arabia (M.M.); the Department of Medicine, St. Michael’s Hospital and University of Toronto, Toronto, Ontario, Canada (A.L.); the Department of Anesthesiology and Critical Care, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA (L.A.F., M.D.N.); the Division of Rheumatology, Department of Medicine; Toronto Western Hospital, Mount Sinai Hospital, and University of Toronto; Toronto, Ontario, Canada (S.R.J.); Leonard Davis Institute for Health Economics, University of Pennsylvania, Philadelphia, PA (L.A.F., J.K., M.D.N.); and Wharton School, University of Pennsylvania, Philadelphia, PA (J.K.).
These results were presented in part as an oral presentation at the 2011 Scientific Sessions of the American Heart Association in Orlando, FL (November 16, 2011).
The online-only Data Supplement is available with this article at http://circoutcomes.ahajournals.org/lookup/suppl/doi:10.1161/CIRCOUTCOMES.112.965632/-/DC1.Correspondence to Duminda N. Wijeysundera, MD, PhD, FRCPC, Li Ka Shing Knowledge Institute, St. Michael’s Hospital, 30 Bond St, Toronto,
Ontario, Canada M5B 1W8. E-mail [email protected]
10.1161/CIRCOUTCOMES.112.965632
2012
July
Wijeysundera et al
Trends in Perioperative β-Blockade
Clinical Evidence, Practice Guidelines, and β-Blocker Utilization Before Major Noncardiac Surgery
Duminda N. Wijeysundera, MD, PhD; Muhammad Mamdani, PharmD, MA, MPH; Andreas Laupacis, MD, MSc; Lee A. Fleisher, MD; W. Scott Beattie, MD, PhD; Sindhu R. Johnson, MD; Jonathan Kolstad, PhD; Mark D. Neuman, MD, MSc
Background—Largely on the basis of 2 randomized trials published in the 1990s, β-blockers were initially promoted as an evidence-based intervention for preventing cardiac complications of noncardiac surgery. However, subsequent studies raised concerns about a widespread use of perioperative β-blockade. Little is known regarding how this changing evidence influenced the use of perioperative β-blockers in clinical practice.
Methods and Results—We conducted a population-based, time-series analysis (April 1999 to March 2010) among residents of Ontario, Canada (age 66 years and older), to evaluate the influence of research publications and practice guidelines on rates of new β-blocker prescriptions before major elective noncardiac surgery. In an analysis of 249 828 procedures, the rate of new β-blocker prescriptions increased from 26.3 per 1000 procedures in April 1999 to 62.7 per 1000 procedures in the first quarter of 2005, after which it decreased to 19.7 per 1000 procedures by March 2010. We observed a marked decrease in prescriptions (P=0.004) during early 2005, without any preceding publications that raised concerns about perioperative β-blockade. There was no change (P=0.98) in prescription rates after the May 2008 publication of a multicenter, randomized trial that showed increased mortality from perioperative β-blockade. Prescribing trends remain unchanged after revisions of related practice guidelines in 2002 (P=0.28) and 2006 (P=0.53).
Conclusions—After a period characterized by increasing adoption of preoperative β-blockade between 1999 and 2005, prescriptions rates subsequently fell from 2005 to 2010. Further research is needed to understand the basis for these changes, which are only partially explained by evidence of potential harm. (Circ Cardiovasc Qual Outcomes. 2012; 5:558-565.)
Key Words: surgery ◼ β-blockers ◼ coronary artery disease ◼ health services research
7,8,100
© 2012 American Heart Association, Inc.
Circ Cardiovasc Qual Outcomes is available at http://circoutcomes.ahajournals.org DOI: 10.1161/CIRCOUTCOMES.112.965632
by guest on October 20, 2017
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on October 20, 2017
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on October 20, 2017
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on October 20, 2017
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on October 20, 2017
http://circoutcomes.ahajournals.org/
Dow
nloaded from

Wijeysundera et al Trends in Perioperative β-Blockade 559
Most recently, the publication of the results of Perioperative Ischemic Evaluation (POISE) trial in May 2008 raised more concerns about the safety of perioperative β-blockade.16 This multicenter RCT showed that individuals randomly assigned to receive β-blockers before surgery had a reduced risk of postoperative myocardial infarction but increased risk of significant hypotension, stroke, and death. The surprising results generated considerable debate (Nainggolan L. POISE published, debate on perioperative β-blockers continues. http://www.theheart.org/article/864785.do) and led to further changes in practice guidelines. Specifically, the 2009 ACC/AHA guidelines only made moderate to strong recommenda-tions for perioperative β-blockade in patients considered to be at highest risk for postoperative cardiac events.2
Despite such important changes in clinical evidence and guideline recommendations, relatively little is known about their influence on physicians’ prescribing of β-blockers before surgery. We therefore conducted a population-based, time-series study in Ontario, Canada, to assess trends in β-blocker use for noncardiac surgery and evaluate shifts in practice potentially attributable to changes in clinical evidence or guidelines recommendations.
MethodsA population-based, cross-sectional, time-series analysis was con-ducted in Ontario, Canada, using the following linked administrative databases: the Discharge Abstract Database of the Canadian Institute for Health Information (hospital admissions), the Ontario Health Insurance Plan database (physician service claims), the Registered Persons Database (demographics and vital statistics), and the Ontario Drug Benefit database (prescription medications for individuals aged older than 65 years). The approximately 13 million residents of Ontario have universal access to physician and hospital services through a publicly funded healthcare program. The research ethics board at Sunnybrook Health Sciences Centre approved this study.
We identified specific elective noncardiac surgeries performed between April 1, 1999, and March 31, 2010, on Ontario residents
who were aged 66 years or older: abdominal aortic aneurysm repair, carotid endarterectomy, peripheral vascular bypass, total hip replace-ment, total knee replacement, large bowel resection, partial liver re-section, Whipple procedure, pneumonectomy, pulmonary lobectomy, gastrectomy, esophagectomy, nephrectomy, and cystectomy. These procedures are intermediate to high risk2 and are previously described in the Discharge Abstract Database.17,18 Procedural information in the Discharge Abstract Database is very accurate.19 An age restriction of 66 years was imposed because data on outpatient medication pre-scriptions were only available for individuals aged 65 years or older, and a 1-year look-back period was used to ascertain preoperative medication use.
Patients were categorized on the basis of their perioperative cardiac risk. We estimated their risk using the Revised Cardiac Risk Index (RCRI),20 which consists of 6 equally weighted components: coro-nary artery disease, congestive heart failure, cerebrovascular disease, diabetes, renal insufficiency, and high-risk surgery (major vascular, intraperitoneal, or intrathoracic procedures). As previously proposed, low-risk was defined as a RCRI score of zero, intermediate-risk as a score of 1 to 2, and high-risk as a score of 3 or more.21 Using the Discharge Abstract Database, we identified the presence of coronary artery disease, congestive heart failure, cerebrovascular disease, and renal insufficiency based on International Classification of Diseases codes (9th or 10th Revisions) from hospitalizations within 3 years be-fore surgery.22 Additionally, validated algorithms were used to ascer-tain diabetes,23 and the Ontario Health Insurance Plan database was used to identify patients who required dialysis before surgery. We also used the Discharge Abstract Database and Registered Persons Database to identify any postoperative 30-day deaths.
The Ontario Drug Benefit database was used to identify outpatient prescriptions for orally administered β-blockers (except sotalol) be-fore each surgical procedure. We excluded sotalol because it is typi-cally used to suppress cardiac arrhythmias, as opposed to preventing cardiac ischemia. Prescription information in Ontario Drug Benefit database is very accurate.24 Practice guidelines recommend that perioperative β-blockade be initiated several days to weeks before surgery,2,10,15 with further suggestions to initiate therapy 7 or more days before surgery.25 Notably, many surgical patients in Ontario who warrant perioperative β-blockade may be able to initiate therapy well before their surgeries. Specifically, once they have been deemed to require surgery, the time required for 90% to undergo their scheduled procedures is 58 days for cancer surgery, 104 days for vascular sur-gery, and 192 days for orthopedic surgery (Ontario Ministry of Health and Long-Term Care. Ontario Wait Times: Wait Time for Surgery, MRIs and CTs. Available at http://waittimes.hco-on.ca/en/search/sur-gery/adult). In addition, 91% of preoperative medical consultations, which are the physician encounters where preoperative β-blocker therapy is most likely to be initiated, occur within 60 days before surgery, as compared with 84% within 30 days before surgery.26
For the purpose of the primary analysis, we therefore defined new preoperative β-blocker use as initiation of therapy within 60 days be-fore surgery. Specifically, new preoperative β-blocker prescriptions were identified on the basis of (1) 1 or more prescriptions within 60 days before hospital admission and (2) no prescriptions between 61 and 365 days before admission. To evaluate whether trends in new preoperative β-blocker use were distinct from trends in patients’ other cardiovascular medications, we used the same database to identify statin and nonperioperative β-blocker prescriptions. Statin use was defined based on the presence of 1 or more statin prescriptions within 100 days before hospital admission. These prescriptions were classi-fied as new preoperative use based on the same algorithm described for new β-blocker prescriptions. Otherwise, the prescriptions were classified as nonperioperative use. Nonperioperative β-blocker use was defined based on the presence of either (1) 1 or more prescrip-tions between 61 to 100 days before hospital admission or (2) 1 or more prescriptions within 60 days before hospital admission, in con-junction with 1 or more prescriptions between 61 to 365 days before admission.
In sensitivity analyses, we used 2 alternative definitions of new β-blocker use, namely, (1) 1 or more prescriptions within 30 days before hospital admission or (2) 1 or more prescriptions within 7 days
WHAT IS KNOWN
•Largely on the basis of 2 randomized trials published in the 1990s, β-blockers were initially promoted for preventing cardiac complications of noncardiac surgery.
•Subsequent research cast doubts on both the efficacy and safety of perioperative β-blockade.
WHAT THE STUDY ADDS
•The mean rate of new β-blocker prescriptions be-fore major elective noncardiac surgery in Ontario, Canada, between 1999 and 2010 was low, at 40.3 per 1000 procedures.
•The rate of new β-blocker prescriptions initially rose from 1999 to early 2005, after which it declined from 2005 to 2010.
•These changing prescribing trends were consistent across patients over varying perioperative cardiac risk but were not explained by the publication of new clinical evidence or revised practice guidelines.
by guest on October 20, 2017
http://circoutcomes.ahajournals.org/
Dow
nloaded from

560 Circ Cardiovasc Qual Outcomes July 2012
before hospital admission, in individuals who had not previously re-ceived any β-blockers within the year before surgery.
AnalysisEach year of the study period was divided into 3-month inter-vals (January to March, April to June, July to September, October to December). Surgeries were assigned to these intervals based on the date of hospital admission. We measured rates of preoperative β-blocker use, preoperative statin use, and 30-day mortality within each interval. Rates of new β-blocker use were calculated among in-dividuals who were not previously using β-blockers, whereas rates of new statin use were calculated among individuals who were not pre-viously using statins. Conversely, rates of nonperioperative β-blocker and statin use were calculated among all patients. These rates were also calculated for subgroups based on RCRI score (low risk: zero points; intermediate-to-high risk: 1 or more points) and surgical pro-cedure (vascular surgery; nonvascular surgery). The sample size was not large enough for a subgroup analysis of only high-risk patients with RCRI scores of 3 or more.
Patterns of preoperative β-blocker and statin use over the study pe-riod were examined using time-series analysis, which is a collection of techniques for modeling autocorrelation in temporally sequenced data.27 In the primary analysis, trends in rates of new β-blocker use, nonperioperative β-blocker use, new statin use, nonperioperative statin use, and 30-day mortality were separately examined. In second-ary analyses, we examined trends in rates of new β-blocker use within strata defined by RCRI score and surgical procedure.
The association of selected publications with rates of new preopera-tive β-blocker use was assessed through interventional autoregressive integrated moving average (ARIMA) models with ramp functions. Ramp functions describe points in time when the trend in data gradually changes slope.28 The publications and guidelines that we considered a priori to have potentially influenced rates of new β-blocker prescriptions are described in the Table.5,10–12,14–16,29 We evaluated the appropriateness of the model assumptions by performing the augmented Dickey-Fuller test,30 calculating the Ljung-Box statistic at various lags,31 and assessing the autocorrelation, partial autocorrelation, and inverse autocorrelation functions. In sensitivity analyses, we reevaluated the impact of these same publications by using a different statistical approach, namely, with segmented regression models within a “difference-in-differences” framework.32 These linear regression models tested for changes in the slope of a linear trend before and after a specific point in time.
All statistical analyses were performed using SAS Version 9.2 (Cary, NC). A 2-sided probability value <0.05 was used to define sta-tistical significance.
ResultsThe analysis included 249 828 procedures that were performed between April 1, 1999, and March 31, 2010. Of these pro-cedures, 191 481 involved individuals who were not previ-ously using β-blockers (characteristics presented in Online Data Supplement Table I). The overall rate of new preopera-tive β-blocker prescriptions during the study period was low (40.3 per 1000 procedures). The rate rose from 26.3 per 1000 procedures in April 1999 and peaked during the first quarter of 2005 (62.7 per 1000 procedures), after which it declined to 19.7 per 1000 procedures by March 2010 (Figure 1). Although rates of new β-blocker prescriptions were generally higher in intermediate- to high-risk patients as opposed to low-risk patients (Figure 2), similar temporal changes occurred in both subgroups. However, these patterns were specific to new β-blocker prescriptions. By comparison, rates of periop-erative and nonperioperative statin prescriptions rose consis-tently over the study period (Figures 1 and 3), whereas rates of nonperioperative β-blocker prescriptions initially rose and reached a plateau by mid-2002 (Figure 3).
Qualitative inspection of trends in new preoperative β-blocker use (Figure 1) suggested a directional change in this trend during the first quarter of 2005, which was confirmed sta-tistically (P<0.001). This directional change was also evident in subgroups of low-risk (P=0.006) and intermediate- to high-risk (P=0.005) patients (Figure 2). Conversely, qualitative inspection of prescription trends did not suggest any changes in prescribing patterns after the publication of the POISE trial in May 2008 (Figure 1 and 2), which was confirmed statisti-cally for all patients (P=0.98), low-risk patients (P=0.95), and intermediate- to high-risk patients (P=0.89). Similarly, there was no evidence of a change in prescribing trends after the earlier presentation of these results at a major international scientific meeting (November 2007). Finally, there was no graphical or statistical evidence of a shift in prescribing trends after the publication of revised ACC/AHA practice guidelines in 2002 (P=0.28) and 2006 (P=0.53). These findings were also similar in the subgroups of low-risk and intermediate- to high-risk patients.
The study findings were qualitatively similar when the time-series analyses were repeated, using different defini-tions for new β-blocker use (Figure 4), subgroups of vascular surgical procedures (Online Data Supplement Figure I), or segmented linear regression methods. In addition, there was no qualitative evidence of changes in 30-day mortality that coincided with shifts in rates of new β-blocker prescriptions (Figure 5).
DiscussionRates of new β-blocker prescriptions before major elective noncardiac surgery in Ontario were relatively low and under-went marked changes between 1999 and 2010. In association with an early positive clinical trial,5 the use of preoperative β-blockers increased rapidly between 1999 and early 2005, after which it began to decline. This decline was not further influenced by either the publication of the POISE trial, a large RCT that demonstrated harm from perioperative β-blockade,16 or revisions of AHA/ACC practice guidelines that advised changes in β-blocker use.10,15
Past examinations of the diffusion of new research findings into clinical practice have typically emphasized delays in cli-nicians’ uptake of guideline recommendations and evidence-based practices.33–36 Conversely, some recent work has also described the potential for innovations with high degrees of intuitive appeal to diffuse rapidly into clinical practice, even if definitive proof of efficacy is lacking.37,38 In this present study, we observed a rapid adoption of preoperative β-blocker treat-ment after initial reports that suggested clinical efficacy.4,5 Notably, this trend in clinicians’ behavior occurred before similar recommendations by perioperative practice guide-lines.10 The increased initiation of β-blocker use from 1999 to early 2005 was specific to the perioperative setting; by comparison, nonperioperative β-blocker use among surgical patients plateaued in mid-2002. These differing prescribing patterns may be explained, in part, by 1999 Canadian prac-tice guidelines recommending against β-blockers as first-line treatment for hypertension in individuals aged 60 years or older.39 Previous research has shown that in the nonopera-tive setting, these recommendations led to subsequent general
by guest on October 20, 2017
http://circoutcomes.ahajournals.org/
Dow
nloaded from

Wijeysundera et al Trends in Perioperative β-Blockade 561
decline in new β-blocker prescriptions among Ontario resi-dents aged 65 years or older.40
We also observed a previously undescribed shift from increasing to decreasing rates of new preoperative β-blocker prescriptions during early 2005. This shift was again spe-cific to new β-blocker prescriptions. Newly published clini-cal evidence in peer-reviewed journals was unlikely to be the
major basis for this shift, especially since it occurred before the publication of any studies that raised doubts about the efficacy of perioperative β-blockade, such as the POBBLE trial (April 2005),11 DiPOM trial (June 2006),12 MAVS trial (November 2006),13 and the cohort study by Lindenauer et al14 (July 2005). It is also unlikely that this shift was caused by general changes in prescribing patterns for β-blockers in
Table. Selected Publications That May Have Influenced Rates of New Prescriptions for β-Blockers Before Noncardiac Surgery
Research Publications
Publication Type Publication Date Results
DECREASE 1 trial16
RCT December 1999 In 112 vascular surgery patients, bisoprolol significantly decreased (RR, 0.09; 95% CI, 0.02–0.37) 30-d cardiac death or nonfatal myocardial infarction.
POBBLE trial11 RCT April 2005 In 103 vascular surgery patients, metoprolol did not cause any significant difference (RR, 0.94; 95% CI, 0.53–1.66) in 30-d myocardial infarction, unstable angina, ventricular tachycardia, or stroke.
Lindenauer et al14
Cohort study
July 2005 (poster presentation at Society of General Internal Medicine
meeting in May 2003)
In 663 635 patients, the association of β-blockers with in-hospital mortality varied, based on perioperative cardiac risk, as estimated by the Revised Cardiac Risk Index (RCRI). In patients with RCRI scores of zero or 1, β-blockers were associated with increased mortality. β-Blockers were associated with decreased mortality in patients with RCRI scores of 2 and higher.
DIPOM trial12 RCT June 2006 (oral presentation at AHA Scientific Sessions in November
2004)
In 921 diabetic patients, metoprolol did not cause any significant difference (HR, 1.06; 95% CI, 0.80–1.41) in time to all-cause mortality, myocardial infarction, unstable angina, or congestive heart failure.
MaVS trial13 RCT November 2006 (oral presentation at Canadian Anesthesiologists’ Society
Meeting in June 2004)
In 496 vascular surgery patients, metoprolol did not cause any significant difference (RR, 0.85; 95% CI, 0.62–1.48) in 30-d nonfatal myocardial infarction, unstable angina, congestive heart failure, atrial or ventricular dysrhythmia, or cardiac death.
POISE trial16 RCT May 2008 (abstract presentation at AHA Scientific Sessions in November
2007)
In 8531 patients, metoprolol significant decreased (HR, 0.84; 95% CI, 0.70–0.99) 30-d cardiac death, nonfatal myocardial infarction or nonfatal cardiac arrest. However, it also led to significantly higher 30-d mortality (HR, 1.33; CI, 1.03–1.74).
Practice Guideline Publication Date Recommendations (Class I Level* or Class IIa Level†)
ACC/AHA 199629 Guideline March 1996 β-Blockers recommended for patients who had required β-blockers in recent past for controlling hypertension, symptomatic arrhythmias, or symptoms of angina (class I level).
ACC/AHA 200210 Guideline March 2002 β-Blockers recommended for:
(1) Vascular surgery patients with inducible ischemia on preoperative testing (class I level).
(2) Any patient with untreated hypertension, known coronary artery disease, or any risk factors for coronary artery disease (class IIa level).
ACC/AHA 200615 Guideline June 2006 β-Blockers recommended for:
(1) Vascular surgery patients with inducible ischemia on preoperative testing (class I level).
(2) Vascular surgery patients with known coronary artery disease (class IIa level).
(3) Vascular surgery patients with multiple risk factors for coronary artery disease (class IIa level)
(4) Patients who are undergoing intermediate- to high-risk procedures and have known coronary artery disease or multiple risk factors for coronary artery disease (class IIa level).
ACC/AHA 20092 Guideline November 2009 β-Blockers recommended for:
(1) Vascular surgery patients with inducible ischemia on preoperative testing (class IIa)
(2) Vascular surgery patients with known coronary artery disease (class IIa)
RCT indicates randomized, controlled trial; RR, relative risk; CI, confidence interval; HR, hazard ratio; ACC, American College of Cardiology; and AHA, American Heart Association.
*Class I recommendation indicates that there is evidence for and/or general agreement that the procedure or treatment is beneficial, useful, and effective.†Class IIa recommendation indicates that there is conflicting evidence and/or a divergence of opinion about the usefulness/efficacy of a procedure or treatment but
that the weight of evidence/opinion is in favor of its usefulness/efficacy.
by guest on October 20, 2017
http://circoutcomes.ahajournals.org/
Dow
nloaded from

562 Circ Cardiovasc Qual Outcomes July 2012
the nonoperative setting. Specifically, rates of new prescrip-tions for β-blockers in the nonoperative setting began to decline in 1999.40 Nonetheless, it is possible that the pre-sentation of some perioperative β-blocker studies at medi-cal conferences could have been partially responsible for the shift in prescribing patterns during early 2005. Specifically, the results of the MAVS trial (June 2004) and DIPOM trial (November 2004) were presented at scientific meetings within the 6-month period preceding the shift. Perioperative physi-cians may have learnt about the findings presented at these conferences before their publication in print journals, either by attending the relevant conferences themselves, discussing with colleagues who attended these conferences, or reading
web-based coverage of newly presented research at medi-cal conferences. The relative contributions of these different mechanisms remain unclear and merit further research.
Although the shift from increasing to decreasing β-blocker use in early 2005 may have been partially attributable to the availability of new clinical evidence (albeit not in the print literature), it is unlikely that changes in clinical evidence were the only reason for this marked shift in prescribing practice. Another potential explanation, which requires evaluation by future research, is clinicians’ own observations of adverse events after preoperative β-blockade (eg, significant hypoten-sion). Especially since perioperative β-blockers are associ-ated with relatively common short-term adverse effects that
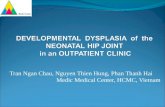
Figure 1. Trends in new outpatient prescriptions for b-blockers and statins within 60 days before major elective noncardiac surgery in Ontario. Rates of new β-blocker (solid line) and statin (dotted line) prescriptions before elective noncardiac surgery in Ontario, Canada. These rates (per 1000 procedures) are reported for 3-month periods from April 1, 1999, to March 31, 2010. Vertical lines represent the timing of publications that may have influenced rates of perioperative β-blockade (Table). Time-series analyses found significant statistical evidence of a shift in trends in the first quarter of 2005 (P<0.001). Conversely, there was no significant evidence (P=0.98) of a shift in the second quarter of 2008, during which the POISE trial was published. AHA indicates American Heart Association.
Figure 2. Trends in new outpatient prescriptions for β-blockers within 60 days before major elective noncardiac surgery in Ontario, stratified by the Revised Cardiac Risk Index (RCRI) score. Rates of new β-blocker prescriptions before elective noncardiac surgery in Ontario, Canada. Dotted line represents trends for low-risk individuals (RCRI: zero points); solid line represents trends for intermediate- to high-risk individuals (RCRI: 1 or more points). These rates (per 1000 procedures) are reported for 3-month periods from April 1, 1999, to March 31, 2010. Vertical lines represent the timing of publications that may have influenced rates of perioperative β-blockade (Table). Time-series analyses found significant statistical evidence of a shift in trend in the first quarter of 2005 for both low-risk (P=0.006) and intermediate- to high-risk (P=0.005) patients. Conversely, there was no significant evidence of a shift in the second quarter of 2008, during which the POISE trial was published, for either low-risk (P=0.95) or intermediate- to high-risk (P=0.89) patients. AHA indicates American Heart Association.
by guest on October 20, 2017
http://circoutcomes.ahajournals.org/
Dow
nloaded from

Wijeysundera et al Trends in Perioperative β-Blockade 563
could be readily attributed to the new medication,16,41 the initial rising rates of perioperative β-blockade from 1999 to 2005 might have led to an increasing recognition of related adverse effects and subsequently dampened enthusiasm for these medications.
By comparison to the significant shift in prescribing trends in early 2005, we found no strong evidence of changes in pre-scribing practice after the release of the results of the POISE trial, either as a conference presentation (November 2007) or print publication (May 2008). There are several poten-tial explanations for this observation. Given the preceding decline in β-blocker use, the POISE trial results may have only confirmed and supported ongoing trends in practice. In addition, controversy surrounding the interpretation of POISE trial, some of which related to its use of high fixed doses of β-blockers, may have lessened the clinical impact of the study findings. Finally, the results of the POISE trial may have most strongly influenced in-hospital initiation of β-blockers imme-diately before surgery, yet our data sources did not capture in-hospital medication use.
Although we identified important directional shifts in pre-scribing trends, these shifts occurred within the context of a low overall prescription rate for β-blockers, which ranged from 19.7 to 62.7 per 1000 procedures over the study period. This low prescription rate in our population-based study
is consistent with other Ontario data sources. Specifically, Ellenberger et al42 reported that the rate of new preoperative β-blocker prescriptions at 2 tertiary care Ontario hospitals was 58.2 per 1000 procedures; notably, these data included both in-hospital and outpatient prescriptions. This low prescription rate suggests that despite strong encouragement by proponents of patient safety,6–9 most clinicians remained reluctant to incor-porate perioperative β-blockade into their clinical practice.
Our study also highlights the importance of research that seeks to describe and understand physicians’ adoption and abandonment of new medical therapies, especially within the context of rapid changes in the biomedical literature. The case of perioperative β-blockade serves as a model for understand-ing how clinical care might be altered when the results of early positive clinical trials are initially promoted enthusiastically but subsequently refuted by larger studies. Future research should therefore examine how clinical practice was altered in other settings associated with similar swings in evidence, such as intensive glucose control in the critically ill.43,44
Our study has limitations. First, our data sources lacked information on β-blocker use occurring in-hospital or among individuals younger than 65 years. Thus, we could not cap-ture de novo administration of β-blockers immediately before surgery, as might be performed by some anesthesiolo-gists. Nonetheless, the absence of information on in-hospital
Figure 3. Trends in preoperative on-going use of β-blockers and statins before major elective noncardiac surgery in Ontario. Rates of nonperioperative β-blocker (solid line) and statin (dotted line) prescriptions before elective non- cardiac surgery in Ontario, Canada. These rates (per 1000 procedures) are reported for 3-month periods from April 1, 1999, to March 31, 2010. Vertical lines represent the timing of publications that may have influenced rates of new perioperative β-blocker use (Table). AHA indicates American Heart Association.
Figure 4. Trends in outpatient prescrip-tions for β-blockers that were new pre-scribed within 30 days or 7 days before major elective noncardiac surgery in Ontario. Rates of β-blockers that were newly prescribed within either 30 days (solid line) or 7 days (dotted line) before elective noncardiac surgery in Ontario, Canada. These rates (per 1000 proce-dures) are reported for 3-month periods from April 1, 1999, to March 31, 2010. Vertical lines represent the timing of publications that may have influenced rates of perioperative β-blockade (Table). AHA indicates American Heart Association.
by guest on October 20, 2017
http://circoutcomes.ahajournals.org/
Dow
nloaded from

564 Circ Cardiovasc Qual Outcomes July 2012
medication use is unlikely to explain the shift to a decreas-ing rate of outpatient β-blocker prescriptions in early 2005. However, it could have masked some of the impact from the results of the POISE trial and might have had a greater impact on in-hospital use of β-blockers. Second, the study population was not large enough to examine specific sub-groups, such as high-risk patients with an RCRI score of 3 or more. It is conceivable that trends in β-blocker prescriptions may differ in these smaller subgroups.
Third, the 60-day window used to identify new preopera-tive β-blocker prescriptions in the primary analysis may be considered excessively long in jurisdictions with shorter wait-ing times for surgery. However, as described previously, this window is appropriate for the setting of the present study. In addition, our overall findings remained consistent in sensitiv-ity analyses that used shorter time-windows for ascertaining new preoperative β-blocker use. Fourth, our results represent clinical practice within Ontario, a region where individuals aged 65 years or older have access to publicly funded pre-scription drug coverage and where several scientists leading the POISE trial are located. Thus, the generalizability of our results to other settings warrants further study.
ConclusionsIn this population-based, time-series analysis, we found that rates of new β-blocker prescriptions before major elective noncardiac surgery in Ontario, while relatively low overall, underwent marked changes between 1999 and 2010. There was statistical and qualitative evidence of a significant shift toward decreasing β-blocker use in early 2005 but no clear change in prescription rates that could be attributable to the publica-tion of a large, randomized trial showing evidence of harm or to 2 prominent clinical practice guidelines published over the period. These findings highlight the importance of research that seeks to understand the processes underlying physicians’ adoption and abandonment of new medical therapies, as well as the potential benefits and harms of the ways in which infor-mation gained from randomized trials, observational studies, and practice guidelines inform medical decision-making.
Sources of FundingDrs Wijeysundera and Johnson are supported by Clinician-Scientist Awards from the Canadian Institutes of Health Research. Drs
Wijeysundera and Beattie are supported by Merit Awards from the Department of Anesthesia at the University of Toronto. Dr Beattie is the R. Fraser Elliot Chair of Cardiac Anesthesia at the University Health Network. This study was supported in part by the Institute for Clinical Evaluative Sciences, which is itself supported in part by the Ontario Ministry of Health and Long-Term Care. The study spon-sor had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; and prepara-tion, review, or approval of the manuscript. The opinions, results, and conclusions are those of the authors, and no endorsement by the Ontario Ministry of Health and Long-Term Care or the Institute for Clinical Evaluative Sciences is intended or should be inferred. The corresponding author (Dr Wijeysundera) had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
DisclosuresNone.
References 1. Djokovic JL, Hedley-Whyte J. Prediction of outcome of surgery and an-
esthesia in patients over 80. JAMA. 1979;242:2301–2306. 2. Fleisher LA, Beckman JA, Brown KA, Calkins H, Chaikof EL,
Fleischmann KE, Freeman WK, Froehlich JB, Kasper EK, Kersten JR, Riegel B, Robb JF. 2009 ACCF/AHA Focused Update on Perioperative Beta Blockade incorporated into the ACC/AHA 2007 Guidelines on Peri-operative Cardiovascular Evaluation and Care for Noncardiac Surgery: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2009;120:e169–e276.
3. Goldman L, Caldera DL, Nussbaum SR, Southwick FS, Krogstad D, Murray B, Burke DS, O’Malley TA, Goroll AH, Caplan CH, Nolan J, Carabello B, Slater EE. Multifactorial index of cardiac risk in noncardiac surgical procedures. N Engl J Med. 1977;297:845–850.
4. Mangano DT, Layug EL, Wallace A, Tateo I. Effect of atenolol on mor-tality and cardiovascular morbidity after noncardiac surgery. N Engl J Med. 1996;335:1713–1720.
5. P Poldermans D, Boersma E, Bax JJ, Thomson IR, van de Ven LL, Blankensteijn JD, Baars HF, Yo TI, Trocino G, Vigna C, Roelandt JR, van Urk H. The effect of bisoprolol on perioperative mortality and myocardial infarction in high-risk patients undergoing vascular surgery. N Engl J Med. 1999;341:1789–1794.
6. Birkmeyer JD, Dimick JB. The Leapfrog Group’s Patient Safety Prac-tices, 2003: The Potential Benefits of Universal Adoption. Washington, DC: Leapfrog Group; 2004.
7. Leape LL, Berwick DM, Bates DW. What practices will most im-prove safety? Evidence-based medicine meets patient safety. JAMA. 2002;288:501–507.
8. National Quality Forum. Safe Practices for Better Healthcare: 2006 Update. Washington, DC: National Quality Forum; 2006.
9. Shojania KG, Duncan BW, McDonald KM, Wachter RM. Making Health Care Safer: A Critical Analysis of Patient Safety Practices.
Figure 5. Trends in postoperative 30-day mortality and new outpatient prescriptions for β-blockers within 60 days before major elective noncardiac surgery. Rates of new preoperative β-blocker prescriptions (dot-ted line) and postoperative 30-day deaths (solid line) for elective noncardiac surgery in Ontario, Canada. These rates (per 1000 procedures), which are reported for 3-month periods from April 1, 1999, to March 31, 2010, were calculated among individuals who had the potential to receive new preoperative β-blocker pre-scriptions (ie, those who were not previ-ously using β-blockers). Vertical lines represent the timing of publications that may have influenced rates of perioperative β-blockade. AHA indicates American Heart Association.
by guest on October 20, 2017
http://circoutcomes.ahajournals.org/
Dow
nloaded from

Wijeysundera et al Trends in Perioperative β-Blockade 565
Evidence Report/Technology Assessment. No. 43. (AHRQ Publication No. 01-E058). Rockville, MD: Agency for Healthcare Research and Qual-ity; 2001.
10. Eagle KA, Berger PB, Calkins H, Chaitman BR, Ewy GA, Fleischmann KE, Fleisher LA, Froehlich JB, Gusberg RJ, Leppo JA, Ryan T, Schlant RC, Winters WLJ, Gibbons RJ, Antman EM, Alpert JS, Faxon DP, Fuster V, Gregoratos G, Jacobs AK, Hiratzka LF, Russell RO, Smith SCJ. ACC/AHA guideline update for perioperative cardiovascular evaluation for noncardiac surgery: executive summary: a report of the American Col-lege of Cardiology/American Heart Association Task Force on Practice Guideline. Circulation. 2002;105:1257–1267.
11. POBBLE Trial Investigators. Perioperative beta-blockade (POBBLE) for patients undergoing infrarenal vascular surgery: results of a randomized double-blind controlled trial. J Vasc Surg. 2005;41:602–609.
12. Juul AB, Wetterslev J, Gluud C, Kofoed-Enevoldsen A, Jensen G, Cal-lesen T, Nørgaard P, Fruergaard K, Bestle M, Vedelsdal R, Miran A, Ja-cobsen J, Roed J, Mortensen M-B, Jørgensen L, Jørgensen J, Rovsing M-L, Petersen PL, Pott F, Haas M, Albret R, Nielsen LL, Johansson G, Stjernholm P, Mølgaard Y, Foss NB, Elkjaer J, Dehlie B, Boysen K, Zaric D, Munksgaard A, Madsen JB, Øberg B, Khanykin B, Blemmer T, Yn-dgaard S, Perko G, Wang LP, Winkel P, Hilden J, Jensen P, Salas N, and the DIPOM Group. Effect of perioperative beta blockade in patients with diabetes undergoing major non-cardiac surgery: randomised placebo controlled, blinded multicentre trial. BMJ. 2006;332:1482.
13. Yang H, Raymer K, Butler R, Parlow J, Roberts R. The effects of perioperative beta-blockade: results of the Metoprolol after Vascu-lar Surgery (MaVS) study, a randomized controlled trial. Am Heart J. 2006;152:983–990.
14. Lindenauer PK, Pekow P, Wang K, Mamidi DK, Gutierrez B, Benjamin EM. Perioperative beta-blocker therapy and mortality after major non-cardiac surgery. N Engl J Med. 2005;353:349–361.
15. Fleisher LA, Beckman JA, Brown KA, Calkins H, Chaikof E, Fleis-chmann KE, Freeman WK, Froehlich JB, Kasper EK, Kersten JR, Robb JF, Smith SC, Jacobs AK, Adams CD, Anderson JL, Antman EM, Faxon DP, Fuster V, Halperin JL, Hiratzka LF, Hunt SA, Lytle BW, Nishimura R, Page RL, Riegel B. ACC/AHA 2006 guideline update on periopera-tive cardiovascular evaluation for noncardiac surgery: focused update on perioperative beta-blocker therapy: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guide-lines. Circulation. 2006;113:2662–2674.
16. POISE Study Group. Effects of extended-release metoprolol succinate in patients undergoing non-cardiac surgery (POISE trial): a randomised controlled trial. Lancet. 2008;371:1839–1847.
17. Technical Supplement: Health Care in Canada 2005. Ottawa, ON, Canada: Canadian Institute for Health Information; 2005.
18. Bourne RB, DeBoer D, Hawker G, Kreder H, Mahomed N, Paterson JM, Warner S, Williams J. Chapter 5: Total Hip and Knee Replacement. In: Tu JV, Pinfold SP, McColgan P, Laupacis A, eds. Access to Health Ser-vice in Ontario: ICES Atlas. Toronto, ON, Canada: Institute for Clinical Evaluative Sciences; 2005;114–115.
19. Juurlink D, Preya C, Croxford R, Chong A, Austin P, Tu J, Laupacis A. Canadian Institute for Health Information Discharge Abstract Database: A Validation Study. ICES Investigative Report. Toronto, ON, Canada: Institute for Clinical Evaluative Sciences; 2006.
20. Lee TH, Marcantonio ER, Mangione CM, Thomas EJ, Polanczyk CA, Cook EF, Sugarbaker DJ, Donaldson MC, Poss R, Ho KK, Ludwig LE, Pedan A, Goldman L. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circula-tion. 1999;100:1043–1049.
21. Auerbach A, Goldman L. Assessing and reducing the cardiac risk of non-cardiac surgery. Circulation. 2006;113:1361–1376.
22. Quan H, Sundararajan V, Halfon P, Fong A, Burnand B, Luthi JC, Saunders LD, Beck CA, Feasby TE, Ghali WA. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care. 2005;43:1130–1139.
23. Hux JE, Ivis F, Flintoft V, Bica A. Diabetes in Ontario: determination of prevalence and incidence using a validated administrative data algorithm. Diabetes Care. 2002;25:512–516.
24. Levy AR, O’Brien BJ, Sellors C, Grootendorst P, Willison D. Coding accuracy of administrative drug claims in the Ontario Drug Benefit data-base. Can J Clin Pharmacol. 2003;10:67–71.
25. Flu W-J, van Kuijk J-P, Chonchol M, Winkel TA, Verhagen HJM, Bax JJ, Poldermans D. Timing of pre-operative beta-blocker treatment in vascular surgery patients: influence on post-operative outcome. J Am Coll Cardiol. 2010;56:1922–1929.
26. Wijeysundera DN, Austin PC, Hux JE, Beattie WS, Buckley DN, Laupacis A. Development of an algorithm to identify preoperative medical consultations using administrative data. Med Care. 2009;47: 1258–1264.
27. Juurlink DN, Mamdani MM, Lee DS, Kopp A, Austin PC, Laupacis A, Redelmeier DA. Rates of hyperkalemia after publication of the Ran-domized Aldactone Evaluation Study. N Engl J Med. 2004;351: 543–551.
28. Helfenstein U. Box-Jenkins modelling in medical research. Stat Methods Med Res. 1996;5:3–22.
29. Eagle KA, Brundage BH, Chaitman BR, Ewy GA, Fleisher LA, Hertzer NR, Leppo JA, Ryan T, Schlant RC, Spencer WH, Spittell JA, Twiss RD, Ritchie JL, Cheitlin MD, Gardner TJ, Garson A, Lewis RP, Gibbons RJ, O’Rourke RA, Ryan TJ. Guidelines for perioperative cardiovascu-lar evaluation for noncardiac surgery: report of the American College of Cardiology/American Heart Association Task Force on Practice Guide-lines. Circulation. 1996;93:1278–1317.
30. Dickey D, Fuller W. Distribution of the estimators for autoregressive time series with a unit root. J Am Stat Assoc. 1979;74:427–431.
31. Ljung GM, Box GEP. Measure of lack of fit in time-series models. Biometrika. 1978;65:297–303.
32. Wagner AK, Soumerai SB, Zhang F, Ross-Degnan D. Segmented re-gression analysis of interrupted time series studies in medication use research. J Clin Pharm Ther. 2002;27:299–309.
33. Antman EM, Lau J, Kupelnick B, Mosteller F, Chalmers TC. A com-parison of results of meta-analyses of randomized control trials and rec-ommendations of clinical experts: treatments for myocardial infarction. JAMA. 1992;268:240–248.
34. Berwick DM. Disseminating innovations in health care. JAMA. 2003;289:1969–1975.
35. Cabana MD, Rand CS, Powe NR, Wu AW, Wilson MH, Abboud PA, Rubin HR. Why don’t physicians follow clinical practice guidelines? A framework for improvement. JAMA. 1999;282:1458–1465.
36. Grol R, Grimshaw J. From best evidence to best practice: effective im-plementation of change in patients’ care. Lancet. 2003;362:1225–1230.
37. Dixon-Woods M, Amalberti R, Goodman S, Bergman B, Glasziou P. Problems and promises of innovation: why healthcare needs to rethink its love/hate relationship with the new. BMJ Qual Saf. 2011;20(Suppl 1): i47–i51.
38. Greenhalgh T, Robert G, Macfarlane F, Bate P, Kyriakidou O. Diffusion of innovations in service organizations: systematic review and recom-mendations. Milbank Q. 2004;82:581–629.
39. Feldman RD. The 1999 Canadian recommendations for the management of hypertension: on behalf of the Task Force for the Development of the 1999 Canadian Recommendations for the Management of Hypertension. Can J Cardiol. 1999;15(Suppl G):57G–64G.
40. Campbell NRC, Tu K, Brant R, Duong-Hua M, McAlister FA, for the Canadian Hypertension Education Program Outcomes Research Task Force. The impact of the Canadian Hypertension Education Program on antihypertensive prescribing trends. Hypertension. 2006;47:22–28.
41. Devereaux PJ, Beattie WS, Choi PT, Badner NH, Guyatt GH, Villar JC, Cina CS, Leslie K, Jacka MJ, Montori VM, Bhandari M, Avezum A, Cavalcanti AB, Giles JW, Schricker T, Yang H, Jakobsen CJ, Yusuf S. How strong is the evidence for the use of perioperative beta blockers in non-cardiac surgery? Systematic review and meta-analysis of ran-domised controlled trials. BMJ. 2005;331:313–321.
42. Ellenberger C, Tait G, Beattie WS. Chronic b blockade is associated with a better outcome after elective noncardiac surgery than acute b block-ade: a single-center propensity-matched cohort study. Anesthesiology. 2011;114:817–823.
43. NICE-SUGAR Investigators. Intensive versus conventional glucose con-trol in critically ill patients. N Engl J Med. 2009;360:1283–1297.
44. Van den Berghe G, Wouters P, Weekers F, Verwaest C, Bruyninckx F, Schetz M, Vlasselaers D, Ferdinande P, Lauwers P, Bouillon R. Intensive insulin therapy in the critically ill patients. N Engl J Med. 2001;345:1359–1367.
by guest on October 20, 2017
http://circoutcomes.ahajournals.org/
Dow
nloaded from

Beattie, Sindhu R. Johnson, Jonathan Kolstad and Mark D. NeumanDuminda N. Wijeysundera, Muhammad Mamdani, Andreas Laupacis, Lee A. Fleisher, W. Scott
Noncardiac Surgery-Blocker Utilization Before MajorβClinical Evidence, Practice Guidelines, and
Print ISSN: 1941-7705. Online ISSN: 1941-7713 Copyright © 2012 American Heart Association, Inc. All rights reserved.
Greenville Avenue, Dallas, TX 75231is published by the American Heart Association, 7272Circulation: Cardiovascular Quality and Outcomes
doi: 10.1161/CIRCOUTCOMES.112.9656322012;5:558-565; originally published online June 26, 2012;Circ Cardiovasc Qual Outcomes.
http://circoutcomes.ahajournals.org/content/5/4/558World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circoutcomes.ahajournals.org/content/suppl/2012/07/12/CIRCOUTCOMES.112.965632.DC1Data Supplement (unedited) at:
http://circoutcomes.ahajournals.org//subscriptions/
at: is onlineCirculation: Cardiovascular Quality and Outcomes Information about subscribing to Subscriptions:
http://www.lww.com/reprints
Information about reprints can be found online at: Reprints:
document. Question and AnswerPermissions and Rightspage under Services. Further information about this process is available in the
which permission is being requested is located, click Request Permissions in the middle column of the WebCopyright Clearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of theCirculation: Cardiovascular Quality and Outcomesin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on October 20, 2017
http://circoutcomes.ahajournals.org/
Dow
nloaded from

SUPPLEMENTAL MATERIAL Supplemental Table 1: Characteristics of individuals who were not previously using beta‐blockers (i.e. those with the potential to receive new preoperative beta‐blocker prescriptions)
1
Cohort
N = 191,481
Demographics
Female sex 104,098 (54.4%)
Age, year, mean (SD) 74.6 (5.8)
Comorbid disease
Coronary artery disease 17,214 (9.0%)
Congestive heart failure 3,890 (2.0%)
Atrial fibrillation 5,788 (3.0%)
Cerebrovascular disease 5,962 (3.1%)
Peripheral vascular disease 15,482 (8.1%)
Hypertension 135,372 (70.7%)
Diabetes mellitus 41,534 (21.7%)
Pulmonary disease 16,753 (8.7%)
Renal disease 3,876 (2.0%)
Revised Cardiac Risk Index score
Zero points 92,768 (48.4%)
One point 70,740 (36.9%)
Two points 21,819 (11.4%)
Three points 4,752 (2.5%)
Four points 1,147 (0.6%)
Five or more points 255 (0.1%)
Procedure
AAA repair 6,931 (3.6%)
Carotid endarterectomy 5,512 (2.9%)
Peripheral vascular bypass 6,335 (3.3%)
Total hip replacement 46,049 (24.0%)
Total knee replacement 77,872 (40.7%)

Large bowel surgery 31,543 (16.5%)
Liver resection 1,212 (0.6%)
Whipple procedure 865 (0.5%)
Pneumonectomy or lobectomy 5,436 (2.8%)
Gastrectomy or esophagectomy 3,256 (1.7%)
Nephrectomy 4,567 (2.4%)
Cystectomy 1,903 (1.0%)
Abbreviations: AAA, abdominal aortic aneurysm; SD, standard deviation
2

Supplemental Figure 1: Trends in new outpatient prescriptions for beta‐blockers within 60 days before major elective vascular surgery procedures in Ontario
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
050
100
150
200
250
DECREASE-1 POISE2002 AHA Guidelines 2006 AHA Guidelines
DIPOM
Lindenauer
Date of Hospital Admission
New
Pre
scrip
tions
(pe
r 10
00 p
roce
dure
s)
Rates of new beta‐blocker prescriptions before elective vascular non‐cardiac surgery in Ontario, Canada. These rates (per 1000 procedures) are reported for three‐month periods from 1 April 1999 to 31 March 2010. The vertical lines represent the timing of publications that may have influenced rates of perioperative beta‐blockade.
3

![Ball−McCulloch−Frantz− © The McGraw−Hill Competitive ...1].pdf · ment professors, “business strategy is now the single most im-portant management issue and will remain](https://static.fdocument.org/doc/165x107/5f2d53eba8a6e10b782099f0/ballamccullochafrantza-the-mcgrawahill-competitive-1pdf-ment.jpg)


![γ λ ω σσά ρι - eclass.unipi.gr¬κρο... · βιώσιμη ανάπτυξη [sustainable develop-ment]: ανάπτυξη που στηρίζεται σε αρ-χές βιωσιμότητας·](https://static.fdocument.org/doc/165x107/5f8931a73a61df27043aeb63/-ff-f-sustainable.jpg)










![ΠΤΡΟ Ν. ΠΑΠΑΪΩΑΝΝΟΤ MD. PHD. FESC · safety end point (Thrombolysis in Myocardial Infarction [TIMI] major bleeding not related to coronary-artery bypass grafting)](https://static.fdocument.org/doc/165x107/5f765ace2664f83f9d7549d0/-md-phd-fesc-safety-end-point-thrombolysis.jpg)
