Παρουσίαση του PowerPoint · After joint compression in a neutral hip position, the...
40
A. PANAGOPOULOS FEMOROACETABULAR IMPINGEMENT
Transcript of Παρουσίαση του PowerPoint · After joint compression in a neutral hip position, the...

A. PANAGOPOULOS
Η εμβιομηχανική του κοτυλιαίου επιχειλίου χόνδρου και η συσχέτισή του με την πρώιμη οστεοαρθρίτιδα του ισχίου
FEMOROACETABULAR IMPINGEMENT

The majority of patients that undergo
THA have a structural disorder of the hip
Primary hip arthritis is extremely rare
Normal
Impingement Instability
Facts

Hip homeostasis Hip homeostasis
impingement instability
activity
injury age
biology
systemic disorders
Hip disease

The most durable, biologically friendly bearing surface is hyaline cartilage-on hyaline cartilage
Facts

Hip and groin injuries account for 5-6% of all adult athletic injuries FAI was first reported in 1957 by Paterson and has more recently been recognized as a site of pathology in symptomatic hips.
Overview
There are two different etiologies, termed CAM and Pincer impingement. They can occur in isolation or together

Hip Anatomy
- ball and socket joint, 3 degrees of freedom.
- articular cartilage ------ type II collagen.
- ligamentum teres may play a role in stability.

Hip Anatomy
Iliofemoral ligament Lies anterior and tightens with extension. Pubofemoral ligament Lies inferomedially which tightens in hip extension and abduction. Ischiofemoral ligament Runs horizontally and posteriorlly. Fibers tighten with extension and limit internal rotation.
Three major ligaments surround the hip:

Labrum
Labrum’s main functions include: Deepening the socket Enhancing stability by providing a negative intra-articular pressure It is also suggested that the labrum is involved in proprioception

An intact labrum causes more equal fluid distribution during weight bearing, resulting in less cartilage deformation, low friction articulation, and less stress across the hip joint (Ferguson et al. 2000, 2003)
Labrum

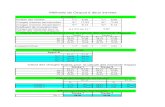
In normal hips, the labrum supports 1–2% of the total load applied across the hip joint under simulation of normal walking In developmental dysplasia (DDH), the supporting load at the labrum increases as much as 4–11% of the total load applied across the joint (Henak et al. 2011)
Labrum biomechanics

Am J Sports Med 2011 39: 103S
After joint compression in a neutral hip position, the labrum continues to resist femoral head dislocation 2 cm or more detachment of the acetabular labrum is needed before hip stability decreases.

Contact between the femoral head-neck junction and the acetabular rim. Impingement occurs with the combined movement of hip flexion, adduction, and internal rotation
Definition of FAI

Younger population (20-40) especially dancers, other sports 10-15% prevalence rate (Tannast et al), (Leunig et al) Gender differences (Ganz et al)
Cam-type FAI - young males. Pincer-type FAI - middle-aged women.
51% FAI in 35 adolescents with anterior groin pain and (+) impingement test Sink et al 63% FAI in 292 males (ages 16-50) with mechanical hip pathology Nogier et al
Prevalence of FAI

Developmental factors:
Coxa profunda
Protrusio acetabuli
Asphericity of femoral head
Reduced femoral head-neck offset
Maloriented acetabulum
SCFE
Samora (2011)
Etiology of FAI

Normal hip CAM FAI Pincer FAI

Aspherical femoral head
Bony prominence at anterolateral head-neck junction
Impinges on rim of acetabulum
Leads to superior OA
CAM type of FAI

In cam FAI, the prominent femoral head/neck junction (C) is jammed into the acetabulum causing damage to the peripheral cartilage at flexion and internal rotation
CAM type of FAI

Overcoverage of femoral head by acetabulum
Acetabulum impinges on neck of femur
Leads to posterior-inferior or central OA
Samora (2011)
Pincer type of FAI

In pincer FAI, linear impact due to the acetabular overcoverage occurs anteriorly. The persistent anterior abutment with chronic leverage of the head in the acetabulum sometimes results in chondral injury in the ‘‘contrecoup’’ region of the posterior-inferior acetabulum.
Pincer type of FAI

CAM type of FAI
Pincer type of FAI In pincer FAI, the linear impact leads to substantial labral damage, while in early phases the adjacent cartilage remains intact.
cam FAI frequently reveals deep-reaching flap-like cleavage lesions of cartilage from the subchondral bone early in the disease.

Symptoms
Persistent insidious deep groin, lateral, or buttock pain Anterior groin pain most common- increased with prolonged sitting or standing and hip flexion-type movements Decreased hip ROM Insidious on-set 50% of cases Difficulty with end range movements

Martin et al JOSPT July 2006 Intra-articular Tests
• FABER Test
• FADIR Test
• Scour Test
• Resisted SLR
• Log Roll Test
Hip special tests

FABER test
with patient supine, limb to be in figure 4 position resting just proximal to contralateral knee. Press on crossed knee while applying counterpressure on opposite anterior superior iliac spine. Posterior hip pain indicates SI joint pathology. Anterior hip pain indicates hip arthritis.

FADIR test
The examiner passively moves the patient’s lower extremity into a position of hip flexion, adduction, and internal rotation. A positive test is reflected by increased hip or groin pain.

The hip is maximally flexed and adducted. Then, with a compressive force applied to the joint in the direction of the shaft of the femur, the examiner moves the femur through a circular arc of motion. The maneuver is considered positive if it recreates pain.
Scour test

Resisted Straight Leg Rise test
assesses labral loading

Log roll test
maximal available range of hip external and internal rotation Eliciting a clicking or popping sensation may indicate an acetabular labral tear

X-Rays of Cam-type FAI
Pistol grip deformity
45 degrees Dunn lateral x-ray = α-angle > 63o is abnormal 45 degrees Dunn x lateral x-ray = Head-Neck Ofset /radius of head = HNO ratio (0.21)

X-Rays of Pincer-type FAI
a) the ischial spine sign, b) the posterior wall sign, c) the cross-over sign d) the calculation of the acetabular retroversion index (ARI), defined as ARI = (BC/AB) × 100. (normally >33%)

May demonstrate labral tear, but often the bony articular pathology are missed
Only 22% sensitivity for cartilage delamination
Gold standard is magnetic resonance arthrogram
MRI (arthrography) pincer
cam

Hip Dysplasia (Adult Form)
Lumbar Spine Pain (Low Back Pain)
Lumbar Radiculopathy ( Low Back Facet Disease)
Sacroiliitis (SI Pain/Dysfunction, back of pelvis)
Trochanteric Bursitis (Outside/Lateral Hip Pain)
Piriformis Syndrome (Back of Hip Pain)
Psychosomatic Pain Disorder (Stress Related Illness)
Iliopsoas Tendinitis
Sports hernia
Differential diagnosis

Treatment
Conservative Surgical • “safe open dislocation”
• Mini open repair technique
• Hip arthroscopy

Highly dependent on the severity of the structural impingement, stage of secondary OA, patient age and patient activity level. • relative rest, • activity modification, • NSAID’s, • local and global strengthening • corticosteroid injections.
Conservative
Hoeksma et al, reported a success rate for manual therapy of 81% versus 50% for exercise.

Ganz 2001 Trochanteric flip osteotomy “starting from posterior area of greater trochanter” Z-capsulotomy – avoid vessels shave off slivers of the area of concern in a stepwise fashion Inspection of labrum Osteochondroplasty
Open surgical dislocation

Mini open repair
“Heuter Approach”or “Short Smith-Pete” Lateral position – traction internervous plane between the femoral nerve (Sartorius) and the superior gluteal nerve (tensor fascia lata). High speed burr for osteochondroplasty

Hip arthroscopy
Lateral or supine position traction device and fluoroscopy anterior, anterolateral, and posterolateral portals Debridement of labrum Chondroplasty Microfracture?

Questions remain, however, about whether FAI is a cause or a result of OA, and whether the joint deformities in FAI are congenital or developmental or are the reaction to the arthritic process, as in the case of osteophytes.

The Genetics of Osteoarthritis and Lifestyle (GOAL) study hip morphology in 566 pt with unilateral hip OA with the contralateral asymptomatic hip and non-osteoarthritic control hips in 1,100 patients who had undergone intravenous urography. All patients were aged ≥45 years (mean, 66 years), and 48% of the subjects were women. 5.5% risk of developing OA in the contralateral non-osteoarthritic hip, compared with a 3% risk in the control group.
Cross-sectional studies

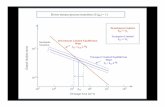
723 patients presenting for the first time with recent onset of hip or knee pain 80% were female, ranging in age from 45 to 65 years. Subjects had doubtful or no OA at baseline, with a Kellgren-Lawrence osteoarthritic grade of 0 or 1 (76% and 24%, respectively). Initial AP pelvic radiographs were measured to determine the alpha angle, and subjects were followed for 5 years Hips with a baseline AP alpha angle >83° had a 25% risk of developing end-stage OA within 5 years, compared with a <2% risk of end-stage OA in hips with an alpha angle of <83°
Longitundinal studies
Cohort Hip and Cohort Knee (CHECK) stydy

Based on cross-sectional studies in which FAI morphology was studied before the presence of radiographic osteoarthritis (OA), and on prevalence studies in younger, asymptomatic persons, it is clear that FAI and its morphologic risk factors are common in young adult hips and predispose to the later development of OA in certain patients.