SeabuPure® - The Best Ingredient for Health Care and Personal Care
Chronic Lyme Disease—The Standard of Care
ξ Two equally legitimate but divergent standards of care currently exist for the diagnosis and treatment of Lyme disease: IDSA guidelines and ILADS guidelines
1) Johnson L, Stricker RB. Treatment of Lyme disease: a medicolegal assessment. Expert Rev Anti Infect Ther. 2004 Aug;2(4):533-57.
2) Evidence-based guidelines for the management of Lyme Disease.
Cameron, Horowitz, et al. Expert Review of Anti Infective Therapy 2(1) 2004
ξ Many doctors in the United States do not follow IDSA guidelines. They treat for seronegative disease, and treat for extended periods of time. “For chronic Lyme disease, 57% of responders treat 3 months or more.”
ξ Ziska MH, Donta ST, Demarest FC. Physician preferences in the diagnosis and treatment of Lyme disease in the United States. Infection 1996 Mar-Apr;24(2):182-6.
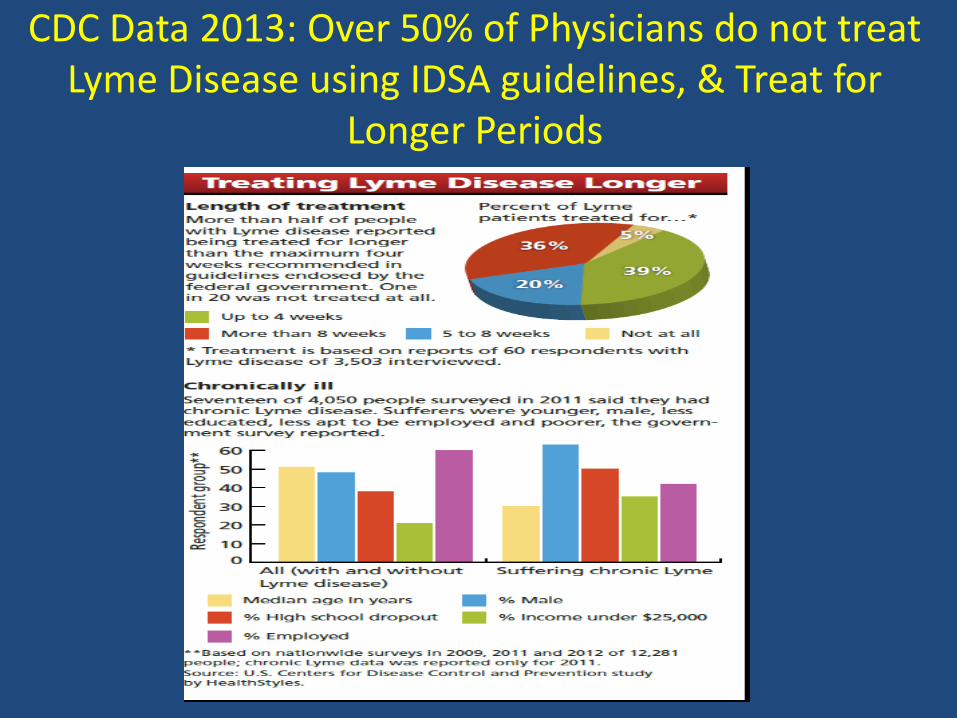
CDC Data 2013: Over 50% of Physicians do not treat Lyme Disease using IDSA guidelines, & Treat for
Longer Periods
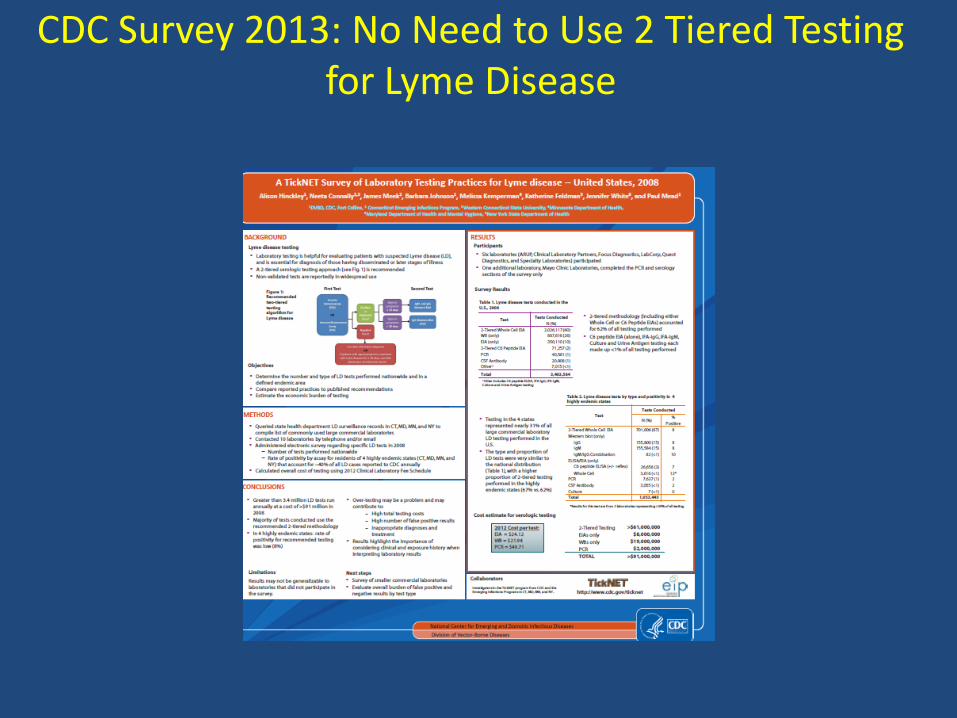
CDC Survey 2013: No Need to Use 2 Tiered Testing for Lyme Disease
Need to Change the CDC/EUCALB criteria
• The IDSA and the European Concerted Action on Lyme Borreliosis (EUCALB, Diagnosis: www.eucalb.com; September 2013) recommend a two-tier testing approach. According to these guidelines, an immunoblot is not to be performed if the ELISA is negative, despite the poor sensitivity of ELISA tests ranging from 34 to 70.5%.
• Effect: Missing roughly half of the people with Lyme disease
-Marangoni, A. et al. Comparative evaluation of three different ELISA methods for the
diagnosis of early culture-confirmed Lyme disease in Italy. J. Med. Microbiol. 54, 361-367 (2005);
-Ang, C.W.,et al. T. Large differences between test strategies for the detection of anti-Borrelia antibodies are revealed by comparing eight ELISAs and five immunoblots. Eur. J. Clin. Microbiol. Infect. Dis. 30, 1027-1032 (2011).
-Wojciechowska-Koszko, et al. Serodiagnosis of borreliosis: indirect immunofluorescence assay, enzymelinked immunosorbent assay and immunoblotting. Arch. Immunol. Ther. Exp. 59, 69-77 (2011).
Lyme Disease Diagnosis: Problems with Testing
1)Intra and Interlaboratory Variation in LD testing -Marangoni J Med Microbiol 2005: 3 different commercial
Elisa tests showed discrepant results. Sensitivity for the same sera 36,8% to 70.5%
-De Marteno Med Mal Infect 2007: Compared 14 Elisa test kits for the diagnosis of neuro Lyme. Sensitivity varied from 20.9% -97.7%
2) Testing Issues: Different species of Borrelia: Rudenko FEMS Microbiol Letter 2009 ; Bouattour Arch Inst Pasteur Tunis 2004 ; Lopes de Carvalho Clin Rheumatol 2008
3) Problems with 2 -Tiered Testing -In 2005, John’s Hopkins University study: found CDC two
tiered testing missed up to 55% of positive Lyme cases Coulter,et al.,J Clin Microbiol 2005;43:5080-5084. CDC correspondance with NYS DOH
Understanding the Role of Laboratory Testing in Lyme Disease and Other Tick Borne Diseases
– The utility of the Western Blot is based on understanding specific bands which reflect exposure to Bb: 23, 31, 34, 39, 83-93
– PCR testing is an important diagnostic tool for seronegative patients, but many require multiple sets over time,? Culture (Advanced Labs)/ ? LTT
– 10-20% of the Borrelia presently in ticks (US) are not Borrelia burgdorferi, but are genetically related to Borrelia miyamotoi, the agent of relapsing fever in Japan. These organisms will not test positive by ELISA, Western Blot, or PCR assays for Lyme Disease. Other tick-borne diseases such as Babesia and Bartonella also may not test positive
Sont vos symptômes dus à la
maladie de Lyme?
Prendre le questionnaire
symptomatologique des SIMS (Syndrome Infectieux Multi Systémique)
/ML de Horowitz dans mon livre
C’est un outil indispensable pour
déterminer la probabilité d’un SIMS et/ou
d’une maladie de Lyme (sans rash EM)
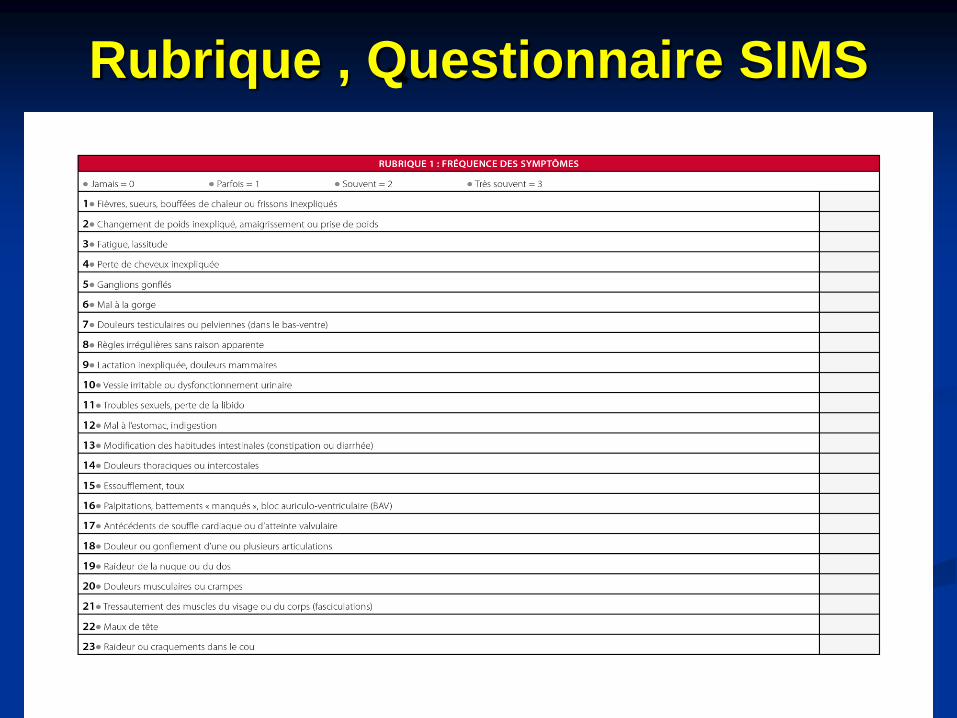
Rubrique , Questionnaire SIMS
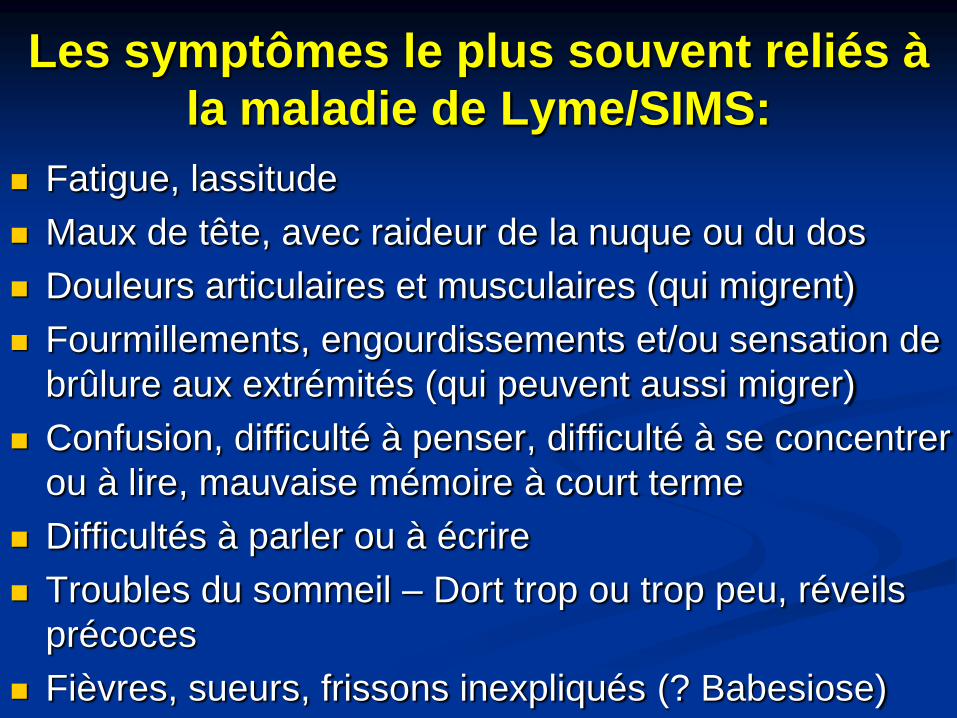
Les symptômes le plus souvent reliés à
la maladie de Lyme/SIMS:
Fatigue, lassitude
Maux de tête, avec raideur de la nuque ou du dos
Douleurs articulaires et musculaires (qui migrent)
Fourmillements, engourdissements et/ou sensation de
brûlure aux extrémités (qui peuvent aussi migrer)
Confusion, difficulté à penser, difficulté à se concentrer
ou à lire, mauvaise mémoire à court terme
Difficultés à parler ou à écrire
Troubles du sommeil – Dort trop ou trop peu, réveils
précoces
Fièvres, sueurs, frissons inexpliqués (? Babesiose)
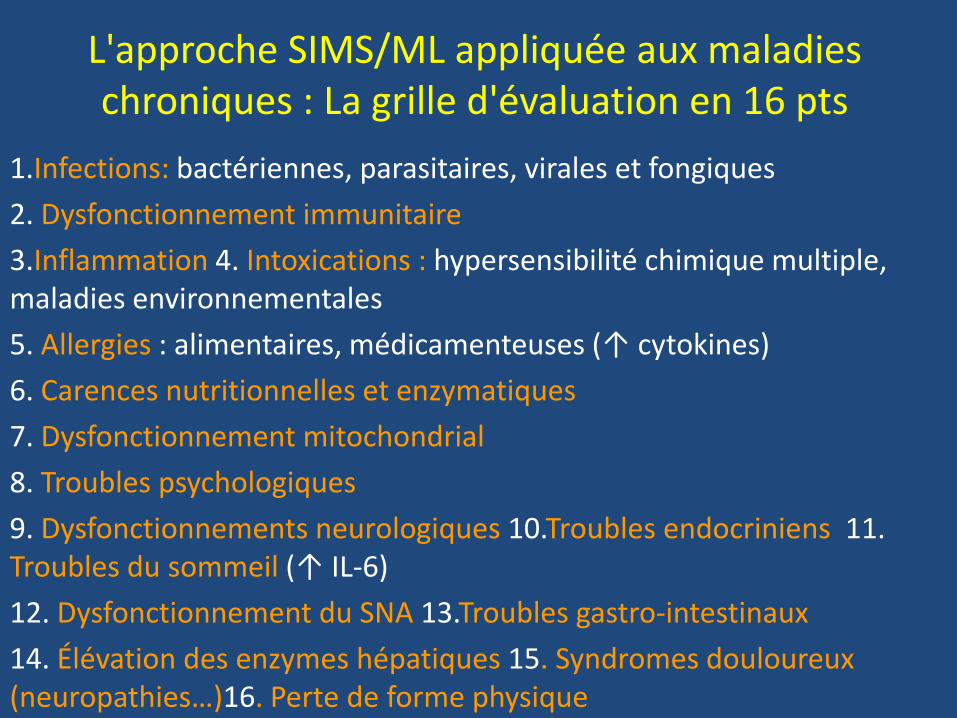
L'approche SIMS/ML appliquée aux maladies chroniques : La grille d'évaluation en 16 pts
1.Infections: bactériennes, parasitaires, virales et fongiques
2. Dysfonctionnement immunitaire
3.Inflammation 4. Intoxications : hypersensibilité chimique multiple, maladies environnementales
5. Allergies : alimentaires, médicamenteuses (↑ cytokines)
6. Carences nutritionnelles et enzymatiques
7. Dysfonctionnement mitochondrial
8. Troubles psychologiques
9. Dysfonctionnements neurologiques 10.Troubles endocriniens 11. Troubles du sommeil (↑ IL-6)
12. Dysfonctionnement du SNA 13.Troubles gastro-intestinaux
14. Élévation des enzymes hépatiques 15. Syndromes douloureux (neuropathies…)16. Perte de forme physique
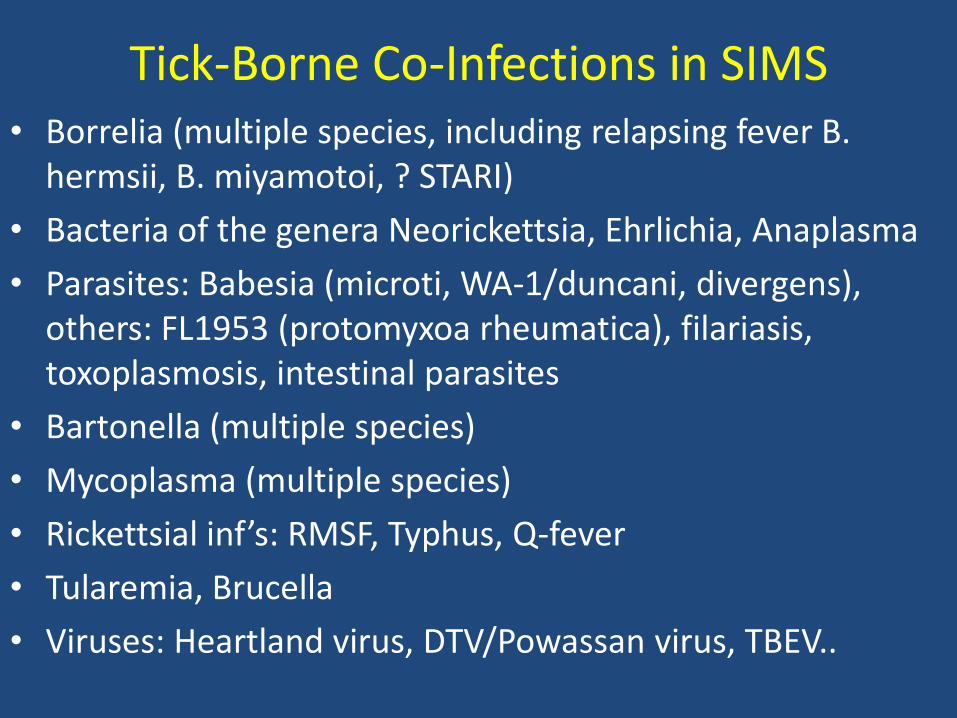
Tick-Borne Co-Infections in SIMS • Borrelia (multiple species, including relapsing fever B.
hermsii, B. miyamotoi, ? STARI)
• Bacteria of the genera Neorickettsia, Ehrlichia, Anaplasma
• Parasites: Babesia (microti, WA-1/duncani, divergens), others: FL1953 (protomyxoa rheumatica), filariasis, toxoplasmosis, intestinal parasites
• Bartonella (multiple species)
• Mycoplasma (multiple species)
• Rickettsial inf’s: RMSF, Typhus, Q-fever
• Tularemia, Brucella
• Viruses: Heartland virus, DTV/Powassan virus, TBEV..
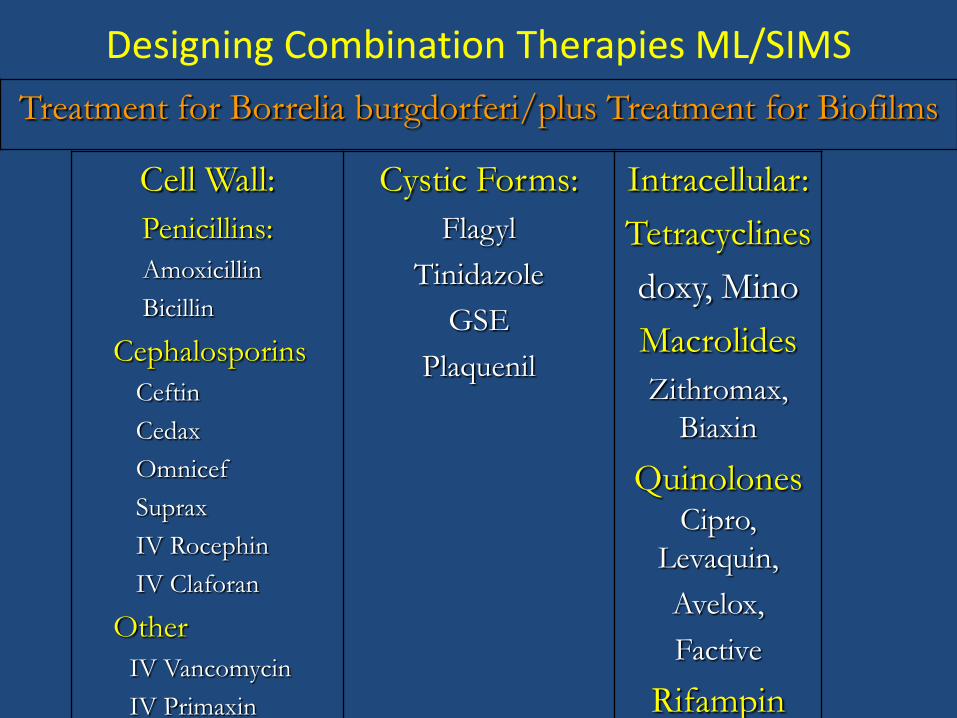
Designing Combination Therapies ML/SIMS
Cell Wall:
Penicillins:
Amoxicillin
Bicillin
Cephalosporins
Ceftin
Cedax
Omnicef
Suprax
IV Rocephin
IV Claforan
Other
IV Vancomycin
IV Primaxin
Cystic Forms:
Flagyl
Tinidazole
GSE
Plaquenil
Intracellular:
Tetracyclines
doxy, Mino
Macrolides
Zithromax,
Biaxin
QuinolonesCipro,
Levaquin,
Avelox,
Factive
Rifampin
Treatment for Borrelia burgdorferi/plus Treatment for Biofilms
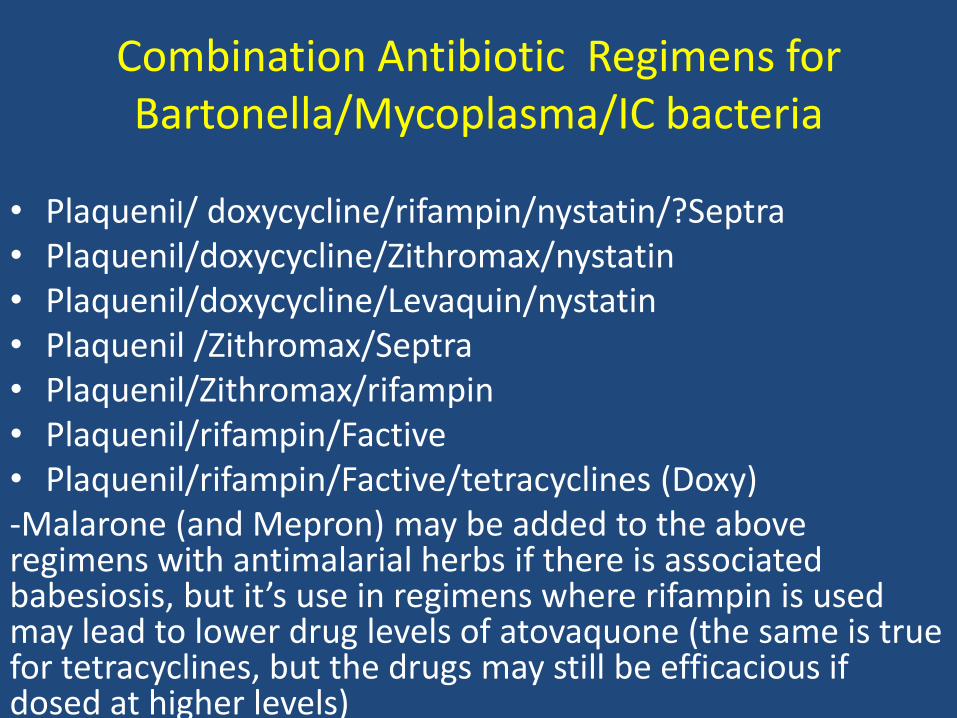
Combination Antibiotic Regimens for Bartonella/Mycoplasma/IC bacteria
• Plaquenil/ doxycycline/rifampin/nystatin/?Septra • Plaquenil/doxycycline/Zithromax/nystatin • Plaquenil/doxycycline/Levaquin/nystatin • Plaquenil /Zithromax/Septra • Plaquenil/Zithromax/rifampin • Plaquenil/rifampin/Factive • Plaquenil/rifampin/Factive/tetracyclines (Doxy) -Malarone (and Mepron) may be added to the above regimens with antimalarial herbs if there is associated babesiosis, but it’s use in regimens where rifampin is used may lead to lower drug levels of atovaquone (the same is true for tetracyclines, but the drugs may still be efficacious if dosed at higher levels) -
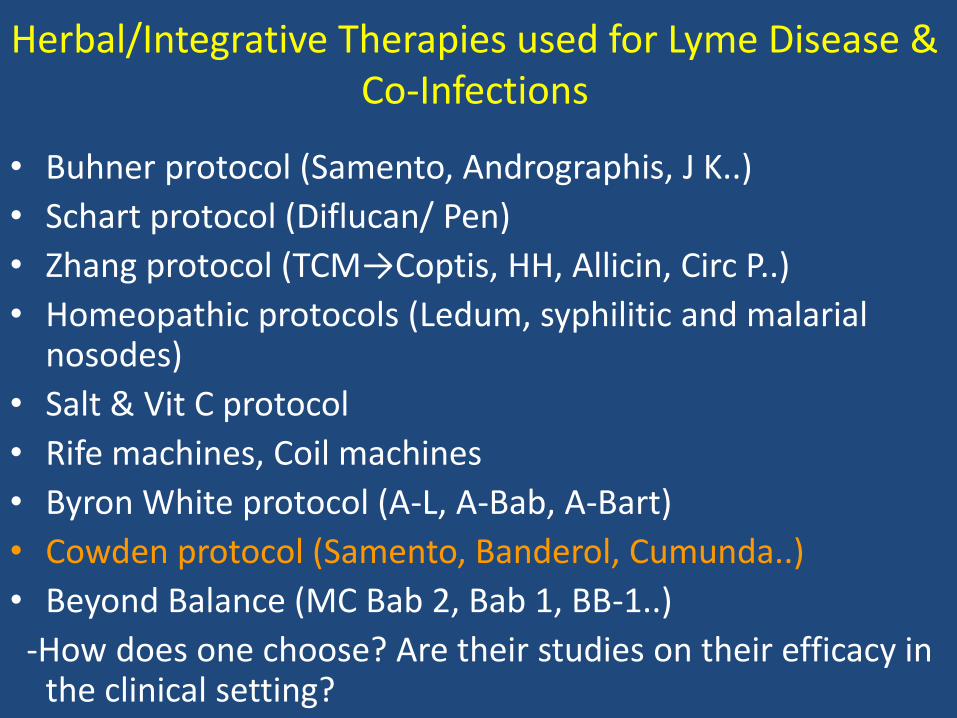
Herbal/Integrative Therapies used for Lyme Disease & Co-Infections
• Buhner protocol (Samento, Andrographis, J K..)
• Schart protocol (Diflucan/ Pen)
• Zhang protocol (TCM→Coptis, HH, Allicin, Circ P..)
• Homeopathic protocols (Ledum, syphilitic and malarial nosodes)
• Salt & Vit C protocol
• Rife machines, Coil machines
• Byron White protocol (A-L, A-Bab, A-Bart)
• Cowden protocol (Samento, Banderol, Cumunda..)
• Beyond Balance (MC Bab 2, Bab 1, BB-1..)
-How does one choose? Are their studies on their efficacy in the clinical setting?
SIMS: Un modèle multifactoriel pour
toutes les maladies chroniques
Ces 16 causes multifactorielles sont souvent au
cœur des états pathologiques chroniques.
Determiner en chaque personne des facteurs
multiples qui sont responsable pour leurs
symptômes
Une fois que tous les différents facteurs sont
découvert et convenablement traités, la plupart
des gens avec du fatigue, les douleurs, troubles
de sommeil, confusion, difficultés à penser, ou
mauvaise mémoire à court terme aller mieux
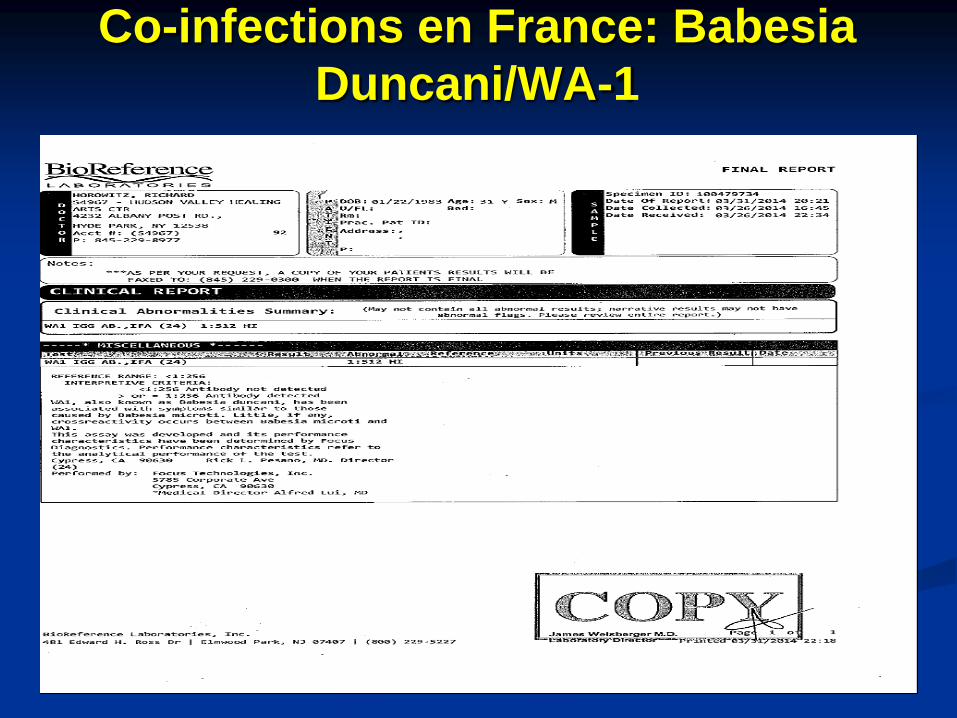
Co-infections en France: Babesia
Duncani/WA-1
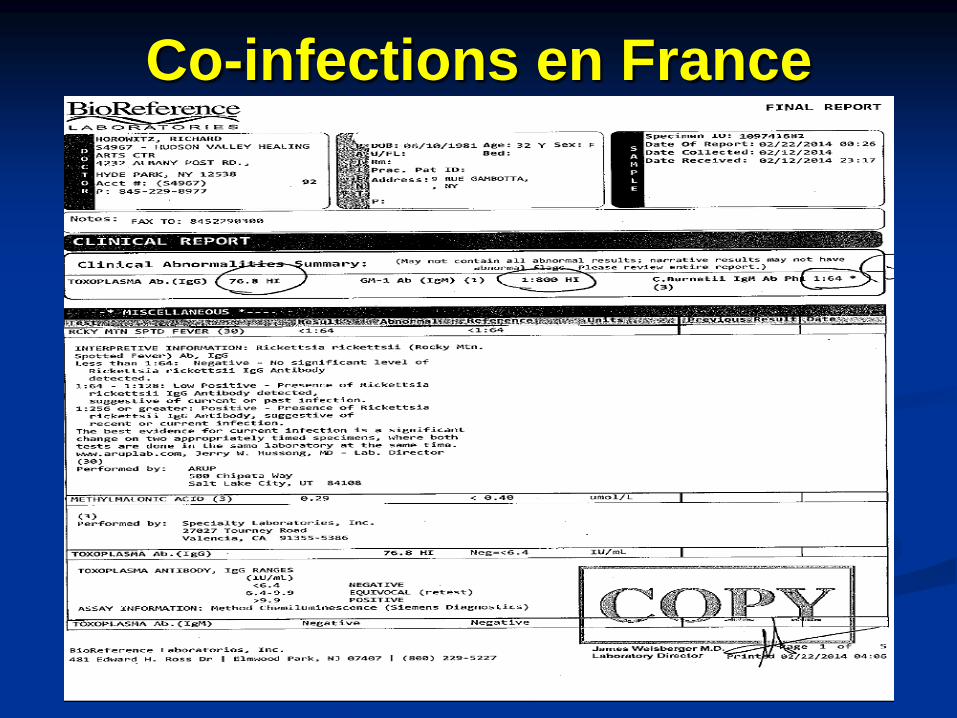
Co-infections en France
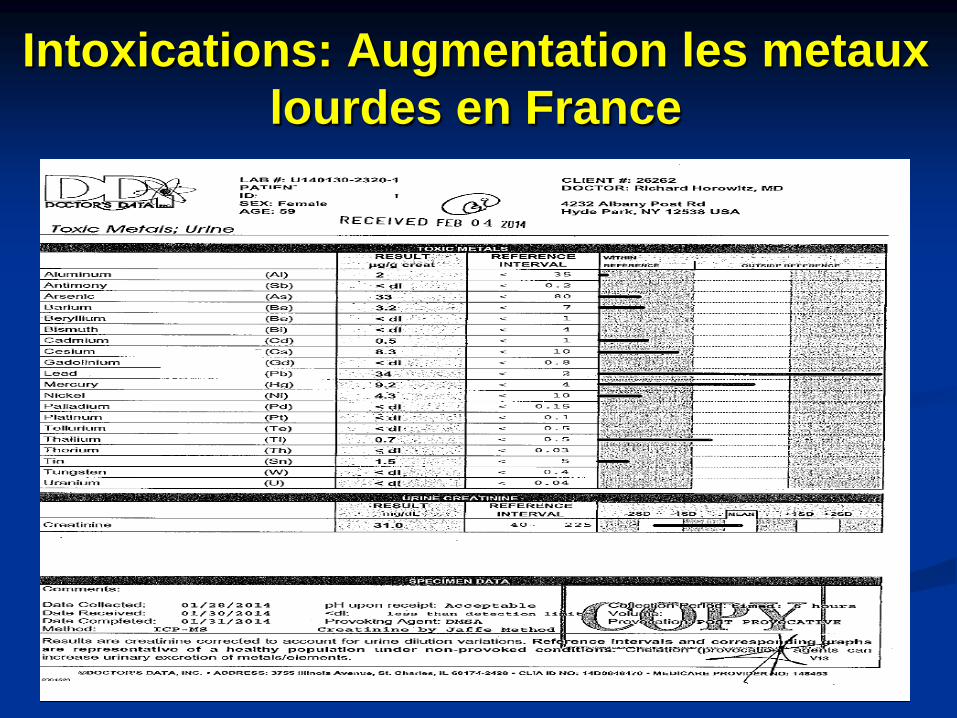
Intoxications: Augmentation les metaux
lourdes en France
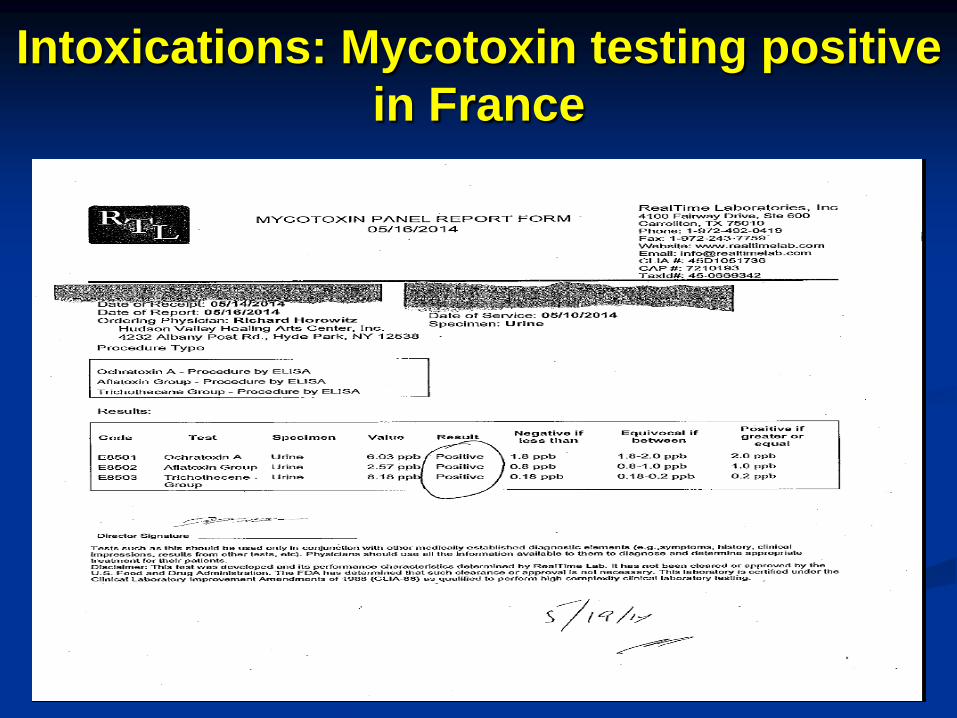
Intoxications: Mycotoxin testing positive
in France
Vous Pouvez Avoir L’Espoir!
Chez les patients français qui sont venus
me voir, lorsqu'on a utilisé la grille de
diagnostic différentiel en 16 points, on a
trouvé que de multiples causes à leurs
symptômes chroniques (résistants) se
superposaient. Une fois traités, l'état de
ces patients qui souffraient depuis des
années a été amélioré.
Douleurs, fatigue, confusion…
Pourquoi je ne m’en sors pas ?
Résoudre le mystère de Lyme et des maladies
chroniques inexpliquées: Editions Thierry Soucar
Juin 2014
J Ju
Why Can't I Get Better?
Richard Horowitz, M.D.
HC ISBN-13: 978-1-250-01940-0
ISBN-10: 1-250-01940-0
6 1/8 9 ¼ ● 526 pages
EISBN-13: 978-1-250-03848-7, St Martin’s Press et Editions Thierry Soucar 2014