4002771 AVANCES 25-3€¦ · avances en 175 Abstract Type 1 diabetes (T1D) is a chronic...
12
Av Diabetol. 2009;25:175-86 Diabetología avances en 175 Abstract Type 1 diabetes (T1D) is a chronic immune-mediated disease, charac- terised by a selective loss of insulin-producing β-cells in the pancreatic islets. Susceptibility is determined by interactions of multiple genes with unknown environmental factors. Around 50% of the genetic risk of the disease is explained by HLA, although other genes with a smaller effect are also involved. Most of the known risk genes for T1D play a role in immunity, mostly through T-cell regulation (CTLA4, PTPN22, IL-2RA) and cytokine production or modulation (VDR, SUMO4). The insulin gene (INS) represents and exception to this, and is probably the only gene specifically associated with T1D and not with other autoimmune dis- eases. Ongoing genome-wide association studies are providing evi- dence of multiple known and previously unknown risk genes. New ana- lytical tools are continuously being developed to handle the vast amounts of data produced, as well as to account for multiple compari- sons and assess combined effects such as gene-gene and gene-envi- ronment interactions. In this review, we will give an overview of the most important genes identified to date, analyse the genetic evidence sup- porting them as T1D susceptibility genes and discuss the mechanisms mediating their contribution to the pathogenesis of the disease. Keywords: autoimmune, insuline-dependent, family risk, prediction. Introduction Type 1 diabetes (T1D) is one of the most common chron- ic diseases in childhood, with an incidence ranging from 0.1 to 64/100 000 per year (China vs Finland) and in- creasing in most of the countries where it has been stud- ied DIAMOND and EURODIAB. 1,2-5 In Spain, accord- ing to most studies, the incidence per 100,000 inhabitants and year ranges between 9.5 and 16.4 for children diag- nosed before the age of 15. 6-13 An exception to these are represented by recent results from Castilla-Leon, show- ing an incidence of 22/100,000/yr, 14 from Ciudad Real (26/100,000/yr) 15 and data from the Canary Islands. The latter region has the highest rate of childhood T1D ever reported in Spain, with the most recent incidence (32/100,000/yr on the island of La Palma) approaching that of some Northern European countries. 16,17 In addi- tion, some studies show an increasing trend in the inci- dence of T1D in Spain, 12,16 whereas others do not. 6 Type 1A diabetes (T1D) is a complex, multifactorial dis- ease, which leads to the autoimmune destruction of pancre- atic, insulin-producing, β-cells. Its ultimate cause is un- known, but both environmental and genetic factors have proved to play a role in its development. The present review will focus on the latter. Although only 10-12% of patients with T1D have a family history of the disease at diagnosis, with longer follow-up the frequency increases to up to 25%. 18 In addition, having a rst degree relative with the disease increases the risk from 2.5 to more than 100 times, depending on who the affected family member is (table 1). The most established genetic locus contributing to T1D and many other autoimmune diseases is the major histo- compatibility complex (MHC), which includes the genes encoding the human leukocyte antigen gene (HLA), cru- cial in antigen presentation. In addition, several other genes have been established as contributing to the devel- opment of the disease, although to a smaller extent than HLA. More than 20 different loci have been proposed to account for the genetic risk of T1D (gure 1), but only a minority had been confirmed until very recently. At Revisión Genetics of type 1 diabetes: recent progress and future perspectives A.M. Wägner, J.C. Wiebe Endocrinology Dept. Hospital Universitario Insular de Gran Canaria Date received: 24 th November 2008 Date accepted: 7 th May 2009 Correspondence: A.M. Wägner, MD PhD. Servicio de Endocrinología y Nutrición. Hospital Universitario Insular de Gran Canaria. Avda. Marítima del Sur, s/n. 35016 Las Palmas de Gran Canaria. E-mail: [email protected] Abbreviations: HLA: human leukocyte antigen; INS: insulin gene; IL-2: interleukin-2; IL-2RA: interleukin-2 receptor; Lyp: lymphoid protein tyrosine kinase; MHC: major compatibility complex; PTPN22: protein tyrosine phosphatase non-receptor type 22; SNP: single-nucleotide polymorphisms, SUMO: small ubiquitin-like modifier; T1D: type 1 diabetes; VDR: vitamin D receptor; VNTR: variable number of tandem repeat.
Transcript of 4002771 AVANCES 25-3€¦ · avances en 175 Abstract Type 1 diabetes (T1D) is a chronic...

Av Diabetol. 2009;25:175-86Diabetologíaavances en
175
AbstractType 1 diabetes (T1D) is a chronic immune-mediated disease, charac-terised by a selective loss of insulin-producing β-cells in the pancreatic islets. Susceptibility is determined by interactions of multiple genes with unknown environmental factors. Around 50% of the genetic risk of the disease is explained by HLA, although other genes with a smaller effect are also involved. Most of the known risk genes for T1D play a role in immunity, mostly through T-cell regulation (CTLA4, PTPN22, IL-2RA) and cytokine production or modulation (VDR, SUMO4). The insulin gene (INS) represents and exception to this, and is probably the only gene specifi cally associated with T1D and not with other autoimmune dis-eases. Ongoing genome-wide association studies are providing evi-dence of multiple known and previously unknown risk genes. New ana-lytical tools are continuously being developed to handle the vast amounts of data produced, as well as to account for multiple compari-sons and assess combined effects such as gene-gene and gene-envi-ronment interactions. In this review, we will give an overview of the most important genes identifi ed to date, analyse the genetic evidence sup-porting them as T1D susceptibility genes and discuss the mechanisms mediating their contribution to the pathogenesis of the disease.
Keywords: autoimmune, insuline-dependent, family risk, prediction.
IntroductionType 1 diabetes (T1D) is one of the most common chron-ic diseases in childhood, with an incidence ranging from
0.1 to 64/100 000 per year (China vs Finland) and in-creasing in most of the countries where it has been stud-ied DIAMOND and EURODIAB.1,2-5 In Spain, accord-ing to most studies, the incidence per 100,000 inhabitants and year ranges between 9.5 and 16.4 for children diag-nosed before the age of 15.6-13 An exception to these are represented by recent results from Castilla-Leon, show-ing an incidence of 22/100,000/yr,14 from Ciudad Real (26/100,000/yr)15 and data from the Canary Islands. The latter region has the highest rate of childhood T1D ever reported in Spain, with the most recent incidence (32/100,000/yr on the island of La Palma) approaching that of some Northern European countries.16,17 In addi-tion, some studies show an increasing trend in the inci-dence of T1D in Spain,12,16 whereas others do not.6
Type 1A diabetes (T1D) is a complex, multifactorial dis-ease, which leads to the autoimmune destruction of pancre-atic, insulin-producing, β-cells. Its ultimate cause is un-known, but both environmental and genetic factors have proved to play a role in its development. The present review will focus on the latter. Although only 10-12% of patients with T1D have a family history of the disease at diagnosis, with longer follow-up the frequency increases to up to 25%.18 In addition, having a Þ rst degree relative with the disease increases the risk from 2.5 to more than 100 times, depending on who the affected family member is (table 1).
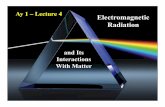
The most established genetic locus contributing to T1D and many other autoimmune diseases is the major histo-compatibility complex (MHC), which includes the genes encoding the human leukocyte antigen gene (HLA), cru-cial in antigen presentation. In addition, several other genes have been established as contributing to the devel-opment of the disease, although to a smaller extent than HLA. More than 20 different loci have been proposed to account for the genetic risk of T1D (Þ gure 1), but only a minority had been confirmed until very recently. At
Revisión
Genetics of type 1 diabetes: recent progress and future perspectivesA.M. Wägner, J.C. WiebeEndocrinology Dept. Hospital Universitario Insular de Gran Canaria
Date received: 24th November 2008Date accepted: 7th May 2009
Correspondence: A.M. Wägner, MD PhD. Servicio de Endocrinología y Nutrición. Hospital Universitario Insular de Gran Canaria. Avda. Marítima del Sur, s/n. 35016 Las Palmas de Gran Canaria. E-mail: [email protected]
Abbreviations:HLA: human leukocyte antigen; INS: insulin gene; IL-2: interleukin-2; IL-2RA: interleukin-2 receptor; Lyp: lymphoid protein tyrosine kinase; MHC: major compatibility complex; PTPN22: protein tyrosine phosphatase non-receptor type 22; SNP: single-nucleotide polymorphisms, SUMO: small ubiquitin-like modifier; T1D: type 1 diabetes; VDR: vitamin D receptor; VNTR: variable number of tandem repeat.

Av Diabetol. 2009;25:175-86
176
present, we are witnessing an «explosion» of risk genes, thanks to the availability of new genotyping technolo-gies and bioinformatic tools.
Recent development in genetic researchThe genotyping and analytical tools made available in recent years have profoundly changed the way we under-stand genetics research. Genotyping methods have al-lowed for several hundreds of thousands genetic varia-tions to be studied, as opposed to only a few at a time with previous technology. This fact has also changed the strategy of studies, moving from directed, hypothesis-based search for candidate genes to non hypothesis-based, unbiased whole genome association studies which
complement the former. Sample sizes have increased from a few hundreds to many thousands of patients. In complex diseases like diabetes, this increase in sample size is crucial if we aim to identify genes with moderate effects on disease risk. In that sense, we have moved from competition to collaboration between research groups and large networks and consortia have been established: the Type 1 Diabetes Genetics Consortium –T1DGC–, the Wellcome Trust Case Control Consorti-um –WTCCC– and The Genetics Association Informa-tion Network –GAIN–.
Finally, new analytical tools have had to be developed in order to tackle the vast amounts of information delivered by high through-put genotyping technologies. Both link-age and association studies become more complex with increasing number of genes being simultaneously in-cluded. The risk of false positive results has to be ac-counted for, interaction analyses are necessary to eluci-date combined genetic effects, and new tools for analysis are in continuous development.19-21
Most established risk genesMajor Histocompatibility ComplexThe genetic region encoding the human MHC, HLA, also designated as IDDM1, is by far the most solidly estab-
Table 1. Risk of T1D for a given individual according to the family member affected18,170-172
Relative risk Absolute risk (%)
No family history 1 0,4
Mother 2.5-5 1-2
Father 12.5-15 5-6
Sibling 15-22.5 6-9
One sibling + one parent 62,5 25
HLA-identical sibling 50 20
Monozygotic twin 75-175 30-70
Image KeyGenome Wilde Associated Region Candidate Region
UnnamedChr1
IDDM7
IDDM12
IDDM13
IDDM10IDDM17
IDDM6
IDDM4
IDDM2
IDDM9 IDDM18
IDDM11
IDDM1IDDM15IDDM5IDDM8
IDDM3UnnamedChr16
Chr1 1p13 Chr2
Chr9
2q24
2q33
Chr10 10p15
Chr3
Chr11
Chr4 4q27
Chr1211p15
Chr5 Chr6 6p216p21
12q13
12q24
Chr13 Chr14
Chr7
Chr15
Chr8
Chr16 16p13
ChrYChrXChr22Chr21Chr20Chr19Chr18Chr17 18p11
18p22
Figure 1. Genomic regions linked or associated with type 1 diabetes. With permission from www.t1dbase.org

RevisiónGenetics of type 1 diabetes. A.M. Wägner, et al.
177
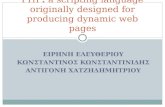
lished risk locus for T1D.22-24 It is located on the short arm of chromosome 6 (6p21.3), a dense region of highly polymorphic genes extending for 3.5 Mb. The classical class I HLA loci (telomeric) comprise HLA-A, -B, and -C, and class II (centromeric) comprise HLA-DR (DRA, DRB), -DQ (DQA, DQB) and -DP (DPA, DPB). The class III HLA region (located between class I and class II) includes the complement genes C2, C4, Bf, heat shock proteins genes (HSP70), tumour necrosis factor genes (TNF), 21-hydroxylase (21-OH) and others (Þ gure 2).
HLA accounts for up to 50% of the genetic risk,25 with major effects attributed to certain DR and DQ genes. However, due to high linkage disequilibrium in the re-gion (DR and DQ alleles tend to be inherited together) it is difÞ cult to determine those responsible for the risk. In-deed, associations of HLA alleles with T1D should be considered haplotype speciÞ c rather than allele speciÞ c. A recent meta-analysis of 38 studies conÞ rmed that hap-lotypes comprised of DRB1*0401, *0402 or *0405 and DQB1*0301 (DR4-DQ8) were associated with the high-est risk of T1D, followed by DRB1*0301 DQB1*0200 (DR3-DQ2) and DRB1*0404 DQB1*0302. The highest risk of T1D is given by the combination of DR3 and
DR4 in one genotype. The “neutral” category of haplo-types includes DRB1*0800 DQB1*0402, DRB1*0901 DQB1*0303 (DR9) and DRB1*0100 DQB1*0501 (DR1) and the most protective includes DRB1*1400 DQB1*0503 and DRB1*1500 DQB1*0602 (DR2).26 Results from the T1DGC expand these haplotypes to in-clude DQA1, as well as DRB1 and DQB127 (table 2). Their results also indicate that the risk associated with certain HLA haplotypes can be inß uenced by the geno-typic context, as exempliÞ ed by the high risk conferred by the trans-complementing DQ heterodimer encoded by the DQA*0501 allele on DR3 and the DQB1*0302 on some DR4 haplotypes.27
In Spain, unlike in other European populations, DR3 seems to confer a higher risk of T1D than DR4 accord-ing to most,28,29 albeit not all of the studies.7 These Þ nd-ings may be due to the particularly high-risk haplotypes associated with DR3 in Spain.28,30
Although DR and DQ alleles confer most of the genetic risk for T1D, class I alleles and maybe other loci within the MHC region are also important in the development of the disease. Further genotyping of class I alleles in
Major Histocompatibility Complex (6p21.3)
0301040504020401
02000301
Alleles
Genes
Telomere Centromere
A C B
MIC
A
TNF
HSP7
0
C4A
CYP2
1B
DRA
DRB1
DQA1
DQB1
TAP2
LAP7
TAP1
LMP2
DPA1
DPB1
Frequentrecombination
Frequentrecombination
Inrequentrecombination
4000
kbp
2000
kbp
1000
kbp
0kbp
Class I Class III Class II
MHC
6p21
.3
Chr6
alleles + alleles haplotypesDRB1 *0401 DQB1 *0301
*0402 DR4-DQ8*0405
DRB1 *0301 DQB1 *0200 DR3-DQ2}}
Figure 2. Description of the MHC region on chromosome 6

Av Diabetol. 2009;25:175-86
178
carriers of high-risk class II HLA haplotypes has given further insight into this matter.31,32 Siblings of patients with T1D, identical for their DR3/DR4-DQ8 genotypes, who share both HLA haplotypes (deÞ ned by HLA A and B, too) with the proband, have a 55% risk of developing T1D by the age of 12 (vs 5% of those sharing 1 or no haplotype).32 Furthermore, the remarkably conserved HLA A1-B8-DR3 haplotype33 seems to reduce the risk conferred by DR3-DQ2.34 Several other reports support an effect of HLA class I genes on disease susceptibility, in particular the HLA-A*2401, *0101 and *0302 and HLA-B*39 alleles.34-38 A highly conserved haplotype (B18 AH 18.2), particularly prevalent in the Spanish population, modulates the risk conferred by the DR3-DQ2 alleles. In fact, markers included in the HLA class III region (BAT-2*2 and TNFa2bI) have been found to predict risk in carriers of DR3-DQ2,30 though it is uncer-tain whether this effect persists after accounting for class I genes. In addition, a recent report from the T1DGC MCH Þ ne-mapping project identiÞ es additional risk sin-gle-nucleotide polymorphisms (SNPs) in the vicinity of HLA-G, COL11A2 and RING1.39 Other genes within the MHC region that have been reported to be associated with T1D include MIC-A40 and ITP3,41 but the results have not been replicated when LD with other class I and class II genes has been taken into account.42,43
Finally, a new locus telomeric to MHC (UBD/MAS1L) has shown to predict development of type 1 diabetes in-
dependently of class I and class II genes.44 Replication in other populations, as well as functional studies of the candidate genes should provide information about their role in the pathogenesis of the disease.
Non-MHC genesAlthough HLA is responsible for up to 50% of the genet-ic risk of T1D, other genes are involved, too, albeit with a weaker effect (odds ratios in the 1.15-1.3 range). Most of these genes play important roles in immunity and many are not speciÞ c to T1D, but also inß uence risk for other autoimmune diseases (table 3).
INSThe insulin gene (INS), located on chromosome 11p15.5 (IDDM2), is expressed in β-cells and in the human thy-mus, an expression site likely to be involved in immune tolerance. Two recent studies conÞ rmed that insulin is a major and primary target for autoreactive T-cells both in humans with T1D and in NOD mice.45,46 The susceptibil-ity locus IDDM2 maps to a minisatellite composed of a variable number of tandem repeat (VNTR) polymor-phism situated 0.5 kb upstream of INS, in the promoter region of the gene.47 In Caucasians, the main classes of VNTR region minisatellites are named VNTR I (26-63 repeating units) and VNTR III (140-210 units) alleles,48 where the former is associated with the highest risk of T1D,49,50 Although the precise function of the VNTR is still uncertain, the feature of the promoter region of INS may inß uence the binding of the AIRE transcription fac-tor. The latter regulates the expression of self antigens51 and controls the thymic expression of insulin and the de-letion of autoreactive T-cells during negative selection. The development of immune tolerance to insulin may be reduced through reduction of insulin transcription in thymic medullary epithelial cells.23,52 Indeed, the level of insulin expression in the human thymus correlates with the VNTR polymorphism, which in turn correlates with diabetes susceptibility.53,54 Recent studies of the INS lo-cus showed that the SNPs -2221MspI, -23HphI (A/T) and +1140 (A/C) confer the highest susceptibility to T1D. Because of their strong linkage disequilibrium with the VNTR, these polymorphism can even be used as markers of the latter.49,55-57
CTLA4The cytotoxic T lymphocyte antigen-4 (CTLA4) plays an important role in immune response regulation and is strongly associated with autoimmune diseases.58,59 This
Table 2. HLA class II haplotypes conferring the highest and the lowest risk of type 1 diabetes
Haplotype Risk of T1D (odds ratio)
High risk
DRB1*0405 DQA1*0301 DQB1*0302 (DR4) 11.37
DRB1*0401 DQA1*0301 DQB1*0302 (DR4) 8.39
DRB1*0301 DQA1*0501 DQB1*0201 (DR3) 3.64
DRB1*0402 DQA1*0301 DQB1*0302 (DR4) 3.63
DRB1*0801 DQA1*0401 DQB1*0402 (DR8) 1.59
Protection
DRB1*0701 DQA1*0201 DQB1*0303 (DR7) 0.02
DRB1*1401 DQA1*0101 DQB1*0503 (DR6) 0.02
DRB1*1501 DQA1*0102 DQB1*0602 (DR2) 0.03
DRB1*1104 DQA1*0501 DQB1*0301 (DR11) 0.07
DRB1*1303 DQA1*0501 DQB1*0301 0.08
Based on Erlich et al.27

RevisiónGenetics of type 1 diabetes. A.M. Wägner, et al.
179
CD28 homologue is mapped to the genetic region of the human IDDM12 locus on chromosome 2q3160 and its ex-clusive expression on activated CD4+ and CD8+ T-cells carrying CD2861 in mice seems to be controlled by the Foxp3 gene.62-64 CTLA4 appears to attenuate immune re-sponses by several mechanisms. As a negative regulator of T-cell activation, CTLA4 inhibits T-cell co-stimula-tion through intercellular interaction, competing for CD28 ligands (CD80/CD86) that are expressed on the surface of antigen presenting cells (APCs). Unlike CD28, which contributes to T-cell activation and maintenance of T-cell response (two signal hypothesis),65,66 CTLA4 restricts the initiation and progression of T-cell immuni-ty.67-69 It also inhibits T-cell activation by different intra-cellular signalling pathways,70,71 mediates apoptosis of activated human T lymphocytes in an antigen-restricted way72,73 and has an effect on the suppressive activity of regulatory T-cells (Tregs).74-78 The latter are important for maintenance of self-tolerance and immune homeos-tasis in the absence of exogenous antigens (Ag) and for control of Ag-speciÞ c responses.79 SpeciÞ c deÞ ciency of CTLA4 in Tregs in knock-out mice impairs suppressive function of Tregs and results in spontaneous develop-ment of systemic lymphoproliferation and fatal T-cell-
mediated autoimmune disease with multiorgan lym-phocytic inÞ ltration and tissue destruction.58,80,81
The T1D-associated CTLA4 haplotype contains several polymorphisms in tight linkage disequilibrium (LD), any one of which or a combination thereof could determine the functional effect. The SNP +6230G>A (CT60 rs30807243), located in the 3’ ß anking region of CTLA4, has been associated with splicing or altered levels of steady state CTLA4 mRNA.59,60 However, recent re-sults82,83 deny the effect of this SNP on modulation of steady-state mRNA of any known CTLA4 isoform but do not rule out its potential role in the development of T1D. Promoter polymorphisms -319C>T and -1661A>G (the latter in Moroccan and Indian population) possibly con-tribute to T1D through transcriptional effects on expres-sion,60,84,85 and SNP +49A>G on exon 1 of CTLA486 causes a change in the signal peptide, resulting in less CTLA4 at the cell surface. This explains the reduced in-hibitory function of CTLA4 reported in individuals with the +49G allele and is associated with reduced control of T-cell proliferation.87,88 Both the CD28 and CTLA4 path-ways are targets for current immunomodulatory thera-pies.89
Table 3. Summary of genes associated with the risk of type 1 diabetes
Gene/region (IDDM)
Reference Location Functional studies
Role Causal variants Association to other AID
HLA (IDDM1) 173,174 6p21.3 Yes Antigen presentation Class II, Class I and others Yes
INS (IDDM2) 48,49,53 11p15.5 Yes Insulin gene VNTR I/III No
CTLA4 (IDDM12) 59,175 2q31 Yes Regulator of T-cell activation -319C>T, +49A>G, +6230G>A (CT60) Yes
PTPN22 90,176 1p13 Yes Inhibits T-cell receptor signalling Arg620Trp (+1 858C>T) Yes
IL2RA (IDDM10) 102,103 10p15-p14 Yes α-chain of IL-2 receptor CD25 rs706778 (A/G), rs3118470 (C/T), ss52580101, rs11594656
Yes
SUMO4 (IDDM5) 136 6p25 Yes Inhibits NFκB Met55Val (163A>G) Yes
VDR 122,123 12q13 Yes Vitamin D receptor. It mediates Class II MHC down-regulation and IL12 inhibition
FokI (ATG>ACG) Yes
IFIH1 (IDDM19) (mda-5 or Helicard)
138-140 2q24 Yes Is involved in antiviral immune response
rs13422767, rs2111485, rs1990760, (A946T) rs3747517
Controversial
KIAA0350(CLEC16A)
146,177 16p13 No Encodes a C-type lectin rs2903692, rs725613, rs17673553, rs887864
Yes
PTPN2 144,157 18p11 No encodes a T-cell protein tyrosine phosphatase
rs1893217, rs478582 ?
UBASH3A (TULA, CLIP4, STS-2)
22 21q22.3 No cellular regulator, may be involved in maintenance of immunological tolerance178
rs876498 ?
AID: autoimmune diseases. VNTR: variable number of tandem repeats. ?: not known at the time of the review.

Av Diabetol. 2009;25:175-86
180
PTPN22Similar to CTLA4, PTPN22 (protein tyrosine phosphatase non-receptor type 22) is a diabetes susceptibility locus that is shared by several autoimmune diseases.90,91 It is lo-cated on chromosome 1p13 and encodes a lymphoid pro-tein tyrosine kinase (Lyp). Lyp is expressed in lymphoid T-cells, where it modulates the activation of protein ki-nases involved in early T-cell receptor (TCR) mediated signalling events,92 acting as a negative regulator of TCR signalling.92-94 The Arg620Trp (1858C/T) SNP in PTPN22 appears to promote autoimmunity in multiple ways, though there is only limited data regarding the mecha-nism by which variations in this gene contribute to the pathogenesis of T1D and how they affect immune func-tion in humans. The Arg620Trp variant has been reported to be associated with the development of insulin autoan-tibodies (in contrast to GAD and IA-2 antibody levels, which were not signiÞ cantly inß uenced by this polymor-phism) and an accelerated progression of the autoimmune process in T1D.95 According to two studies,93,96 the Ar-g620Trp variant causes a gain-of-inhibitory function that leads to enhanced suppression of TCR signal transduc-tion, a profound defect in T-cell responsiveness to antigen stimulation and decreased interleukin 2 (IL-2) secretion in T-cells. IL-2 is mainly produced by activated T-cells, promoting their proliferation and expansion.97 Homozy-gosity for the Arg620Trp variant is associated with reduced CD4+T-cell and B-cell activation and a shift in the mem-ory T- and B-cell populations to an increase in circulating memory T-cells and fewer and less effective memory B-cells.94,90 Lower T-cell signalling may allow the escape of self-reactive T-cells from thymic deletion and lead to im-paired self tolerance and reduced Treg development,96,98 and cause autoimmunity.52 There have been attempts to assess whether the SNPArg620Trp is the sole T1D suscep-tibility variant in PTPN22 and, although it seems to be the major risk variant for T1D in this chromosomic re-gion in European populations, the possibility still remains that a yet unidentiÞ ed variant could have a role in suscep-tibility to the disease.99-101
IL-2RAA polymorphism in Interleukin-2 receptor (IL-2RA), lo-cated on chromosome 10p15-p14,102 has recently shown an association with risk of T1D. IL-2RA encodes the α-chain of the high-afÞ nity heterodimeric IL-2 cytokine re-ceptor (CD25), highly expressed by activated Tregs.103,104 Genetic evidence also suggests a crucial role for IL-2 in T1D.102,103 Located on chromosome 4q27, IL-2 plays a
critical role in programming T-cells for activation-induced cell death and interferes with immune regulation.52 IL-2 or IL-2RA knock-out mice completely lack Tregs and suffer from a lymphoproliferative syndrome and spontaneous autoimmune disease.105 The association of IL-2 and IL-2RA to T1D is probably due to reduced proliferation of a variety of lymphocytes, including Tregs, whose depletion and altered function directly contribute to T1D pathogen-esis.106 Still, the precise role by which IL-2RA/IL-2 are in-volved in T1D susceptibility needs to be evaluated.
VDREpidemiological studies show differences in T1D inci-dence which are associated with geographical latitude and sun exposure107 and vitamin D intake before108 and during infancy109-112 seems to protect against the disease. In vitro, vitamin D suppresses the antigen-presenting ca-pacity of T-cells and dendritic cells.113 In fact, down-reg-ulation of MHC class II molecules and adhesion mole-cules114 and inhibition of IL-12 is seen after treatment with vitamin D or its analogues.115-119 The relationship between Vitamin D and autoimmune diseases has been thoroughly reviewed elsewhere.120,121
Vitamin D actions are mediated by the highly polymor-phic vitamin D receptor115 which is encoded by VDR, lo-cated on 12q12-14.122 The FokI polymorphism in exon 2 leads to a shorter and more active form of VDR protein, and displays a different distribution (P 0.0049) in sub-jects with T1D and controls.112 However, genetic studies are somewhat contradictory, with some showing an asso-ciation between VDR variations and T1D,122-131 whereas others do not.132-134 Population heterogeneity and differ-ences in exposure to ultraviolet radiation may account for these differences. A recent meta-analysis of 16 stud-ies in 19 regions showed an interaction with ambient winter ultraviolet radiation and association between cer-tain VDR alleles and T1D.135 This study supports the role of vitamin D in the development of T1D, though further studies combining genetic data and information on expo-sure to ultraviolet radiation and vitamin D status should further clarify this matter.
SUMO4The association of the small ubiquitin-like modifier (SUMO) gene, SUMO4, located in the IDDM5 locus on chromosome 6q25, has been conÞ rmed in Asian popula-tions despite controversial observations in Caucasians. A single amino acid substitution (163A>G, Met55Val) at an

RevisiónGenetics of type 1 diabetes. A.M. Wägner, et al.
181
evolutionarily conserved residue of SUMO4 enhances NFκB transcriptional activity and IL-12B expression and is associated with increased risk for T1D.136,137
Other genes and regionsInterferon induced with helicase C domain 1 gene (IFIH1), involved in anti-viral response, is the most plau-sible risk gene for T1D in a linkage disequilibrium block on chromosome 2q24 (IDDM19),138-140 though its asso-ciation with other autoimmune diseases, like Graves’ disease141,142 and multiple sclerosis,143 is controversial.
A number of other associations with type 1 diabetes have been identiÞ ed and replicated for SNPs in two regions on chromosome 12, 12q24 near C12orf30 and 12q13 near erythroblastic leukemia viral oncogene homolog 3 (ERBB3), a region on 16p13 near C-type lectin domain family 16, member A (CLEC16A/KIAA0350), a region on 18p11 near protein tyrosine phosphatase, nonreceptor type 2 (PTPN2), a region on 2q12-22 encoding inter-leukin 1 receptor 1 and a region on 21q22.3 in the ubiq-uitin associated and SH3 domain containing, A (UBA-SH3A, STS/TULA family) locus.22,112,144-148 Many other chromosomic regions are likely to be discovered during ongoing analysis of the data obtained from the WTCCC, T1DGC and GAIN consortia. Detailed and updated in-formation about T1D associated loci can be found in T1DBase (www.t1dbase.org ).
Additional candidate genesA different approach to identifying new genes involved in T1D consists of trying to replicate results found in closely related diseases, such as T2D, autoimmune dia-betes presenting as part of a syndrome and other autoim-mune diseases.
Several attempts have been made at associating T2D genes to T1D, but most have been negative.149,150 Patients with autoimmune diabetes diagnosed after the age of 35 and with a clinical presentation more close to T2D (LA-DA) are an exception. These patients have features of both type 1 and type 2 diabetes, clinically as well as ge-netically.151-153
Autoimmune diabetes is also a minor component of se-vere monogenic syndromes such as APS-I or IPEX. APS1 (autoimmune polyglandular syndrome type 1)
or autoimmune polyendocrinopathy candidiasis ectoder-mal dystrophy (APECED)154-156 is a recessive disease caused by mutations of the AIRE gene,157 located on 21q22,158 which encodes a transcription factor with an important role in promoting tolerance and preventing au-toimmunity.159-161 Children with the IPEX syndrome (immune dysregulation, polyendocrinopathy, enteropa-thy, X-linked), also termed the XPID syndrome (X-linked Polyendocrinopathy, Immune Dysfunction and Diarrhoea), present with severe multiorgan autoimmuni-ty (including diabetes) and lymphoproliferation which may lead to death in the Þ rst 2 years of life,162 caused by regulatory T-cell failure due to mutations in FOXP3, lo-cated on Xq11.23-Xq13.3.163-165
PerspectivesAt present, the clinically useful application of genetics in type 1 diabetes is limited to identifying monogenic forms of diabetes where an atypical clinical presentation of T1D (eg: in the Þ rst 6 months of life, with a strong fam-ily history of diabetes or as part of a distinct syndrome) suggests a monogenic etiology of the disease and where treatments other than insulin may be considered. In ad-dition, identiÞ cation of individuals at a high risk of de-veloping T1D may be of clinical interest in the future, if interventions that are presently being tested in clinical trials166-168 prove to be safe and effective.
HLA genotyping is a complex process, due to the highly polymorphic nature of the genetic region. Taking advan-tage of the high linkage disequilibrium in the HLA re-gion, high-risk HLA can be detected by simply analys-ing a few SNPs169 and thus, high-risk individuals, candidates for intervention, could be easily identiÞ ed. The already established markers of disease plus the dis-covery of additional ones may allow further deÞ nition in risk assessment. Nevertheless, for the time being, genet-ic counselling to families of patients with T1D cannot be accompanied by preventive measures.
ConclusionsT1D is a complex autoimmune disease with a proved ge-netic background. Most (around 50%) of its genetic risk is accounted for by class I and class II HLA haplotypes, although other genes with a smaller effect are also in-volved. Most of the known risk genes for T1D play a role in immunity, mostly through T-cell regulation (CT-

Av Diabetol. 2009;25:175-86
182
LA4, PTPN22, IL-2RA) and cytokine production or mod-ulation (VDR, SUMO4). The insulin gene (INS) repre-sents and exception to this, and is probably the only gene speciÞ cally associated with T1D and not with other au-toimmune diseases.
Ongoing genome-wide association studies are providing evidence of multiple known and previously unknown risk genes. New analytical tools are continuously being developed to handle the vast amounts of data produced, as well as to account for multiple comparisons and as-sess combined effects such as gene-gene and gene-envi-ronment interactions. ■
Acknowledgements:JCW is being supported by a research grant from the EFSD/ JDRF/ Novo Nordisk Programme 2008.
Potential conß icts of interestThe authors are not aware of any conß icts of interest related to the subject of the review.
References1. Robles DT, Eisenbarth GS. Type 1A diabetes induced by infection and
immunization. J Autoimmun. 2001;16:355-62.2. Svensson J, Carstensen B, Molbak A, Christau B, Mortensen HB, Nerup J,
et al. Increased risk of childhood type 1 diabetes in children born after 1985. Diabetes Care. 2002;25:2197-201.
3. Gottlieb PA, Eisenbarth GS. Insulin-specifi c tolerance in diabetes. Clin Immunol. 2002;102:2-11.
4. Harjutsalo V, Sjoberg L, Tuomilehto J. Time trends in the incidence of type 1 diabetes in Finnish children:a cohort study. Lancet. 2008;371:1777-82.
5. Soltesz G, Patterson CC, Dahlquist G. Worldwide childhood type 1 diabetes incidence--what can we learn from epidemiology? Pediatr Diabetes. 2007;8 Suppl 6:6-14.
6. Chueca M, Oyarzabal M, Reparaz F, Garagorri JM, Sola A. Incidence of type I diabetes mellitus in Navarre, Spain (1975-91). Acta Paediatr. 1997;86:632-7.
7. Escribano-de-Diego J, Sanchez-Velasco P, Luzuriaga C, Ocejo-Vinyals JG, Paz-Miguel JE, Leyva-Cobian F. HLA class II immunogenetics and incidence of insulin-dependent diabetes mellitus in the population of Cantabria (Northern Spain). Hum Immunol. 1999;60:990-1000.
8. Lora-Gomez RE, Morales-Perez FM, Arroyo-Diez FJ, Barquero-Romero J. Incidence of Type 1 diabetes in children in Caceres, Spain, during 1988-1999. Diabetes Res Clin Pract. 2005;69:169-74.
9. Morales-Perez FM, Barquero-Romero J, Perez-Miranda M. Incidence of type I diabetes among children and young adults (0-29 years) in the province of Badajoz, Spain during 1992 to 1996. Acta Paediatr. 2000;89:101-4.
10. Ruiz-Ramos M, Escolar-Pujolar A, Mayoral-Sanchez E, Corral-San Laureano F, Fernandez-Fernandezc I. [Mellitus diabetes in Spain:death rates, prevalence, impact, costs and inequalities.]. Gac Sanit. 2006;20 Suppl 1:15-24.
11. Soria J, Garagorri JM, Rodriguez M, Rodriguez G, Larrad L, Elizalde M. Epidemiology and genetic risk of type 1 diabetes among children in Aragon community, Spain. Diabetes Res Clin Pract. 2008;79:112-6.
12. Lopez Siguero JP, Martinez-Aedo Ollero MJ, Moreno Molina JA, Lora Espinosa A, Martinez Valverde A. [The development of the incidence of diabetes mellitus I in children 0 to 14 years of age in Malaga (1982-1993)]. An Esp Pediatr. 1997;47:17-22.
13. Cepedano Dans A, Barreiro Conde J, Pombo Arias M. [Incidence and clinical manifestations at onset of type 1 diabetes mellitus in Galicia (Spain):2001-2002]. An Pediatr (Barc). 2005;62:123-7.
14. Bahillo MP, Hermoso F, Ochoa C, Garcia-Fernandez JA, Rodrigo J, Marugan JM, et al. Incidence and prevalence of type 1 diabetes in children aged <15 yr in Castilla-Leon (Spain). Pediatr Diabetes. 2007;8:369-73.
15. Giralt Muina P, Santillana Ferrer L, Madrigal Barchino D, Merlo Garrido A, Toledo De La Torre B, Anaya Barea F. [Incidence of diabetes mellitus and prevalence of type 1A diabetes mellitus in children younger than 16 years old from the province of Ciudad Real]. An Esp Pediatr. 2001;55:213-8.
16. Belinchón BM, Hernández Bayo JA, Cabrera Rodríguez R. Incidence of childhood type 1 diabetes (0-14yrs) in La Palmas Island. Diabetologia. 2008;51(Suppl 1).
17. Carrillo Dominguez A. [Incidence of type 1 diabetes mellitus in the Canary Islands (1995-1996). Epidemiologic Group of the Canary Society of Endocrinology and Nutrition]. Rev Clin Esp. 2000;200:257-60.
18. Lorenzen T, Pociot F, Hougaard P, Nerup J. Long-term risk of IDDM in fi rst-degree relatives of patients with IDDM. Diabetologia. 1994;37:321-7.
19. Bergholdt R, Storling ZM, Lage K, Karlberg EO, Olason PI, Aalund M, et al. Integrative analysis for fi nding genes and networks involved in diabetes and other complex diseases. Genome Biol. 2007;8:R253.
20. Pociot F, Karlsen AE, Pedersen CB, Aalund M, Nerup J. Novel analytical methods applied to type 1 diabetes genome-scan data. Am J Hum Genet. 2004;74:647-60.
21. Brorsson CA, Hansen NT, Lage K, Bergholdt R, Brunak S, Pociot F. Identifi cation of type 1 diabetes genes in the MHC region by a novel approach combining genetic data with information on functional pathways. Diabetologia. 2008;51(Suppl. 1).
22. Concannon P, Onengut-Gumuscu S, Todd JA, Smyth DJ, Pociot F, Bergholdt R, et al. A human type 1 diabetes susceptibility locus maps to chromosome 21q22.3. Diabetes. 2008;57:2858-61.
23. Kantarova D, Buc M. Genetic susceptibility to type 1 diabetes mellitus in humans. Physiol Res. 2007;56:255-66.
24. Steck AK, Pugliese A, Eisenbarth GS, Type 1 Diabetes:Cellular, Molecular & Clinical Immunology, Online Edition Version 3.0, G.S. Eisenbarth, Editor. 2008.
25. Jones MA, Hislop AD, Snaith JS. Synthesis and biological evaluation of two chemically modifi ed peptide epitopes for the class I MHC protein HLA-B*2705. Org Biomol Chem. 2006;4:3769-77.
Practical considerations
• Genetics can improve risk prediction in type 1 diabetes.
• HLA haplotypes can explain the main part of ge-netic risk in type 1 diabetes.
• Due to the lack of effi cient intervention protocols/measures, routine genotyping of type 1 diabetes patients and relatives is not recommended at present.

RevisiónGenetics of type 1 diabetes. A.M. Wägner, et al.
183
26. Thomson G, Valdes AM, Noble JA, Kockum I, Grote MN, Najman J, et al. Relative predispositional effects of HLA class II DRB1-DQB1 haplotypes and genotypes on type 1 diabetes:a meta-analysis. Tissue Antigens. 2007;70:110-27.
27. Erlich H, Valdes AM, Noble J, Carlson JA, Varney M, Concannon P, et al. HLA DR-DQ haplotypes and genotypes and type 1 diabetes risk:analysis of the type 1 diabetes genetics consortium families. Diabetes. 2008;57:1084-92.
28. Vicario JL, Martinez-Laso J, Corell A, Martin-Villa JM, Morales P, Lledo G, et al. Comparison between HLA-DRB and DQ DNA sequences and classic serological markers as type 1 (insulin-dependent) diabetes mellitus predictive risk markers in the Spanish population. Diabetologia. 1992;35:475-81.
29. Goday A, Motana E, Ercilla G, Fernandez J, Gomis R, Vilardell E. HLA antigens in Spanish type 1 diabetic population. Correlations with clinical, biological and autoimmune markers. Acta Diabetol Lat. 1990;27:215-22.
30. Urcelay E, Santiago JL, de la Calle H, Martinez A, Mendez J, Ibarra JM, et al. Type 1 diabetes in the Spanish population:additional factors to class II HLA-DR3 and -DR4. BMC Genomics. 2005;6:56.
31. Robinson BH, Dosch HM, Martin JM, Akerblom HK, Savilahti E, Knip M, et al. A model for the involvement of MHC class II proteins in the development of type 1 (insulin-dependent) diabetes mellitus in response to bovine serum albumin peptides. Diabetologia. 1993;36:364-8.
32. Aly TA, Ide A, Jahromi MM, Barker JM, Fernando MS, Babu SR, et al. Extreme genetic risk for type 1A diabetes. Proc Natl Acad Sci U S A. 2006;103:14074-9.
33. Aly TA, Eller E, Ide A, Gowan K, Babu SR, Erlich HA, et al. Multi-SNP analysis of MHC region:remarkable conservation of HLA-A1-B8-DR3 haplotype. Diabetes. 2006;55:1265-9.
34. Noble JA, Martin A, Valdes AM, Lane JA, Galgani A, Petrone A, et al. Type 1 diabetes risk for human leukocyte antigen (HLA)-DR3 haplotypes depends on genotypic context:association of DPB1 and HLA class I loci among DR3- and DR4-matched Italian patients and controls. Hum Immunol. 2008;69:291-300.
35. Chuang LM, Jou TS, Wu HP, Tai TY, Lin BJ. A rapid method to study heat shock protein 70-2 gene polymorphism in insulin-dependent diabetes mellitus. Pancreas. 1996;13:268-72.
36. Chuang LM, Wu HP, Tsai WY, Lai CS, Tai TY, Lin BJ. Mitochondrial gene mutations in patients with insulin-dependent diabetes mellitus in Taiwan. Pancreas. 1996;12:243-7.
37. Karjalainen J, Salmela P, Ilonen J, Surcel HM, Knip M. A comparison of childhood and adult type I diabetes mellitus. N Engl J Med. 1989;320:881-6.
38. Nejentsev S, Howson JM, Walker NM, Szeszko J, Field SF, Stevens HE, et al. Localization of type 1 diabetes susceptibility to the MHC class I genes HLA-B and HLA-A. Nature. 2007;450:887-92.
39. Eike MC, Becker T, Humphreys K, Olsson M, Lie BA. Conditional analyses on the T1DGC MHC dataset:novel associations with type 1 diabetes around HLA-G and confi rmation of HLA-B. Genes Immun. 2008.
40. Bilbao JR, Martin-Pagola A, Calvo B, Perez de Nanclares G, Gepv N, Castano L. Contribution of MIC-A polymorphism to type 1 diabetes mellitus in Basques. Ann N Y Acad Sci. 2002;958:321-4.
41. Roach JC, Deutsch K, Li S, Siegel AF, Bekris LM, Einhaus DC, et al. Genetic mapping at 3-kilobase resolution reveals inositol 1,4,5-triphosphate receptor 3 as a risk factor for type 1 diabetes in Sweden. Am J Hum Genet. 2006;79:614-27.
42. Field SF, Nejentsev S, Walker NM, Howson JM, Godfrey LM, Jolley JD, et al. Sequencing-based genotyping and association analysis of the MICA and MICB genes in type 1 diabetes. Diabetes. 2008;57:1753-6.
43. Qu HQ, Marchand L, Szymborski A, Grabs R, Polychronakos C. The association between type 1 diabetes and the ITPR3 gene polymorphism due to linkage disequilibrium with HLA class II. Genes Immun. 2008;9:264-6.
44. Aly TA, Baschal EE, Jahromi MM, Fernando MS, Babu SR, Fingerlin TE, et al. Analysis of single nucleotide polymorphisms identifi es major type 1A
diabetes locus telomeric of the major histocompatibility complex. Diabetes. 2008;57:770-6.
45. Kent SC, Chen Y, Bregoli L, Clemmings SM, Kenyon NS, Ricordi C, et al. Expanded T cells from pancreatic lymph nodes of type 1 diabetic subjects recognize an insulin epitope. Nature. 2005;435:224-8.
46. Nakayama M, Abiru N, Moriyama H, Babaya N, Liu E, Miao D, et al. Prime role for an insulin epitope in the development of type 1 diabetes in NOD mice. Nature. 2005;435:220-3.
47. Pugliese A, Miceli D. The insulin gene in diabetes. Diabetes Metab Res Rev. 2002;18:13-25.
48. Bell GI, Horita S, Karam JH. A polymorphic locus near the human insulin gene is associated with insulin-dependent diabetes mellitus. Diabetes. 1984;33:176-83.
49. Barratt BJ, Payne F, Lowe CE, Hermann R, Healy BC, Harold D, et al. Remapping the insulin gene/IDDM2 locus in type 1 diabetes. Diabetes. 2004;53:1884-9.
50. Bennett ST, Lucassen AM, Gough SC, Powell EE, Undlien DE, Pritchard LE, et al. Susceptibility to human type 1 diabetes at IDDM2 is determined by tandem repeat variation at the insulin gene minisatellite locus. Nat Genet. 1995;9:284-92.
51. Cheng MH, Shum AK, Anderson MS. What’s new in the Aire? Trends Immunol. 2007;28:321-7.
52. Chentoufi AA, Binder NR, Berka N, Abunadi T, Polychronakos C. Advances in type I diabetes associated tolerance mechanisms. Scand J Immunol. 2008;68:1-11.
53. Pugliese A, Zeller M, Fernandez A, Jr., Zalcberg LJ, Bartlett RJ, Ricordi C, et al. The insulin gene is transcribed in the human thymus and transcription levels correlated with allelic variation at the INS VNTR-IDDM2 susceptibility locus for type 1 diabetes. Nat Genet. 1997;15:293-7.
54. Vafi adis P, Bennett ST, Todd JA, Nadeau J, Grabs R, Goodyer CG, et al. Insulin expression in human thymus is modulated by INS VNTR alleles at the IDDM2 locus. Nat Genet. 1997;15:289-92.
55. Awata T, Kawasaki E, Ikegami H, Kobayashi T, Maruyama T, Nakanishi K, et al. Insulin gene/IDDM2 locus in Japanese type 1 diabetes:contribution of class I alleles and infl uence of class I subdivision in susceptibility to type 1 diabetes. J Clin Endocrinol Metab. 2007;92:1791-5.
56. Ramos-Lopez E, Lange B, Kahles H, Willenberg HS, Meyer G, Penna-Martinez M, et al. Insulin gene polymorphisms in type 1 diabetes, Addison‘s disease and the polyglandular autoimmune syndrome type II. BMC Med Genet. 2008;9:65.
57. Haller K, Kisand K, Nemvalts V, Laine AP, Ilonen J, Uibo R. Type 1 diabetes is insulin -2221 MspI and CTLA-4 +49 A/G polymorphism dependent. Eur J Clin Invest. 2004;34:543-8.
58. Kristiansen OP, Larsen ZM, Pociot F. CTLA-4 in autoimmune diseases--a general susceptibility gene to autoimmunity? Genes Immun. 2000;1:170-84.
59. Ueda H, Howson JM, Esposito L, Heward J, Snook H, Chamberlain G, et al. Association of the T-cell regulatory gene CTLA4 with susceptibility to autoimmune disease. Nature. 2003;423:506-11.
60. Anjos SM, Tessier MC, Polychronakos C. Association of the cytotoxic T lymphocyte-associated antigen 4 gene with type 1 diabetes:evidence for independent effects of two polymorphisms on the same haplotype block. J Clin Endocrinol Metab. 2004;89:6257-65.
61. Lindsten T, Lee KP, Harris ES, Petryniak B, Craighead N, Reynolds PJ, et al. Characterization of CTLA-4 structure and expression on human T cells. J Immunol. 1993;151:3489-99.
62. Hori S, Nomura T, Sakaguchi S. Control of regulatory T cell development by the transcription factor Foxp3. Science. 2003;299:1057-61.
63. Ono M, Yaguchi H, Ohkura N, Kitabayashi I, Nagamura Y, Nomura T, et al. Foxp3 controls regulatory T-cell function by interacting with AML1/Runx1. Nature. 2007;446:685-9.
64. Wing K, Onishi Y, Prieto-Martin P, Yamaguchi T, Miyara M, Fehervari Z, et al. CTLA-4 control over Foxp3+ regulatory T cell function. Science. 2008;322:271-5.
65. Bretscher PA, Cohn M. Minimal model for the mechanism of antibody induction and paralysis by antigen. Nature. 1968;220:444-8.

Av Diabetol. 2009;25:175-86
184
66. Bluestone JA. New perspectives of CD28-B7-mediated T cell costimulation. Immunity. 1995;2:555-9.
67. Krummel MF, Allison JP. CTLA-4 engagement inhibits IL-2 accumulation and cell cycle progression upon activation of resting T cells. J Exp Med. 1996;183:2533-40.
68. Krummel MF, Sullivan TJ, Allison JP. Superantigen responses and co-stimulation:CD28 and CTLA-4 have opposing effects on T cell expansion in vitro and in vivo. Int Immunol. 1996;8:519-23.
69. Krummel MF, Allison JP. CD28 and CTLA-4 have opposing effects on the response of T cells to stimulation. J Exp Med. 1995;182:459-65.
70. Chuang E, Lee KM, Robbins MD, Duerr JM, Alegre ML, Hambor JE, et al. Regulation of cytotoxic T lymphocyte-associated molecule-4 by Src kinases. J Immunol. 1999;162:1270-7.
71. Parry RV, Chemnitz JM, Frauwirth KA, Lanfranco AR, Braunstein I, Kobayashi SV, et al. CTLA-4 and PD-1 receptors inhibit T-cell activation by distinct mechanisms. Mol Cell Biol. 2005;25:9543-53.
72. Gribben JG, Freeman GJ, Boussiotis VA, Rennert P, Jellis CL, Greenfi eld E, et al. CTLA4 mediates antigen-specifi c apoptosis of human T cells. Proc Natl Acad Sci U S A. 1995;92:811-5.
73. Noel PJ, Boise LH, Thompson CB. Regulation of T cell activation by CD28 and CTLA4. Adv Exp Med Biol. 1996;406:209-17.
74. Ziegler SF. FOXP3:of mice and men. Annu Rev Immunol. 2006;24:209-26.
75. Sakaguchi S. Naturally arising Foxp3-expressing CD25+CD4+ regulatory T cells in immunological tolerance to self and non-self. Nat Immunol. 2005;6:345-52.
76. Fontenot JD, Rudensky AY. A well adapted regulatory contrivance:regulatory T cell development and the forkhead family transcription factor Foxp3. Nat Immunol. 2005;6:331-7.
77. Jiang H, Chess L. Regulation of immune responses by T cells. N Engl J Med. 2006;354:1166-76.
78. Fontenot JD, Gavin MA, Rudensky AY. Foxp3 programs the development and function of CD4+CD25+ regulatory T cells. Nat Immunol. 2003;4:330-6.
79. Sakaguchi S, Sakaguchi N, Shimizu J, Yamazaki S, Sakihama T, Itoh M, et al. Immunologic tolerance maintained by CD25+ CD4+ regulatory T cells:their common role in controlling autoimmunity, tumor immunity, and transplantation tolerance. Immunol Rev. 2001;182:18-32.
80. Tivol EA, Borriello F, Schweitzer AN, Lynch WP, Bluestone JA, Sharpe AH. Loss of CTLA-4 leads to massive lymphoproliferation and fatal multiorgan tissue destruction, revealing a critical negative regulatory role of CTLA-4. Immunity. 1995;3:541-7.
81. Waterhouse P, Penninger JM, Timms E, Wakeham A, Shahinian A, Lee KP, et al. Lymphoproliferative disorders with early lethality in mice defi cient in Ctla-4. Science. 1995;270:985-8.
82. Anjos SM, Shao W, Marchand L, Polychronakos C. Allelic effects on gene regulation at the autoimmunity-predisposing CTLA4 locus:a re-evaluation of the 3’ +6230G>A polymorphism. Genes Immun. 2005;6:305-11.
83. Mayans S, Lackovic K, Nyholm C, Lindgren P, Ruikka K, Eliasson M, et al. CT60 genotype does not affect CTLA-4 isoform expression despite association to T1D and AITD in northern Sweden. BMC Med Genet. 2007;8:3.
84. Bouqbis L, Izaabel H, Akhayat O, Perez-Lezaun A, Calafell F, Bertranpetit J, et al. Association of the CTLA4 promoter region (-1661G allele) with type 1 diabetes in the South Moroccan population. Genes Immun. 2003;4:132-7.
85. Baniasadi V, Narain N, Goswami R, Das SN. Promoter region -318 C/ T and -1661 A/G CTLA-4 single nucleotide polymorphisms and type 1 diabetes in North Indians. Tissue Antigens. 2006;67:383-9.
86. Donner H, Rau H, Walfi sh PG, Braun J, Siegmund T, Finke R, et al. CTLA4 alanine-17 confers genetic susceptibility to Graves’ disease and to type 1 diabetes mellitus. J Clin Endocrinol Metab. 1997;82:143-6.
87. Kouki T, Sawai Y, Gardine CA, Fisfalen ME, Alegre ML, DeGroot LJ. CTLA-4 gene polymorphism at position 49 in exon 1 reduces the inhibitory function of CTLA-4 and contributes to the pathogenesis of Graves’ disease. J Immunol. 2000;165:6606-11.
88. Maurer M, Loserth S, Kolb-Maurer A, Ponath A, Wiese S, Kruse N, et al. A polymorphism in the human cytotoxic T-lymphocyte antigen 4 ( CTLA4) gene (exon 1 +49) alters T-cell activation. Immunogenetics. 2002;54:1-8.
89. Tang AL, Teijaro JR, Njau MN, Chandran SS, Azimzadeh A, Nadler SG, et al. CTLA4 expression is an indicator and regulator of steady-state CD4+ FoxP3+ T cell homeostasis. J Immunol. 2008;181:1806-13.
90. Bottini N, Musumeci L, Alonso A, Rahmouni S, Nika K, Rostamkhani M, et al. A functional variant of lymphoid tyrosine phosphatase is associated with type I diabetes. Nat Genet. 2004;36:337-8.
91. Onengut-Gumuscu S, Ewens KG, Spielman RS, Concannon P. A functional polymorphism (1858C/T) in the PTPN22 gene is linked and associated with type I diabetes in multiplex families. Genes Immun. 2004;5:678-80.
92. Cohen S, Dadi H, Shaoul E, Sharfe N, Roifman CM. Cloning and characterization of a lymphoid-specifi c, inducible human protein tyrosine phosphatase, Lyp. Blood. 1999;93:2013-24.
93. Vang T, Congia M, Macis MD, Musumeci L, Orru V, Zavattari P, et al. Autoimmune-associated lymphoid tyrosine phosphatase is a gain-of-function variant. Nat Genet. 2005;37:1317-9.
94. Rieck M, Arechiga A, Onengut-Gumuscu S, Greenbaum C, Concannon P, Buckner JH. Genetic variation in PTPN22 corresponds to altered function of T and B lymphocytes. J Immunol. 2007;179:4704-10.
95. Hermann R, Lipponen K, Kiviniemi M, Kakko T, Veijola R, Simell O, et al. Lymphoid tyrosine phosphatase (LYP/PTPN22) Arg620Trp variant regulates insulin autoimmunity and progression to type 1 diabetes. Diabetologia. 2006;49(6):1198-208.
96. Aarnisalo J, Treszl A, Svec P, Marttila J, Oling V, Simell O, et al. Reduced CD4+T cell activation in children with type 1 diabetes carrying the PTPN22/Lyp 620Trp variant. J Autoimmun. 2008;31:13-21.
97. Burchill MA, Yang J, Vang KB, Farrar MA. Interleukin-2 receptor signaling in regulatory T cell development and homeostasis. . Immunol Lett 2007;114:1-8.
98. Jacobson EM, Tomer Y. The CD40, CTLA-4, thyroglobulin, TSH receptor, and PTPN22 gene quintet and its contribution to thyroid autoimmunity:back to the future. J Autoimmun. 2007;28:85-98.
99. Onengut-Gumuscu S, Buckner JH, Concannon P. A haplotype-based analysis of the PTPN22 locus in type 1 diabetes. Diabetes. 2006;55:2883-9.
100. Smyth DJ, Cooper JD, Howson JM, Walker NM, Plagnol V, Stevens H, et al. PTPN22 Trp620 explains the association of chromosome 1p13 with type 1 diabetes and shows a statistical interaction with HLA class II genotypes. Diabetes. 2008;57:1730-7.
101. Cinek O, Hradsky O, Ahmedov G, Slavcev A, Kolouskova S, Kulich M, et al. No independent role of the -1123 G>C and+2740 A>G variants in the association of PTPN22 with type 1 diabetes and juvenile idiopathic arthritis in two Caucasian populations. Diabetes Res Clin Pract. 2007;76:297-303.
102. Vella A, Cooper JD, Lowe CE, Walker N, Nutland S, Widmer B, et al. Localization of a type 1 diabetes locus in the IL2RA/CD25 region by use of tag single-nucleotide polymorphisms. Am J Hum Genet. 2005;76:773-779.
103. Chistiakov DA, Voronova NV, Chistiakov PA. The crucial role of IL-2/IL-2RA-mediated immune regulation in the pathogenesis of type 1 diabetes, an evidence coming from genetic and animal model studies. Immunol Lett. 2008;118:1-5.
104. Lowe CE, Cooper JD, Brusko T, Walker NM, Smyth DJ, Bailey R, et al. Large-scale genetic fi ne mapping and genotype-phenotype associations implicate polymorphism in the IL2RA region in type 1 diabetes. Nat Genet. 2007;39:1074-82.
105. Schimpl A, Berberich I, Kneitz B, Kramer S, Santner-Nanan B, Wagner S, et al. IL-2 and autoimmune disease. Cytokine Growth Factor Rev. 2002;13:369-78.
106. Tree TI, Roep BO, Peakman M. A mini meta-analysis of studies on CD4+ CD25+ T cells in human type 1 diabetes:report of the Immunology of Diabetes Society T CellWorkshop. Ann NY Acad Sc 2006;1079:9-18.
107. Mathieu C, Gysemans C, Giulietti A, Bouillon R. Vitamin D and diabetes. Diabetologia. 2005;48:1247-57.

RevisiónGenetics of type 1 diabetes. A.M. Wägner, et al.
185
108. Fronczak CM, Baron AE, Chase HP, Ross C, Brady HL, Hoffman M, et al. In utero dietary exposures and risk of islet autoimmunity in children. Diabetes Care. 2003;26:3237-42.
109. Stene LC, Joner G. Use of cod liver oil during the fi rst year of life is associated with lower risk of childhood-onset type 1 diabetes:a large, population-based, case-control study. Am J Clin Nutr. 2003;78:1128-34.
110. Hypponen E, Laara E, Reunanen A, Jarvelin MR, Virtanen SM. Intake of vitamin D and risk of type 1 diabetes:a birth-cohort study. Lancet. 2001;358:1500-3.
111. EURODIAB. Vitamin D supplement in early childhood and risk for Type I (insulin-dependent) diabetes mellitus. The EURODIAB Substudy 2 Study Group. Diabetologia. 1999;42:51-4.
112. Zemunik T, Skrabic V, Boraska V, Diklic D, Terzic IM, Capkun V, et al. FokI polymorphism, vitamin D receptor, and interleukin-1 receptor haplotypes are associated with type 1 diabetes in the Dalmatian population. J Mol Diagn. 2005;7:600-4.
113. van Etten E, Decallonne B, Bouillon R, Mathieu C. NOD bone marrow-derived dendritic cells are modulated by analogs of 1,25-dihydroxyvitamin D3. J Steroid Biochem Mol Biol. 2004;89-90:457-9.
114. Griffi n MD, Lutz WH, Phan VA, Bachman LA, McKean DJ, Kumar R. Potent inhibition of dendritic cell differentiation and maturation by vitamin D analogs. Biochem Biophys Res Commun. 2000;270:701-8.
115. D’Ambrosio D, Cippitelli M, Cocciolo MG, Mazzeo D, Di Lucia P, Lang R, et al. Inhibition of IL-12 production by 1,25-dihydroxyvitamin D3. Involvement of NF-kappaB downregulation in transcriptional repression of the p40 gene. J Clin Invest. 1998;101:252-62.
116. Penna G, Adorini L. 1 Alpha,25-dihydroxyvitamin D3 inhibits differentiation, maturation, activation, and survival of dendritic cells leading to impaired alloreactive T cell activation. J Immunol. 2000;164:2405-11.
117. Overbergh L, Decallonne B, Valckx D, Verstuyf A, Depovere J, Laureys J, et al. Identifi cation and immune regulation of 25-hydroxyvitamin D-1-alpha-hydroxylase in murine macrophages. Clin Exp Immunol. 2000;120:139-46.
118. Boonstra A, Barrat FJ, Crain C, Heath VL, Savelkoul HF, O’Garra A. 1alpha,25-Dihydroxyvitamin d3 has a direct effect on naive CD4(+) T cells to enhance the development of Th2 cells. J Immunol. 2001;167:4974-80.
119. Gregori S, Giarratana N, Smiroldo S, Uskokovic M, Adorini L. A 1alpha,25-dihydroxyvitamin D(3) analog enhances regulatory T-cells and arrests autoimmune diabetes in NOD mice. Diabetes. 2002;51:1367-74.
120. Adorini L, Penna G. Control of autoimmune diseases by the vitamin D endocrine system. Nat Clin Pract Rheumatol. 2008;4:404-12.
121. Szodoray P, Nakken B, Gaal J, Jonsson R, Szegedi A, Zold E, et al. The complex role of vitamin D in autoimmune diseases. Scand J Immunol. 2008;68(3):261-9.
122. Pani MA, Knapp M, Donner H, Braun J, Baur MP, Usadel KH, et al. Vitamin D receptor allele combinations infl uence genetic susceptibility to type 1 diabetes in Germans. Diabetes. 2000;49:504-7.
123. McDermott MF, Ramachandran A, Ogunkolade BW, Aganna E, Curtis D, Boucher BJ, et al. Allelic variation in the vitamin D receptor infl uences susceptibility to IDDM in Indian Asians. Diabetologia. 1997;40(8):971-5.
124. Ban Y, Taniyama M, Yanagawa T, Yamada S, Maruyama T, Kasuga A, et al. Vitamin D receptor initiation codon polymorphism infl uences genetic susceptibility to type 1 diabetes mellitus in the Japanese population. BMC Med Genet. 2001;2:7.
125. Ogunkolade BW, Boucher BJ, Prahl JM, Bustin SA, Burrin JM, Noonan K, et al. Vitamin D receptor (VDR) mRNA and VDR protein levels in relation to vitamin D status, insulin secretory capacity, and VDR genotype in Bangladeshi Asians. Diabetes. 2002;51:2294-300.
126. Yokota I, Satomura S, Kitamura S, Taki Y, Naito E, Ito M, et al. Association between vitamin D receptor genotype and age of onset in juvenile Japanese patients with type 1 diabetes. Diabetes Care. 2002;25:1244.
127. Motohashi Y, Yamada S, Yanagawa T, Maruyama T, Suzuki R, Niino M, et al. Vitamin D receptor gene polymorphism affects onset pattern of type 1 diabetes. J Clin Endocrinol Metab. 2003;88:3137-40.
128. Marti G, Audi L, Esteban C, Oyarzabal M, Chueca M, Gussinye M, et al. [Association of vitamin D receptor gene polymorphism with type 1 diabetes mellitus in two Spanish populations]. Med Clin (Barc). 2004;123:286-90.
129. Ramos-Lopez E, Jansen T, Ivaskevicius V, Kahles H, Klepzig C, Oldenburg J, et al. Protection from type 1 diabetes by vitamin D receptor haplotypes. Ann N Y Acad Sci. 2006;1079:327-34.
130. Shimada A, Kanazawa Y, Motohashi Y, Yamada S, Maruyama T, Ikegami H, et al. Evidence for association between vitamin D receptor BsmI polymorphism and type 1 diabetes in Japanese. J Autoimmun. 2008;30:207-11.
131. Boraska V, Skrabic V, Zeggini E, Groves CJ, Buljubasic M, Peruzovic M, et al. Family-based analysis of vitamin D receptor gene polymorphisms and type 1 diabetes in the population of South Croatia. J Hum Genet. 2008;53:210-4.
132. Nejentsev S, Cooper JD, Godfrey L, Howson JM, Rance H, Nutland S, et al. Analysis of the vitamin D receptor gene sequence variants in type 1 diabetes. Diabetes. 2004;53:2709-12.
133. Turpeinen H, Hermann R, Vaara S, Laine AP, Simell O, Knip M, et al. Vitamin D receptor polymorphisms:no association with type 1 diabetes in the Finnish population. Eur J Endocrinol. 2003;149:591-6.
134. Lemos MC, Fagulha A, Coutinho E, Gomes L, Bastos M, Barros L, et al. Lack of association of vitamin D receptor gene polymorphisms with susceptibility to type 1 diabetes mellitus in the Portuguese population. Hum Immunol. 2008;69:134-8.
135. Ponsonby AL, Pezic A, Ellis J, Morley R, Cameron F, Carlin J, et al. Variation in associations between allelic variants of the vitamin D receptor gene and onset of type 1 diabetes mellitus by ambient winter ultraviolet radiation levels:a meta-regression analysis. Am J Epidemiol. 2008;168:358-65.
136. Guo D, Li M, Zhang Y, Yang P, Eckenrode S, Hopkins D, et al. A functional variant of SUMO4, a new I kappa B alpha modifi er, is associated with type 1 diabetes. Nat Genet. 2004;36:837-41.
137. Wang CY, She JX. SUMO4 and its role in type 1 diabetes pathogenesis. Diabetes Metab Res Rev. 2008;24:93-102.
138. Liu S, Wang H, Jin Y, Podolsky R, Linga Reddy MV, Pedersen J, et al. The IFIH1 Polymorphisms Are Signifi cantly Associated with Type 1 Diabetes and IFIH1 Gene Expression in Peripheral Blood Mononuclear Cells. Hum Mol Genet. 2008.
139. Qu HQ, Marchand L, Grabs R, Polychronakos C. The association between the IFIH1 locus and type 1 diabetes. Diabetologia. 2008;51:473-5.
140. Smyth DJ, Cooper JD, Bailey R, Field S, Burren O, Smink LJ, et al. A genome-wide association study of nonsynonymous SNPs identifi es a type 1 diabetes locus in the interferon-induced helicase (IFIH1) region. Nat Genet. 2006;38:617-9.
141. Sutherland A, Davies J, Owen CJ, Vaikkakara S, Walker C, Cheetham TD, et al. Genomic polymorphism at the interferon-induced helicase (IFIH1) locus contributes to Graves’ disease susceptibility. J Clin Endocrinol Metab. 2007;92:3338-41.
142. Zhao ZF, Cui B, Chen HY, Wang S, Li I, Gu XJ, et al. The A946T polymorphism in the interferon induced helicase gene does not confer susceptibility to Graves’ disease in Chinese population. Endocrine. 2007;32:143-7.
143. Martinez A, Santiago JL, Cenit MC, de Las Heras V, de la Calle H, Fernandez-Arquero M, et al. IFIH1-GCA-KCNH7 locus:infl uence on multiple sclerosis risk. Eur J Hum Genet. 2008;16:861-4.
144. Todd JA, Walker NM, Cooper JD, Smyth DJ, Downes K, Plagnol V, et al. Robust associations of four new chromosome regions from genome-wide analyses of type 1 diabetes. Nat Genet. 2007;39:857-64.
145. Hakonarson H, Qu HQ, Bradfi eld JP, Marchand L, Kim CE, Glessner JT, et al. A novel susceptibility locus for type 1 diabetes on Chr12q13 identifi ed by a genome-wide association study. Diabetes. 2008;57:1143-6.
146. Zoledziewska M, Costa G, Pitzalis M, Cocco E, Melis C, Moi L, et al. Variation within the CLEC16A gene shows consistent disease association with both multiple sclerosis and type 1 diabetes in Sardinia. Genes Immun. 2008.

Av Diabetol. 2009;25:175-86
186
147. Bergholdt R, Larsen ZM, Andersen NA, Johannesen J, Kristiansen OP, Mandrup-Poulsen T, et al. Characterization of new polymorphisms in the 5’ UTR of the human interleukin-1 receptor type 1 (IL1R1) gene:linkage to type 1 diabetes and correlation to IL-1RI plasma level. Genes Immun. 2000;1:495-500.
148. Thomas HE, Irawaty W, Darwiche R, Brodnicki TC, Santamaria P, Allison J, et al. IL-1 receptor defi ciency slows progression to diabetes in the NOD mouse. Diabetes. 2004;53:113-21.
149. Qu HQ, Grant SF, Bradfi eld JP, Kim C, Frackelton E, Hakonarson H, et al. Association analysis of type 2 diabetes Loci in type 1 diabetes. Diabetes. 2008;57:1983-6.
150. Brorsson C, Bergholdt R, Sjogren M, Eising S, Sorensen KM, Hougaard DM, et al. A non-synonymous variant in SLC30A8 is not associated with type 1 diabetes in the Danish population. Mol Genet Metab. 2008;94:386-8.
151. Cervin C, Lyssenko V, Bakhtadze E, Lindholm E, Nilsson P, Tuomi T, et al. Genetic similarities between latent autoimmune diabetes in adults, type 1 diabetes, and type 2 diabetes. Diabetes. 2008;57:1433-7.
152. Bakhtadze E, Cervin C, Lindholm E, Borg H, Nilsson P, Arnqvist HJ, et al. Common variants in the TCF7L2 gene help to differentiate autoimmune from non-autoimmune diabetes in young (15-34 years) but not in middle-aged (40-59 years) diabetic patients. Diabetologia. 2008;51:2224-32.
153. Leslie RD, Kolb H, Schloot NC, Buzzetti R, Mauricio D, De Leiva A, et al. Diabetes classifi cation:grey zones, sound and smoke:Action LADA 1. Diabetes Metab Res Rev. 2008;24:511-9.
154. Halonen M, Eskelin P, Myhre AG, Perheentupa J, Husebye ES, Kampe O, et al. AIRE mutations and human leukocyte antigen genotypes as determinants of the autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy phenotype. J Clin Endocrinol Metab. 2002;87:2568-74.
155. DeVoss JJ, Anderson MS. Lessons on immune tolerance from the monogenic disease APS1. Curr Opin Genet Dev. 2007;17:193-200.
156. Perheentupa J. Autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy. J Clin Endocrinol Metab. 2006;91:2843-50.
157. WTCCC WTCCC. Genome-wide association study of 14,000 cases of seven common diseases and 3,000 shared controls. Nature. 2007;447:661-78.
158. Nagamine K, Peterson P, Scott HS, Kudoh J, Minoshima S, Heino M, et al. Positional cloning of the APECED gene. Nat Genet. 1997;17:393-8.
159. Mathis D, Benoist C. Back to central tolerance. Immunity. 2004;20(5):509-16.
160. Anderson MS, Venanzi ES, Chen Z, Berzins SP, Benoist C, Mathis D. The cellular mechanism of Aire control of T cell tolerance. Immunity. 2005;23:227-39.
161. Gotter J, Brors B, Hergenhahn M, Kyewski B. Medullary epithelial cells of the human thymus express a highly diverse selection of tissue-specifi c genes colocalized in chromosomal clusters. J Exp Med. 2004;199:155-66.
162. van der Vliet HJ, Nieuwenhuis EE. IPEX as a result of mutations in FOXP3. Clin Dev Immunol. 2007:89017.
163. Wildin RS, Ramsdell F, Peake J, Faravelli F, Casanova JL, Buist N, et al. X-linked neonatal diabetes mellitus, enteropathy and endocrinopathy
syndrome is the human equivalent of mouse scurfy. Nat Genet. 2001;27:18-20.
164. Bennett CL, Christie J, Ramsdell F, Brunkow ME, Ferguson PJ, Whitesell L, et al. The immune dysregulation, polyendocrinopathy, enteropathy, X-linked syndrome (IPEX) is caused by mutations of FOXP3. Nat Genet. 2001;27:20-1.
165. Brunkow ME, Jeffery EW, Hjerrild KA, Paeper B, Clark LB, Yasayko SA, et al. Disruption of a new forkhead/winged-helix protein, scurfi n, results in the fatal lymphoproliferative disorder of the scurfy mouse. Nat Genet. 2001;27:68-73.
166. Ludvigsson J, Faresjo M, Hjorth M, Axelsson S, Cheramy M, Pihl M, et al. GAD treatment and insulin secretion in recent-onset type 1 diabetes. N Engl J Med. 2008;359:1909-20.
167. Elias D, Avron A, Tamir M, Raz I. DiaPep277 preserves endogenous insulin production by immunomodulation in type 1 diabetes. Ann N Y Acad Sci. 2006;1079:340-4.
168. Gandhi GY, Murad MH, Flynn DN, Elamin MB, Erwin PJ, Montori VM, et al. Immunotherapeutic agents in type 1 diabetes:a systematic review and meta-analysis of randomized trials. Clin Endocrinol (Oxf). 2008;69:244-52.
169. Barker JM, Triolo TM, Aly TA, Baschal EE, Babu SR, Kretowski A, et al. Two Single Nucleotide Polymorphisms Identify Highest-Risk Diabetes Human Leukocyte Antigen Genotype:Potential for Rapid Screening. Diabetes. 2008.
170. Redondo MJ, Yu L, Hawa M, Mackenzie T, Pyke DA, Eisenbarth GS, et al. Heterogeneity of type I diabetes:analysis of monozygotic twins in Great Britain and the United States. Diabetologia. 2001;44:354-62.
171. Redondo MJ, Rewers M, Yu L, Garg S, Pilcher CC, Elliott RB, et al. Genetic determination of islet cell autoimmunity in monozygotic twin, dizygotic twin, and non-twin siblings of patients with type 1 diabetes:prospective twin study. BMJ. 1999;318:698-702.
172. Lorenzen T, Pociot F, Stilgren LS, Kristiansen OP, Johannesen J, Olsen PB, et al. [Markers for risk of IDDM in children of Danish patients with IDDM. A population-based, historical prospective study]. Ugeskr Laeger. 1999;161:953-8.
173. Jenkins D, Mijovic C, Fletcher J, Jacobs KH, Bradwell AR, Barnett AH. Identifi cation of susceptibility loci for type 1 (insulin-dependent) diabetes by trans-racial gene mapping. Diabetologia. 1990;33:387-95.
174. Todd JA, Mijovic C, Fletcher J, Jenkins D, Bradwell AR, Barnett AH. Identifi cation of susceptibility loci for insulin-dependent diabetes mellitus by trans-racial gene mapping. Nature. 1989;338:587-9.
175. Wicker LS, Chamberlain G, Hunter K, Rainbow D, Howlett S, Tiffen P, et al. Fine mapping, gene content, comparative sequencing, and expression analyses support Ctla4 and Nramp1 as candidates for Idd5.1 and Idd5.2 in the nonobese diabetic mouse. J Immunol. 2004;173:164-73.
176. Zheng W, She JX. Genetic association between a lymphoid tyrosine phosphatase (PTPN22) and type 1 diabetes. Diabetes. 2005;54:906-8.
177. Hakonarson H, Grant SF, Bradfi eld JP, Marchand L, Kim CE, Glessner JT, et al. A genome-wide association study identifi es KIAA0350 as a type 1 diabetes gene. Nature. 2007;448:591-4.
178. Tsygankov AY. Multidomain STS/TULA proteins are novel cellular regulators. IUBMB Life. 2008;60:224-31.