B Pathway κ HBx/ERK/NF- with Chronic Hepatitis B Is Mediated by ...

Ventricular Assist Devices for Chronic Heart Failure
Σ.Γ.Δράκος, Επικ. Καθ/τής
Medical Director, Cardiac Mechanical Support Program
Investigator, Molecular Medicine Program
University of Utah

0
50
100
150
200
250
300
350
400
1980 1990 2000
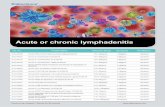
Coronary Deaths
Coronary deaths are down by half But heart failure has almost tripled
Heart Failure
Source: National Hospital Discharge Survey data. Centers for Disease Control and Prevention/National Center for
Health Statistics and National Heart, Lung, and Blood Institute.
Enhanced survival in other CV diseases leads to expansion of HF Population
Heart Failure: The Final Cardiovascular DiseaseChronic Heart Failure: Global Epidemic
- 2.5% of population
- 1 in 5 over 40
- Most common hospital admission diagnosis

322 670 1,2
54
2,3
49
2,9
89
3,5
04
3,7
96
4,4
56
4,6
69
4,6
39
4,8
41
4,7
47
4,7
41
4,6
14
4,5
16
4,2
58
3,9
92
3,8
55
3,8
30
3,7
25
3,6
50
3,6
08
3,7
08
3,7
64
3,7
65
3,7
20
3,7
42
187
0
500
1000
1500
2000
2500
3000
3500
4000
4500
5000
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
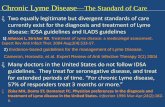
Nu
mb
er
of
Tra
ns
pla
nts
Stehlik J et al. ISHLT Registry; J Heart Lung Transpl 2011
Advanced Heart Failure Therapies:
Heart Transplantation cannot meet the need

Chronic Mechanical Circulatory Support
1. Βridge to Transplant (BTT)
2. Destination Therapy (DT)
3. Bridge to Recovery (BTR)

1. Βridge to Transplant (BTT)
2. Destination Therapy (DT)
3. Bridge to Recovery (BTR)
Chronic Mechanical Circulatory Support

Bridge to Heart Transplant
Proportion of patients surviving to Transplant
Frazier O, et al, JTCS 2001
Aaronson K, et al, JACC 2002
LVAD
Medical
Therapy

Drakos S, …, Renlund D. J Thorac Cardiovasc Surg 2006
Bridge to Heart Transplant
VAD effects Prior to Transplant: HLA sensitization
Drakos S, …, Renlund D. J Heart Lung Transpl 2007
IVIG
No IVIG
Drakos SG, et al. J Heart Lung Transpl 2009
Pulsatile
flow VAD
Continuous
flow VAD

Bridge to Heart Transplant
Survival After Transplant – UTAH program
Drakos SG, et al. J Heart Lung Transpl 2006
Bridged to Tx with LVAD
Bridged to Tx with Medical Therapy
n=278

2nd Era Continuous LVAD
2nd Era Pulsatile LVAD
Nativi JN, Drakos SG, et al. J Heart Lung Transpl 2011
Survival After Transplant – ISHLT Registry
Bridge to Heart Transplant
Bridged to Tx with LVAD
Bridged to Tx with Medical Therapy

1. Βridge to Transplant (BTT)
2. Destination Therapy (DT)
3. Bridge to Recovery (BTR)
Chronic Mechanical Circulatory Support

- N=130 end stage HF patients
- Randomization: LVAD (1st generation) vs Optimal Medical
Therapy
- Too old or too sick for heart transplant- Age 68
- NYHA Class IV
- LVEF 17%
- Wedge 25mmHg
- Cardiac Index 1.9
- IV Inotrope dependent 72%
REMATCH 2001
Disadvantages of 1st Generation, Pulsatile LVADs
2. Engineering Malfunctions after 12-15 months
1. Large Size – Morbidity / Infections
Destination Therapy (DT): Landmark Trials
Medical therapy
LVAD – Pulsatile, 1st generation

Landmark REMATCH Trial:
Late VS. Early Results: UTAH contribution
Park S, et al, J. Thor Cardiovasc Surg 2005

Advantages of 2nd Generation, Continuous-flow LVADs
2. Small Size – Decreased Perioperative Morbidity / Infections
1. No Engineering Malfunctions – Extended Durability (>10 years)
LVAD 2nd generation,
Continuous-flow
LVAD 1st generation,
Pulsatile-flow
“REMATCH II” 2009
Destination Therapy (DT): Landmark Trials

• Meta to Quality of Life tha akolouthisoun ta
complications – “Not everything is perfect”
“REMATCH II” Trial: Complications

• Meta to Quality of Life tha akolouthisoun ta
complications – “Not everything is perfect”
“REMATCH II” Trial: Complications

Medical Therapy Arm of
REMATCH
TRANSPLANT
ISHLT Registry
n>40,000
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
VAD Arm of
REMATCH 2001
(1st generation)
2ndgeneration VAD
INTERMACS 2011,
n=1936
6 12 18 24
Months post LVAD implant
The Field Is Evolving…
3rd generation VAD
1. Technological Advances
2. Patient Management
3. Patient Selection
Su
rviv
al
1. Technological Advances
2. Patient Management
3. Patient Selection

Technology evolves…
2. Wireless energy transfer = elimination of percutaneous
abdominal exit site (3-5 years away from clinic)
1. Size matters!

The Field Is Evolving…
1. Technological Advances
2. Patient Management
3. Patient Selection

Balance Anticoagulation Between…
Wever O, Drakos SG. Pharmacol & Ther 2011

The Field Is Evolving…
1. Technological Advances
2. Patient Management
3. Patient Selection

“…the optimal time for referral in an individual patient’s course of
progressive HF is an art and a science…”
James Fang, NEJM 2009

The Right Time for LVAD Implantation
“Optimal Window”
Operative Risk
Right heart failureEnd-organ dysfunction
Cachexia
Too earlyToo late
AHA statement, Circ 2012
Referred to HF program for VAD/ Tx evaluation if:
a) NYHA III or IV
and
b) two of the following:
- Serum sodium < 136 mmol/L
- Creatinine > 1.8mg/dl
- Intolerant or refractory to ACE/ARB/BB
- Diuretic dose > 1.5 mg/kg/d
- Heart failure-related hospital admissions
- QRS > 140 ms refractory to CRT therapy
- Hematocrit < 35%
Russell S, Miller L , Pagani F. Congestive Heart Failure 2010
Moderate Indication
Strong Indication
Aaronson K, et al. Eur J Heart Fail 2010

Patient Selection to Prevent Post LVAD
Implantation Right Ventricular Failure
Drakos SG, et al. Am J Cardiol 2010
Right Ventricular Failure Risk Score

Quality of Life
Dick Cheney
Who has LVAD?
Πρόγραμμα Χρ. Mητ. Υποβ.
Noζοκ. Eσαγγελιζμoύ -
Γ’ Καρδιολογικής Κλινικής
Παν/μίοσ Αθηνών


HF=2.6 % Population* or6.24 Million
~50 % Preserved Systolic Function
3.12 Million
~240 Million Population≥ age 20 years old
Advanced Stage C and Stage D ≥ age 20 years old
280,800
Theoretical No. of Adults With Advanced HF in US -Potential LVAD candidates for BTT or DT
Advanced Stage C / NYHA class IIIB
124,800
Stage D / NYHA functional class IV
156,000
~50 % Systolic HF
3.12 Million
80-85% Stage A-B
0.5-5 % Stage D
15-20% Stage C (3-4% advanced Stage C)
~ 30% = ~ 90,000 accessible patients
30 BTT or DT LVADs / 100,000 population
Modified after permission from:
Starling R, O’ Connell J

199
93
12
27
0
200
400
600
800
1,000
1,200
1,400
1,600
1,800
2,000
2,200
2,400
2,600
2,800
3,000
3,200
20082007 2010 20112009
U.S. VAD Implants for currently approved indications (BTT, DT)

1. Βridge to Transplant (BTT)
2. Destination Therapy (DT)
3. Bridge to Recovery (BTR)
Chronic Mechanical Circulatory Support

Load Drives Cardiac Remodeling and
HF progression
LV
F
un
cti
on
T
LOAD
Initial Insult
LV
LV
LV
Cardiac Remodeling Trajectory
LV Structure
Hypothesis:
Load ‘Removal’ via LVAD=
Reverse Remodeling?
Cardiac Recovery?

Pre LVAD Post LVADwhen
postdurpre
Mean
value
100,00
90,00
80,00
70,00
60,00
50,00
what: edd
par
kaz
ax
al
who
LV End-diastolic Diameter (mm)
90
80
70
60
50
Drakos S, ..., Yacoub M, Nanas J. Eur Heart J 2007;28: 143Drakos S, …, Yacoub M, Nanas J. Ann Thor Surg 2008; 91: 764
QRS
QTc
Drakos SG, …, Yacoub MH, Nanas JN. JACC Imaging 2008: 3: 64
Pre LVAD Post LVAD
Sympathetic innervation MIBG imaging
Harefield Athens Recovery Program (HARP)
LVAD Unloading: Reverse Remodeling?
Dimopoulos S,…, Nanas S. J Heart Lung Transpl 2010

Drakos S, et al, Circulation 2012
Cardiac Recovery? LVAD Weaning?
Fascinating and Rare Anecdote?
Vs.
Consistent and ‘Real’ Phenomenon?
Harefield Athens Recovery Program

LVAD Induced Cardiac RecoveryFascinating Anecdote Vs. ‘Real’ Phenomenon?
Circulation, July 2012
Reasons for Variable ResultsStudy Design Issues
1. Small Numbers, Retrospective Design
2. Heart Function Monitoring
3. Concurrent Drug Therapy
4. Variable Explantation Criteria (Recovery ‘definition’)
5. Patients Diversity in Recovery Propensity - HF etiologies - extent of pre-LVAD pathologic changes
Drakos SG, et al. Circulation 2012

What Does the Field Need to Advance?
Large- scale, Prospective, Translational Programs:
1. Evaluate Extent of functional Recovery
2. Investigate mechanisms of Recovery

Molecular Medicine Program
HF/ Tx/ VAD Programs
Basic ScienceComponent
Clinical Component
Utah LVAD Recovery Program
Two-phase Translational Program Started in 2008

Hypertrophy Evaluation
Drakos, …, Li DY. JACC 2010; 56: 382-91
1st Phase (Years 1 and 2): Standardization of Tissue Protocols
Microvascular EvaluationFibrosis Evaluation
Utah LVAD Recovery Program

Post LVAD echo
Post LVAD ‘Turn-Down’ echo
Pre LVAD echo
1st Phase (Years 1 and 2): Imaging Protocols Standardization
Utah LVAD Recovery Program

2nd Phase (Year 3): Apply Protocols at Full Scale
Prospective Translational Program:
1. Evaluate Extent of functional Recovery
2. Investigate mechanisms of Recovery
Utah LVAD Recovery Program

1. Evaluate Extent of functional Recovery
2. Investigate mechanisms of Recovery
Prospective Translational Program:
Utah LVAD Recovery Program

1. Infrastructure / Recruit Patients
2. Control for Confounders & Limitations
3. Serial Monitoring of Functional Recovery
Evaluate Extent of functional Recovery
Utah LVAD Recovery Program

1. Infrastructure / Recruit Patients
2. Control for Confounders & Limitations
3. Serial Monitoring of Functional Recovery
Evaluate Extent of functional Recovery
Utah LVAD Recovery Program

Infrastructure/ Recruit Patients
Utah
Progress so far (Tissue & Clinical data):
- 171 LVAD pts prospectively enrolled
- 26 Donors (not allocated for Tx)
Utah LVAD Recovery Program

1. Infrastructure / Recruit Patients
2. Control for Confounders & Limitations
- Concurrent drug therapies
- Duration of unloading
3. Serial Monitoring of Functional Recovery
Utah LVAD Recovery Program
Determine Extent of functional Recovery

1. Infrastructure / Recruit Patients
2. Control for Confounders & Limitations
- Concurrent drug therapies
- Duration of unloading
3. Serial Monitoring of Functional Recovery
- Echo evaluation
- Hemodynamic evaluation
Determine Extent of functional Recovery
Utah LVAD Recovery Program

Pre LVAD Post LVAD (‘Turn-Down’ echo)
Patient “A” Improved Cardiac Function= RESPONDER
Utah LVAD Recovery Program

Patient “B” DID NOT Improve= NON RESPONDERDespite Same Unloading duration, HF duration, HF etiology
Utah LVAD Recovery Program
Pre LVAD Post LVAD (‘Turn-Down’ echo)

Utah LVAD Recovery Program
Drakos SG, et al. JACC In Press
LV Functional ‘Responders’: 19% of pts
Relative LVEF Increase: 50-350%
(echo results on 90 prospectively enrolled pts)
Drakos SG, et al. JACC In Press

Drakos SG, et al. JACC in press
Utah LVAD Recovery Program
Time Course of Unloading- induced Functional Response

LVAD Induced Recovery?Fascinating Anecdote Vs. ‘Real’ Phenomenon?
- Single-program, large-scale
Utah LVAD Preliminary Data
- LVEF degree of improvement superior Pharmac./Regenerative trials
- ‘Burned-out’ HF… exciting implications for less advanced HF

LVAD Induced Recovery?Fascinating Anecdote Vs. ‘Real’ Phenomenon?
- Single-program, large-scale
Utah LVAD Preliminary Data
- LVEF degree of improvement superior Pharmac./Regenerative trials
- ‘Burned-out’ HF… exciting implications for less advanced HF
- Revisit view: human heart incapable of repair/ recovery
- Opportunity understand human heart’s potential to respond to injury/death

Prospective Translational Program:
1. Determine Extent of functional Recovery
2. Investigate mechanisms of Recovery
Utah LVAD Recovery Program

Utah LVAD Recovery Program

Recovery Mechanisms: More Energy Efficient Metabolism?
Utah LVAD Recovery Program
unpublished data

Cell cycle reentry
Recovery Mechanisms: Regeneration?
unpublished data
Utah LVAD Recovery Program

Opportunity to Transform HF Biology and HF Clinical Practice
HF patients
Optimal Medical Therapy
LVADBridge to
Heart Recovery
Utah LVAD Recovery Program
Heart Transplant
Stem cells
Surgical Therapies

Basic ScienceClinical
Research Fellows
Nikos Diakos
Omar Wever
Abdul Saidi
Div Verma
Chi Yen

LVAD Unloading & RecoveryWhat are the Future Research Targets?
Drakos SG, et al. Circulation 2012

Guest Faculty
David Kass, MD, Johns Hopkins
Douglas Mann, MD, Washington Univ.
Joseph Hill, MD, PhD, Univ. Texas Southwestern
Michael Givertz, MD, Harvard Univ.
Joseph Rogers, MD, DUKE Univ.
Roger Hajjar, MD, Mount Sinai
Simon Maybaum, MD, Albert Einstein College of Medicine
Evangelia Kranias, PhD, Univ. of Cincinnati
Mark Slaughter, MD, Univ. of Louisville
Francis Spinale, MD, MUSC
Evgenij Potapov, MD, Berlin Heart Institute, Germany
John V. Terrovitis, MD, University of Athens, Greece

Summary
- Bridge to Transplant, Destination Therapy:
1st line therapeutic options for selected HF patients
- Room for Improvement / Decrease Complications:
1. Technological Advances,
2. Patient Management,
3. Patient Selection

Summary
Research in LVAD Recovery field:
- Transform role of LVAD from BTT to enabler of cardiac recovery?
- Revisit view: human heart incapable of repair/ recovery
- Redirect Basic Science of cardiac recovery by focusing
the field on basic pathways relevant to humans (i.e. biomarkers derived
from LVAD ‘Responders’)


Funding Sources for UTAH Recovery Program
1. VA Merit Award
2. American Heart Association
3. CTSA/NIH Award
4. Deseret Foundation
5. U of U Molecular Medicine (U2M2)
6. Intermountain Health Care


Importance of Pulse in Flow both for the
Peripheral Organs and the Heart ?
2nd Generation, Continuous-flow VADs: Concerns due to non- pulsatile/ non- physiologic
blood flow pattern

Coronary Flow
Cardiac
Output
Aortic Pressure
Right Atrial Pressure
Non-Pulsatile flow
Pulsatile flow
Drakos S, Ntalianis A, …, Nanas J. ASAIO J 2002
Short-term Support: Pulse in Flow Does Matter!Porcine model of ACUTE HF

Animal data suggested adaptation to the non–physiologic/ non-pulsatile flow over a period of few weeks
Jett, et al, ASAIO J 1999Saito, et al, Ann Thor Surg 2002
Tominaga, et al, J Thorac Cardiovasc Surg 1996
Long-term Support: Pulse Less Crucial ?

Long-term support: Human Peripheral Organs Adapt to Non Pulsatile flow

Increased GI Bleeding with
Non-Pulsatile LVADs?
Crow et al. J Thorac Cardiovasc Surg 2009

LVAD Unloading & Recovery: Future DirectionsOptimal Type of Unloading ?
Drakos, Kfoury, ..., Li. Circulation 2012, In Press