IL-4 Indirectly Suppresses IL-2 Production by Human T Lymphocytes ...

Cite this article: Bekaroğl MG, Arslan BA (2014) Natural Killer (NK) Cells in β Thalassemia Major Patients. JSM Biotechnol Bioeng 2(2): 1040.
JSMBiotechnology & Biomedical EngineeringSpecial Issue on
Cell-Microenvironment InteractionEdited by:Feng ZhaoAssistant Professor, Department of Biomedical Engineering, Michigan Technological University, Houghton, MI, USA
Central
*Corresponding authorBelkis Atasever Arslan, Department of Molecular Biology and Genetics, Faculty of Engineering and Natural Sciences, Üsküdar University, Istanbul, Turkey, Tel: +90 216 400 2222; Fax: 90 216 530 06 15; E-mail:
Submitted: 24 December 2013
Accepted: 09 September 2014
Published: 09 September 2014
ISSN: 2333-7117
Copyright© 2014 Bekaroğl et al.
OPEN ACCESS
Keywords• Thalassemia• NK cells• Immune system
Review Article
Natural Killer (NK) Cells in β Thalassemia Major PatientsMaide Gökçe Bekaroğlu1,2, Belkis Atasever Arslan1*1Department of Molecular Biology and Genetics, Faculty of Engineering and Natural Sciences, Üsküdar University, Turkey 2Physics Engineering Department, Faculty of Science and Letters, Istanbul Technical University, Turkey
Abstract
β-Thalassemia major is a genetic and severe blood disorder caused by absence of β-globin chain production. Regular blood transfusion treatments can lead to modifications in cytokine levels and lymphocyte subsets. Natural killer (NK) cells are lymphocyte subtypes that are a major part of innate immune responses against infectious pathogens and tumor cells. NK activity is critical for susceptibility of β-Thalassemia major patients against cancer and bacterial infections. This review discusses recent literature focused on this issue. As independent from regular blood transfusions and iron overload, effects of the other cellular and transcriptional factors causing decreased NK activity in β-Thalassemia major patients are still unknown. If NK activity mechanisms and its abnormalities in β-Thalassemia major patients were fully understood, activity rate can be regulated to reduce the risk of cancer and infectious diseases.
INTRODUCTIONThalassemia is an inherited epidemic disease which is usually
seen in Mediterranean region, Middle East countries, India, Far East and tropical Africa. As the population of world increases rapidly, thalassemia has started to be seen in the non-epidemical countries [1]. Three percent of World’s population suffers from heterozygous β -Thalassemia and in general 270 million people are carriers of mutant β-globin gene which can cause thalassemia [2]. Each year more than 300.000 children are born with a β-globin gene disorder [3,4]. It can be said that thalassemia is a very common genetic disorder which can cause mortality and morbidity. Most common causes of death in β−Thalassemia major are heart diseases, infections, liver diseases, and malignancy [5].
Increased susceptibility to infections and cancerous diseases
are commonly seen in β-Thalassemia major patients [6,7]. Studies demonstrate that NK activity is decreased in β-Thalassemia major patients [8,9]. In general NK cells play an important role in the destruction of pathogen microorganisms and infected cells especially in the early phase. In addition, NK cells kill tumor cells. They play especially a vital role in defense against cytopathic viruses [10-13]. It is believed that iron overload and splenectomy causes decreased NK activity in β-Thalassemia major patients[14]. However, there are very limited amount of studies about physiological mechanisms of decreased NK activity in β-Thalassemia major patients. Many micro environmental factors causing decreased activity in NK cells are still unknown. If the physiological mechanism underlying for decreased activity of NK cells were known, it could be used to prevent infection and cancer risks in β-Thalassemia major patients.

Central
Bekaroğl et al. (2014)Email:
JSM Biotechnol Bioeng 2(2): 1040 (2014) 2/6
Reduced synthesis of β-globin chain causes β-Thalassemia [15]. There are 200 mutations in β-globin gene that can cause β-Thalassemia. While some of the mutations block the expression of the β-globin genes totally, some of them just reduce it. If β-globin chains are not completely expressed, it is called β-Thalassemia and when it’s just reduced it is called β-Thalassemia [16]. Absence of β-globin chain production in erythrocytes leads to over production of β-globin chain in β-Thalassemia major patients. β-globin chains are not stable, and excessive β-globin chain production increases the erythrocyte sedimentation rate. Ineffective erythropoiesis leads to apoptosis of erythrocyte precursors in bone marrows and shortens lifetime of erythrocytes [1] Ineffective erythropoiesis can cause many complications such as anemia, free iron and oxygen radicals in the blood, altered immune responses, osteoporosis and osteopenia, damaged cytoskeletons, etc. [15,17-19]. Without treatment, life expectancy is reduced to several years [20]. Regular blood transfusions, stem-cell transplantations and iron chelation treatments are applied to elongate the life span of β-Thalassemia major patients [21]. In most cases, regular blood transfusions are used to treat thalassemia and its symptoms [20].
REGULAR BLOOD TRANSFUSIONS AND IRON OVERLOAD
β-Thalassemia major patients are treated with repeated blood transfusions to prevent anemia [22]. Regular blood transfusions and ineffective erythropoiesis triggering intestinal iron absorption can cause iron overload in β-Thalassemia patients. Regular blood transfusions, done every 2-4 week, lead to approximately 15-20 mg/day iron overload in patients [23-26]. Iron overload is still the main reason for the mortality and morbidity in β-Thalassemia major patients. Because of the reducing properties of free iron
in the system; iron overload, due to regular blood transfusions leads to the production of toxic oxygen radicals. These oxygen radicals mediating protein degeneration and lipid peroxidation on cell membrane and organelles causes death of cells and organ failure such as cardiac insufficiency, endocrine abnormalities, and cirrhosis [1-27]. Also, it is shown that regular transfusion treatments decrease NK activity and alter the immune responses in β-Thalassemia major patients [28]. Low activity of NK cells and immune abnormalities reduce the resistance against infections and developing malignancy [25]. Cellular iron homeostasis is important for immune functions. Both iron deficiency and iron overload can affect the immune system. Iron plays a critical role in macrophage mediated cytotoxicity by catalyzing reactive oxygen species production in phagolysosomes [29]. It’s also important for the immune response of mononuclear phagocyte system cells. The increase of unbounded iron to ferritin in cells causes decreasing of effects of IFN on mononuclear phagocytes [30]. Studies show that iron overload is not the only cause for immune abnormalities and the decreased activity of NK cells in β-Thalassemia; also there are many different functional defects in immune system components such as T and B lymphocytes, NK cells, etc. [32]. However, there are not enough studies showing these functional defects in particular.
Immune system in β-Thalassemia major
In β-Thalassemia major patients, infections are one of the main reasons of mortality of 12-46 % of patients. Recent studies show that gram negative microorganisms are responsible for at least half of the serious bacterial infections in thalassemia patients [32]. In addition, sepsis, soft tissue infections, osteomyelitis, corneal ulcers, enteritises and abscesses on liver, lungs, kidneys, intra abdominal area, retropharynx, gingival
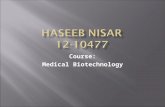
Figure 1 The immune response cascade between NK cells and dendritic cells.

Central
Bekaroğl et al. (2014)Email:
JSM Biotechnol Bioeng 2(2): 1040 (2014) 3/6
and hips were reported clinically. It is found that splenectomy and iron chelation therapy are an independent risk factor in the development of infectious diseases [33]. Increased susceptibility to infectious diseases (independent of multiple transfusions) indicates the existence of immune deficiency in β-Thalassemia major patients [32]. NK cell activity plays an important role in immune system homeostasis. Factors that affect NK activity are crucial for optimizing the NK activity. Therefore, these factors are important to achieve immune system homeostasis [34,35,36].
In β-Thalassemia major patients, monocyte and neutrophil activities are declined, whereas polyclonal immunoglobin synthesis increases and the activity of alternative complement pathway is corrupted. In addition, lymphocyte subgroups have changed functionally and numerically for these patients. It’s also reported that lymphocyte phenotypes of splenectomized patients and their C-reactive protein levels were altered [34]. Also, a different study shows that while NK cell number of children with β-Thalassemia was decreased, their T lymphocytes were increased. It’s also reported that the number of NK cells and transfusion number are inversely proportional. These abnormalities are thought to result from transfusions, iron overload or splenectomy [25,34,35]. The primary mechanism causing these immunological modifications is still unknown.
NK cells and their functions
The presence of cytotoxic cells against the virus infected cells and tumors were found by Paul Ehrlich 100 years ago. In 1950’s MacFarlane Burnet showed that the immune system plays a role in the regulation of cellular transformation and decreasing tumor growth [37]. The identification of NK cells was made approximately 30 years ago by Rolf Kiessling [38]. In the human body, NK cells form the third subgroup of lymphocytes after T cells and B cells and they constitute the 5-15% of the total lymphocytes in peripheral blood. NK cells are classically known with CD56+ and CD3- surface markers. In addition, natural cytotoxicity receptors , leukocyte marker 7 (Leu-7/ CD57), interleukin 2 receptors (IL2R β), CD69, several activator receptors bonded to target cell and Killer cell lectin-like receptor B1(KLRB1/CD161) are also identified as NK markers [39-42]. Also in adulthood stage the expression of NKG2A decreases and KIR expression in NK cells increases [43].
Although NK cells are parts of innate immunity, also they play a role in adaptive immune response directly via dendritic cells. The interaction between NK cells and dendritic cells provides positively or negatively regulation of dendritic cell activity. Dendritic cells, antigen presenting cells, are important for T cell response. This interaction contributes to feedback regulation of T cell-mediated immune response. On T cell-mediated activation, NK cells are thought to be a regulator both as trigger and suppressor. Because NK cells can costimulate via interacting directly with T lymphocytes, CD40L (CD154) and OX40L ligands expressed by NK cells allows to transmit co-stimulator signals of NK cells to T and B lymphocytes. Thus, a bridge between innate and adaptive immunity is built [44-47]. Immune alterations can affect both the innate and adaptive immune- system, these alterations can lead to functional defects in neutrophil chemotaxis, natural killer (NK) function, neutrophil and macrophage phagocytosis [48].
NK cells mediate cytotoxicity and also produce chemokines and inflammatory cytokines such as IFNγ and TNFα [41,47,49]. The killing function of NK cells against the target cell (simultaneously without antigenic stimulation) is decided by the inhibitor and activator signals located on cell surface [50-53]. Inhibitor receptor superfamily (IRS) located on the surface of NK cells prevents from harming the cells expressing self-MHC molecules [45,46]. Decreased MHC class I expression of virus infected cells or tumor cells increases their sensitivity against NK mediated lysis [40,46]. As a result, NK cells kill the cells which are absent or ineffectively expressed of MHC class I molecules [54]. Also, when bone marrow transplant procedure is used to cure thalassemia, NK cells play an important role in bone marrow transplantation and preventing graft-versus-host disease [39,14].
γThe other important effector function of NK cells is that they can induce inflammatory responses by secreting proinflammatory cytokines and chemokine [55]. These cytokines are: IFNγ, TNFα, lymphotoxinα (LTαGM-CSF, IL5, IL13, IL10 macrophage inflamatory protein (MIP-1(α and β) CCL3[41,13,46,56,31]. NK cells are important for immune regulation, when these cells are stimulated by IL12/ IL1, IL12/IL15 or IL12/IL18, they secrete IFNγ, TNFα, IL10,IL13 and GM-CFS[28=13]. IFNγ is an essential cytokine, which has a central role in immune defense. IFNγ plays also an important role for regulation of hundreds of genes, which are related with immune system functions and resistance against infections. IFNγ, activates macrophage and neutrophils, stimulates the alienation of Th1 CD4+ lymphocytes, enhances antigen presenting by increasing the expression of MHC, and this leads to the interactions between IgG and B cells. Thereby IFNγ has a binding function on adaptive immunity [38, 41]. While IL2, IL12, IL15, IL18, TNF α and IFN α/β contributes to the activation of NK cells; IL4, IL10 and TGFβ suppresses NK cell activity. IL12 and IL18 are important for triggering immune response. The secretion of IL12 and IL18 increases IFNγ level [13,38,41]. NK cells trigger dendritic cells to secrete IL18. This cytokine does not increase cytolytic activation of NK cells as distinct from other helper factors increasing NK activation but causes differentiation of NK cells to help the activation [57]. IL2, IL18 or TLR2 ligands cause activation dependent on NF-κB in NK cells. Natural cytotoxicity receptor (NKp30) causes a fast degradation of l-κB and NF-κB nuclear translocation for NK activation [58]. Receptors like NKp30, NKp44 and NKp46 are important for NK cells to mediate cytotoxicity [59], but ligands of these receptors are not known completely.
NK cell activity in β-Thalassemia Major
Most of the studies show that NK activity is decreased in β-Thalassemia major patients [25,55,60]. However cellular mechanism and transcriptional regulation of NK cells of those patients are still unknown. There are limited numbers of articles on NK activity in β-Thalassemia major patients [61-64]. Some studies show that, In vitro conditions, desferrioxamine or 2,3- dihydroxybenzoic acid (DHB) chelators can increase the activity of NK cells [55,65]. Also, it is demonstrated that Vitamin C increases NK activation in those patients [60]. Other studies showed that NKp30 and aberrant secretion of IL10, TGFb1 and IL15 cytokines are possible major reasons of underlying mechanism of decreased NK activity in β-Thalassemia Major patients [66]. So, it can be

Central
Bekaroğl et al. (2014)Email:
JSM Biotechnol Bioeng 2(2): 1040 (2014) 4/6
said that NK cell activity is not only dependent to environmental factors; there can be a defect at the physiological mechanisms of NK cells in β-Thalassemia major patients. Also, these studies show that lower NK activity of β-Thalassemia patients caused by iron overload and oxidative stress can be modulated.
SUMMARY AND FUTURE OUTLOOK It is mentioned that β-Thalassemia major is a severe disease
which can lead to infection and cancer related mortality and morbidity. This condition indicates that there are some problems in the immune system. Previously it is shown that NK cell activity is an important part of the adaptive and innate immune system and factors that affect NK activity can also affect immune responses against cancer and infectious diseases. Many studies show that NK activity is decreased in β-Thalassemia major patients. Decreased NK cell activity is a serious problem which must be fixed in order to prevent infectious diseases and cancer for these patients. Until this day iron overload and splenectomy was blamed for the decreased activity of NK cells, but cellular mechanisms and transcriptional regulations of NK cells are still unknown. There are not many studies searching these unknown mechanisms. It is stated before that some of these few studies showed that DHB chelators and vitamin C can increase NK activity for β-Thalassemia major patients. Also, NKp30 receptors and IL10, TGFb1 and IL15 cytokine secretions were stated unusual for β-Thalassemia major patients. Many other micro environmental factors are still unknown. Considering the network of mononuclear cells, not only regular blood transfusion and iron overload causes decreased NK activity; also other mononuclear cells may affect NK activity or iron overload can affect indirectly NK activity through other mononuclear cells. If the physiological mechanisms underlying for decreased activity of NK cells were known, it could be used to modulate NK activity and prevent infection and cancer risks and improve life standards of β-Thalassemia major patients. The answer of these questions is important to develop new strategies against the disease and its complications.
REFERENCES1. Birgens H, Ljung R. The thalassaemia syndromes. Scand J Clin Lab
Invest. 2007; 67: 11-25.
2. Quek L,Thein SL. Molecular therapies in beta-thalassaemia. Br J Haematol. 2007; 136: 353-365.
3. Efremov GD. Dominantly Inherited beta-Thalassemia. Hemoglobin. 2007; 31: 193-207.
4. Authors Weatherall D,Akinyanju O, Fucharoen S, Olivieri N, Musgrove P. Inherited Disorders of Hemoglobin.
5. Gaziev J, Sodani P, Polchi P,Andreani M,Lucarelli G. Bone marrow transplantation in adults with thalassemia. Treatment and long-term follow-up. Ann N Y Acad Sci. 2005; 1054: 196-205.
6. Rahav G, Volach V, Shapiro M, Rund D, Rachmilewitz EA, Goldfarb A. Severe infections in thalassaemic patients: prevalence and predisposing factors. Br J Haematol. 2006; 133: 667-674.
7. Zurlo MG, De Stefano P, Borgna-Pignatti C, Di Palma A, Piga A, Melevendi C,et al. Survival and causes of death in thalassaemia major. Lancet, 1989; 2: 27-30.
8. Akbar AN, Fitzgerald-Bocarsly PA, de Sousa M, Giardina PJ, Hilgartner MW. Decreased natural killer activity in thalassemia major: a possible consequence of iron overload. J Immunol. 1986; 136: 1635-1640.
9. Atasever B, Ertan NZ, Erdem-Kuruca S, Karakas Z. In vitro effects of vitamin C and selenium on NK activity of patients with beta-thalassemia major. Pediatr Hematol Oncol. 2006; 23: 187-197.
10. Gati A, Da Rocha S, Guerra N, Escudier B, Moretta A, Chouaib S, Angevin E. Analysis of the natural killer mediated immune response in metastatic renal cell carcinoma patients. Int J Cancer. 2004; 109: 393-401.
11. Matsushita N, Aruga A, Kobayashi Y, Tanigawa K, Yamamoto M. Separation methods of T cells, natural killer, and dendritic cells from peripheral blood of cancer patients using interleukin-2 and functional analysis of natural killer cells after separation. Immunopharmacol Immunotoxicol. 2007; 29 : 31-47.
12. Akbar AN, Fitzgerald-Bocarsly PA, de Sousa M, Giardina PJ, Hilgartner MW, Grady RW,. Decreased natural killer activity in thalassemia major: a possible consequence of iron overload. J Immunol. 1986; 136: 1635-1640.
13. Walzer T, Dalod M, Robbins SH, Zitvogel L, Vivier E. Natural-killer cells and dendritic cells: “l’union fait la force” Blood. 2005; 106: 2252-2258.
14. Walker EM Jr, Walker SM. Effects of iron overload on the immune system. Ann Clin Lab Sci. 2000; 30: 354-365.
15. Cao A, Galanello R, Origa R. Beta-Thalassemia. In: Pagon RA, Adam MP, Bird TD, editors. Seattle (WA): University of Washington, Seattle. 1993-2014.
16. Weatherall DJ. Thalassemia as a global health problem: recent progress toward its control in the developing countries. Ann N Y Acad Sci. 2010; 1202: 17-23.
17. Benetatos L, Alymara V, Vassou A, Bourantas KL. Malignancies in beta-thalassemia patients: a single-center experience and a concise review of the literature. Int J Lab Hematol. 2008; 30: 167-172.
18. Efremov GD. Thalassemias and other hemoglobinopathies in the Republic of Macedonia. Hemoglobin. 2007; 31: 1-15.
19. Perrotta S, Cappellini MD, Bertoldo F, Servedio V, Iolascon G, D’Agruma L, et al. Osteoporosis in beta-thalassaemia major patients: analysis of the genetic background. Br J Haematol. 2000; 111: 461-466.
20. Rachmilewitz EA, Giardina PJ. How I treat thalassemia. Blood. 2011; 118: 3479-3488.
21. Marziali M, Isgrò A, Gaziev J, Lucarelli G. Hematopoietic stem cell transplantation in thalassemia and sickle cell disease. Unicenter experience in a multi-ethnic population. Mediterr J Hematol Infect Dis. 2009; 1: e2009027.
22. Akbar AN, Fitzgerald-Bocarsly PA, Giardina PJ, Hilgartner MW, Grady RW. Modulation of the defective natural killer activity seen in thalassaemia major with desferrioxamine and alpha-interferon. Clin Exp Immunol. 1987; 70: 345-353.
23. Li K, Wong A, Li CK, Shing MM, Chik KW, Tsang KS. Granulocyte colony-stimulating factor-mobilized peripheral blood stem cells in beta-thalassemia patients: kinetics of mobilization and composition of apheresis product. Exp Hematol. 1999; 27: 526-532.
24. Vitucci A, Lucivero G, Locatelli F, Capocasale M, Tannoia N. Lymphocyte subset reconstitution after HLA-identical placental blood transplantation (PBT) or PBT plus bone marrow transplantation (BMT) in three children with beta-thalassemia major. Bone Marrow Transplant. 2000; 26: 743-747
25. Li K, Li CK, Wong RP, Wong A, Shing MM, Chik KW, Yuen PM. Transfusion-related immunomodulation in Chinese children with thalassaemia. Vox Sang. 1997; 73: 167-173.
26. Kontoghiorghes GJ. Iron mobilization from transferrin and non-

Central
Bekaroğl et al. (2014)Email:
JSM Biotechnol Bioeng 2(2): 1040 (2014) 5/6
transferrin-bound-iron by deferiprone. Implications in the treatment of thalassemia, anemia of chronic disease, cancer and other conditions. Hemoglobin. 2006; 30: 183-200.
27. Beutler E. Iron storage disease: facts, fiction and progress. Blood Cells Mol Dis. 2007; 39: 140-147.
28. Li K, Wong A, Li CK, Shing MM, Chik KW, Tsang KS, et al. Granulocyte colony-stimulating factor-mobilized peripheral blood stem cells in beta-thalassemia patients: kinetics of mobilization and composition of apheresis product. Exp Hematol. 1999 ; 27: 526-532.
29. Gordeuk VR, Delanghe JR, Langlois MR, Boelaert JR. Iron status and the outcome of HIV infection: an overview. J Clin Virol. 2001; 20: 111-115.
30. Weiss G. Iron and immunity: a double-edged sword. Eur J Clin Invest. 2002; 32 Suppl 1: 70-78.
31. Zwirner NW, Fuertes MB, Girart MV, Domaica C, Rossi LE. Cytokine-driven regulation of NK cell functions in tumor immunity: role of the MICA-NKG2D system. Cytokine Growth Factor Rev. 2007; 18: 159-170.
32. Farmakis D, Giakoumis A, Polymeropoulos E, Aessopos A. Pathogenetic aspects of immune deficiency associated with beta-thalassemia. Med Sci Monit. 2003; 9: 19-22.
33. Wang SC, Lin KH, Chern JP, Lu MY, Jou ST, Lin DT, Lin KS. Severe bacterial infection in transfusion-dependent patients with thalassemia major. Clin Infect Dis. 2003; 37: 984-988.
34. Lombardi G, Matera R, Minervini MM, Cascavilla N, D’Arcangelo P, Carotenuto M, Di Giorgio G. Serum levels of cytokines and soluble antigens in polytransfused patients with beta-thalassemia major: relationship to immune status. Haematologica. 1994; 79: 406-412.
35. Moshtaghi-Kashanian GR, Gholamhoseinian A, Hoseinimoghadam A, Rajabalian S. Splenectomy changes the pattern of cytokine production in beta-thalassemic patients. Cytokine. 2006; 35: 253-257.
36. Wilkinson GW, Tomasec P, Stanton RJ, Armstrong M, Prod’homme V, et al. Modulation of natural killer cells by human cytomegalovirus. J Clin Virol. 2008; 41: 206-212.
37. Gomes AQ, Correia DV, Silva-Santos B. Non-classical major histocompatibility complex proteins as determinants of tumour immunosurveillance. EMBO Rep. 2007; 8: 1024-1030.
38. Arnon T, Markel G, Mandelboim O. Tumor and viral recognition by natural killer cells receptors. Semin Cancer Biol. 2006; 16: 348-358.
39. Whiteside TL, Herberman RB. Role of human natural killer cells in health and disease. Clin Diagn Lab Immunol. 1994; 1: 125-133.
40. Albertsson PA, Basse PH, Hokland M, Goldfarb RH, Nagelkerke JF, et al. NK cells and the tumour microenvironment: implications for NKcell function and anti-tumour activity. Trends Immunol 2003; 24: 603-609.
41. Korbel DS, Finney OC, Riley EM. Natural killer cells and innate immunity to protozoan pathogens. Int J Parasitol. 2004; 34: 1517-1528.
42. Matsushita N, Aruga A, Kobayashi Y, Tanigawa K, Yamamoto M. Separation methods of T cells, natural killer, and dendritic cells from peripheral blood of cancer patients using interleukin-2 and functional analysis of natural killer cells after separation. Immunopharmacol Immunotoxicol. 2007; 29: 31-47.
43. Sundström Y, Nilsson C, Lilja G, Kärre K, Troye-Blomberg M, et al. The expression of human natural killer cell receptors in early life. Scand J Immunol. 2007; 66: 335-344.
44. Backström E, Kristensson K, Ljunggren HG. Activation of natural killer
cells: underlying molecular mechanisms revealed. Scand J Immunol. 2004; 60: 14-22.
45. Poggi A, Zocchi MR. Human natural killer lymphocytes through the engagement of natural cytotoxicity receptors and NKG2D can trigger self-aggression. Autoimmun Rev. 2007; 6: 295-299.
46. Orange JS, Ballas ZK. Natural killer cells in human health and disease. Clin Immunol. 2006; 118: 1-10.
47. Raulet DH. Interplay of natural killer cells and their receptors with the adaptive immune response. Nat Immunol. 2004; 5: 996-1002.
48. Ricerca BM, Di Girolamo A, Rund D. Infections in thalassemia and hemoglobinopathies: focus on therapy-related complications. Mediterr J Hematol Infect Dis. 2009; 1: e2009028.
49. Caligiuri MA. Human natural killer cells. Blood. 2008; 112: 461-469.
50. Costello RT, Fauriat C, Sivori S, Marcenaro E, Olive D. NK cells: innate immunity against hematological malignancies? Trends Immunol. 2004; 25: 328-333.
51. Fischer L,Hummel M, Burmeister T, Schwartz S,Thiel E. Skewed expression of natural-killer (NK)-associated antigens on lymphoproliferations of large granular lymphocytes (LGL). Hematol Oncol. 2006; 24: 78-85.
52. Ogbomo H, Michaelis M, Kreuter J, Doerr HW, Cinatl J Jr. Histone deacetylase inhibitors suppress natural killer cell cytolytic activity. FEBS Lett. 2007; 581: 1317-1322.
53. De Celis R, Feria-Velasco A, Bravo-Cuellar A, Hicks-Gómez JJ, García-Iglesias T, et al.Expression of NK cells activation receptors after occupational exposure to toxics: a preliminary study. Immunol Lett. 2008; 118: 125-131.
54. Moretta L, Biassoni R, Bottino C, Cantoni C, Pende D, et al. Human NK cells and their receptors. Microbes Infect. 2002; 4: 1539-1544.
55. Akbar AN, Fitzgerald-Bocarsly PA, de Sousa M, Giardina PJ, Hilgartner MW, Grady RW, et al. Decreased natural killer activity in thalassemia major: a possible consequence of iron overload. J Immunol. 1986; 136: 1635-1640.
56. Poggi A, Prevosto C, Massaro AM, Negrini S, Urbani S, Pierri I, et al. Interaction between human NK cells and bone marrow stromal cells induces NK cell triggering: role of NKp30 and NKG2D receptors. J Immunol. 2005; 175: 6352-6360.
57. Semino C, Ceccarelli J, Lotti LV, Torrisi MR, Angelini G, Rubartelli A. The maturation potential of NK cell clones toward autologous dendritic cells correlates with HMGB secretion. J Leukoc Biol. 2007; 81: 92-99.
58. Pandey R, DeStephan CM, Madge LA, May MJ, Orange JS. NKp30 ligation induces rapid activation of the canonical NF-kappaB pathway in NK cells. J Immunol. 2007; 179: 7385-7396.
59. Koch J, Steinle A, Watzl C, Mandelboim O. Activating natural cytotoxicity receptors of natural killer cells in cancer and infection. Trends Immunol. 2013; 34: 182-191.
60. Atasever B, Ertan NZ, Erdem-Kuruca S, Karakas Z. In vitro effects of vitamin C and selenium on NK activity of patients with beta-thalassemia major. Pediatr Hematol Oncol. 2006; 23: 187-197.
61. Baldini M, Serafino S, Zanaboni L, Cappellini MD. Thyroid cancer in β-thalassemia. Hemoglobin. 2012; 36: 407-408.
62. Poggi M,Sorrentino F, Pascucci C, Monti S, Lauri C, Bisogni V, et al. Malignancies in β-thalassemia patients: first description of two cases of thyroid cancer and review of the literature. Hemoglobin. 2011; 35: 439-446.
63. Govoni MR, Sprocati M, Fabbri E, Zanforlin N, De Sanctis V. Papillary

Central
Bekaroğl et al. (2014)Email:
JSM Biotechnol Bioeng 2(2): 1040 (2014) 6/6
Bekaroğl MG, Arslan BA (2014) Natural Killer (NK) Cells in β Thalassemia Major Patients. JSM Biotechnol Bioeng 2(2): 1040.
Cite this article
thyroid cancer in thalassaemia. Pediatr Endocrinol Rev. 2011; 8 Suppl 2: 314-321.
64. Sallam MM, Alsuliman AM, Alahmed HE, Alabdulaali MK. Chronic myelogenous leukemia in sickle cell/beta 0-thalassemia. Indian J Pathol Mi crobiol. 2011; 54: 597-598.
65. Akbar AN, Fitzgerald-Bocarsly PA, Giardina PJ, Hilgartner MW, Grady RW. Modulation of the defective natural killer activity seen in
thalassaemia major with desferrioxamine and alpha-interferon. Clin Exp Immunol. 1987; 70: 345-353.
66. Atasever Arslan B, Erdem-Kuruca S, Karakas Z, Erman B, Ergen A. Effects of micro environmental factors on natural killer activity (NK) of beta thalassemia major patients. Cell Immunol. 2013 Apr; 282: 93-99.