4 ΣΥΜΠΟΣΙΟ ΚΛΙΝΙΚΗΣ ΟΓΚΟΛΟΓΙΑΣ: Ακτινοθεραπεία στον...
39
Συστηματικη θεραπεία όγκων GIST ΑΛΕΞΗΣ ΣΤΡΙΜΠΑΚΟΣ Παθολόγος Ογκολόγος Δ/της Δ’Ογκολογικής Κλινικής Ευρωκλινική Αθηνών
-
Upload
isrodoy-isr -
Category
Health & Medicine
-
view
53 -
download
3
Transcript of 4 ΣΥΜΠΟΣΙΟ ΚΛΙΝΙΚΗΣ ΟΓΚΟΛΟΓΙΑΣ: Ακτινοθεραπεία στον...
Συστηματικη θεραπεία όγκων GIST
ΑΛΕΞΗΣ ΣΤΡΙΜΠΑΚΟΣΠαθολόγος Ογκολόγος
Δ/της Δ’Ογκολογικής ΚλινικήςΕυρωκλινική Αθηνών
EPIDEMIOLOGY
GIST represents a form of sarcoma that comprises approx. 1% to 3% of all malignant GI tumors.
GIST occurs predominantly in adults . The incidence has been slightly higher in men than
women. Small asymptomatic GISTs are found at autopsy in
more than 50 % of individuals over the age of 50 GIST treatment trials estimate an annual incidence
of 4,500 – 6,000 new cases (USA)
Συστηματική θεραπεία όγκων GIST
Επικουρική θεραπεία
Θεραπεία προχωρημένης νόσου– Unresectable
• ?potentially resectable– metastatic
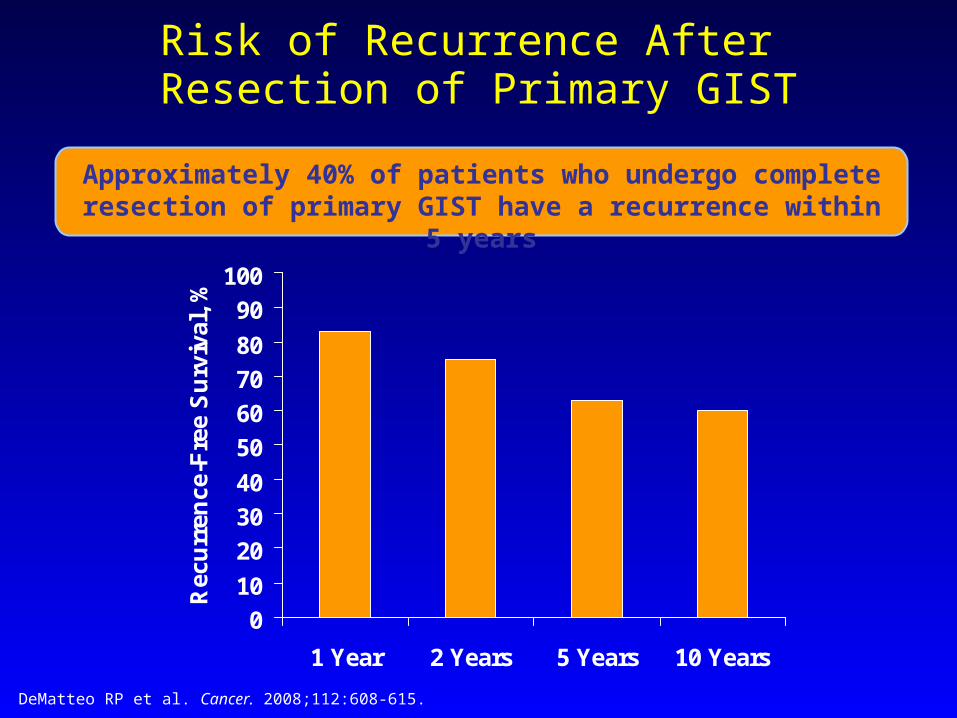
Risk of Recurrence After Resection of Primary GIST
DeMatteo RP et al. Cancer. 2008;112:608-615.
Approximately 40% of patients who undergo complete resection of primary GIST have a recurrence within 5 years
0102030405060708090
100
1 Year 2 Years 5 Years 10 Years
Rec
urre
nce-
Free
Sur
viva
l, %
Risk Assessment
Accurate assessment of risk of aggressive malignant behaviour in GIST poses a challenge1
Morphologic features most predictive of outcome1,2
- Mitotic index - Tumour size
Tumour site and rupture also affect risk of recurrence and progression2,3
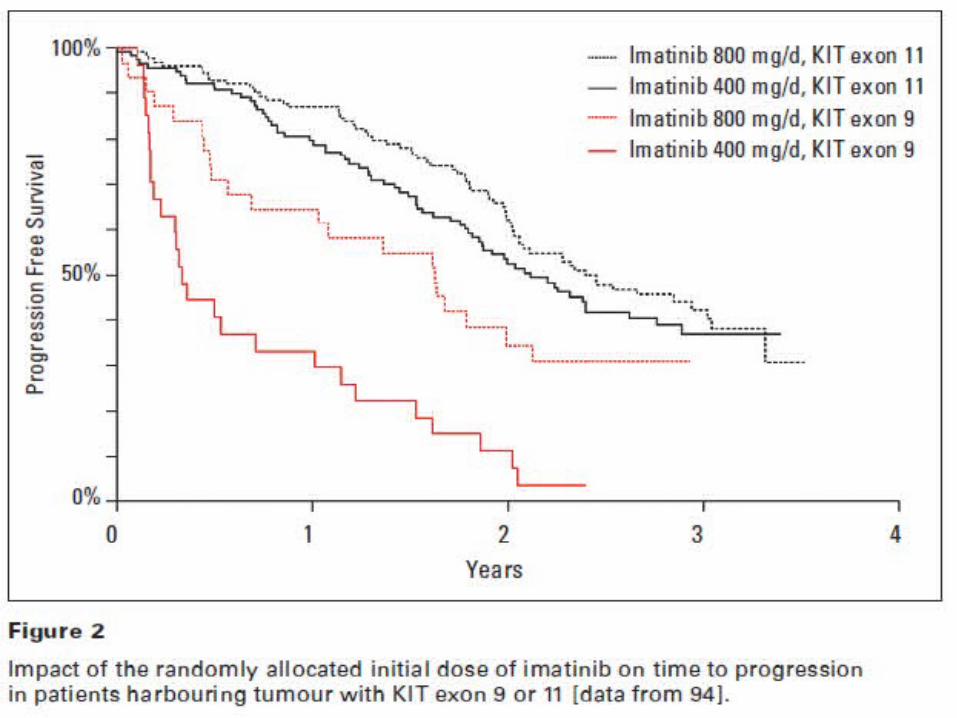
Mutational status is useful in predicting treatment response in the metastatic setting4,5
?applicable in the adjuvant setting
1. Fletcher CD et al. Hum Pathol. 2002;33:459-465.2. Demetri GD et al. J Natl Compr Cancer Netw. 2007;5(suppl 2):S1-S29.3. Miettinen M, Lasota J. Arch Pathol Lab Med. 2006;130:1466-1478. 4. Debiec-Rychter M et al. Eur J Cancer. 2006;42:1093-1103. 5. Heinrich MC et al. J Clin Oncol. 2003;21:4342-4349.
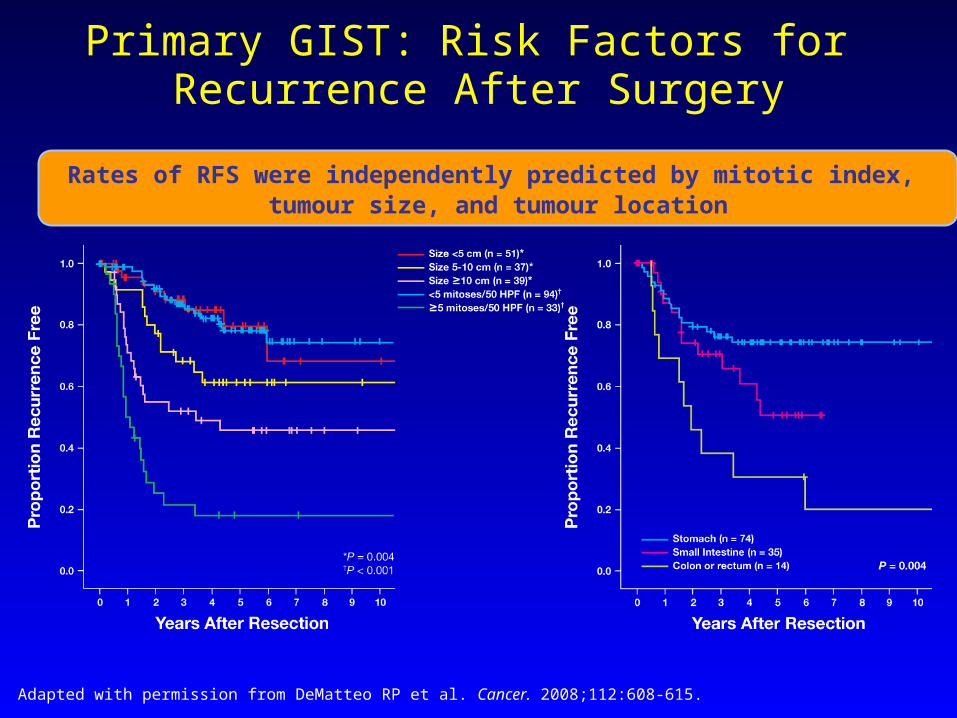
Primary GIST: Risk Factors for Recurrence After Surgery
Adapted with permission from DeMatteo RP et al. Cancer. 2008;112:608-615.
Rates of RFS were independently predicted by mitotic index, tumour size, and tumour location
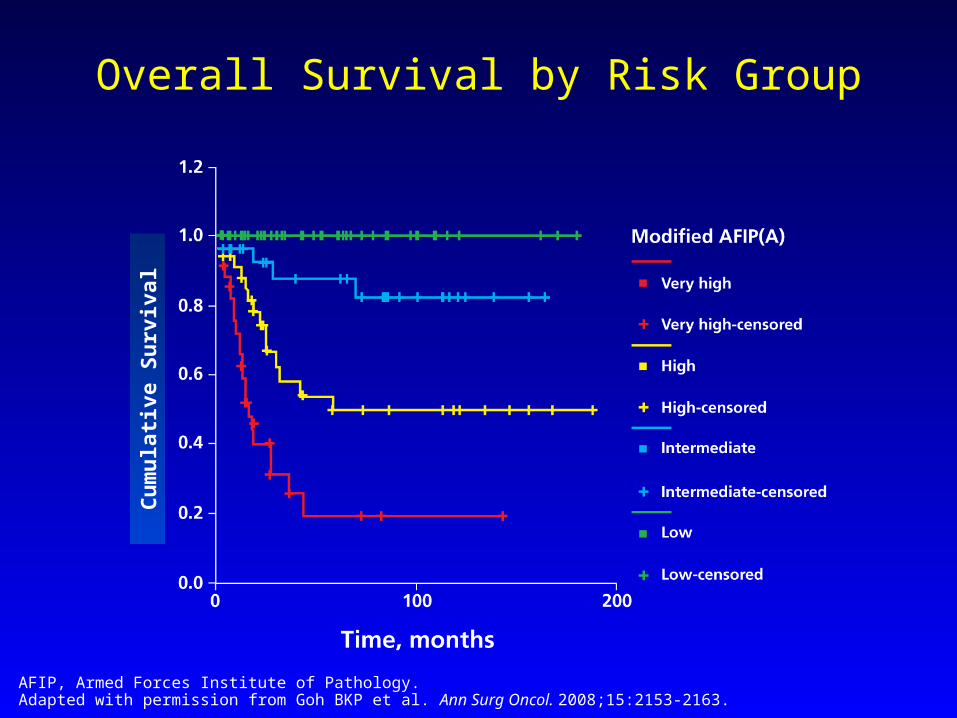
Overall Survival by Risk Group
AFIP, Armed Forces Institute of Pathology.Adapted with permission from Goh BKP et al. Ann Surg Oncol. 2008;15:2153-2163.
Cum
ulat
ive
Surv
ival
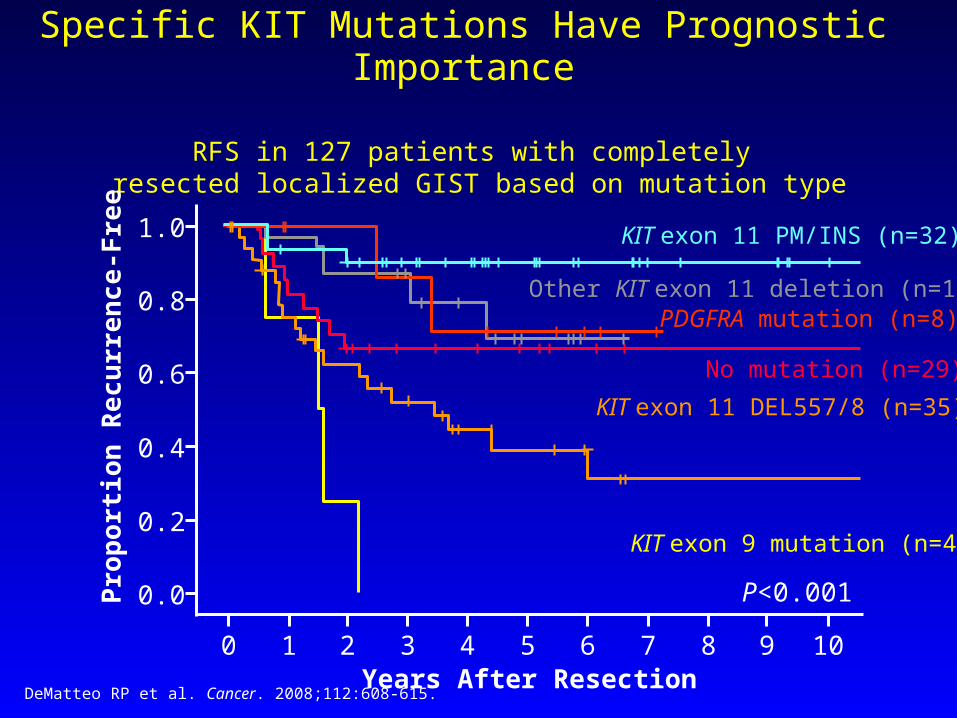
Specific KIT Mutations Have Prognostic Importance
RFS in 127 patients with completely resected localized GIST based on mutation type
Prop
ortio
n R
ecur
renc
e-Fr
ee
Years After Resection
1.0
0.8
0.6
0.4
0.2
0.0
0 1 2 3 4 5 6 7 8 9 10
P<0.001
KIT exon 9 mutation (n=4)
KIT exon 11 DEL557/8 (n=35)No mutation (n=29)
KIT exon 11 PM/INS (n=32)
Other KIT exon 11 deletion (n=17)PDGFRA mutation (n=8)
DeMatteo RP et al. Cancer. 2008;112:608-615.
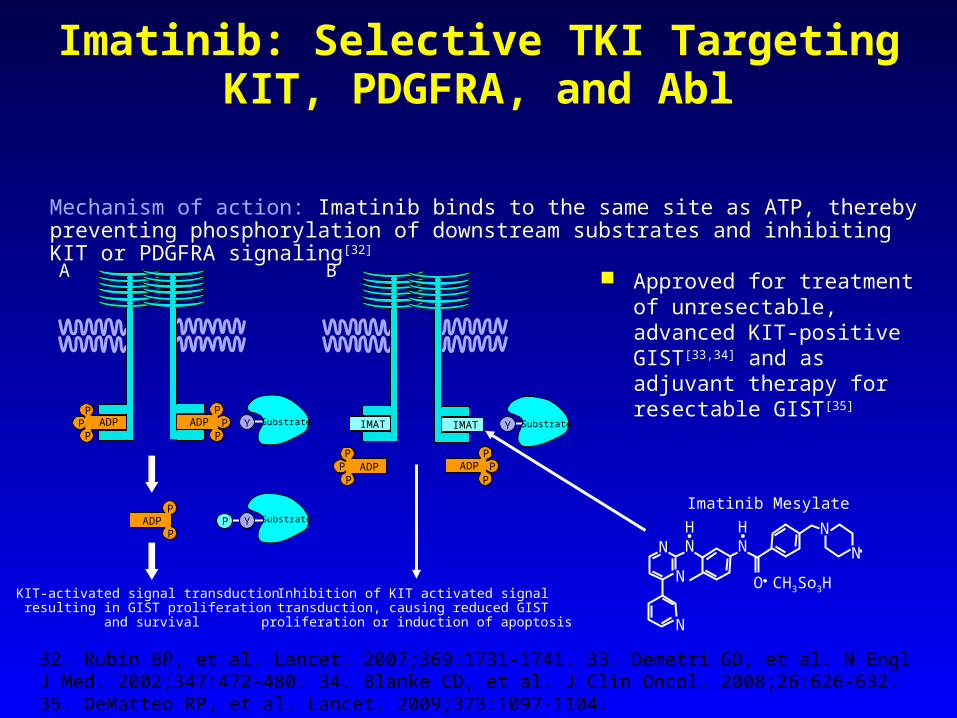
Imatinib: Selective TKI Targeting KIT, PDGFRA, and Abl
Approved for treatment of unresectable, advanced KIT-positive GIST[33,34] and as adjuvant therapy for resectable GIST[35]
32. Rubin BP, et al. Lancet. 2007;369:1731-1741. 33. Demetri GD, et al. N Engl J Med. 2002;347:472-480. 34. Blanke CD, et al. J Clin Oncol. 2008;26:626-632. 35. DeMatteo RP, et al. Lancet. 2009;373:1097-1104.
Mechanism of action: Imatinib binds to the same site as ATP, thereby preventing phosphorylation of downstream substrates and inhibiting KIT or PDGFRA signaling [32]
Imatinib Mesylate
N
N
N
HN
HN
NN
O CH3So3HInhibition of KIT activated signal transduction, causing reduced GIST proliferation or induction of apoptosis
KIT-activated signal transduction resulting in GIST proliferation
and survival
P
PADP P Y Substrate
ADPP
PP
IMATY SubstrateADPADPP
PP
P
PP
A B
IMAT
ADPP
PP
Y Substrate
Επικουρική θεραπεία
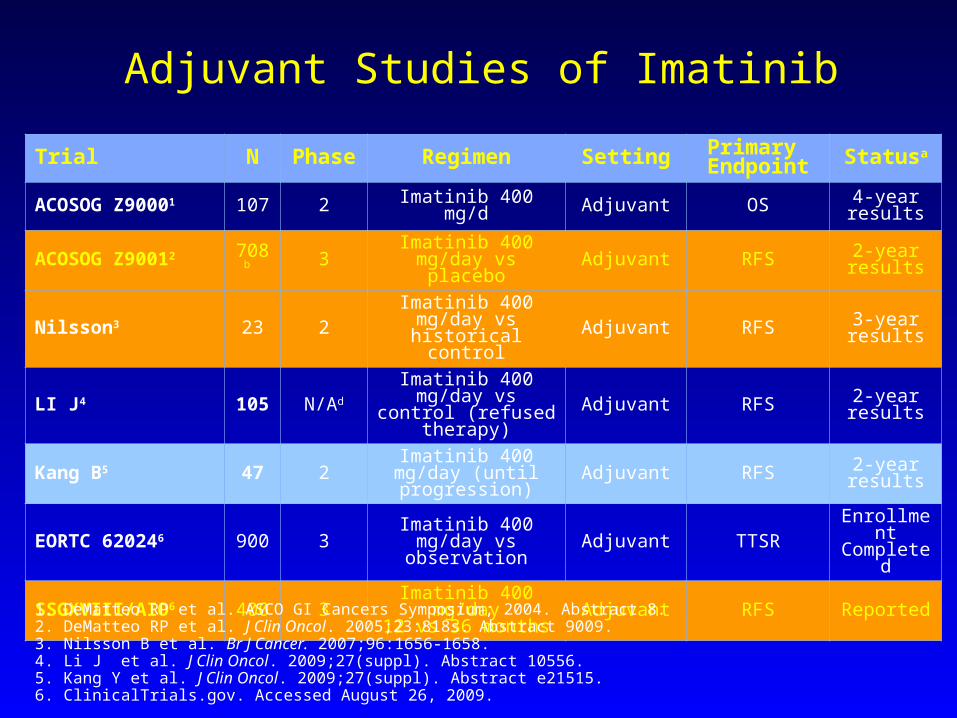
Adjuvant Studies of Imatinib
Trial N Phase Regimen Setting Primary Endpoint Statusa
ACOSOG Z90001 107 2 Imatinib 400 mg/d Adjuvant OS 4-year results
ACOSOG Z90012 708b 3 Imatinib 400 mg/day vs placebo Adjuvant RFS 2-year
results
Nilsson3 23 2 Imatinib 400 mg/day vs historical control Adjuvant RFS 3-year
results
LI J4 105 N/AdImatinib 400 mg/day vs control (refused
therapy)Adjuvant RFS 2-year
results
Kang B5 47 2 Imatinib 400 mg/day (until progression) Adjuvant RFS 2-year
results
EORTC 620246 900 3 Imatinib 400 mg/day vs observation Adjuvant TTSR Enrollment
Completed
SSGXVIII/AIO6 400 3 Imatinib 400 mg/day12 vs 36 months Adjuvant RFS Reported
1. DeMatteo RP et al. ASCO GI Cancers Symposium; 2004. Abstract 8. 2. DeMatteo RP et al. J Clin Oncol. 2005;23:818s. Abstract 9009. 3. Nilsson B et al. Br J Cancer. 2007;96:1656-1658. 4. Li J et al. J Clin Oncol. 2009;27(suppl). Abstract 10556. 5. Kang Y et al. J Clin Oncol. 2009;27(suppl). Abstract e21515. 6. ClinicalTrials.gov. Accessed August 26, 2009.
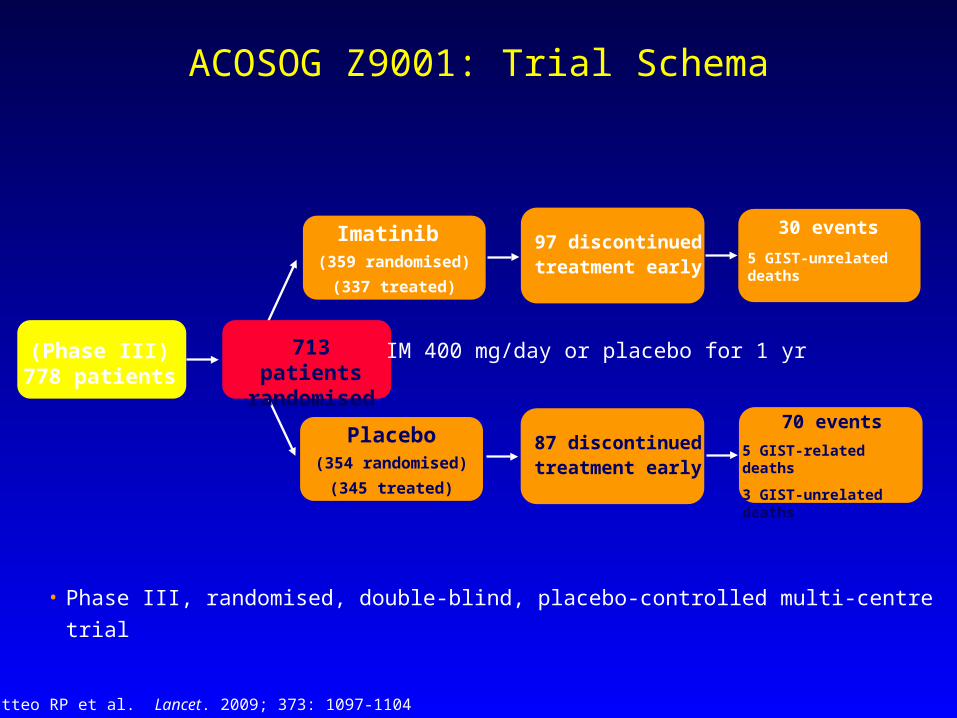
ACOSOG Z9001: Trial Schema
(Phase III)778 patients
Placebo(354 randomised)
(345 treated)
87 discontinued treatment early
Imatinib (359 randomised)
(337 treated)
97 discontinued treatment early
30 events5 GIST-unrelated deaths
713 patients randomised
• Phase III, randomised, double-blind, placebo-controlled multi-centre trial
IM 400 mg/day or placebo for 1 yr
70 events5 GIST-related deaths
3 GIST-unrelated deaths
DeMatteo RP et al. Lancet. 2009; 373: 1097-1104
ACOSOG Z9001: Study Design/Methods
Key Eligibility Criteria:• Patients ≥18 years with localised and primary GIST• KIT-positive tumours ≥3 cm• Complete surgical resection
Endpoints:• Primary: Recurrence-free Survival (RFS)• Secondary: Overall Survival (OS) and safety
Other Key Elements:• Dose modifications upon grade 3 or 4 events• PD patients unblinded:
- If placebo IM 400 mg/day or- If IM 400 mg/day IM 800 mg/day
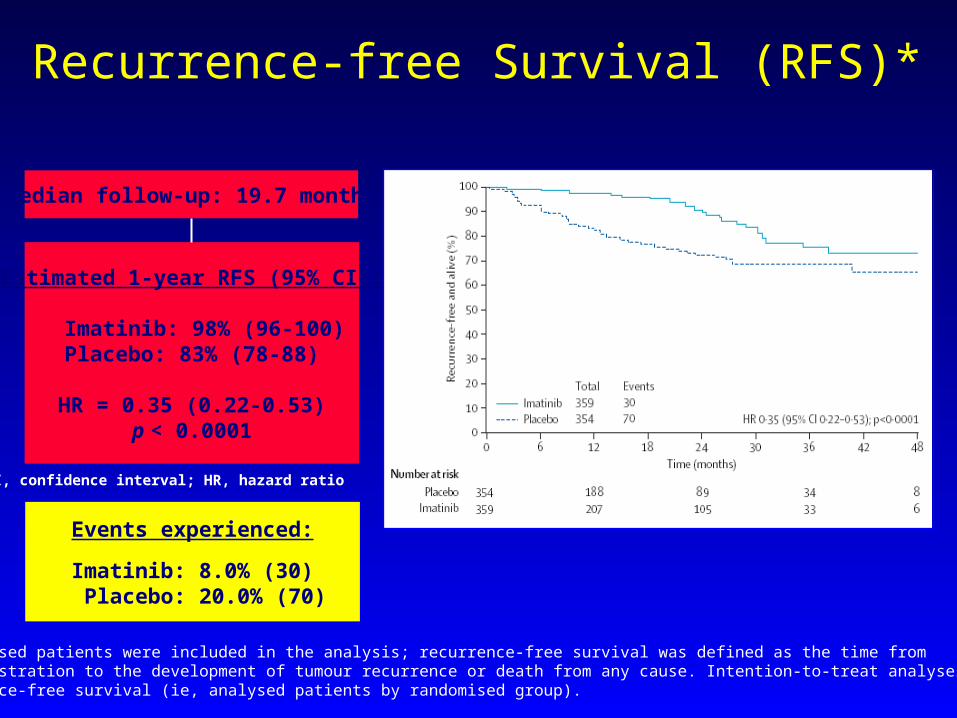
Median follow-up: 19.7 months
Estimated 1-year RFS (95% CI):
Imatinib: 98% (96-100)Placebo: 83% (78-88)
HR = 0.35 (0.22-0.53)p < 0.0001
CI, confidence interval; HR, hazard ratio
Events experienced:
Imatinib: 8.0% (30) Placebo: 20.0% (70)
Recurrence-free Survival (RFS)*
*All randomised patients were included in the analysis; recurrence-free survival was defined as the time frompatient registration to the development of tumour recurrence or death from any cause. Intention-to-treat analyses were done for recurrence-free survival (ie, analysed patients by randomised group).
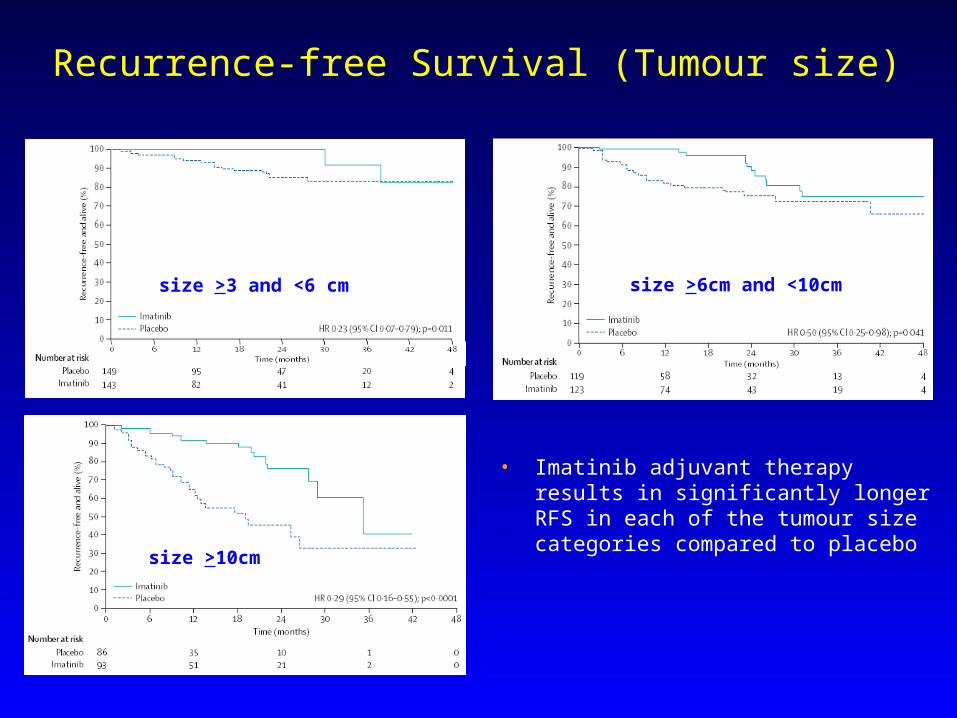
• Imatinib adjuvant therapy results in significantly longer RFS in each of the tumour size categories compared to placebo
Recurrence-free Survival (Tumour size)
size >10cm
size >3 and <6 cm size >6cm and <10cm
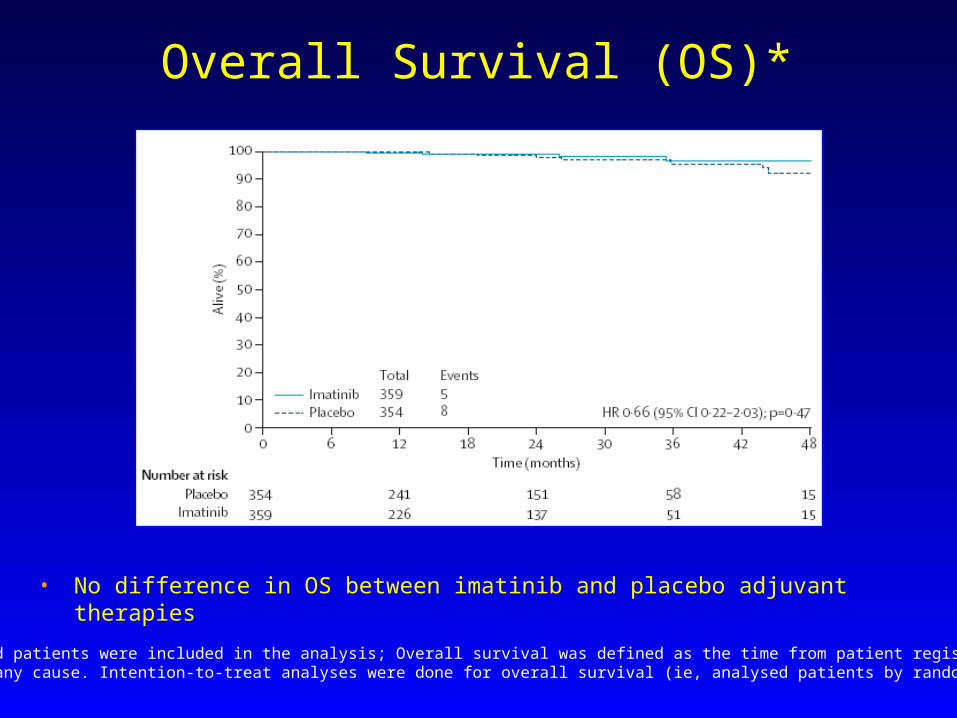
• No difference in OS between imatinib and placebo adjuvant therapies
Overall Survival (OS)*
*All randomised patients were included in the analysis; Overall survival was defined as the time from patient registration to death from any cause. Intention-to-treat analyses were done for overall survival (ie, analysed patients by randomised group).
Imatinib at 400 mg/day is safe and well tolerated when administered as adjuvant therapy after complete resection of primary GIST
Adjuvant imatinib resulted in an improvement in RFS in patients with all tumour sizes
- Especially relevant for high-risk patients (e.g. tumour size ≥10 cm or high mitotic rate) since this patient population has a 50% higher chance of recurrence at 2 years without adjuvant therapy
OS between imatinib and placebo groups comparable at this time A longer follow-up period is likely required to observe differences
Ongoing trials in the adjuvant setting are under way to determine appropriate treatment duration of imatinib and impact on OS
– SSGXVIII/AIO – EORTC 62024
Summary
Adjuvant Imatinib: Beyond 1 Year of Treatment
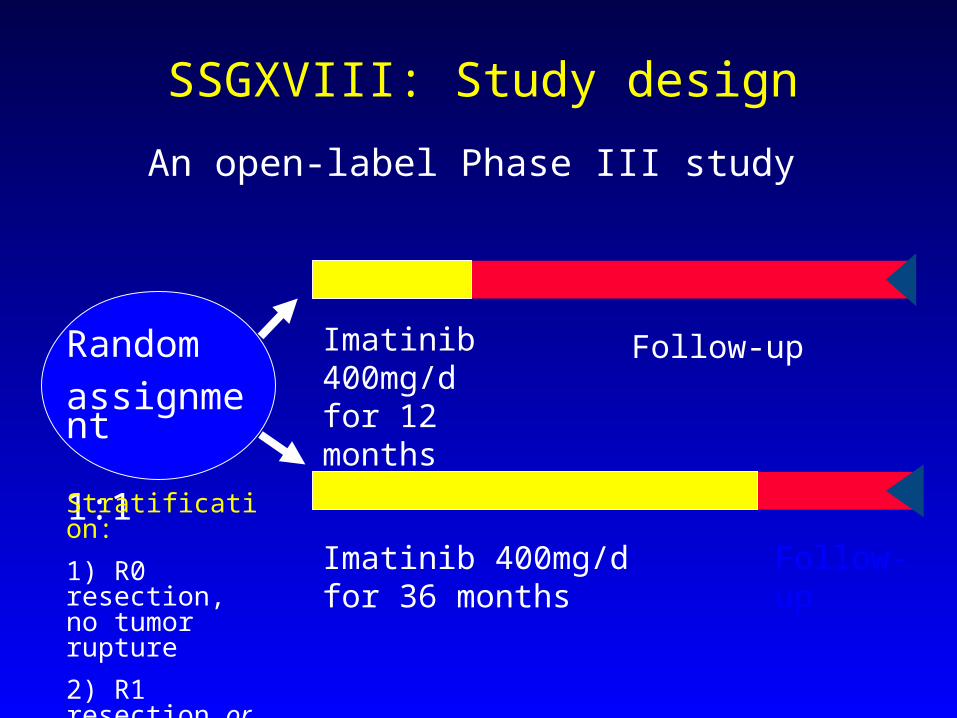
Imatinib 400mg/d for 12 months
An open-label Phase III study
Imatinib 400mg/d for 36 months
Follow-up
Follow-up
SSGXVIII: Study design
Randomassignment 1:1Stratification: 1) R0 resection, no tumor rupture 2) R1 resection or tumor rupture
SSGXVIII: Objectives
Primary: RFS
Time from randomization to GIST recurrence or death
Secondary objectives included:
SafetyOverall survival
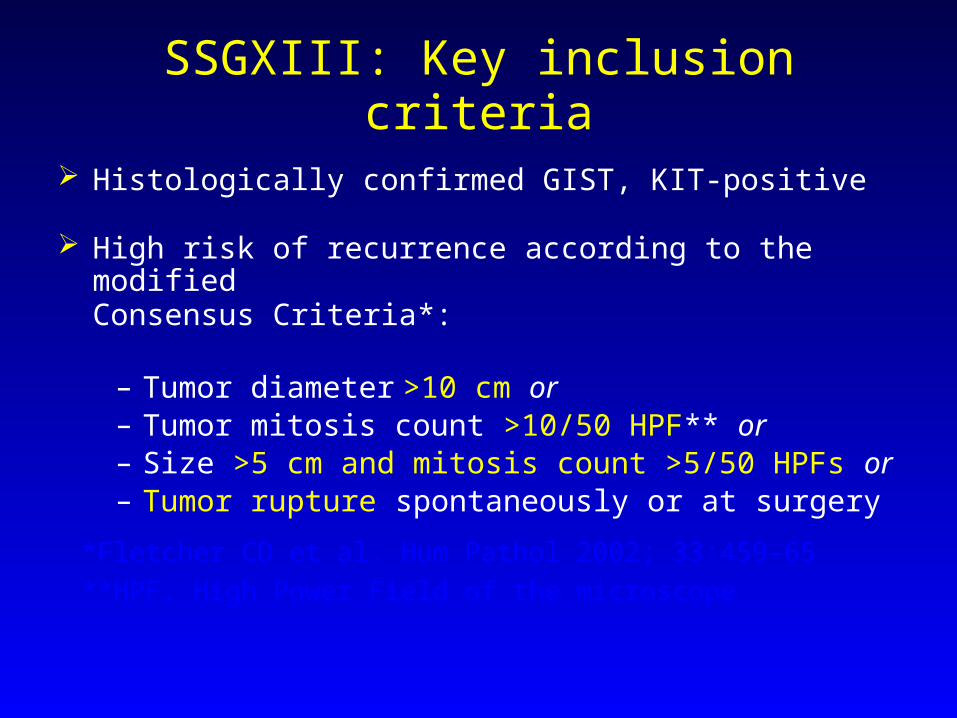
SSGXIII: Key inclusion criteria
Histologically confirmed GIST, KIT-positive
High risk of recurrence according to the modified Consensus Criteria*:
– Tumor diameter >10 cm or – Tumor mitosis count >10/50 HPF** or – Size >5 cm and mitosis count >5/50 HPFs or– Tumor rupture spontaneously or at surgery
*Fletcher CD et al. Hum Pathol 2002; 33:459-65 **HPF, High Power Field of the microscope
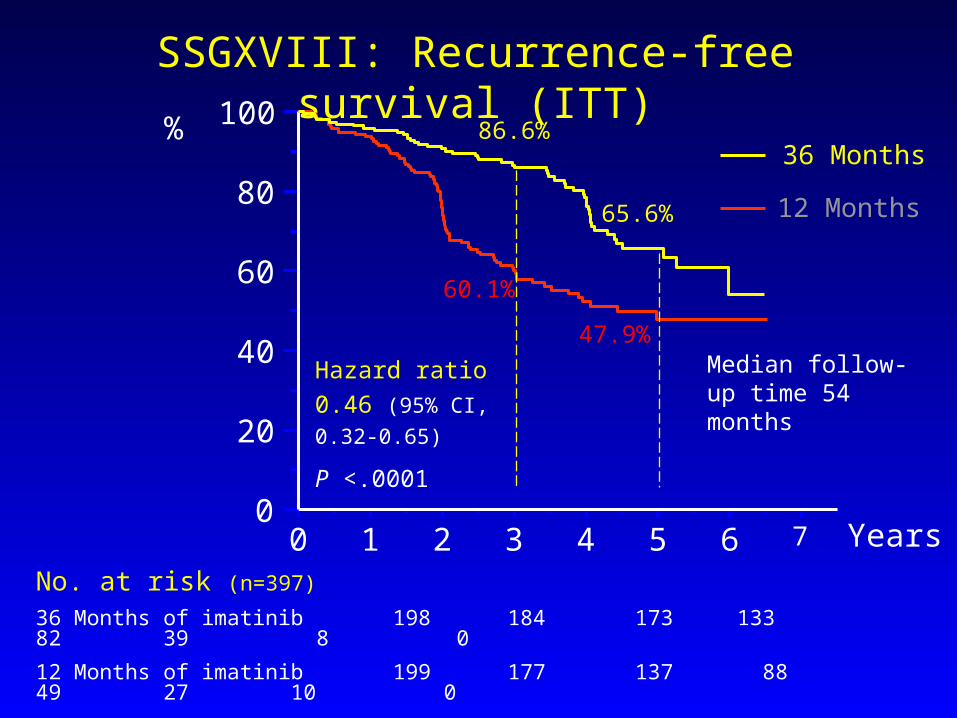
SSGXVIII: Recurrence-free survival (ITT)
No. at risk (n=397)
36 Months of imatinib 198 184 173 133 82 39 8 0 12 Months of imatinib 199 177 137 88 49 27 10 0
60.1%
47.9%
86.6%
65.6%
36 Months
12 Months
Hazard ratio 0.46 (95% CI, 0.32-0.65)
P <.0001
0 1 2 3 4 5 6 70
20
40
60
80
100%
Median follow-up time 54 months
Years
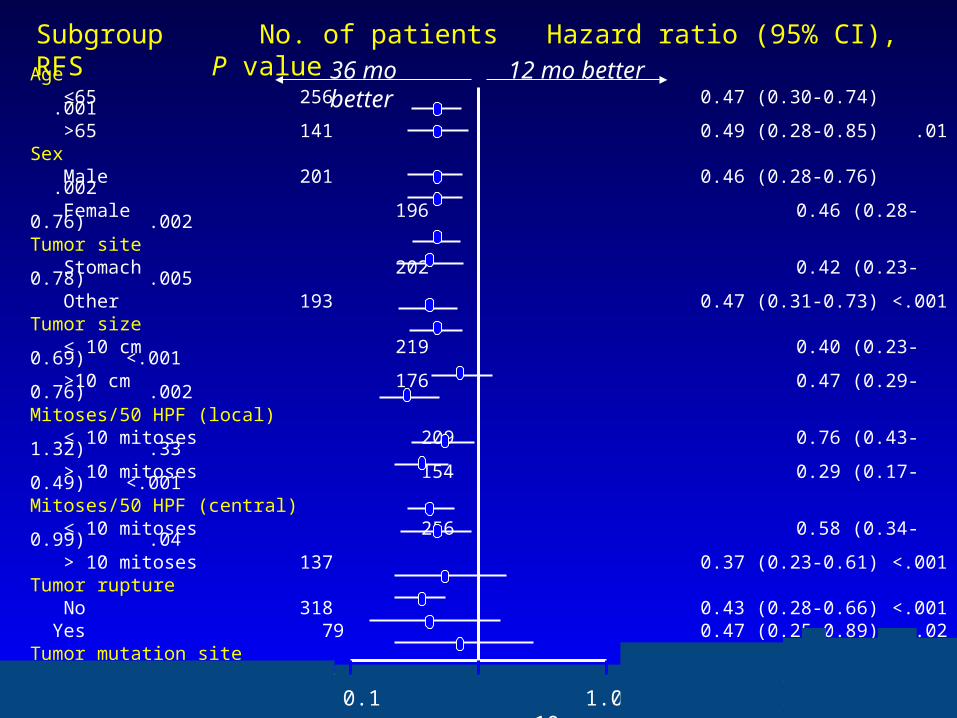
Subgroup No. of patients Hazard ratio (95% CI), RFS P valueAge ≤65 256 0.47 (0.30-0.74) .001 >65 141 0.49 (0.28-0.85) .01Sex Male 201 0.46 (0.28-0.76) .002 Female 196 0.46 (0.28-0.76) .002Tumor site Stomach 202 0.42 (0.23-0.78) .005 Other 193 0.47 (0.31-0.73) <.001Tumor size ≤ 10 cm 219 0.40 (0.23-0.69) <.001 >10 cm 176 0.47 (0.29-0.76) .002Mitoses/50 HPF (local) ≤ 10 mitoses 209 0.76 (0.43-1.32) .33 > 10 mitoses 154 0.29 (0.17-0.49) <.001Mitoses/50 HPF (central) ≤ 10 mitoses 256 0.58 (0.34-0.99) .04 > 10 mitoses 137 0.37 (0.23-0.61) <.001Tumor rupture No 318 0.43 (0.28-0.66) <.001 Yes 79 0.47 (0.25-0.89) .02Tumor mutation site KIT exon 9 26 0.61 (0.22-1.68) .34 KIT exon 11 256 0.35 (0.22-0.56) <.001 Wild type 33 0.41 (0.11-1.51) .16 Other 51 0.78 (0.22-2.78) .70
0.1 1.0 10
36 mo better 12 mo better
0.1 1.0 10
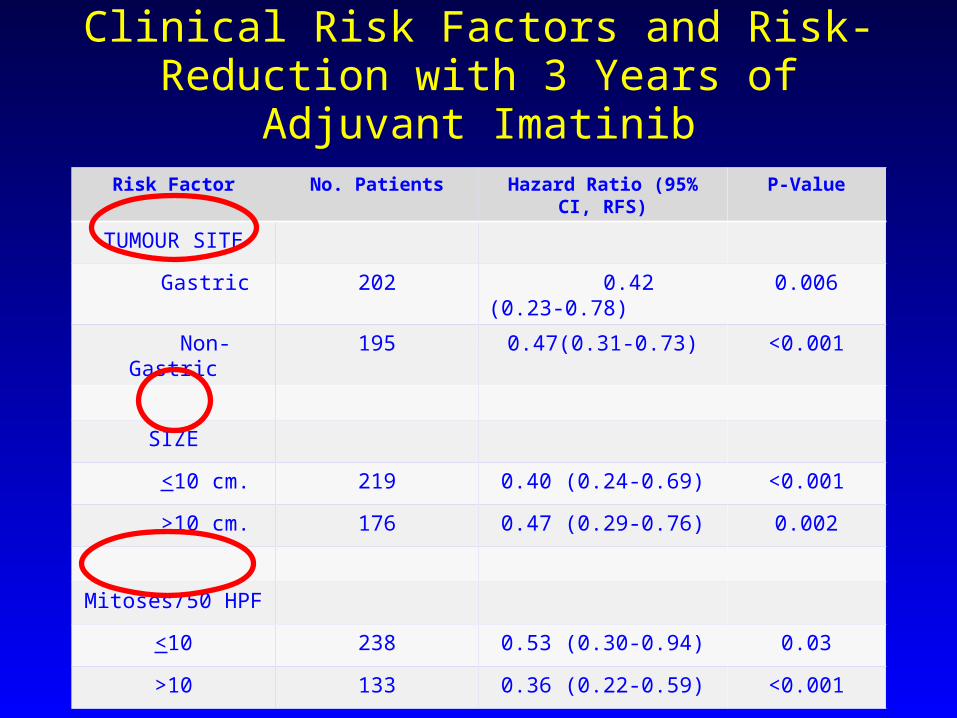
Clinical Risk Factors and Risk-Reduction with 3 Years of Adjuvant Imatinib
Risk Factor No. Patients Hazard Ratio (95% CI, RFS)
P-Value
TUMOUR SITE
Gastric 202 0.42 (0.23-0.78) 0.006
Non-Gastric 195 0.47(0.31-0.73) <0.001
SIZE
<10 cm. 219 0.40 (0.24-0.69) <0.001
>10 cm. 176 0.47 (0.29-0.76) 0.002
Mitoses/50 HPF
<10 238 0.53 (0.30-0.94) 0.03
>10 133 0.36 (0.22-0.59) <0.001
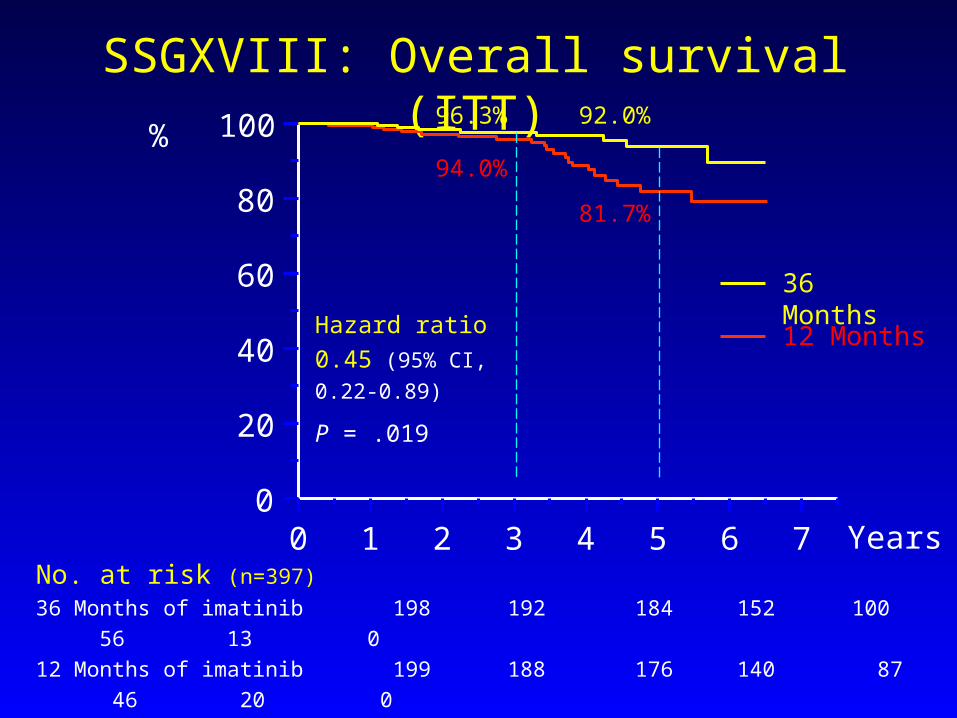
No. at risk (n=397)36 Months of imatinib 198 192 184 152 100 56 13 0 12 Months of imatinib 199 188 176 140 87 46 20 0
SSGXVIII: Overall survival (ITT)
Hazard ratio 0.45 (95% CI, 0.22-0.89)
P = .019
96.3% 92.0%
94.0%
81.7%
36 Months
12 Months
0 1 2 3 4 5 6 70
20
40
60
80
100%
Years
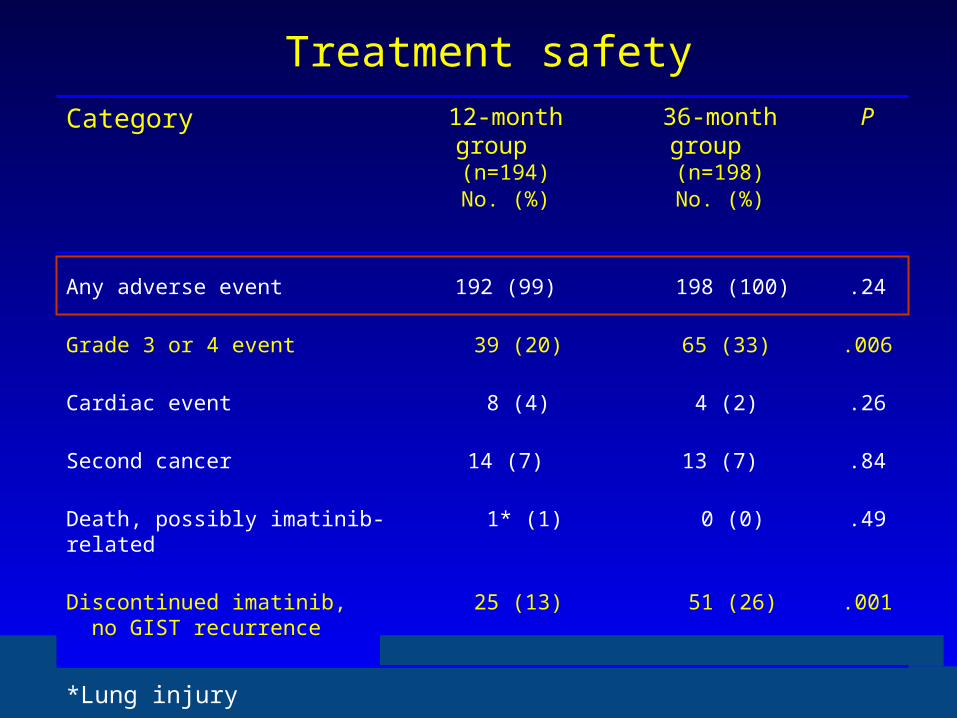
Treatment safetyCategory 12-month group
(n=194)No. (%)
36-month group (n=198)No. (%)
P
Any adverse event 192 (99) 198 (100) .24
Grade 3 or 4 event 39 (20) 65 (33) .006
Cardiac event 8 (4) 4 (2) .26
Second cancer 14 (7) 13 (7) .84
Death, possibly imatinib-related 1* (1) 0 (0) .49
Discontinued imatinib, no GIST recurrence
25 (13) 51 (26) .001
*Lung injury
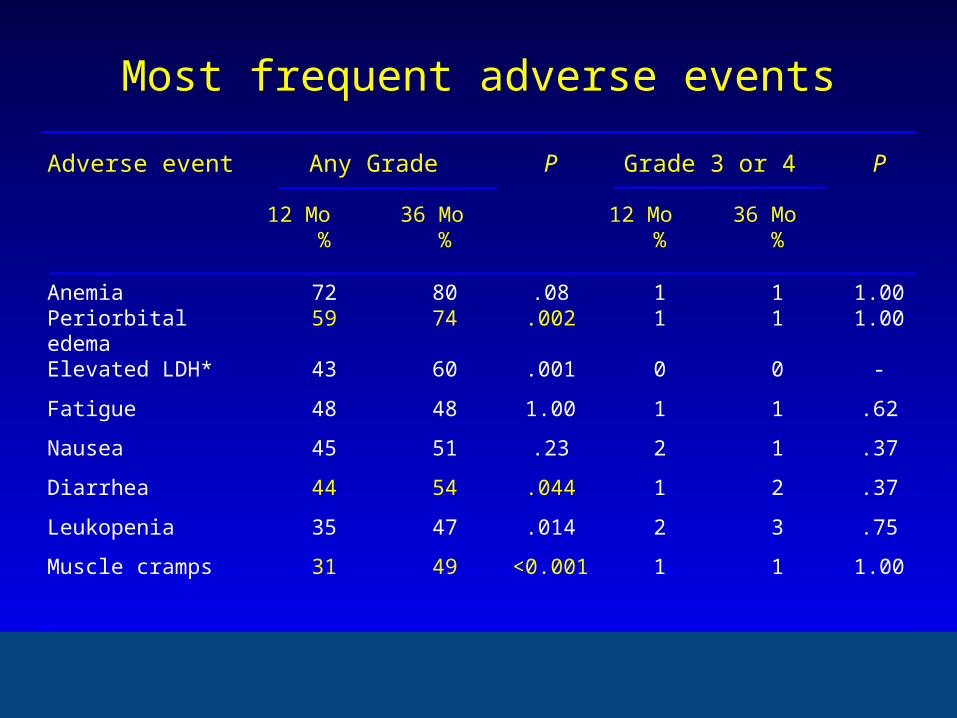
Most frequent adverse events
Adverse event Any Grade P Grade 3 or 4 P
12 Mo % 36 Mo % 12 Mo % 36 Mo %
Anemia 72 80 .08 1 1 1.00Periorbital edema 59 74 .002 1 1 1.00
Elevated LDH* 43 60 .001 0 0 -
Fatigue 48 48 1.00 1 1 .62
Nausea 45 51 .23 2 1 .37
Diarrhea 44 54 .044 1 2 .37
Leukopenia 35 47 .014 2 3 .75
Muscle cramps 31 49 <0.001 1 1 1.00
Conclusions
Compared to 1 year of adjuvant imatinib, 3 years of imatinib improves
- RFS - Overall survival
as treatment of GIST patients who have a high estimated risk of recurrence after surgery.
Adjuvant imatinib is relatively well tolerated; severe adverse events are infrequent.
Θεραπεία προχωρημένης νόσου
Beyond imatinib
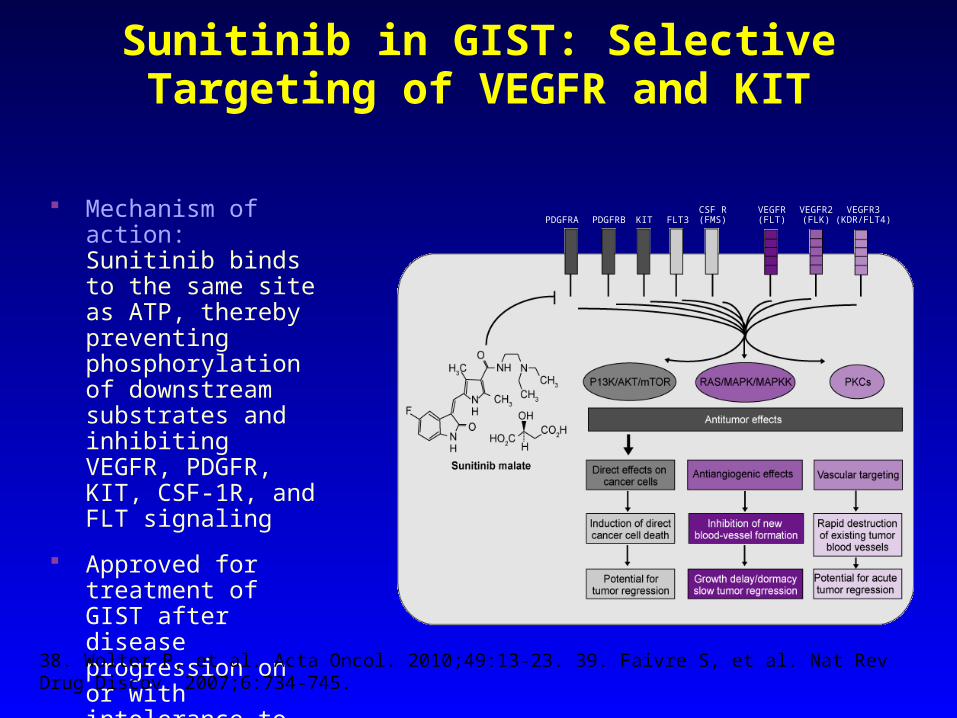
Sunitinib in GIST: Selective Targeting of VEGFR and KIT
Mechanism of action: Sunitinib binds to the same site as ATP, thereby preventing phosphorylation of downstream substrates and inhibiting VEGFR, PDGFR, KIT, CSF-1R, and FLT signaling
Approved for treatment of GIST after disease progression on or with intolerance to imatinib
38. Wolter P, et al. Acta Oncol. 2010;49:13-23. 39. Faivre S, et al. Nat Rev Drug Discov. 2007;6:734-745.
PDGFRA PDGFRB KIT FLT3CSF R(FMS)
VEGFR(FLT)
VEGFR2(FLK)
VEGFR3(KDR/FLT4)
Andrea Eva Neal
include a spell out for PKC?
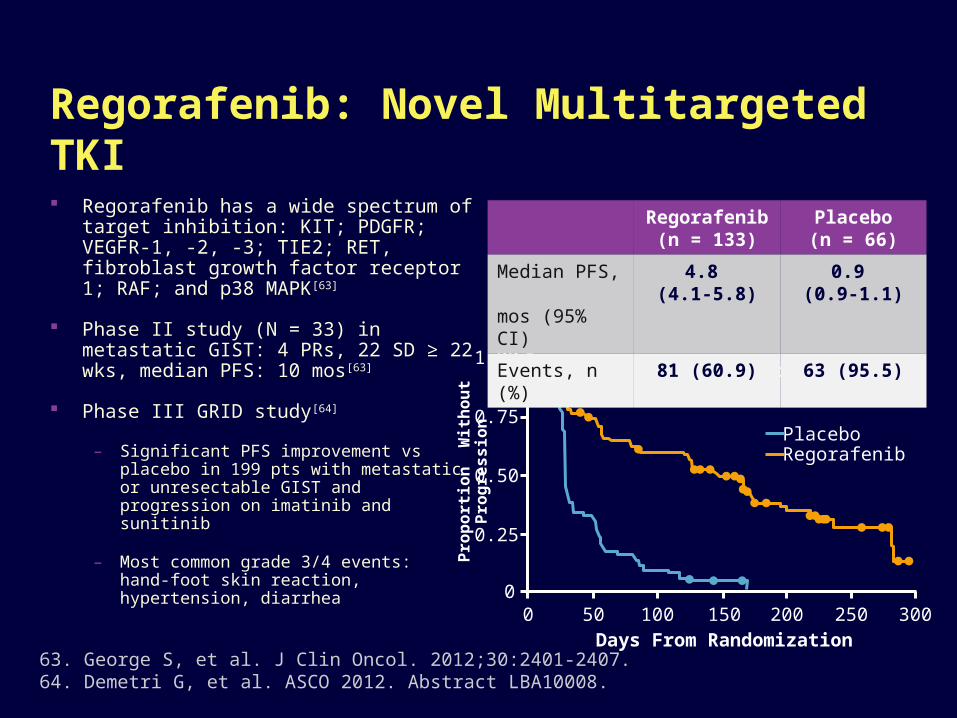
Regorafenib: Novel Multitargeted TKI Regorafenib has a wide spectrum of
target inhibition: KIT; PDGFR; VEGFR-1, -2, -3; TIE2; RET, fibroblast growth factor receptor 1; RAF; and p38 MAPK[63]
Phase II study (N = 33) in metastatic GIST: 4 PRs, 22 SD ≥ 22 wks, median PFS: 10 mos[63]
Phase III GRID study[64]
– Significant PFS improvement vs placebo in 199 pts with metastatic or unresectable GIST and progression on imatinib and sunitinib
– Most common grade 3/4 events:hand-foot skin reaction, hypertension, diarrhea
63. George S, et al. J Clin Oncol. 2012;30:2401-2407.64. Demetri G, et al. ASCO 2012. Abstract LBA10008.
Prop
ortio
n W
ithou
t Pro
gres
sion 1.00
0.75
0.50
0.25
00 50 100 150 200 250 300
Days From Randomization
PlaceboRegorafenib
HR: 0.27 (95% CI: 0.19-0.39)1-sided P < .0001
Regorafenib(n = 133)
Placebo(n = 66)
Median PFS, mos (95% CI)
4.8 (4.1-5.8)
0.9 (0.9-1.1)
Events, n (%) 81 (60.9) 63 (95.5)
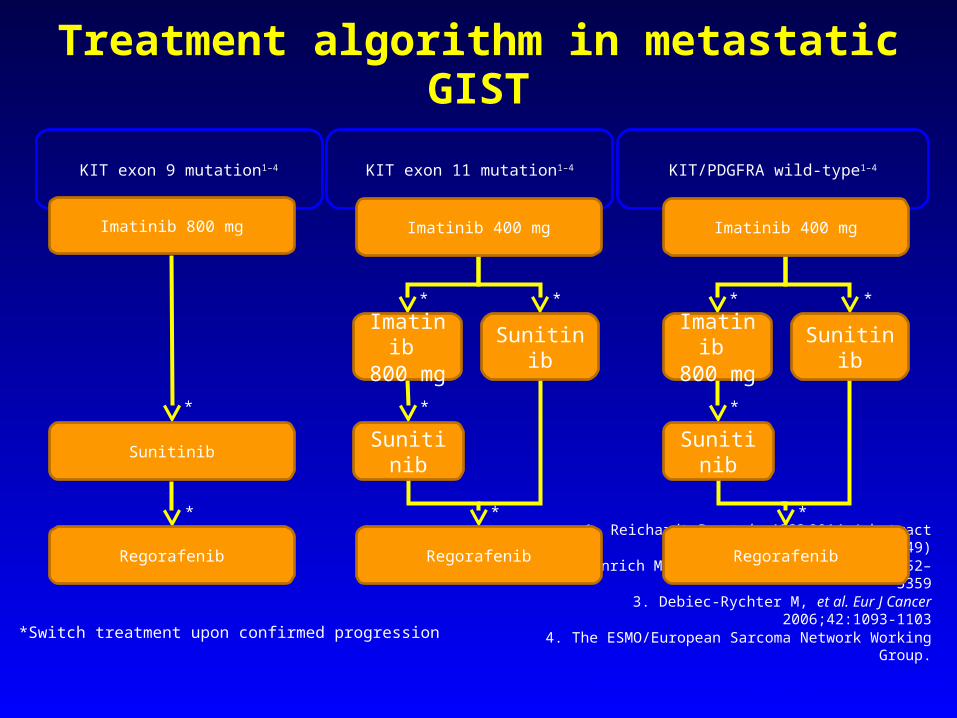
Treatment algorithm in metastatic GISTKIT exon 9 mutation1–4 KIT/PDGFRA wild-type1–4KIT exon 11 mutation1–4
1. Reichardt P, et al. ASCO 2014 (abstract 10549)2. Heinrich MC, et al. J Clin Oncol 2008;26:5352–5359
3. Debiec-Rychter M, et al. Eur J Cancer 2006;42:1093-1103
4. The ESMO/European Sarcoma Network Working Group.
Ann Oncol 2014;25 (Suppl 3): iii21–iii26
*Switch treatment upon confirmed progression
*
*
*
*
*
*
*
*
*
*
Imatinib 400 mgImatinib 800 mg Imatinib 400 mg
Imatinib 800 mg Sunitinib
Sunitinib Sunitinib
Regorafenib Regorafenib
Imatinib 800 mg
Sunitinib
Regorafenib
Sunitinib