ΔΟΡΥΦΟΡΙΚΗ ΔΙΑΛΕΞΗstatic.livemedia.gr/kebe/documents/al15435_us63... · ESC/EAS...
58
‹#› ΔΟΡΥΦΟΡΙΚΗ ΔΙΑΛΕΞΗ Αναστολή της PCSK9: νεότερα δεδομένα στην αντιμετώπιση του κινδύνου της υψηλής LDL
Transcript of ΔΟΡΥΦΟΡΙΚΗ ΔΙΑΛΕΞΗstatic.livemedia.gr/kebe/documents/al15435_us63... · ESC/EAS...
‹#›
ΔΟΡΥΦΟΡΙΚΗ ΔΙΑΛΕΞΗ
Αναστολή της PCSK9: νεότερα δεδοµένα στην αντιµετώπιση του κινδύνου της υψηλής LDL
‹#›
ΑΜΟΙΒΕΣ ΑΠΟ ΠΟΛΥΚΕΝΤΡΙΚΕΣ ΜΕΛΕΤΕΣ, HONORARIA
SERVIER, NOVARTIS, LILLY, ASTRA, SANOFI
‹#›
ESC/EAS 2011: Κατευθυντήριες οδηγίες για την διαχείριση της δυσλιπιδαιµίας
Reiner Z., et al Eur Heart J. 2011 Jul;32(14):1769-818
‹#›
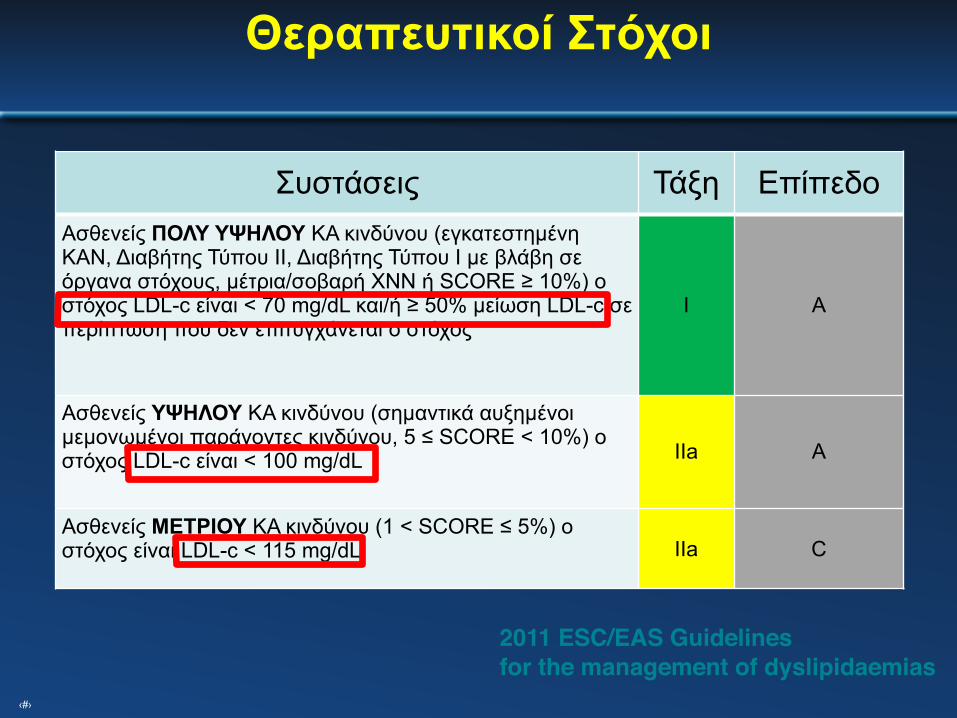
Συστάσεις Τάξη ΕπίπεδοΑσθενείς ΠΟΛΥ ΥΨΗΛΟΥ ΚΑ κινδύνου (εγκατεστηµένη ΚΑΝ, Διαβήτης Τύπου ΙΙ, Διαβήτης Τύπου Ι µε βλάβη σε όργανα στόχους, µέτρια/σοβαρή ΧΝΝ ή SCORE ≥ 10%) ο στόχος LDL-c είναι < 70 mg/dL και/ή ≥ 50% µείωση LDL-c σε περίπτωση που δεν επιτυγχάνεται ο στόχος
I Α
Ασθενείς ΥΨΗΛΟΥ ΚΑ κινδύνου (σηµαντικά αυξηµένοι µεµονωµένοι παράγοντες κινδύνου, 5 ≤ SCORE < 10%) o στόχος LDL-c είναι < 100 mg/dL IΙa A
Ασθενείς ΜΕΤΡΙΟΥ ΚΑ κινδύνου (1 < SCORE ≤ 5%) o στόχος είναι LDL-c < 115 mg/dL IIa C
Θεραπευτικοί Στόχοι
2011 ESC/EAS Guidelinesfor the management of dyslipidaemias
‹#›
‹#›
◆ Πρωταρχική λιπιδαιµική παράµετρος η LDL-C και στόχος η ισχυρή ελάττωσή της
◆ Οι κατευθυντήριες οδηγίες συνιστούν ότι πρέπει να επιτευχθεί σηµαντική µείωση της LDL-C δια µέσου υγιεινοδιαιτητικών παρεµβάσεων και θεραπείας µε στατίνες.
◆ Μη συγκεκριµένα όρια-στόχοι για κάθε κατηγορία ασθενών.
◆ Συνιστούν τη χρήση κατάλληλης δυναµικότητας / δοσολογίας στατίνης για την επίτευξη της µείωσης της LDL-C
δηλ. χρήση υψηλής ισχύος στατίνης σε υψηλού κινδύνου ασθενείς (>50% µείωση της LDL-C) ή µέτριας ισχύος στατίνη για τους ασθενείς µέτριου κινδύνου (επιθυµητή µείωση >30 –50%)
6
Τα πιο σηµαντικά σηµεία των συστάσεων ACC/AHA 2013:
http://content.onlinejacc.org/article.aspx?doi=10.1016/j.jacc.2013.11.002 http://circ.ahajournals.org/lookup/doi/10.1161/01.cir.0000437738.63853.7a
‹#›
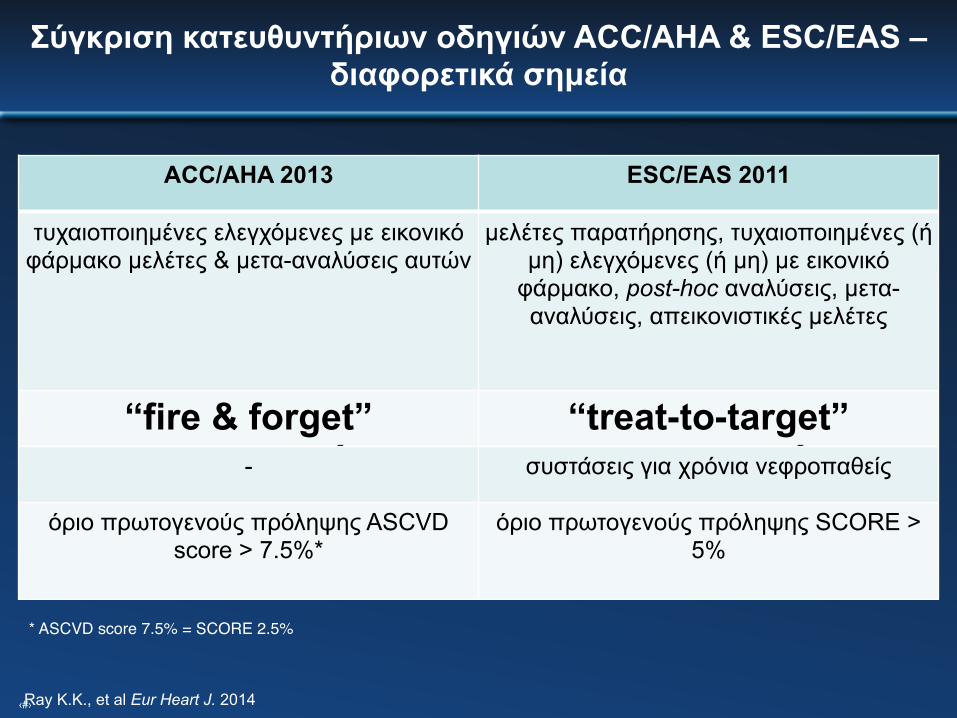
Σύγκριση κατευθυντήριων οδηγιών ACC/AHA & ESC/EAS – διαφορετικά σηµεία
ACC/AHA 2013 ESC/EAS 2011
τυχαιοποιηµένες ελεγχόµενες µε εικονικό φάρµακο µελέτες & µετα-αναλύσεις αυτών
µελέτες παρατήρησης, τυχαιοποιηµένες (ή µη) ελεγχόµενες (ή µη) µε εικονικό φάρµακο, post-hoc αναλύσεις, µετα-αναλύσεις, απεικονιστικές µελέτες
“fire & forget” στρατηγική
“treat-to-target” στρατηγική- συστάσεις για χρόνια νεφροπαθείς
όριο πρωτογενούς πρόληψης ASCVD score > 7.5%*
όριο πρωτογενούς πρόληψης SCORE > 5%
* ASCVD score 7.5% = SCORE 2.5%
Ray K.K., et al Eur Heart J. 2014
‹#›
‹#›
‹#›
Επιδηµιολογικά Δεδοµένα Tί γίνεται στη πράξη ;
‹#›
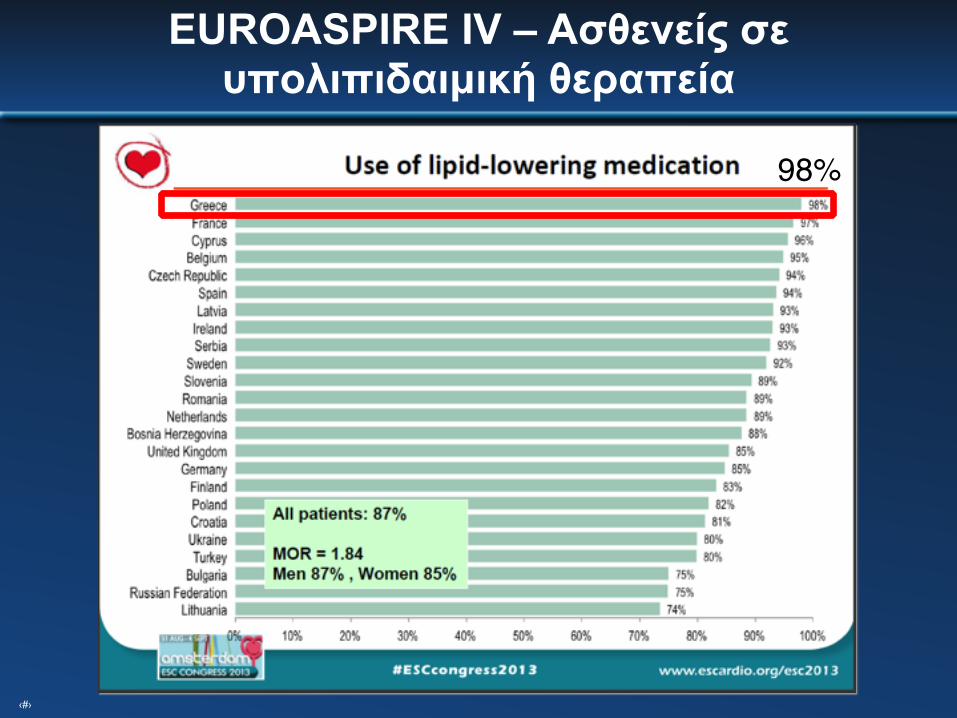
EUROASPIRE IV – Ασθενείς σε υπολιπιδαιµική θεραπεία
98%
‹#›
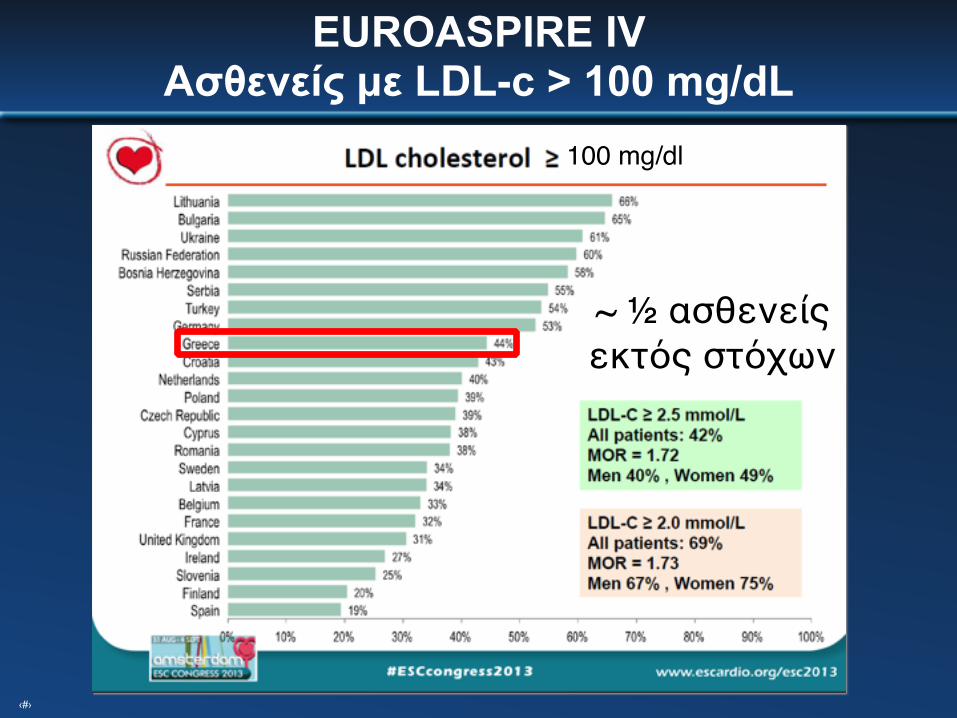
EUROASPIRE IVAσθενείς µε LDL-c > 100 mg/dL
~ ½ ασθενείς εκτός στόχων
100 mg/dl
‹#›
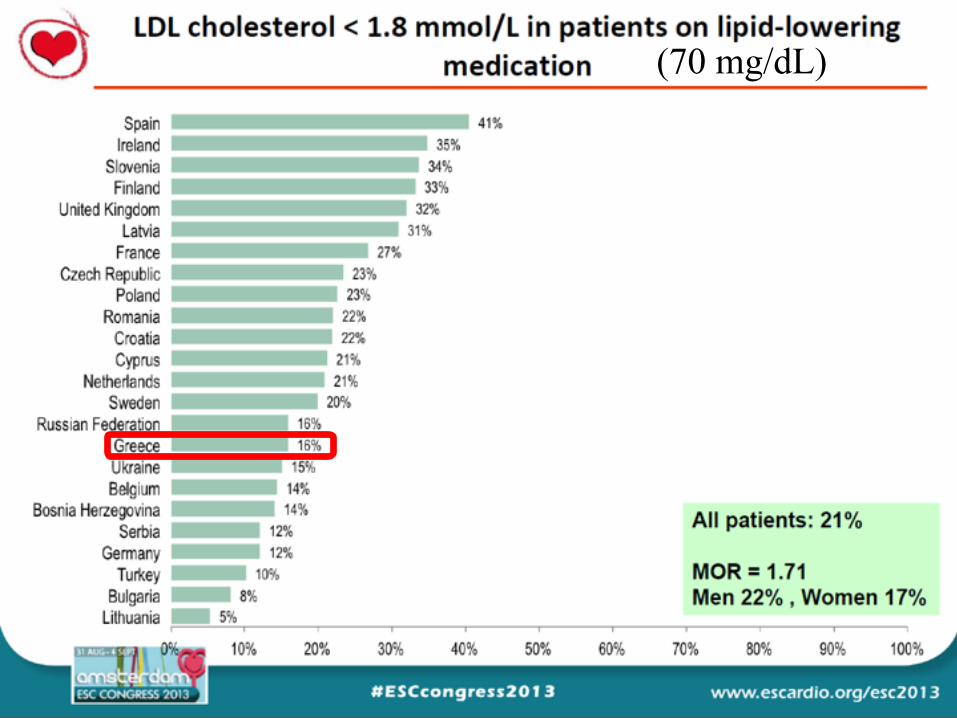
(70 mg/dL)(70 mg/dL)

‹#›
⬧ Μειωµένη συµµόρφωση των ασθενών
⬧ Ανεπιθύµητες ενέργειες (δοσοεξαρτώµενες)
⬧ Περιορισµένη αποτελεσµατικότητα της υπολιπιδαιµικής αγωγής («κανόνας του 6»)
⬧Aνεπαρκής χορήγηση συνδυασµού υπολιπιδαιµικών φαρµάκων
ΑΔΥΝΑΜΙΑ ΕΠΙΤΕΥΞΗΣ ΤΩΝ ΣΤΟΧΩΝ ΤΗΣ ΥΠΟΛΙΠΙΔΑΙΜΙΚΗΣ ΑΓΩΓΗΣ
Μονοκλωνικά Αντισώµατα
15
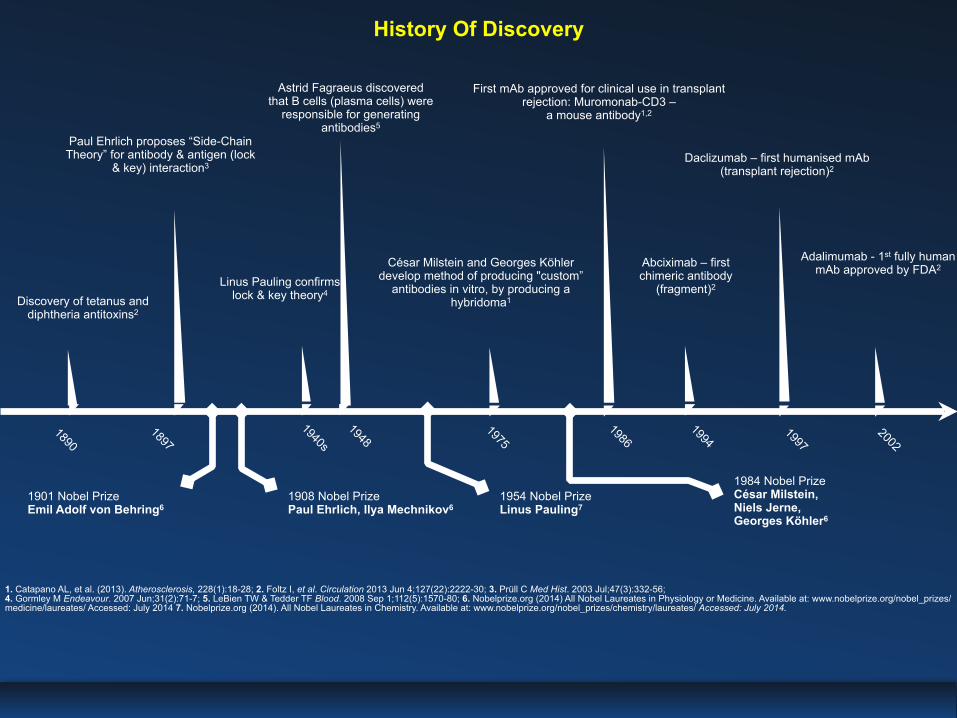
History Of Discovery
Discovery of tetanus and diphtheria antitoxins2
Paul Ehrlich proposes “Side-Chain Theory” for antibody & antigen (lock
& key) interaction3
Linus Pauling confirms lock & key theory4
Astrid Fagraeus discovered that B cells (plasma cells) were
responsible for generating antibodies5
César Milstein and Georges Köhler develop method of producing "custom”
antibodies in vitro, by producing a hybridoma1
First mAb approved for clinical use in transplant rejection: Muromonab-CD3 –
a mouse antibody1,2
Abciximab – first chimeric antibody
(fragment)2
Daclizumab – first humanised mAb (transplant rejection)2
Adalimumab - 1st fully human mAb approved by FDA2
18971890
1940s
1901 Nobel Prize Emil Adolf von Behring6
1908 Nobel Prize Paul Ehrlich, Ilya Mechnikov6
1954 Nobel Prize Linus Pauling7
1984 Nobel Prize César Milstein, Niels Jerne, Georges Köhler6
19481975
19861994
19972002
1. Catapano AL, et al. (2013). Atherosclerosis, 228(1):18-28; 2. Foltz I, et al. Circulation 2013 Jun 4;127(22):2222-30; 3. Prüll C Med Hist. 2003 Jul;47(3):332-56; 4. Gormley M Endeavour. 2007 Jun;31(2):71-7; 5. LeBien TW & Tedder TF Blood. 2008 Sep 1;112(5):1570-80; 6. Nobelprize.org (2014) All Nobel Laureates in Physiology or Medicine. Available at: www.nobelprize.org/nobel_prizes/medicine/laureates/ Accessed: July 2014 7. Nobelprize.org (2014). All Nobel Laureates in Chemistry. Available at: www.nobelprize.org/nobel_prizes/chemistry/laureates/ Accessed: July 2014.
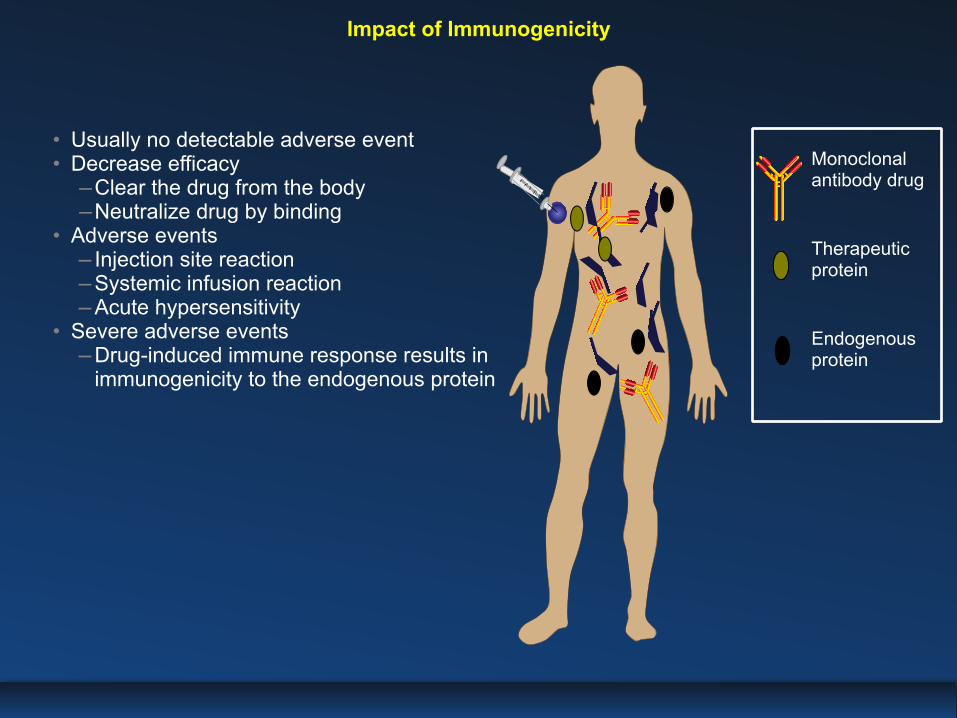
• Usually no detectable adverse event • Decrease efficacy −Clear the drug from the body −Neutralize drug by binding
• Adverse events −Injection site reaction −Systemic infusion reaction −Acute hypersensitivity
• Severe adverse events −Drug-induced immune response results in
immunogenicity to the endogenous protein
Impact of Immunogenicity
Y
YY Therapeutic
protein
Monoclonal antibody drug
Endogenous protein
YYYYY Y
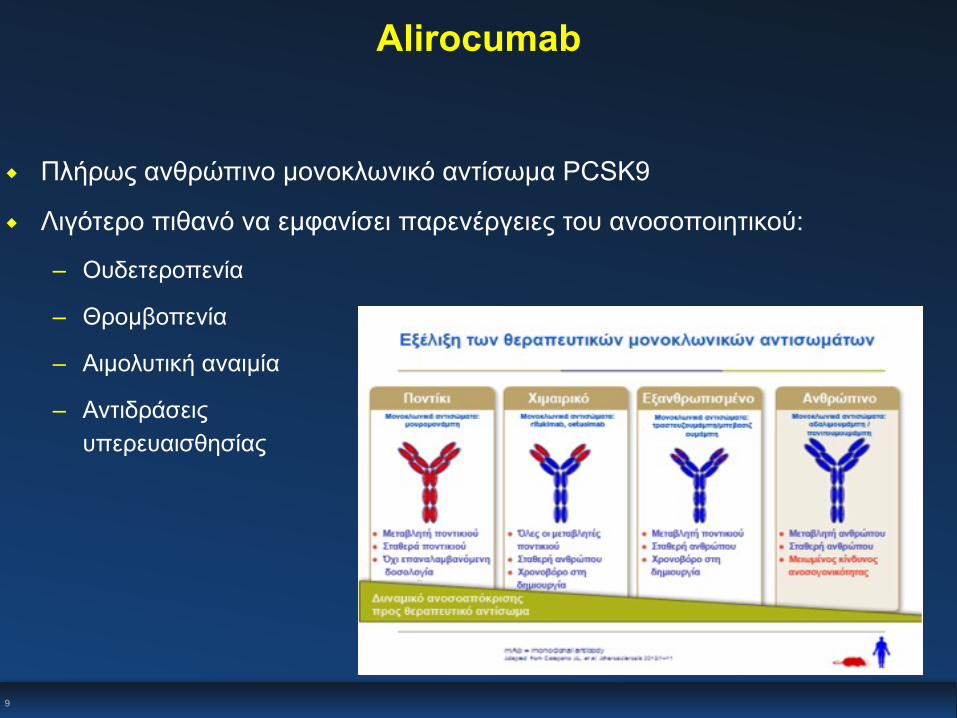
Alirocumab
◆ Πλήρως ανθρώπινο µονοκλωνικό αντίσωµα PCSK9 ◆ Λιγότερο πιθανό να εµφανίσει παρενέργειες του ανοσοποιητικού:
– Ουδετεροπενία
– Θροµβοπενία
– Αιµολυτική αναιµία
– Αντιδράσεις υπερευαισθησίας
9

‹#›
Πρώτο άτοµο που θεραπεύεται µε PCSK9 mAb (Alirocumab)
Seidah NG. Proc Natl Acad Sci USA 2003;100:928-33. Abifadel M. Nat Genet 2003;34:154-6. Maxwell KN. Proc Natl Acad Sci USA 2004;101:7100-5. Rashid S. Proc Natl Acad Sci USA 2005;102:5374-79. Cohen JC. NEJM 2006;354:1264-72. Zhao Z. Am J Hum Genet 2006;79:514-23. Hooper AJ. Atherosclerosis 2007;193:445-8. Chan JC. Proc Natl Acad Sci USA 2009;106:9820-5. Stein et al. NEJM 2012;366:1108-18. McKenney et al. JACC 2012;59:2344-53. Stein et al. Lancet 2012;380:29-36. Roth et al. NEJM 2012;367:1891-900. Giugliano et al. Lancet 2012;380:2007-17. Koren et al. Lancet 2012;380:1995-2006. Raal et al. Circulation 2012;126:2408-17. Sullivan et al. JAMA 2012:308:2497-506.
mAb που στοχεύει στο PCSK9 προκλινικάΑνακάλυψη του PCSK9
Απόδειξη της ύπαρξης του PCSK9 στα ζώα
Δηµοσίευση µελετών φάσης 2
Επικύρωση της ύπαρξης του PCSK9 στον άνθρωπο
PCSK9 - Ταχεία εξέλιξη από το εργαστήριο στην κλινική σε λιγότερο από µια δεκαετία
2000 2001 2002 2007 2008 20112003 2004 2005 2006 2009 2010 2012 2013
Πρώτα διαθέσιµα δεδοµένα µελετών φάσης 3 (ODYSSEY MONO)
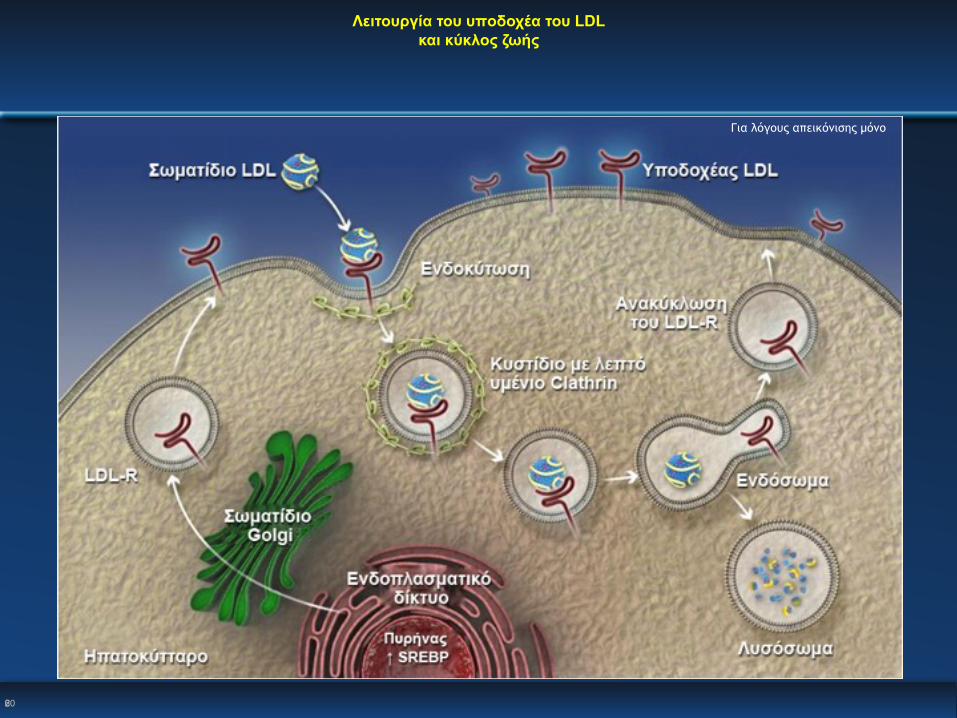
Λειτουργία του υποδοχέα του LDL και κύκλος ζωής
620
Για λόγους απεικόνισης µόνο
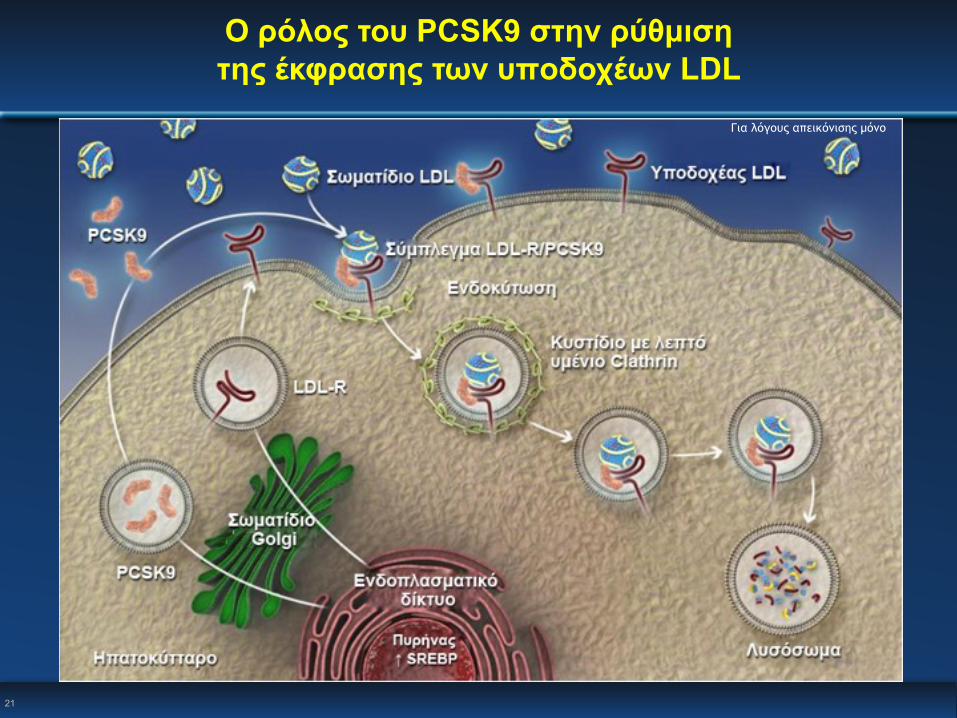
Ο ρόλος του PCSK9 στην ρύθµιση της έκφρασης των υποδοχέων LDL
Για λόγους απεικόνισης µόνο
21
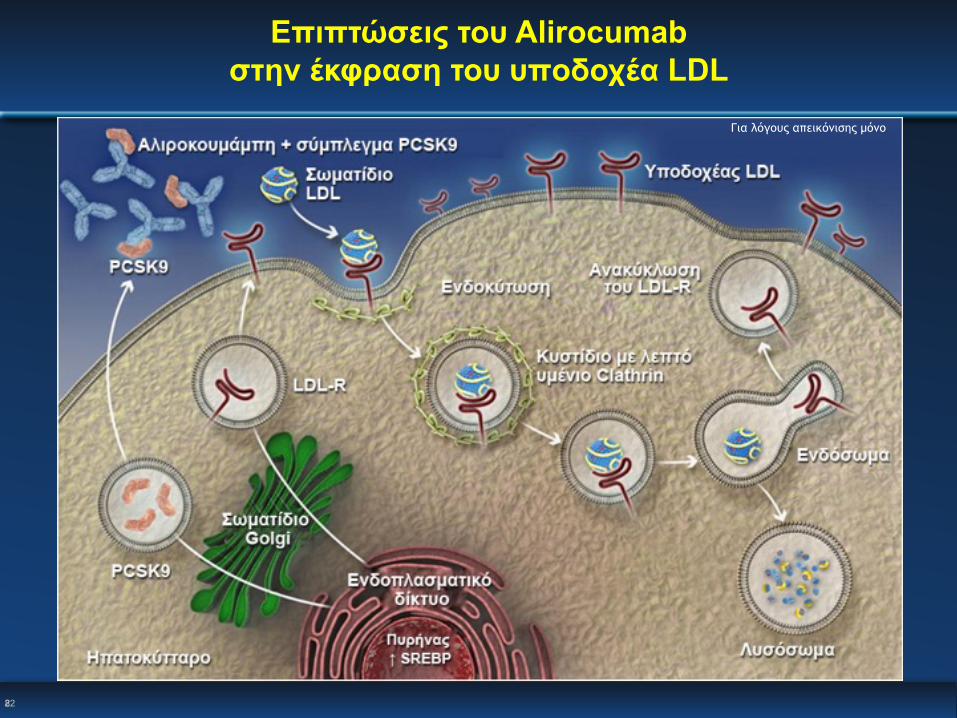
Επιπτώσεις του Alirocumab στην έκφραση του υποδοχέα LDL
822
Για λόγους απεικόνισης µόνο
LDL-C ως παράγοντας Καρδιαγγειακού κινδύνου δεδοµένα απο την µείωση
23
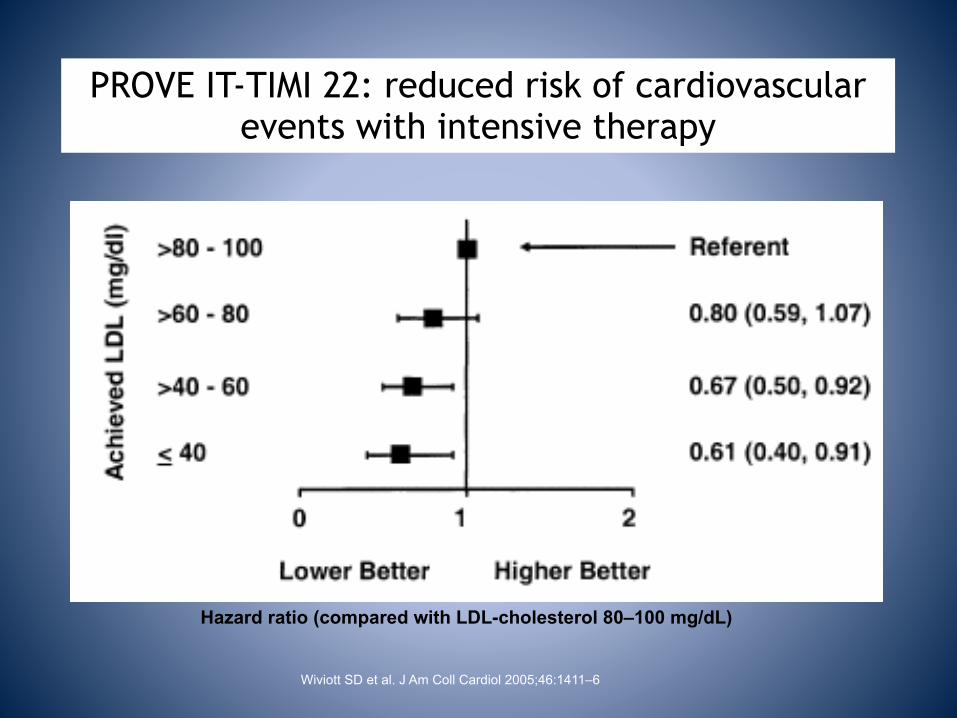
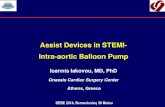
PROVE IT-TIMI 22: reduced risk of cardiovascular events with intensive therapy
Hazard ratio (compared with LDL-cholesterol 80–100 mg/dL)
Wiviott SD et al. J Am Coll Cardiol 2005;46:1411–6
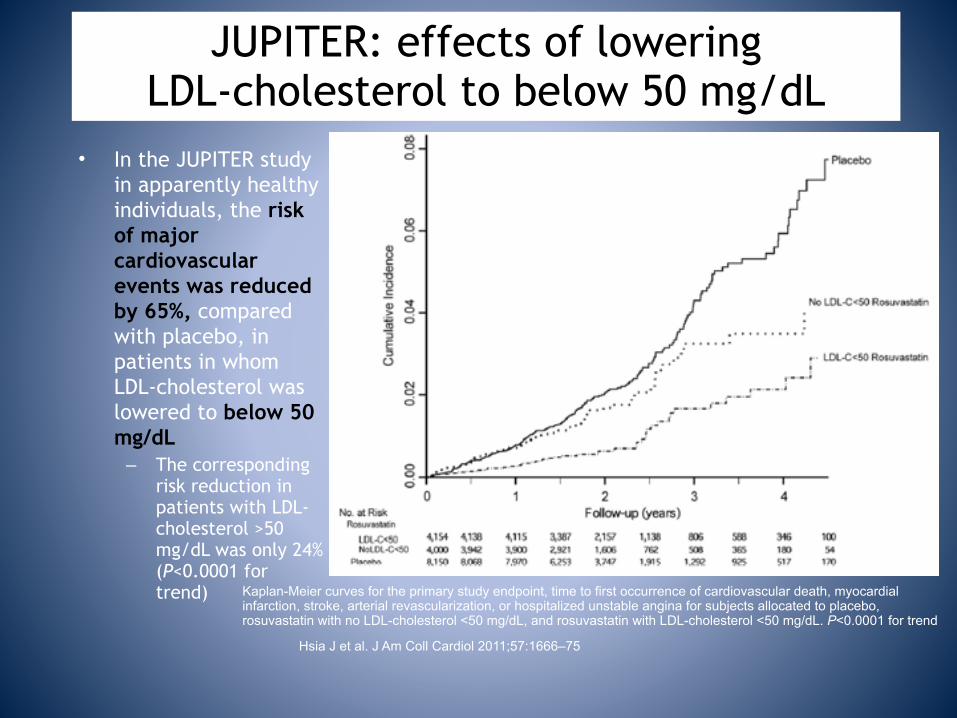
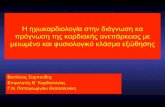
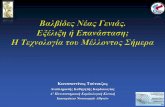
JUPITER: effects of lowering LDL-cholesterol to below 50 mg/dL
• In the JUPITER study in apparently healthy individuals, the risk of major cardiovascular events was reduced by 65%, compared with placebo, in patients in whom LDL-cholesterol was lowered to below 50 mg/dL
– The corresponding risk reduction in patients with LDL-cholesterol >50 mg/dL was only 24% (P<0.0001 for trend)
Hsia J et al. J Am Coll Cardiol 2011;57:1666–75
Kaplan-Meier curves for the primary study endpoint, time to first occurrence of cardiovascular death, myocardial infarction, stroke, arterial revascularization, or hospitalized unstable angina for subjects allocated to placebo, rosuvastatin with no LDL-cholesterol <50 mg/dL, and rosuvastatin with LDL-cholesterol <50 mg/dL. P<0.0001 for trend
Figure: time to occurrence of major cardiovascular events according to treatment group and achieved LDL-cholesterol concentrations
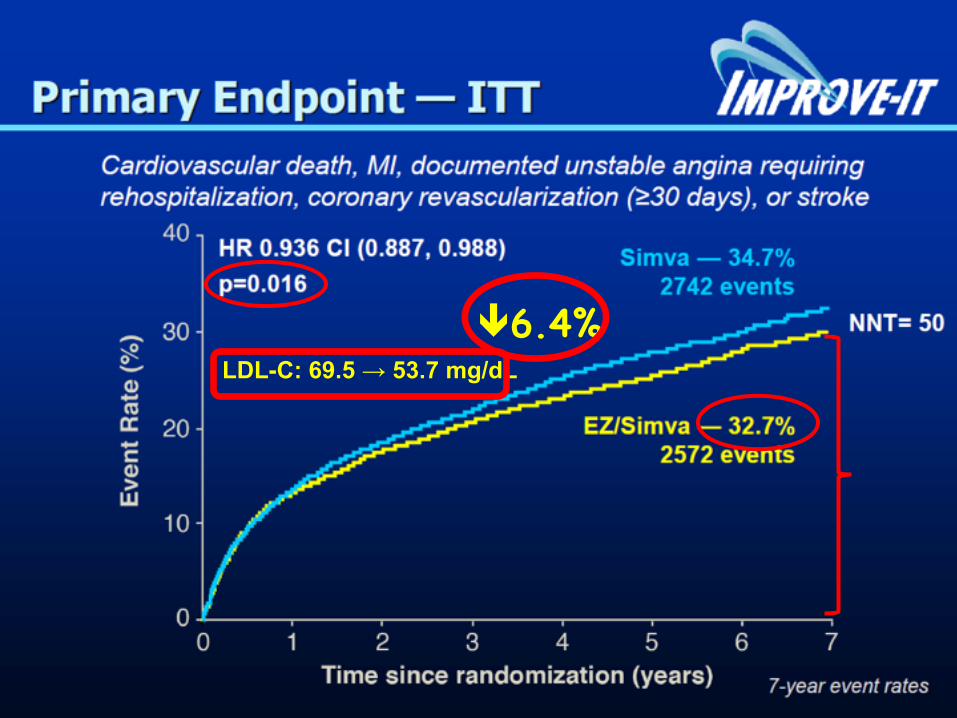
!6.4%LDL-C: 69.5 → 53.7 mg/dL
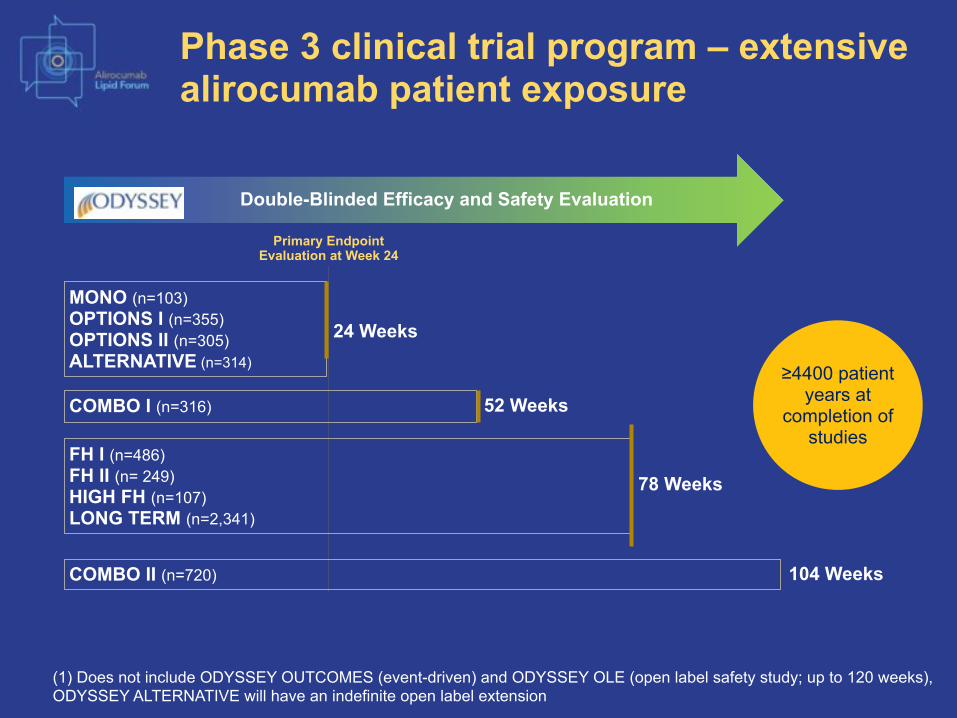
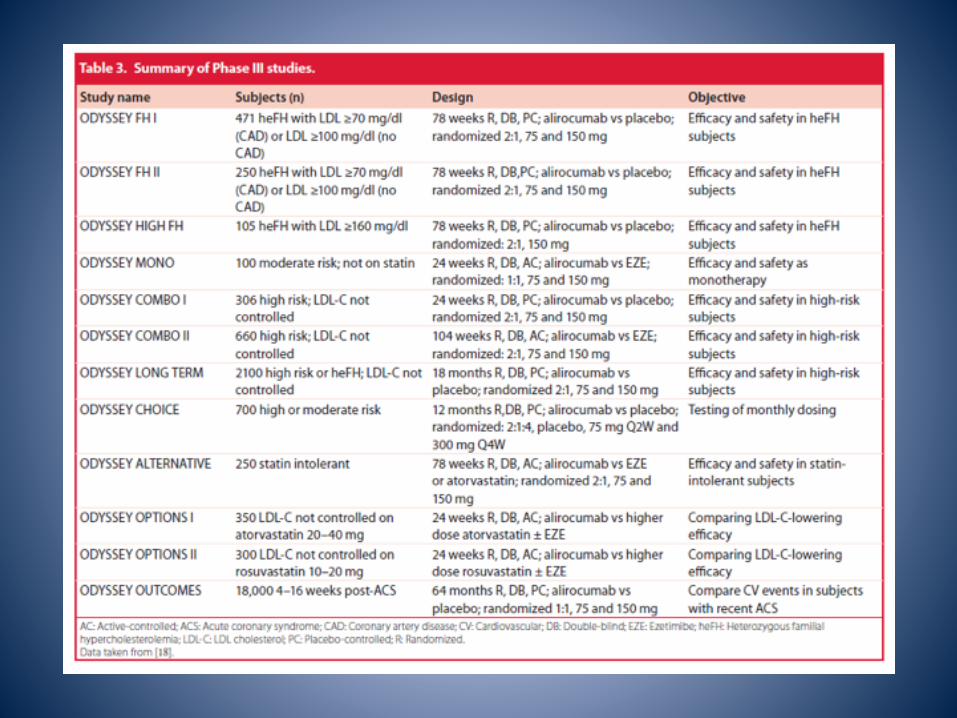
Phase 3 clinical trial program – extensive alirocumab patient exposure
(1) Does not include ODYSSEY OUTCOMES (event-driven) and ODYSSEY OLE (open label safety study; up to 120 weeks), ODYSSEY ALTERNATIVE will have an indefinite open label extension
Double-Blinded Efficacy and Safety Evaluation
MONO (n=103) OPTIONS I (n=355) OPTIONS II (n=305) ALTERNATIVE (n=314)
24 Weeks
COMBO I (n=316) 52 Weeks
COMBO II (n=720) 104 Weeks
FH I (n=486) FH II (n= 249) HIGH FH (n=107) LONG TERM (n=2,341)
78 Weeks
Primary Endpoint Evaluation at Week 24
≥4400 patient years at
completion of studies
Efficacy and safety of alirocumab in high cardiovascular risk patients with inadequately controlled
hypercholesterolaemia on maximally tolerated daily statin: results from the ODYSSEY COMBO II study
Christopher P. Cannon,1 Bertrand Cariou,2 Dirk Blom,3 James M. McKenney,4 Christelle Lorenzato,5 Robert Pordy,6
Umesh Chaudhari,7 Helen M. Colhoun8
1Harvard Clinical Research Institute, Boston, MA, USA; 2L’Institut du Thorax, CHU de Nantes, Nantes, France; 3Division of Lipidology, Department of Medicine, University of
Cape Town and MRC Cape Heart Group, Cape Town, South Africa; 4Virginia Commonwealth University and National Clinical Research, Inc., Richmond, VA, USA;
5Sanofi, Paris, France; 6Regeneron Pharmaceuticals, Inc., Tarrytown, NY, USA; 7Sanofi, Bridgewater, NJ, USA; 8University of Dundee, Dundee, Scotland, UK
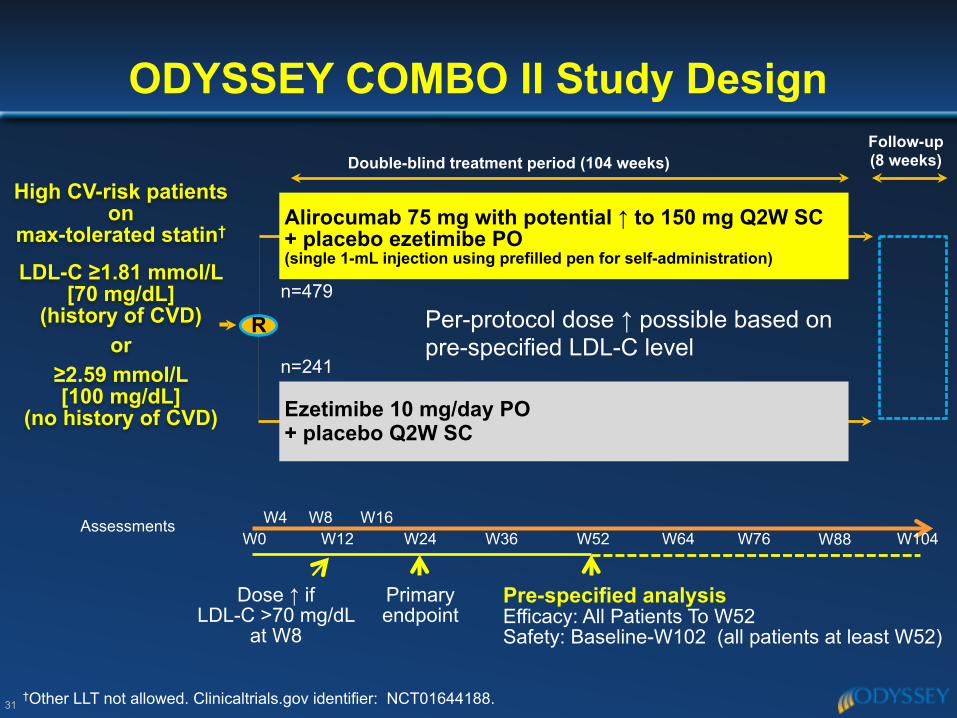
ODYSSEY COMBO II Study Design
31†Other LLT not allowed. Clinicaltrials.gov identifier: NCT01644188.
Double-blind treatment period (104 weeks)
High CV-risk patients on
max-tolerated statin† LDL-C ≥1.81 mmol/L
[70 mg/dL] (history of CVD)
or ≥2.59 mmol/L [100 mg/dL]
(no history of CVD)
Rn=479
n=241
AssessmentsW0
W4 W8W12
W16W24 W36 W52
Primary endpoint
W64 W76 W104
Dose ↑ if LDL-C >70 mg/dL
at W8
W88
Follow-up (8 weeks)
Alirocumab 75 mg with potential ↑ to 150 mg Q2W SC + placebo ezetimibe PO (single 1-mL injection using prefilled pen for self-administration)
Ezetimibe 10 mg/day PO + placebo Q2W SC
Pre-specified analysis Efficacy: All Patients To W52 Safety: Baseline-W102 (all patients at least W52)
Per-protocol dose ↑ possible based on pre-specified LDL-C level
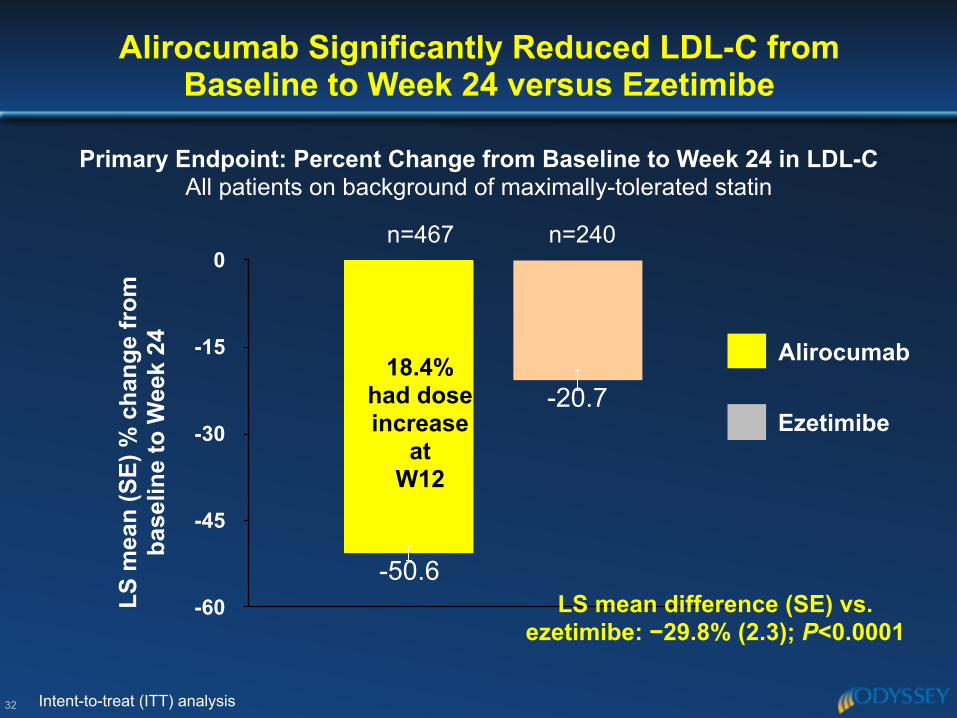
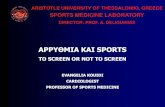
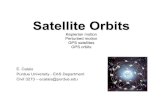
Alirocumab Significantly Reduced LDL-C from Baseline to Week 24 versus Ezetimibe
32
-60
-45
-30
-15
0
-20.7
-50.6
LS m
ean
(SE)
% c
hang
e fr
om
base
line
to W
eek
24
LS mean difference (SE) vs. ezetimibe: −29.8% (2.3); P<0.0001
n=467 n=240
Primary Endpoint: Percent Change from Baseline to Week 24 in LDL-C All patients on background of maximally-tolerated statin
Ezetimibe
Alirocumab
Intent-to-treat (ITT) analysis
18.4% had dose increase
at W12
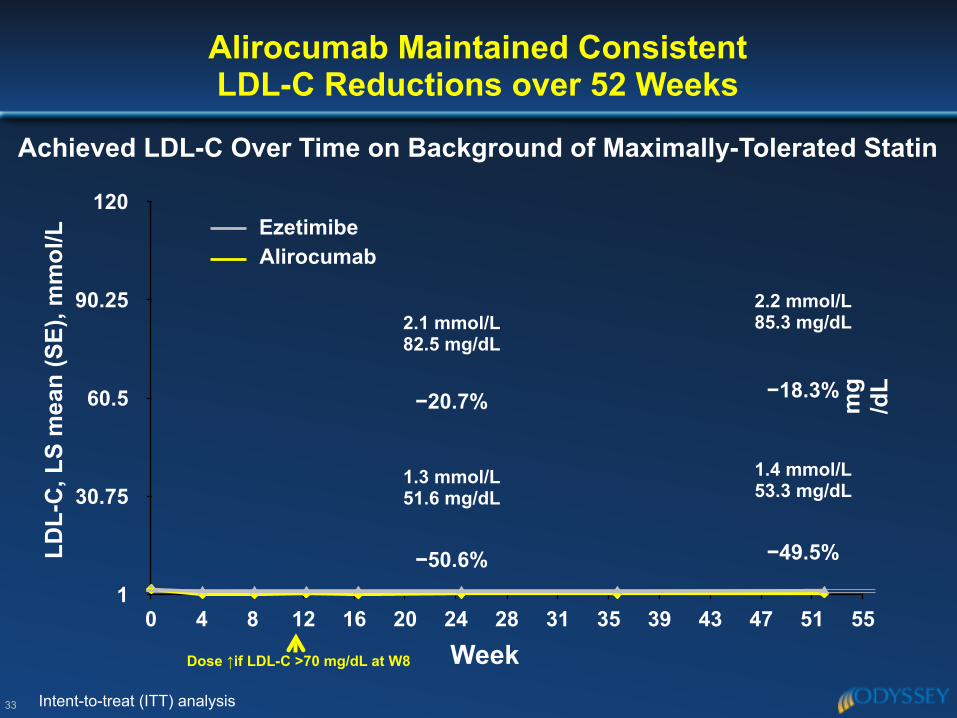
Alirocumab Maintained Consistent LDL-C Reductions over 52 Weeks
LDL-
C, L
S m
ean
(SE)
, mm
ol/L
Achieved LDL-C Over Time on Background of Maximally-Tolerated Statin
1
30.75
60.5
90.25
120
0 4 8 12 16 20 24 28 31 35 39 43 47 51 55
Ezetimibe
Week
2.1 mmol/L82.5 mg/dL
1.3 mmol/L51.6 mg/dL
Alirocumab
2.2 mmol/L85.3 mg/dL
1.4 mmol/L53.3 mg/dL
mg
/dL
33 Intent-to-treat (ITT) analysis
Dose ↑if LDL-C >70 mg/dL at W8
−20.7%
−50.6%
−18.3%
−49.5%
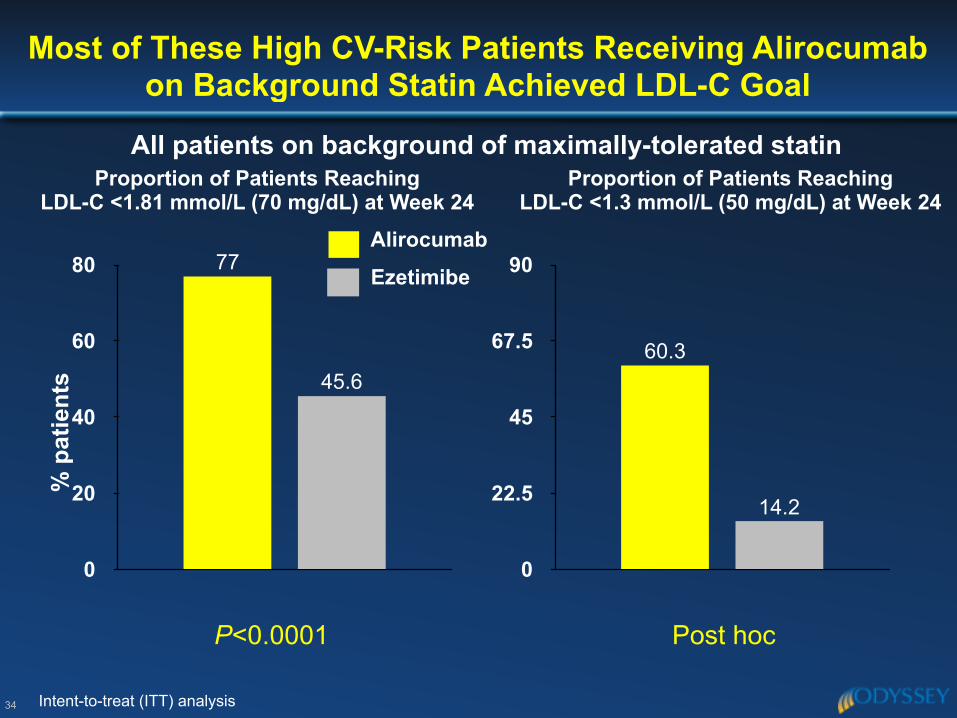
Most of These High CV-Risk Patients Receiving Alirocumab on Background Statin Achieved LDL-C Goal
34
Proportion of Patients Reaching LDL-C <1.81 mmol/L (70 mg/dL) at Week 24
% p
atie
nts
0
20
40
60
80
45.6
77
P<0.0001
Intent-to-treat (ITT) analysis
0
22.5
45
67.5
90
14.2
60.3
Proportion of Patients Reaching LDL-C <1.3 mmol/L (50 mg/dL) at Week 24
% p
atie
nts
Ezetimibe
Alirocumab
Post hoc
All patients on background of maximally-tolerated statin
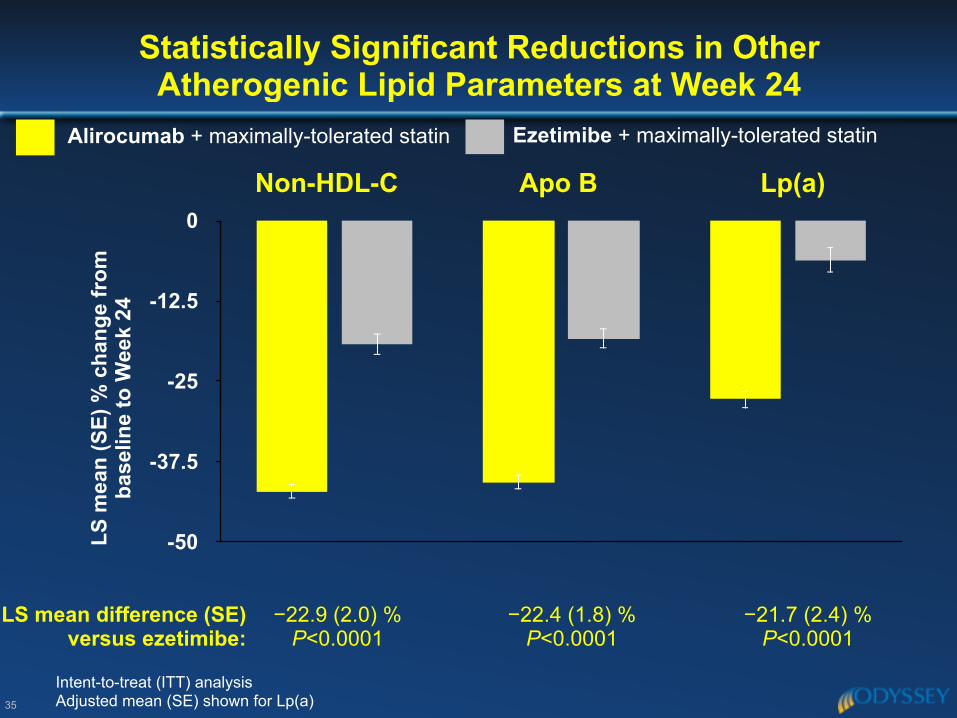
Statistically Significant Reductions in Other Atherogenic Lipid Parameters at Week 24
35
-50
-37.5
-25
-12.5
0Apo B
Ezetimibe + maximally-tolerated statinAlirocumab + maximally-tolerated statin
−22.9 (2.0) % P<0.0001
Non-HDL-C
LS m
ean
(SE)
% c
hang
e fr
om
base
line
to W
eek
24
Intent-to-treat (ITT) analysis Adjusted mean (SE) shown for Lp(a)
Lp(a)
−22.4 (1.8) % P<0.0001
−21.7 (2.4) % P<0.0001
LS mean difference (SE) versus ezetimibe:
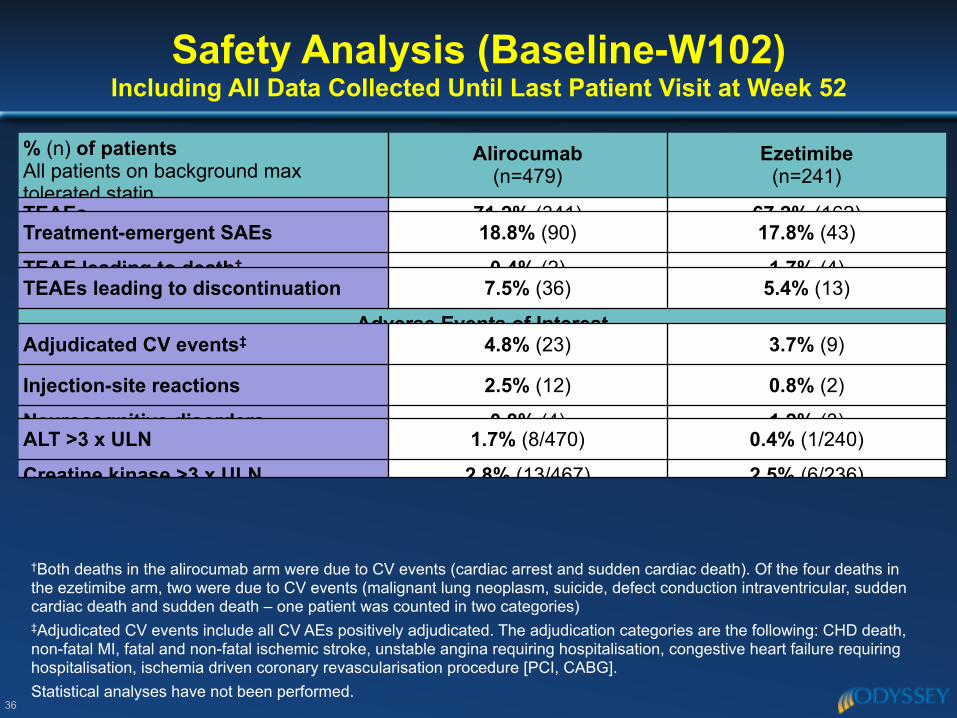
Safety Analysis (Baseline-W102)Including All Data Collected Until Last Patient Visit at Week 52
36
% (n) of patients All patients on background max tolerated statin
Alirocumab (n=479)
Ezetimibe (n=241)
TEAEs 71.2% (341) 67.2% (162)Treatment-emergent SAEs 18.8% (90) 17.8% (43)
TEAE leading to death† 0.4% (2) 1.7% (4)TEAEs leading to discontinuation 7.5% (36) 5.4% (13)
Adverse Events of InterestAdjudicated CV events‡ 4.8% (23) 3.7% (9)
Injection-site reactions 2.5% (12) 0.8% (2)
Neurocognitive disorders 0.8% (4) 1.2% (3)ALT >3 x ULN 1.7% (8/470) 0.4% (1/240)
Creatine kinase >3 x ULN 2.8% (13/467) 2.5% (6/236)
†Both deaths in the alirocumab arm were due to CV events (cardiac arrest and sudden cardiac death). Of the four deaths in the ezetimibe arm, two were due to CV events (malignant lung neoplasm, suicide, defect conduction intraventricular, sudden cardiac death and sudden death – one patient was counted in two categories) ‡Adjudicated CV events include all CV AEs positively adjudicated. The adjudication categories are the following: CHD death, non-fatal MI, fatal and non-fatal ischemic stroke, unstable angina requiring hospitalisation, congestive heart failure requiring hospitalisation, ischemia driven coronary revascularisation procedure [PCI, CABG]. Statistical analyses have not been performed.
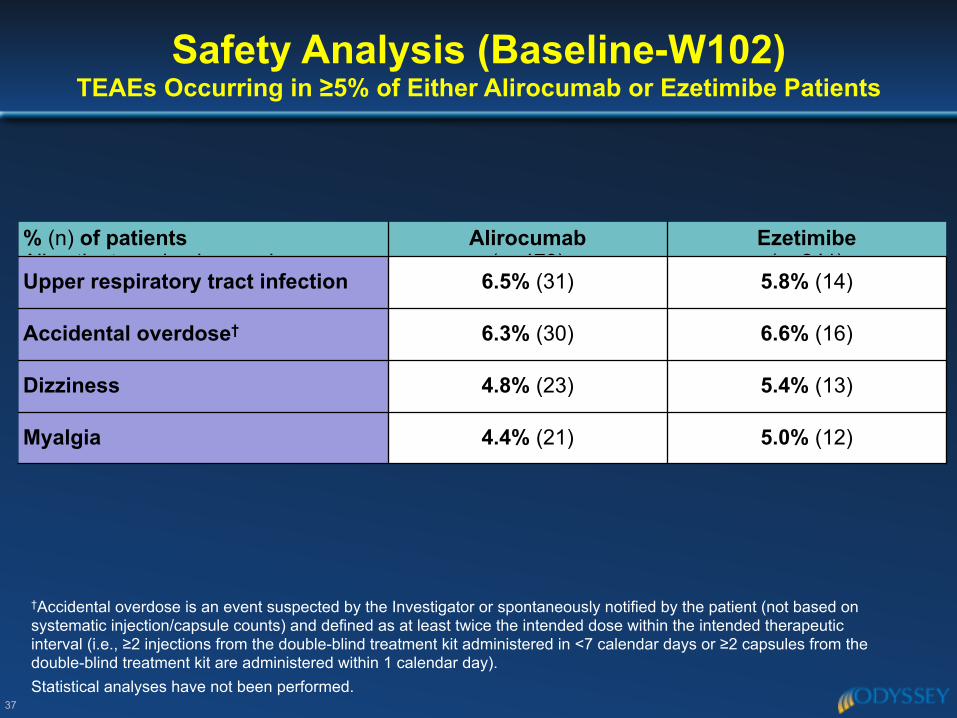
Safety Analysis (Baseline-W102)TEAEs Occurring in ≥5% of Either Alirocumab or Ezetimibe Patients
37
% (n) of patients All patients on background max
Alirocumab (n=479)
Ezetimibe (n=241)
Upper respiratory tract infection 6.5% (31) 5.8% (14)
Accidental overdose† 6.3% (30) 6.6% (16)
Dizziness 4.8% (23) 5.4% (13)
Myalgia 4.4% (21) 5.0% (12)
†Accidental overdose is an event suspected by the Investigator or spontaneously notified by the patient (not based on systematic injection/capsule counts) and defined as at least twice the intended dose within the intended therapeutic interval (i.e., ≥2 injections from the double-blind treatment kit administered in <7 calendar days or ≥2 capsules from the double-blind treatment kit are administered within 1 calendar day). Statistical analyses have not been performed.
◆ In this population of high CV-risk patients who had poorly controlled LDL-C on maximally-tolerated statin therapy:
– LDL-C ↓ from baseline maintained with alirocumab: significantly greater ↓ vs. ezetimibe at W24, 51% vs 21% (P<0.0001)
– Self-administered alirocumab had good compliance and was well-tolerated
– This “treat-to-target” approach with alirocumab resulted in ~80% pts not requiring a dose ↑ to 150 mg at W12
– 77% of alirocumab pts achieved LDL-C <1.81 mmol/L (70 mg/dL) at W24
– Mean achieved LDL-C levels of 1.4 mmol/L (53.3 mg/dL) at W52 with alirocumab
– TEAEs similar between alirocumab and ezetimibe arms
Conclusions
38
Long-term safety, tolerability and efficacy of alirocumab in high cardiovascular risk patients: ODYSSEY LONG TERM
Efficacy by subgroup, and safety when LDL-C <25 mg/dL
Jennifer G. Robinson,1 Michel Farnier,2 Michel Krempf,3 Jean Bergeron,4 Gérald Luc,5 Maurizio Averna,6 Erik Stroes,7 Gisle Langslet,8 Frederick J. Raal,9 Mahfouz El Shahawy,10 Michael J. Koren,11 Norman Lepor,12 Christelle Lorenzato,13 Robert Pordy,14 Umesh Chaudhari,15 John J.P. Kastelein7
1University of Iowa, Iowa City, IA, USA; 2Point Médical, Dijon, France; 3CHU de Nantes - Hôpital Nord Laennec, Saint-Herblain, France; 4Clinique des Maladies Lipidiques de Quebec Inc., Quebec, Canada; 5University Hospital of Lille, Lille,
France; 6Università di Palermo – Policlinico “P.Giaccone”, Palermo, Italy; 7Department of Vascular Medicine, Academic Medical Center, Amsterdam, The Netherlands; 8Lipid Clinic, Oslo University Hospital, Oslo, Norway; 9University of Witwatersrand, Johannesburg, South Africa; 10Cardiovascular Center of Sarasota, Sarasota, FL, USA; 11Jacksonville Center For Clinical
Research, Jacksonville, FL, USA; 12Westside Medical Associates of Los Angeles, Beverly Hills, CA, USA; 13Sanofi, Chilly-Mazarin, France; 14Regeneron Pharmaceuticals, Inc., Tarrytown, NY, USA; 15Sanofi, Bridgewater, NJ, USA
This study was funded by Sanofi and Regeneron Pharmaceuticals, Inc.
40
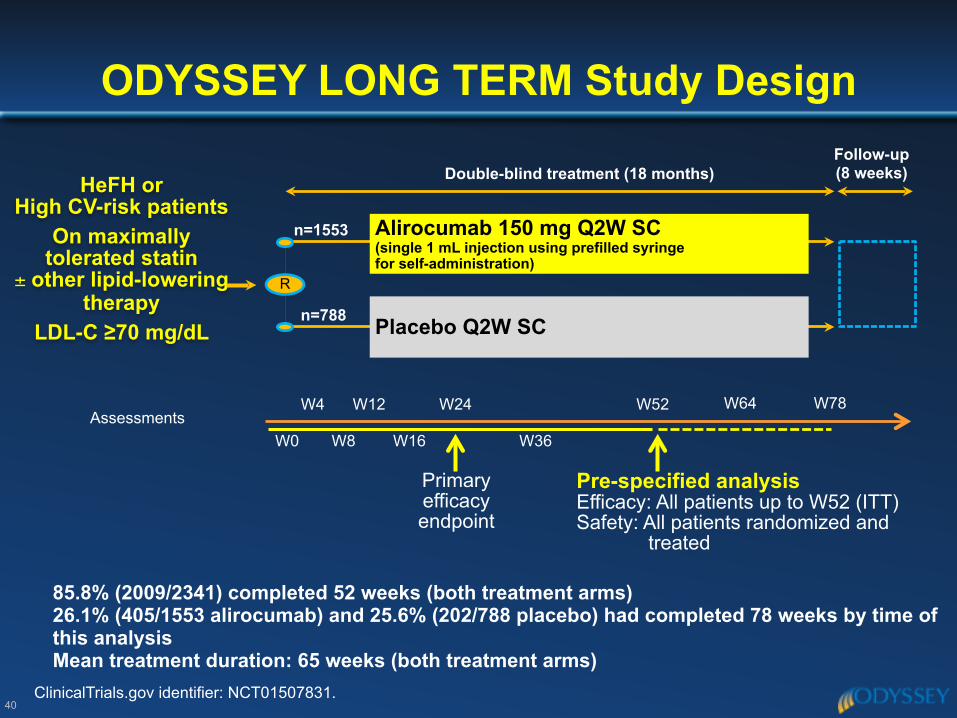
ODYSSEY LONG TERM Study Design
ClinicalTrials.gov identifier: NCT01507831.
HeFH or High CV-risk patients
On maximally tolerated statin
± other lipid-lowering therapy
LDL-C ≥70 mg/dL
Double-blind treatment (18 months)
n=1553
n=788
R
Follow-up (8 weeks)
Alirocumab 150 mg Q2W SC (single 1 mL injection using prefilled syringe for self-administration)
Placebo Q2W SC
AssessmentsW0
W4
W8
W12
W16
W24
W36
W52
Primary efficacy endpoint
Pre-specified analysis Efficacy: All patients up to W52 (ITT) Safety: All patients randomized and
treated
W64 W78
85.8% (2009/2341) completed 52 weeks (both treatment arms) 26.1% (405/1553 alirocumab) and 25.6% (202/788 placebo) had completed 78 weeks by time of this analysis Mean treatment duration: 65 weeks (both treatment arms)
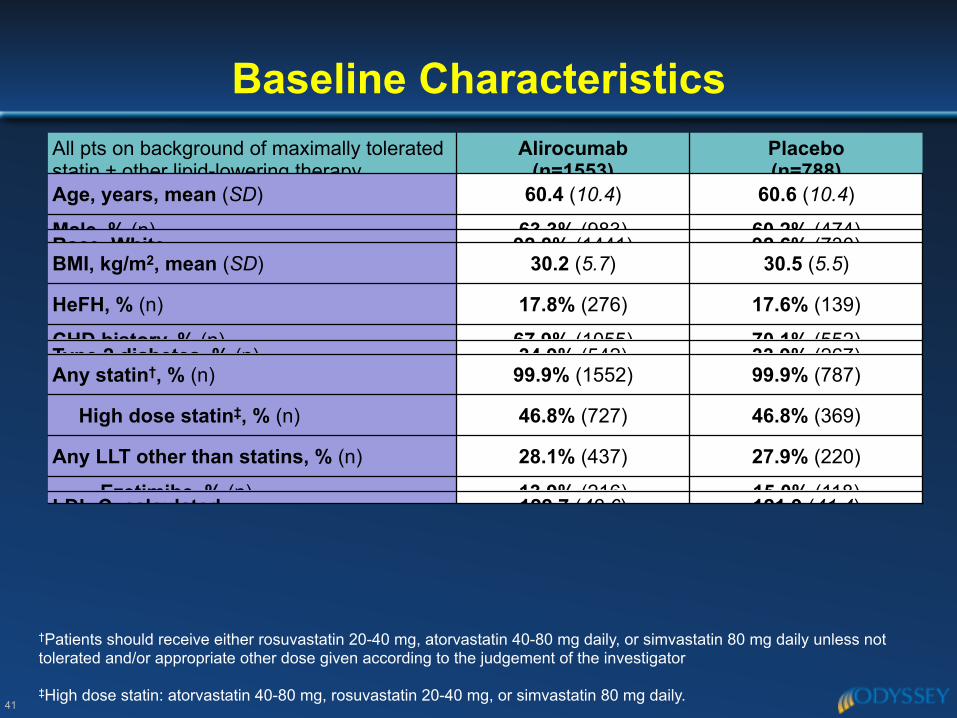
All pts on background of maximally tolerated statin ± other lipid-lowering therapy
Alirocumab(n=1553)
Placebo(n=788)
Age, years, mean (SD) 60.4 (10.4) 60.6 (10.4)
Male, % (n) 63.3% (983) 60.2% (474)Race, White 92.8% (1441) 92.6% (730)BMI, kg/m2, mean (SD) 30.2 (5.7) 30.5 (5.5)
HeFH, % (n) 17.8% (276) 17.6% (139)
CHD history, % (n) 67.9% (1055) 70.1% (552)Type 2 diabetes, % (n) 34.9% (542) 33.9% (267)Any statin†, % (n) 99.9% (1552) 99.9% (787)
High dose statin‡, % (n) 46.8% (727) 46.8% (369)
Any LLT other than statins, % (n) 28.1% (437) 27.9% (220)
Ezetimibe, % (n) 13.9% (216) 15.0% (118)LDL-C, calculated 122.7 (42.6) 121.9 (41.4)
Baseline Characteristics
41
†Patients should receive either rosuvastatin 20-40 mg, atorvastatin 40-80 mg daily, or simvastatin 80 mg daily unless not tolerated and/or appropriate other dose given according to the judgement of the investigator ‡High dose statin: atorvastatin 40-80 mg, rosuvastatin 20-40 mg, or simvastatin 80 mg daily.
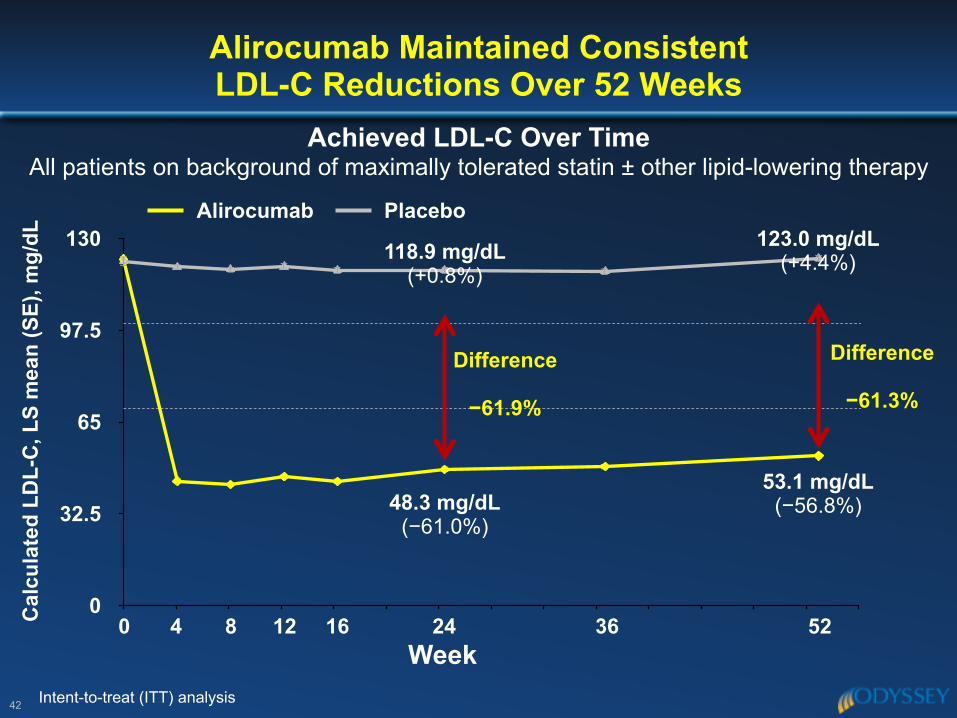
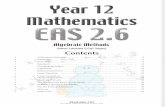
Alirocumab Maintained Consistent LDL-C Reductions Over 52 Weeks
42
0
32.5
65
97.5
130
Week
118.9 mg/dL(+0.8%)
48.3 mg/dL(−61.0%)
123.0 mg/dL (+4.4%)
53.1 mg/dL (−56.8%)
PlaceboAlirocumab
Cal
cula
ted
LDL-
C, L
S m
ean
(SE)
, mg/
dL
Achieved LDL-C Over Time All patients on background of maximally tolerated statin ± other lipid-lowering therapy
Intent-to-treat (ITT) analysis
Difference
−61.9%
0 4 8 12 16 24 36 52
Difference
−61.3%
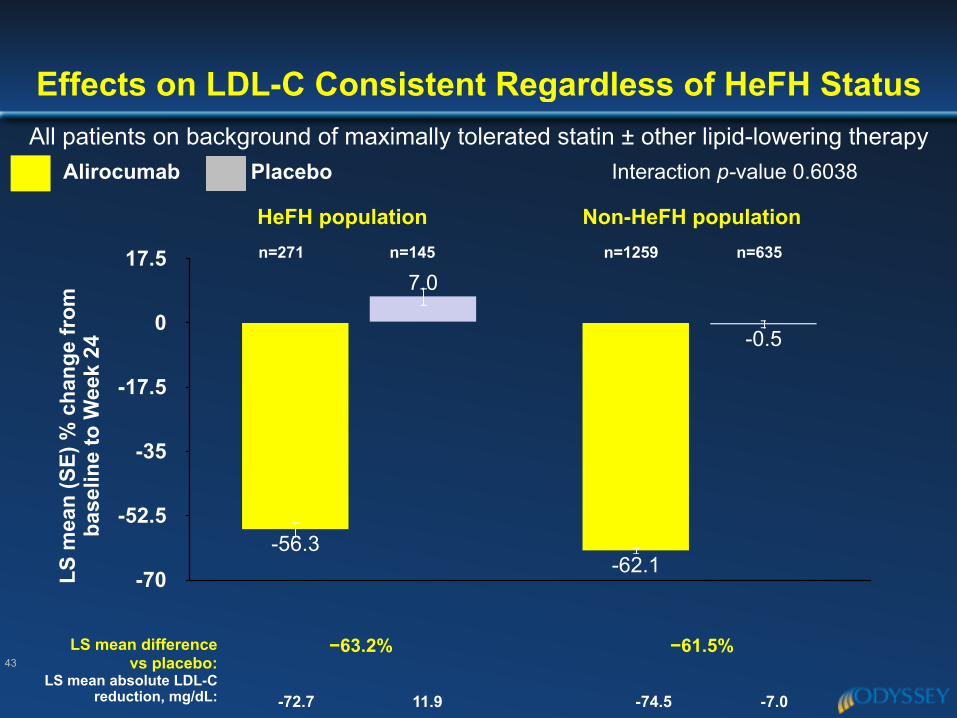
Effects on LDL-C Consistent Regardless of HeFH StatusAll patients on background of maximally tolerated statin ± other lipid-lowering therapy
43
-70
-52.5
-35
-17.5
0
17.5
-0.5
7.0
-62.1-56.3
HeFH population
LS m
ean
(SE)
% c
hang
e fr
om
base
line
to W
eek
24
Non-HeFH population
−63.2%LS mean difference vs placebo:
−61.5%
PlaceboAlirocumab Interaction p-value 0.6038
n=271 n=145 n=1259 n=635
LS mean absolute LDL-C reduction, mg/dL: -72.7 11.9 -74.5 -7.0
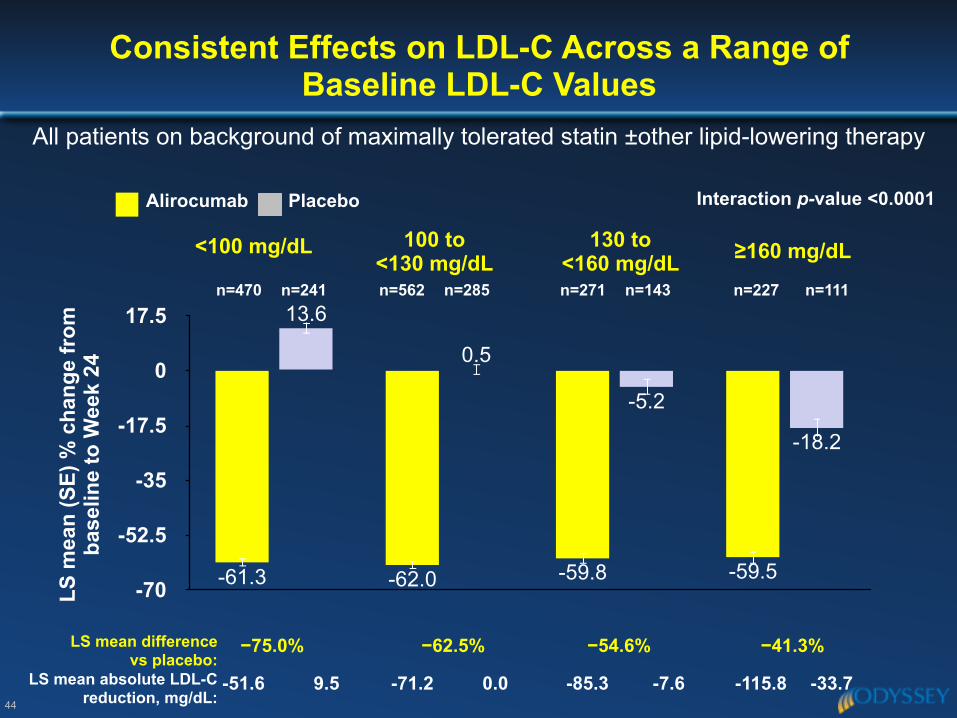
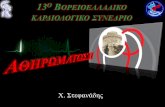
Consistent Effects on LDL-C Across a Range of Baseline LDL-C Values
44
-70
-52.5
-35
-17.5
0
17.5
-18.2
-5.2
0.5
13.6
-59.5-59.8-62.0-61.3
100 to <130 mg/dL
<100 mg/dL 130 to <160 mg/dL ≥160 mg/dL
All patients on background of maximally tolerated statin ±other lipid-lowering therapy
−75.0%LS mean difference vs placebo:
−62.5% −54.6% −41.3%
Interaction p-value <0.0001
n=470 n=241 n=562 n=285 n=271 n=143 n=227 n=111
LS m
ean
(SE)
% c
hang
e fr
om
base
line
to W
eek
24
-51.6 9.5 -71.2 0.0 -85.3 -7.6 -115.8 -33.7LS mean absolute LDL-C reduction, mg/dL:
PlaceboAlirocumab
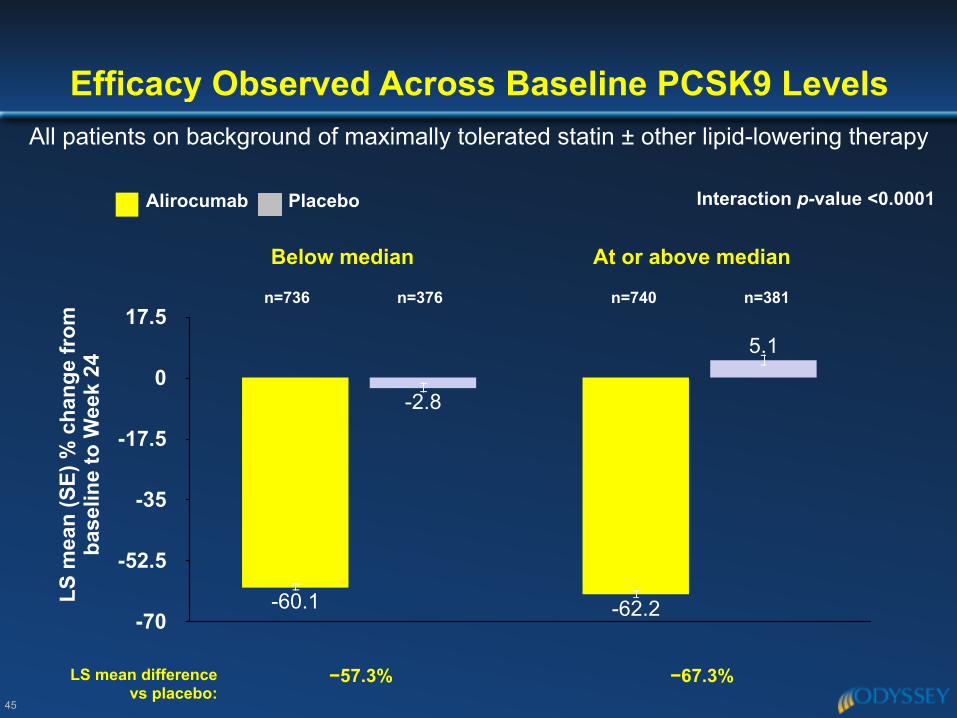
45
-70
-52.5
-35
-17.5
0
17.55.1
-2.8
-62.2-60.1
Below median At or above median
Efficacy Observed Across Baseline PCSK9 LevelsAll patients on background of maximally tolerated statin ± other lipid-lowering therapy
−57.3%LS mean difference vs placebo:
−67.3%
Interaction p-value <0.0001
n=736 n=376 n=740 n=381
LS m
ean
(SE)
% c
hang
e fr
om
base
line
to W
eek
24
PlaceboAlirocumab
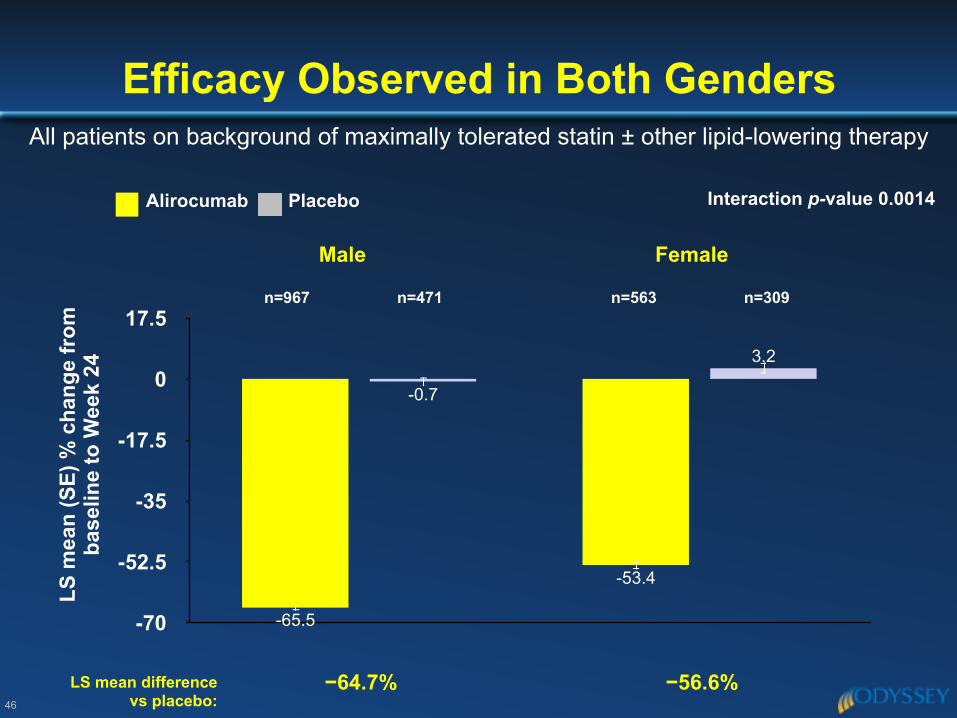
46
-70
-52.5
-35
-17.5
0
17.53.2
-0.7
-53.4
-65.5
Male Female
Efficacy Observed in Both GendersAll patients on background of maximally tolerated statin ± other lipid-lowering therapy
−64.7%LS mean difference vs placebo:
−56.6%
Interaction p-value 0.0014
n=967 n=471 n=563 n=309
LS m
ean
(SE)
% c
hang
e fr
om
base
line
to W
eek
24
PlaceboAlirocumab
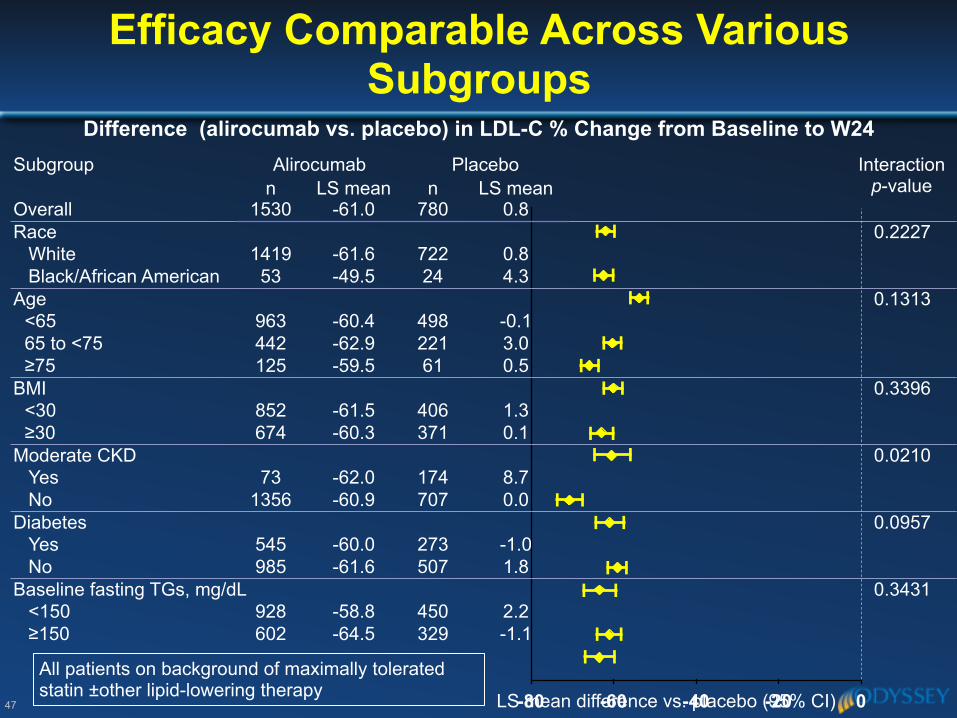
47 -80 -60 -40 -20 0
All patients on background of maximally tolerated statin ±other lipid-lowering therapy
Subgroup Alirocumab Placebo Interaction p-valuen LS mean n LS mean
Overall 1530 -61.0 780 0.8Race 0.2227
White 1419 -61.6 722 0.8Black/African American 53 -49.5 24 4.3
Age 0.1313<65 963 -60.4 498 -0.165 to <75 442 -62.9 221 3.0 ≥75 125 -59.5 61 0.5
BMI 0.3396<30 852 -61.5 406 1.3 ≥30 674 -60.3 371 0.1
Moderate CKD 0.0210Yes 73 -62.0 174 8.7 No 1356 -60.9 707 0.0
Diabetes 0.0957Yes 545 -60.0 273 -1.0 No 985 -61.6 507 1.8
Baseline fasting TGs, mg/dL 0.3431<150 928 -58.8 450 2.2≥150 602 -64.5 329 -1.1
LS mean difference vs. placebo (95% CI)
Difference (alirocumab vs. placebo) in LDL-C % Change from Baseline to W24
Efficacy Comparable Across Various Subgroups
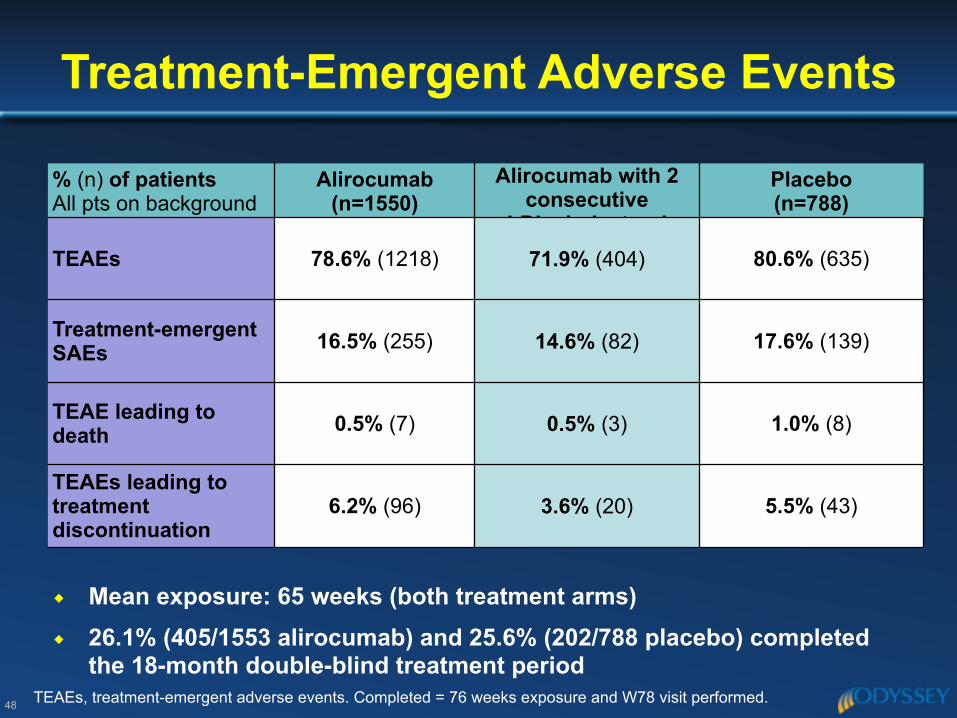
Treatment-Emergent Adverse Events
48
% (n) of patients All pts on background of maximal statin
Alirocumab(n=1550)
Alirocumab with 2 consecutive
LDL cholesterol
Placebo(n=788)
TEAEs 78.6% (1218) 71.9% (404) 80.6% (635)
Treatment-emergent SAEs 16.5% (255) 14.6% (82) 17.6% (139)
TEAE leading to death 0.5% (7) 0.5% (3) 1.0% (8)
TEAEs leading to treatment discontinuation
6.2% (96) 3.6% (20) 5.5% (43)
◆ Mean exposure: 65 weeks (both treatment arms) ◆ 26.1% (405/1553 alirocumab) and 25.6% (202/788 placebo) completed
the 18-month double-blind treatment periodTEAEs, treatment-emergent adverse events. Completed = 76 weeks exposure and W78 visit performed.
49
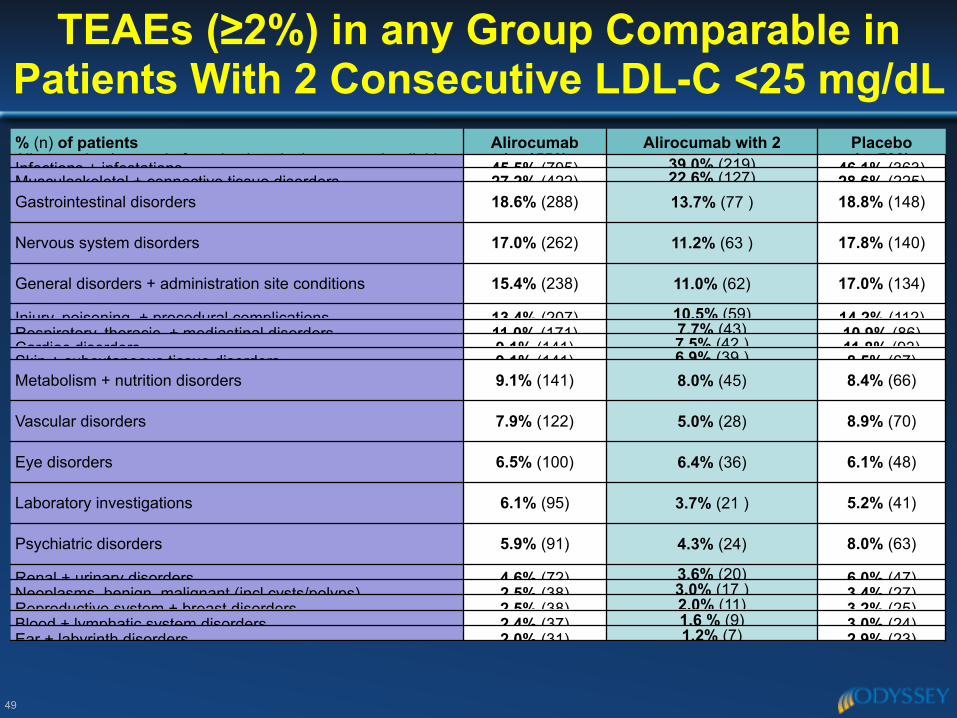
% (n) of patients All pts on background of maximal statin therapy ± other lipid-
Alirocumab(n=1550)
Alirocumab with 2 consecutive
Placebo(n=788)Infections + infestations 45.5% (705) 39.0% (219) 46.1% (363)
Musculoskeletal + connective tissue disorders 27.2% (422) 22.6% (127) 28.6% (225)Gastrointestinal disorders 18.6% (288) 13.7% (77 ) 18.8% (148)
Nervous system disorders 17.0% (262) 11.2% (63 ) 17.8% (140)
General disorders + administration site conditions 15.4% (238) 11.0% (62) 17.0% (134)
Injury, poisoning, + procedural complications 13.4% (207) 10.5% (59) 14.2% (112)Respiratory, thoracic, + mediastinal disorders 11.0% (171) 7.7% (43) 10.9% (86)Cardiac disorders 9.1% (141) 7.5% (42 ) 11.8% (93)Skin + subcutaneous tissue disorders 9.1% (141) 6.9% (39 ) 8.5% (67)Metabolism + nutrition disorders 9.1% (141) 8.0% (45) 8.4% (66)
Vascular disorders 7.9% (122) 5.0% (28) 8.9% (70)
Eye disorders 6.5% (100) 6.4% (36) 6.1% (48)
Laboratory investigations 6.1% (95) 3.7% (21 ) 5.2% (41)
Psychiatric disorders 5.9% (91) 4.3% (24) 8.0% (63)
Renal + urinary disorders 4.6% (72) 3.6% (20) 6.0% (47)Neoplasms, benign, malignant (incl cysts/polyps) 2.5% (38) 3.0% (17 ) 3.4% (27)Reproductive system + breast disorders 2.5% (38) 2.0% (11) 3.2% (25)Blood + lymphatic system disorders 2.4% (37) 1.6 % (9) 3.0% (24)Ear + labyrinth disorders 2.0% (31) 1.2% (7) 2.9% (23)
TEAEs (≥2%) in any Group Comparable in
Patients With 2 Consecutive LDL-C <25 mg/dL
50
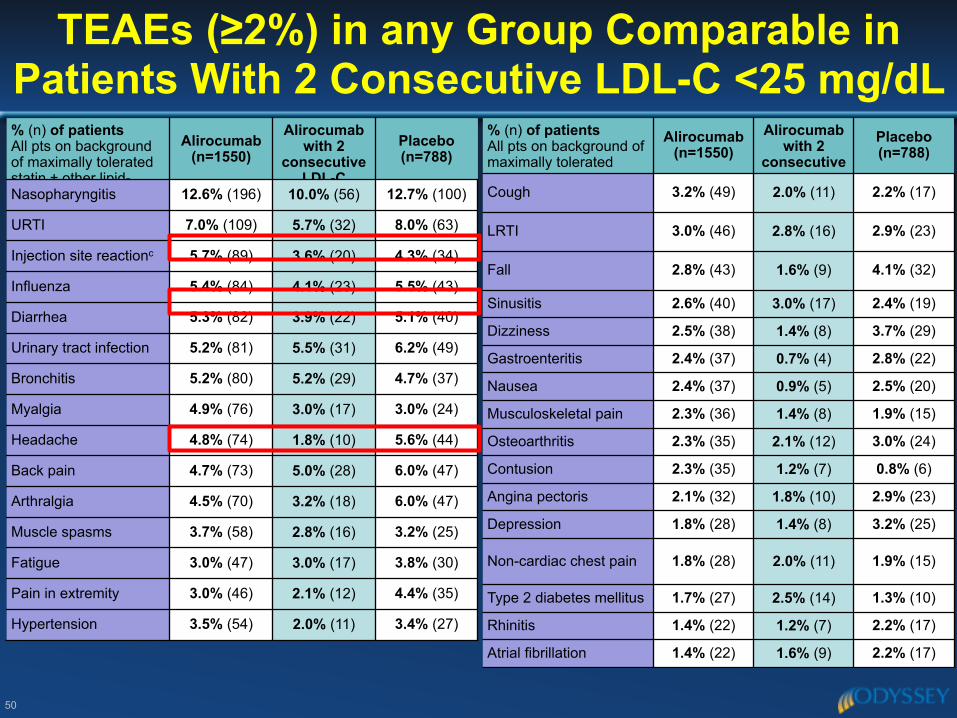
TEAEs (≥2%) in any Group Comparable in
Patients With 2 Consecutive LDL-C <25 mg/dL % (n) of patients All pts on background of maximally tolerated statin ± other lipid-
Alirocumab(n=1550)
Alirocumab with 2
consecutive LDL-C
Placebo (n=788)
Nasopharyngitis 12.6% (196) 10.0% (56) 12.7% (100)
URTI 7.0% (109) 5.7% (32) 8.0% (63)
Injection site reactionc 5.7% (89) 3.6% (20) 4.3% (34)
Influenza 5.4% (84) 4.1% (23) 5.5% (43)
Diarrhea 5.3% (82) 3.9% (22) 5.1% (40)
Urinary tract infection 5.2% (81) 5.5% (31) 6.2% (49)
Bronchitis 5.2% (80) 5.2% (29) 4.7% (37)
Myalgia 4.9% (76) 3.0% (17) 3.0% (24)
Headache 4.8% (74) 1.8% (10) 5.6% (44)
Back pain 4.7% (73) 5.0% (28) 6.0% (47)
Arthralgia 4.5% (70) 3.2% (18) 6.0% (47)
Muscle spasms 3.7% (58) 2.8% (16) 3.2% (25)
Fatigue 3.0% (47) 3.0% (17) 3.8% (30)
Pain in extremity 3.0% (46) 2.1% (12) 4.4% (35)
Hypertension 3.5% (54) 2.0% (11) 3.4% (27)
% (n) of patients All pts on background of maximally tolerated statin ± other lipid-
Alirocumab (n=1550)
Alirocumab with 2
consecutive LDL-C
Placebo (n=788)
Cough 3.2% (49) 2.0% (11) 2.2% (17)
LRTI 3.0% (46) 2.8% (16) 2.9% (23)
Fall 2.8% (43) 1.6% (9) 4.1% (32)
Sinusitis 2.6% (40) 3.0% (17) 2.4% (19)
Dizziness 2.5% (38) 1.4% (8) 3.7% (29)
Gastroenteritis 2.4% (37) 0.7% (4) 2.8% (22)
Nausea 2.4% (37) 0.9% (5) 2.5% (20)
Musculoskeletal pain 2.3% (36) 1.4% (8) 1.9% (15)
Osteoarthritis 2.3% (35) 2.1% (12) 3.0% (24)
Contusion 2.3% (35) 1.2% (7) 0.8% (6)
Angina pectoris 2.1% (32) 1.8% (10) 2.9% (23)
Depression 1.8% (28) 1.4% (8) 3.2% (25)
Non-cardiac chest pain 1.8% (28) 2.0% (11) 1.9% (15)
Type 2 diabetes mellitus 1.7% (27) 2.5% (14) 1.3% (10)
Rhinitis 1.4% (22) 1.2% (7) 2.2% (17)
Atrial fibrillation 1.4% (22) 1.6% (9) 2.2% (17)
51
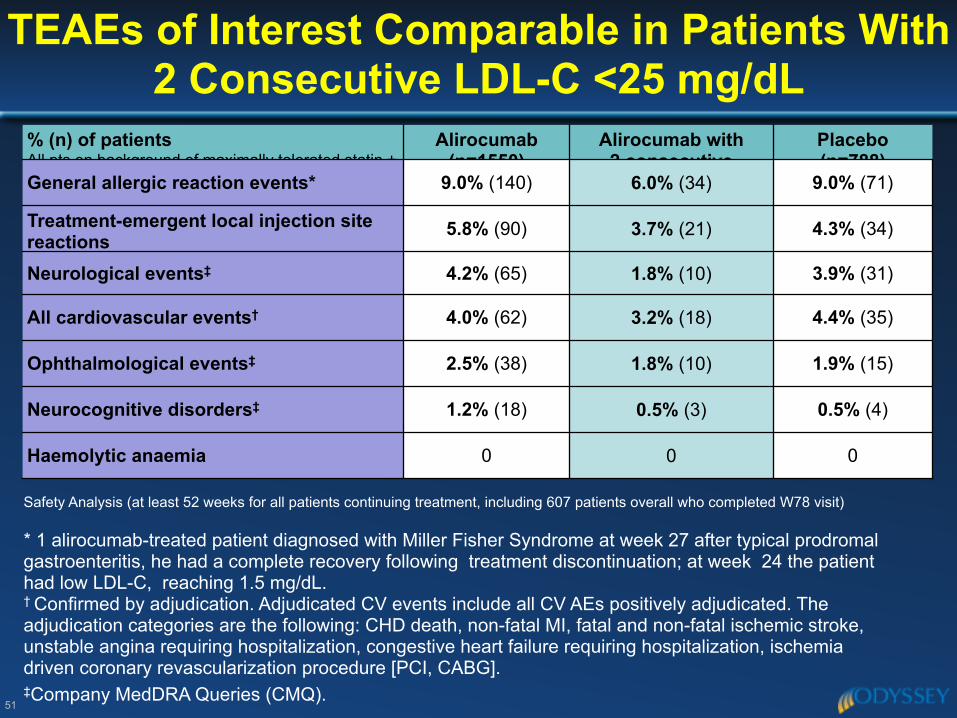
TEAEs of Interest Comparable in Patients With
2 Consecutive LDL-C <25 mg/dL% (n) of patients All pts on background of maximally tolerated statin ±
Alirocumab (n=1550)
Alirocumab with2 consecutive
Placebo(n=788)
General allergic reaction events* 9.0% (140) 6.0% (34) 9.0% (71)
Treatment-emergent local injection site reactions
5.8% (90) 3.7% (21) 4.3% (34)
Neurological events‡ 4.2% (65) 1.8% (10) 3.9% (31)
All cardiovascular events† 4.0% (62) 3.2% (18) 4.4% (35)
Ophthalmological events‡ 2.5% (38) 1.8% (10) 1.9% (15)
Neurocognitive disorders‡ 1.2% (18) 0.5% (3) 0.5% (4)
Haemolytic anaemia 0 0 0
* 1 alirocumab-treated patient diagnosed with Miller Fisher Syndrome at week 27 after typical prodromal gastroenteritis, he had a complete recovery following treatment discontinuation; at week 24 the patient had low LDL-C, reaching 1.5 mg/dL.† Confirmed by adjudication. Adjudicated CV events include all CV AEs positively adjudicated. The adjudication categories are the following: CHD death, non-fatal MI, fatal and non-fatal ischemic stroke, unstable angina requiring hospitalization, congestive heart failure requiring hospitalization, ischemia driven coronary revascularization procedure [PCI, CABG]. ‡Company MedDRA Queries (CMQ).
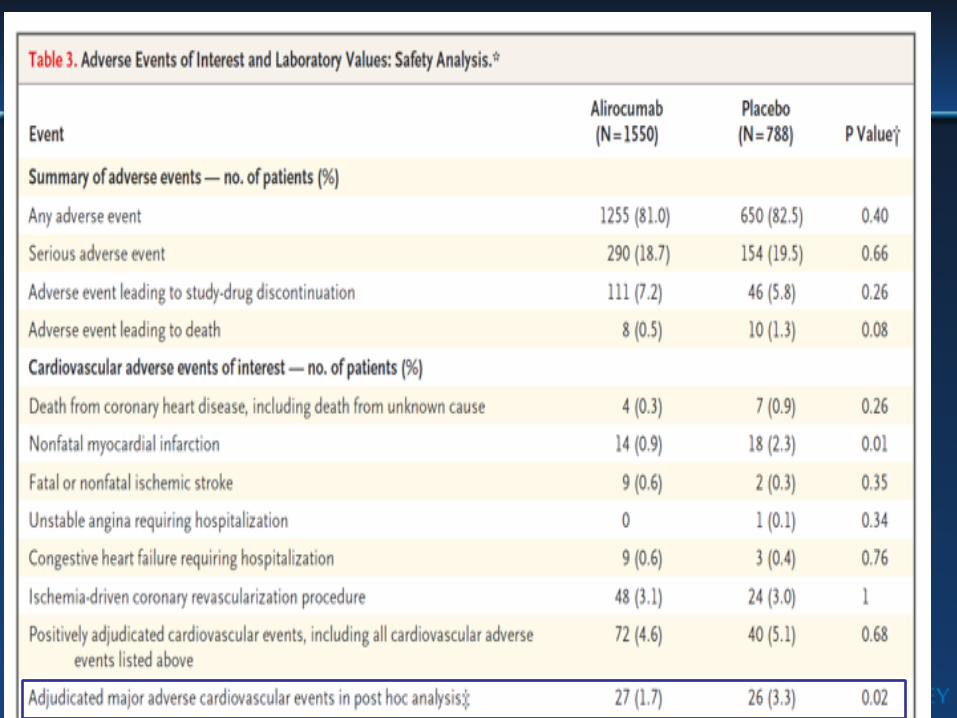
Safety Analysis (at least 52 weeks for all patients continuing treatment, including 607 patients overall who completed W78 visit)
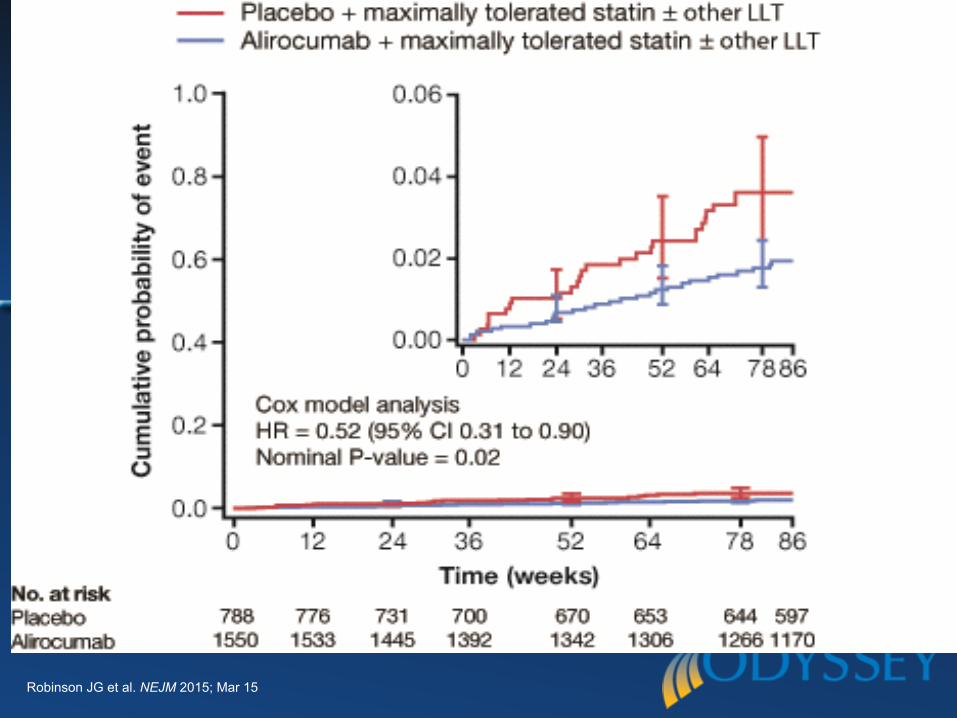
Robinson JG et al. NEJM 2015; Mar 15
Conclusions: ODYSSEY LONG TERM
54
◆ Consisted of 80% high CV risk patients and 20% of HeFH patients receiving max tolerated dose of statins (68% with previous CHD)
◆ 61% LDL C reduction vs. baseline (61.9% vs. placebo) starting from week 4 and maintained over time
◆ 80% of patients reached LDL-C<70mg/dL ◆ Reduction in LDL-C was seen across age, gender, body mass index (BMI),
race, baseline LDL-C levels, patients with HeFH and non-HeFH, and patients with mixed dyslipidemia, including diabetic patients
◆ TEAEs were generally comparable in both treatment arms and in 562 pts with confirmed low LDL-C (LDL-C < 25 mg/dL) vs. patients with LDL-C > 25 mg
◆ In a post-hoc analysis of a subgroup of adjudicated major adverse CV events, a lower rate of MACE was observed in the ALI arm compared to the PBO arm, HR=0.52 (95% CI 0.31 to 0.90, nominal P = 0.02))
Ανεπιθύµητες ενέργειες στο ODYSSEY program
55
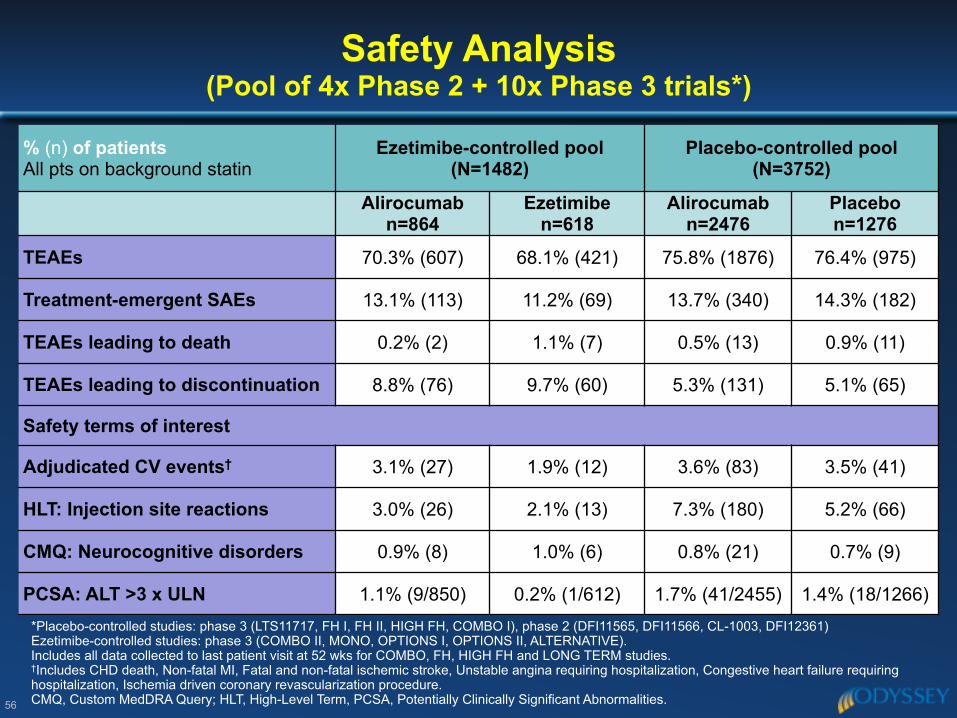
% (n) of patients All pts on background statin
Ezetimibe-controlled pool (N=1482)
Placebo-controlled pool (N=3752)
Alirocumab n=864
Ezetimibe n=618
Alirocumab n=2476
Placebon=1276
TEAEs 70.3% (607) 68.1% (421) 75.8% (1876) 76.4% (975)
Treatment-emergent SAEs 13.1% (113) 11.2% (69) 13.7% (340) 14.3% (182)
TEAEs leading to death 0.2% (2) 1.1% (7) 0.5% (13) 0.9% (11)
TEAEs leading to discontinuation 8.8% (76) 9.7% (60) 5.3% (131) 5.1% (65)
Safety terms of interest
Adjudicated CV events† 3.1% (27) 1.9% (12) 3.6% (83) 3.5% (41)
HLT: Injection site reactions 3.0% (26) 2.1% (13) 7.3% (180) 5.2% (66)
CMQ: Neurocognitive disorders 0.9% (8) 1.0% (6) 0.8% (21) 0.7% (9)
PCSA: ALT >3 x ULN 1.1% (9/850) 0.2% (1/612) 1.7% (41/2455) 1.4% (18/1266)
Safety Analysis (Pool of 4x Phase 2 + 10x Phase 3 trials*)
56
*Placebo-controlled studies: phase 3 (LTS11717, FH I, FH II, HIGH FH, COMBO I), phase 2 (DFI11565, DFI11566, CL-1003, DFI12361) Ezetimibe-controlled studies: phase 3 (COMBO II, MONO, OPTIONS I, OPTIONS II, ALTERNATIVE). Includes all data collected to last patient visit at 52 wks for COMBO, FH, HIGH FH and LONG TERM studies. †Includes CHD death, Non-fatal MI, Fatal and non-fatal ischemic stroke, Unstable angina requiring hospitalization, Congestive heart failure requiring hospitalization, Ischemia driven coronary revascularization procedure. CMQ, Custom MedDRA Query; HLT, High-Level Term, PCSA, Potentially Clinically Significant Abnormalities.
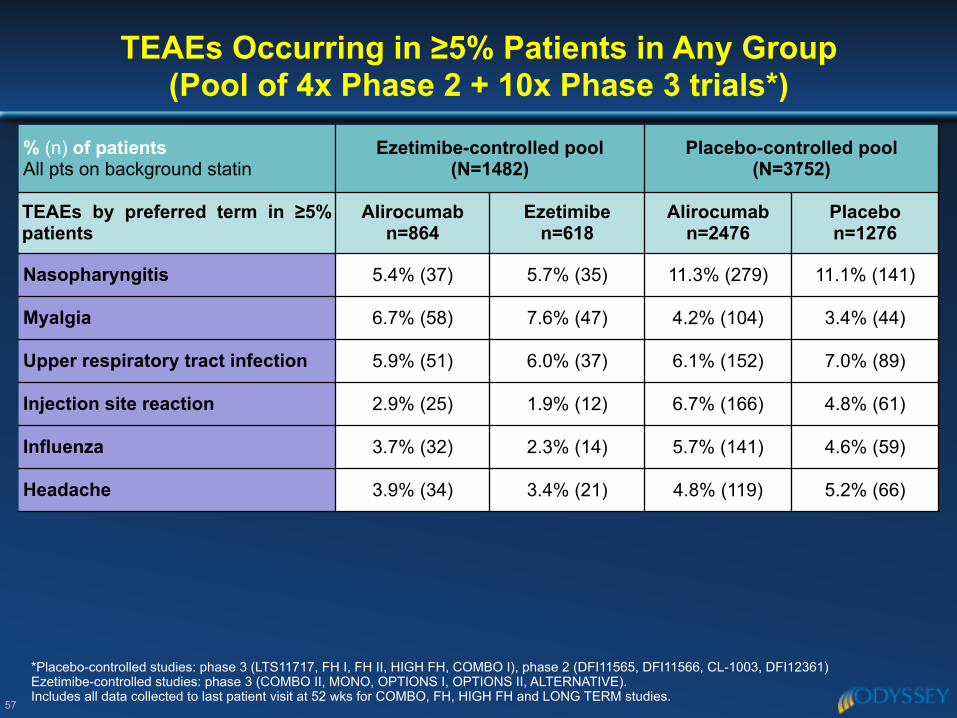
% (n) of patients All pts on background statin
Ezetimibe-controlled pool (N=1482)
Placebo-controlled pool (N=3752)
TEAEs by preferred term in ≥5% patients
Alirocumab n=864
Ezetimibe n=618
Alirocumab n=2476
Placebon=1276
Nasopharyngitis 5.4% (37) 5.7% (35) 11.3% (279) 11.1% (141)
Myalgia 6.7% (58) 7.6% (47) 4.2% (104) 3.4% (44)
Upper respiratory tract infection 5.9% (51) 6.0% (37) 6.1% (152) 7.0% (89)
Injection site reaction 2.9% (25) 1.9% (12) 6.7% (166) 4.8% (61)
Influenza 3.7% (32) 2.3% (14) 5.7% (141) 4.6% (59)
Headache 3.9% (34) 3.4% (21) 4.8% (119) 5.2% (66)
TEAEs Occurring in ≥5% Patients in Any Group (Pool of 4x Phase 2 + 10x Phase 3 trials*)
57
*Placebo-controlled studies: phase 3 (LTS11717, FH I, FH II, HIGH FH, COMBO I), phase 2 (DFI11565, DFI11566, CL-1003, DFI12361) Ezetimibe-controlled studies: phase 3 (COMBO II, MONO, OPTIONS I, OPTIONS II, ALTERNATIVE). Includes all data collected to last patient visit at 52 wks for COMBO, FH, HIGH FH and LONG TERM studies.
58