![arXiv:1507.06453v1 [astro-ph.SR] 23 Jul 2015Takizawa and Kitai the surface, i.e., the so-called “island δ-spot”, ii) emergence of large satellite spots near a larger and older](https://static.fdocument.org/doc/165x107/5ea02e646842616ae0446919/arxiv150706453v1-astro-phsr-23-jul-2015-takizawa-and-kitai-the-surface-ie.jpg)
α-Adrenergic agonist drugs, left ventricular function, and emergence from cardiopulmonary bypass
6
a-Adrenergic Agonist Drugs, Left Ventricular Function, and Emergence From Cardiopulmonary Bypass Charles E. Smith, MD, FRCPC, Thomas L. Higgins, MD, Erik J. Kraenzler, MD, Norman J. Starr, MD, Joseph P. Coyle, MD, Michael G. Licina. MD, and James Blum, BSET The relationship between preoperative left ventricu- lar (LVI dysfunction and the use of a-adrenoceptor agonists during weaning from cardiopulmonary by- pass was studied in 102 patients undergoing coro- nary artery surgery. LV function was evaluated subjectively by examination of the 30° right anterior oblique left ventriculogram. Group 1 consisted of 75 patients with normal or mild impairment in LV function, whereas group 2 consisted of 27 patients with moderate-severe LV dysfunction. Cardiovascu- lar parameters were measured at baseline, during hypothermic bypass with the aorta clamped, during normothermic bypass after unclamping, and 1 and 15 minutes after separation from bypass. Thirty-seven C OMPARED WITH patients with normal left ventricular (LV) function, patients with LV dysfunction, as evidenced by low ejection fraction and LV dyssynergy, are more likely to experience significant and prolonged biventricu- lar dysfunction after myocardial revasculariza- tion. I These patients have been reported to have an increased need for postoperative inotropic drug support and intraaortic balloon counterpul- sation.? However, separation from cardiopulmo- nary bypass (CPB) following coronary artery bypass grafting (CABG) surgery requires both an adequate cardiac output (CO) and systemic vascular resistance (SVR) in order to maintain mean arterial pressure (MAP). Thus, vasopres- sor drug therapy alone, or in addition to inotropic drugs, may occasionally be necessary for the orderly and successful transition from CPB to the patient's own cardiovascular function. Little is known about the relationship be- tween preoperative LV dysfunction and the use of a-adrenergic receptor agonists such as phenyl- ephrine and norepinephrine following CPB. Schwinn et al 3 reported that the pressor effect of phenylephrine prior to CPB may be significantly impaired in anesthetized patients with low ejec- tion fractions and congestive heart failure under- going CABG. However, this difference was not observed during CPB after application of the aortic cross-clamp." The objective of this study was to characterize the relationship between preoperative LV dysfunction and the require- patients in group 1 (49%) and 11 patients in group 2 (39%1 required some form of inotropic and/or vaso- pressor support during weaning from bypass. Group 2 required significantly higher cumulative doses of phenylephrine after bypass compared with group 1 (1.69 ± 0.70 mg, n = 9, v 0.24 ± 0.04 mg, n = 27, P < 0.05). Similarly, the dose of norepinephrine infu- sion in group 2 was 3.3 times that in group 1 (10 ± 6 I'g/min, n = 2, v 3 ± 0.6 I'g/min, n = 2, P = NS). The higher doses of a-adrenoceptor agonists re- quired in patients with moderate-severe LV dysfunc- tion may be due to differences in a-adrenoceptor agonist affinity and / or receptor density. © 1990 by W.B. Saunders Company. ment for a-adrenoceptor agonist drugs in pa- tients undergoing CABG during emergence from CPB. MATERIALS AND METHODS One hundred two patients undergoing elective pri- mary or repeat CABG were investigated. Institutional review board approval was obtained. Because participation in this descriptive study did not alter perioperative care, informed consent from each patient was unnecessary. Patients with combined vascular or valvular surgery were excluded, as were unstable patients requiring preoperative intraaortic balloon counterpulsation or inotropic medications. All patients under- went preoperative left heart catheterization, coronary arterio- graphy, and left ventriculography. LV dysfunction was evalu- ated subjectively by examination of the 30° right anterior oblique left ventriculogram and categorized as normal func- tion or mild, moderate, or severe impairment. Of the 102 patients, 34 had normal function, 41 had mild dysfunction, 19 had moderate dysfunction, and 8 had severe dysfunction. Group 1 consisted of 75 patients with normal or mild impairment in LV function, whereas group 2 consisted of 27 patients with moderate or severe LV dysfunction. All patients were premedicated with morphine, 0.1 mg/kg, and scopolamine, 0.2 to 0.4 mg, intramuscularly (1M), 1 hour prior to arrival in the operating room. Patients were maintained on their usual doses of tI-blockers, calcium channel blockers, and nitrates up until and including the From the Department of Cardiothoracic Anesthesia. Cleveland Clinic Foundation, Cleveland, OH. Address reprint requests to Charles E. Smith, MD, FRCPC, Department of Anesthesia, Metro Health Medical Center, 3395 Scranton Rd. Cleveland. OH 44109. © 1990 by W.H. Saunders Company. 0888-6296/90/0406-0003$03.00/0 Journal of Cardiothoracic Anesthesia, Vol 4, No 6 (December). 1990: pp 681-686 681
Transcript of α-Adrenergic agonist drugs, left ventricular function, and emergence from cardiopulmonary bypass

a-Adrenergic Agonist Drugs, Left Ventricular Function, andEmergence From Cardiopulmonary Bypass
Charles E. Smith, MD, FRCPC, Thomas L. Higgins, MD, Erik J. Kraenzler, MD, Norman J. Starr, MD,
Joseph P. Coyle, MD, Michael G. Licina. MD, and James Blum, BSET
The relationship between preoperative left ventricular (LVI dysfunction and the use of a-adrenoceptoragonists during weaning from cardiopulmonary bypass was studied in 102 patients undergoing coronary artery surgery. LV function was evaluatedsubjectively by examination of the 30° right anterioroblique left ventriculogram. Group 1 consisted of 75patients with normal or mild impairment in LVfunction, whereas group 2 consisted of 27 patientswith moderate-severe LV dysfunction. Cardiovascular parameters were measured at baseline, duringhypothermic bypass with the aorta clamped, duringnormothermic bypass after unclamping, and 1 and 15minutes after separation from bypass. Thirty-seven
CO MPAR ED WITH patients with normalleft ventricular (LV) function, patients with
LV dysfunction, as evidenced by low ejectionfraction and LV dyssynergy, are more likely toexperience significant and prolonged biventricular dysfunction after myocardial revascularization. I These patients have been reported to havean increased need for postoperative inotropicdrug support and intraaortic balloon counterpulsation.? However, separation from cardiopulmonary bypass (CPB) following coronary arterybypass grafting (CABG) surgery requires bothan adequate cardiac output (CO) and systemicvascular resistance (SVR) in order to maintainmean arterial pressure (MAP). Thus, vasopressor drug therapy alone, or in addition to inotropicdrugs, may occasionally be necessary for theorderly and successful transition from CPB tothe patient's own cardiovascular function.
Little is known about the relationship between preoperative LV dysfunction and the useof a-adrenergic receptor agonists such as phenylephrine and norepinephrine following CPB.Schwinn et al 3 reported that the pressor effect ofphenylephrine prior to CPB may be significantlyimpaired in anesthetized patients with low ejection fractions and congestive heart failure undergoing CABG. However, this difference was notobserved during CPB after application of theaortic cross-clamp." The objective of this studywas to characterize the relationship betweenpreoperative LV dysfunction and the require-
patients in group 1 (49%) and 11 patients in group 2(39%1 required some form of inotropic and/or vasopressor support during weaning from bypass. Group2 required significantly higher cumulative doses ofphenylephrine after bypass compared with group 1(1.69 ± 0.70 mg, n = 9, v 0.24 ± 0.04 mg, n = 27,P < 0.05). Similarly, the dose of norepinephrine infusion in group 2 was 3.3 times that in group 1 (10 ± 6I'g/min, n = 2, v 3 ± 0.6 I'g/min, n = 2, P = NS).The higher doses of a-adrenoceptor agonists required in patients with moderate-severe LV dysfunction may be due to differences in a-adrenoceptoragonist affinity and / or receptor density.© 1990 by W.B. Saunders Company.
ment for a-adrenoceptor agonist drugs in patients undergoing CABG during emergence fromCPB.
MATERIALS AND METHODS
One hundred two patients undergoing elective primary or repeat CABG were investigated. Institutional reviewboard approval was obtained. Because participation in thisdescriptive study did not alter perioperative care, informedconsent from each patient was unnecessary. Patients withcombined vascular or valvular surgery were excluded, as wereunstable patients requiring preoperative intraaortic ballooncounterpulsation or inotropic medications. All patients underwent preoperative left heart catheterization, coronary arteriography, and left ventriculography. LV dysfunction was evaluated subjectively by examination of the 30° right anterioroblique left ventriculogram and categorized as normal function or mild, moderate, or severe impairment. Of the 102patients, 34 had normal function, 41 had mild dysfunction, 19had moderate dysfunction, and 8 had severe dysfunction.Group 1 consisted of 75 patients with normal or mildimpairment in LV function, whereas group 2 consisted of 27patients with moderate or severe LV dysfunction.
All patients were premedicated with morphine, 0.1mg/kg, and scopolamine, 0.2 to 0.4 mg, intramuscularly(1M), 1 hour prior to arrival in the operating room. Patientswere maintained on their usual doses of tI-blockers, calciumchannel blockers, and nitrates up until and including the
From the Department of Cardiothoracic Anesthesia.Cleveland Clinic Foundation, Cleveland, OH.
Address reprint requests to Charles E. Smith, MD,FRCPC, Department of Anesthesia, Metro Health MedicalCenter, 3395 Scranton Rd. Cleveland. OH 44109.
© 1990 by W.H. Saunders Company.0888-6296/90/0406-0003$03.00/0
Journal ofCardiothoracic Anesthesia, Vol 4, No 6 (December). 1990: pp 681-686 681

682
morning of surgery. Heart rate, MAP, central venous pressure, mean pulmonary artery pressure, and pulmonary artery, bladder, and lower esophageal temperatures were measured and recorded continuously; pulmonary capillary wedgepressure was recorded intermittently. CO was determined bythermodilution. The choice of anesthetic was at the discretionof the attending anesthesiologist, but generally consisted of ahigh-dose narcotic (fentanyl or sufentanil) muscle relaxanttechnique supplemented with either benzodiazepines (diazepam, midazolam), enflurane, droperidol, or ketamine. Thepatient's lungs were ventilated with 100% oxygen in order tomaintain normocarbia using a nonrebreathing system.
During CPB, nonpulsatile flow, systemic hypothermia, and electrolyte priming solutions were used. Temperature-uncorrected (alpha-stat) blood gas management wasused. Phenylephrine and nitroprusside were used as necessaryto maintain MAPs between 60 and 80 mm Hg during CPB.Myocardial protection was with cold, hyperkalemic blood oroxygenated crystalloid cardioplegia. When the aorta wascross-clamped, the lungs were deflated and not ventilated orperfused.
Weaning from CPB was accomplished after rewarming to a bladder temperature of 37°C, normalization ofarterial blood gases, and correction of serum ionized calcium.Atrial or atrioventricular sequential pacing was generallyused for heart rates less than 80 beats/min prior to weaningoffCPB.
Inotropic drug therapy was considered necessary forcardiac indices less than 2.0 L/min/m2 despite optimal heartrate and ventricular filling pressures. The choice of inotrope(dobutamine, epinephrine, isoproterenol, dopamine, ephedrine) was at the discretion of the anesthesiologist. Phenylephrine boluses (50 to 100 /Lg) were administered alone or inconjunction with inotropic medication in order to maintainMAPs at preoperative levels (generally between 60 and 80mm Hg). Norepinephrine infusion was used to treat severehypotension (MAP < 50 mm Hg) associated with a low SVR« 600 dyne. sec· cm"). Nitroprusside and/or nitroglycerin were used to treat systemic hypertension (MAP> 100mm Hg) after CPB. These vasodilators were also used inconjunction with inotropic medications in order to optimizeventricular function. All vasoactive medications administeredduring emergence from CPB and the respective dosages wererecorded.
Hemodynamic measurements were obtained at fivestudy intervals: (1) baseline, prior to induction; (2) duringhypothermic CPB with the aorta cross-clamped; (3) duringnormothermic CPB after release of the aortic clamp; (4) Iminute after separation from CPB; and (5) 15 minutes afterseparation. During CPB, CO was considered equivalent tothe nonpulsatile bypass flow.
The number of patients requiring inotropic and/orvasopressor drug support after CPB was compared betweengroups using x2 analysis. The total cumulative dose ofphenylephrine required in the first 15 minutes followingcessation of CPB was compared between groups using theStudent's t test. Preoperative and intraoperative variableswere compared between groups using x2 and Student's t test,with the Bonferroni correction when applicable. Results areexpressed as mean ± standard error ofthe mean (SEM). A Pvalue < 0.05 was considered significant.
SMITH ET AL
RESULTS
Preoperative and intraoperative patient dataare summarized in Table 1. Group 2 had a higherincidence of myocardial infarction prior to surgery than did group 1. Otherwise, there were nosignificant intergroup differences. None of thepatients required intraaortic balloon pump support or left-heart assist device following CPB.Hemodynamic data are shown in Table 2. Therewere no significant differences between groups atany study interval.
Inotropic and vasopressor drug therapyduring emergence from CPB is summarized inTable 3. A total of 37 patients in group 1 (49.3%)
Table 1. Perioperative Data
Group 1 Group 2(n = 75) In = 27)
Age (yr) 63.1 ± 1.3 62.8 ± 2.1Weight (kg) 79.3 ± 1.7 80.9 ± 2.1Surface area (m2
) 1.88 ± 0.03 1.92 ± 0.04Male/female 62/13 24/3Previous MI 29 (39) 17 (63)-
Within 3 months 13 (17) 8 (30)-
Within 3 to 6 months 4 (5) 4 (15)-
Previous CABG 19 (25) 6 (22)History of CHF 1(1) 1(4)
Diabetes on insulin 8 (11) 1(4)
Hypertension 20(27) 5 (19),a-Blockers 32 (43) 13(48)Calcium blockers 57 (76) 22 (82)
Nifedipine 16 (21) 8(30)Diltiazem 38 (51) 13 (48)
Verapamil 3(4) 1(4)
Anesthetic agentFentanyl/sufentanil 33/41 16/10Diazepam/midazolam 45/14 17/6Droperidol/ketamine 11/8 4/1Enflurane 43 (57) 11(41)
Morphine/thiopental 3/2 0Prebypass time (min) 107.8 ± 4.9 107.6 ± 7.9Aortic clamp (min) 67.7 ± 3.2 73.2 ± 5.8Bypass (min) 106.7 ± 4.7 125.5 ± 10.7Rewarming (min) 47.7 ± 1.8 55.7 ± 4.8PeakT (OC) 38.6 ± 0.13 38.8 ± 0.18Peak T > 38°C (min) 12.5 ± 1.3 15.6 ± 2.4Distal grafts Ino.) 3.2 ± 0.2 3.5 ± 0.3Cardioplegia type
Blood/crystalloidt 46/28 17/8
NOTE. All values given as mean ± SEM. Numbers inparentheses are percentages.
Abbreviations: MI, myocardial infarction; CABG, coronaryartery bypass grafting; CHF. congestive heart failure: Hypertension, BP > 160/100 mm Hg or on antihypertensives; T, peakinflow rewarming temperature.
- P < 0.05 between groups.tThree missing data points.

a-ADRENERGIC DRUGS AFTER BYPASS 683
Table 2. Cardiovascular Parameters
CPB Emergence From CPB
94 ± 294 ± 2
68 ± 269 ± 3
8 ± 0.410 ± 1
2.8 ± 0.12.6 ± 0.1
1 Minute 15 Minutes
87 ± 1 86 ± 193 ± 2 94 ± 2
72 ± 1 80 ± 176 ± 2 79 ± 2
21 ± 21 ± 123 ± 22 ± 1
12 ± 1 12 ± 112 ± 1 13 ± 1
10 ± 0.4 10 ± 111 ± 1 10 ± 1
2.7 ± 0.1 2.8 ± 0.12.7 ± 0.1 2.9 ± 0.1
1,040 ± 42 1,126 ± 391,074 ± 68 1,005 ± 49
37.2 ± 0.1 36.1 ± 0.137.5 ± 0.2 36.6 ± 0.1
27.3 ± 0.527.0 ± 0.6
1.20 ± 0.021.19 ± 0.04
72 ± 375 ± 7
7 ± 111 ± 1
9 ± 110 ± 1
70 ± 1
66 ± 2
2.3 ± 0.12.4 ± 0.1
Unclamped
24.7 ± 0.424.5 ± 0.6
36.4 ± 0.336.6 ± 0.5
1,186 ± 351,046 ± 59
64 ± 267 ± 2
8 ± 1
8 ± 1
7 ± 1
7 ± 1
2.1 ± 0.12.1 ± 0.1
1.05 ± 0.021.04 ± 0.03
24.9 ± 0.526.0 ± 0.6
24.0 ± 0.525.0 ± 0.6
Cross-Clamped
1,218 ± 441,217 ± 59
1.14 ± 0.011.15 ± 0.01
40.3 ± 0.540.2 ± 1.0
36.0 ± 0.136.2 ± 0.1
1,413 ± 471,389 ± 67
Baseline
Heart rate (beats/min)
Group 1
Group 2
Mean arterial pressure (mm Hg)
Group 1
Group 2Mean pulmonary pressure (mm Hg)
Group 1 22 ± 1Group 2 25 ± 2
Pulmonary capillary wedge pressure (mm Hg)
Group 1 12±1Group 2 14 ± 1
Central venous pressure (rnrn Hg)
Group 1
Group 2Cardiac index (L/min/m2
)
Group 1
Group 2Systemic resistance (dyne· s • cm- 5
)
Group 1
Group 2Pharyngeal temperature (0 C)
Group 1
Group 2Hematocrit (%)
Group 1
Group 2Ionized calcium (mEq/L)
Group 1
Group 2
NOTE. Values given as mean ± SEM. There were no significant differences between groups.
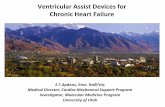
and 11 patients in group 2 (39.2%) required someform of inotropic and/or vasopressor supportafter CPB (P = NS). There were no intergroupdifferences in the incidence of patients requiringinotropes and vasodilators or inotropes and vasopressors after CPB (Fig 1). Fewer group 2
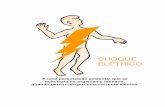
patients required only vasopressor medicationafter CPB compared with patients in group 1(14.8 v 32.0%, P < 0.05; Fig 1). However, group2 patients required significantly greater cumulative doses of phenylephrine after CPB comparedwith group 1 patients (1.69 ± 0.70 mg, n = 8, v
Table 3. Number of Patients (%) Requiring Vasoactive
Drug Therapy During Emergence From CPB
NOTE. There were no significant differences between
groups. Some patients received more than one drug.
Phenylephrine
Norepinephrine
Dobutamine
Calcium chloride
Epinephrine
Ephedrine
Dopamine
Isoproterenol
Nitroglycerin
Nitroprusside
Group 1 In = 75)
27 (36)4 (5)
9 (12)59 (79)
4 (5)
2 (3)
1(1)
1(1)
19 (25)14 (19)
Group2 (n = 27)
9 (33)2 (7)
6 (22)
23 (85)1 (4)
2 (7)
6 (27)4(15)
a.. 40::J o GROUP10 n=24 ~ GROUP2a:CJ 30u,0r- 20zw *o n=4 n=4a:w 10a..
VASOPRESSORS INOTROPES INOTROPESONLY & &
VASODILATORS VASOPRESSORS
Fig 1. Percent of patients requiring vasoactivedrug support during separation from CPB. • P < 0.05between groups.

684 SMITH ET AL
Fig 2. Cumulative dose of phenylephrine lIeft) andaverage dose of norepinephrine infusion (right! in patientsduring separation from CPB. • P < 0.05 between groups.
volemic hemodilution with hetastarch significantly blunted the vasoconstrictor response tonorepinephrine in the rat hindquarter vascularbed. This decreased vascular responsiveness maybe caused by diminished oxygen delivery to thetissues, which may trigger local vasodilatationdue to hypoxia or local vasodilator metabolites.l''Similarly, temperature changes during rewarming and following release of the aortic crossclamp may also affect a-adrenergic responsiveness, perhaps due to the effect of temperatureand shear rate on the relative viscosity of theblood. 4
,1l .12 However, the degrees of hemodilution and temperature changes were unlikely tohave played an important role in the presentstudy, because there were no intergroup differences in hematocrit during and after CPB, andboth groups experienced a similar pattern ofrewarming in terms of peak inflow temperaturesof the heat exchanger, duration of rewarming,and lower esophageal-bladder temperature gradients prior to weaning from CPB.
Schwinn et al 3 have shown that patientswith low ejection fractions undergoing CABGrequired higher doses of phenylephrine to increase MAP by 20% (PD20), although the degree of scatter of the PD20 at low ejectionfractions was similar to that observed in patientswith normal ejection fractions. The altereda-adrenergic responsiveness in patients with LVdysfunction was not evident during hypothermicCPB with the aorta cross-damped, suggestingthat in the study of Schwinn et al, other factorssuch as altered phenylephrine pharmacokineticsor elevated plasma catecholamines during CPBmay have exerted significant influencing effects.'Because the conduct of CPB was similar for bothgroups in the present study, it is difficult toinvoke altered phenylephrine pharmacokineticsor elevated plasma catecholamines during CPBas the cause of the increased dose of o-adrenoceptor agonist required after CPB in group 2.
Calcium channel blocking drugs can produce vasodilatation and modify the vascularresponsiveness to e-adrenoceptor agonists. 11,13-1S
However, the groups were similar with respect topreoperative calcium channel blocking drug therapy (nifedipine, diltiazem, and verapamil), andall patients received their usual doses of calciumchannel blockers up until and including themorning of surgery. It is known that anesthetic
o0.0 l----l_
o Group 1 ....3.0 fa Group 2 15 II:
ii E! <,.. * !....III •0 III'a 2.0 10 0.. 'a
f •II:.II: 'CGo .II:
.! Do•>- 1.0 5 II:II: 'I... f.II:Go 0
Z
0.24 ± 0.04 mg, n = 27, P < 0.05; Fig 2). Similarly, the dose of norepinephrine infusion ingroup 2 was 3.3 times that in group 1 (10 ± 6/oLg/min, n = 2, v 3 ± 0.6 /oLg/min, n = 4), butdue to the small number of patients requiringnorepinephrine, this did not achieve statisticalsignificance. The dose of calcium chloride wassimilar between groups 1 (1.0 ± 0.05 g) and 2(1.1 ± 0.11 g), as was the dose of dobutamine(6.7 ± 0.7 v 6.3 ± 0.9 /oLg/kg/min, respectively).
DISCUSSION
Discontinuance of CPB following CABGrepresents a critical period during which theheart must gradually resume the hydraulic workload of the circulation: pressure x flow." Although weaning from CPB is often accomplishedwithout pharmacological intervention, o-adrenoceptor agonists such as phenylephrine and, occasionally, norepinephrine may be required to increase SVR and maintain blood pressure.'
The present study documented that duringweaning from CPB, patients with moderate andsevere LV dysfunction (group 2) required higherdoses of phenylephrine and norepinephrine tomaintain MAP compared with patients in group1. These differences may be due to variation ino-adrenoceptor-mediated arterial sensitivity between groups."" Several factors may affecto-adrenoceptor-mediated arterial sensitivity, including blood viscosity changes due to acutenormovolemic hemodilution, and temperaturechanges during the rewarming phase of CPB.Estafanous et al 9 demonstrated that acute normo-

a-ADRENERGIC DRUGS AFTER BYPASS
agents can modify SVR and, therefore, have thepotential to alter a-adrenergic pressor responsiveness to phenylephrine and norepinephrine. Although no attempts were made to standardize theanesthetic drugs in the present study, the majority of patients received fentanyl or sufentanil astheir primary anesthetic, and there were nodifferences between groups with respect to primary or supplemental anesthetic agents.
It is possible that the decreased a-adrenergic responsiveness in group 2 was due to differences in o-adrenoceptor agonist affinity and/orreceptor density." a-Adrenergic hyporesponsiveness (phenylephrine and norepinephrine) of vascular contractility has been previously describedin rabbits." However, Zucker and Amory'? wereunable to document any down-regulation of platelet a2-adrenergic receptors in patients undergoing CABG after CPB. Bristow et ai's showedthat ai-adrenergic receptor density was maintained at normal levels in failing human ventricular myocardium without any evidence of downregulation, although the biological significanceof these findings is uncertain because the actualreceptor density and biochemical responses of theai-receptor population were of low magnitude inboth normal and failing human hearts.
The two groups were well matched in termsof preoperative and intraoperative characteristics except for degree of LV dysfunction andhistory of myocardial infarction. The increasedfrequency of myocardial infarctions (especiallyrecent infarcts) in group 2 patients was mostlikely the cause of impaired LV function in thisgroup. It is possible that some degree of recoveryof LV function may have occurred in group 2patients following cardiac catheterization, whichmay have accounted for the similarity of baselinehemodynamics between groups, although all patients underwent cardiac catheterization within 3to 4 weeks of surgery. The influence of preoperative LV dysfunction on the early and late courseof CABG has been well documented. '9·2' TheCASS study demonstrated a strong associationbetween operative mortality and LV ventriculardysfunction'P; whereas Goenen et at2 reportedthat patients with preoperative LV dysfunctionhave an increased need for preoperative andpostoperative intraaortic balloon pump and inotropic drug therapy in the intensive care unit.However, the use of inotropic drug support dur-
685
ing weaning from CPB in their study was independent of LV dysfunction.i In the present study,there was a similar lack of concordance of LVdysfunction and use of inotropic drugs to assist inseparation from CPB. This suggests that factorsother than the degree of preoperative LV dysfunction, such as inadequate myocardial protectionduring CPB and/or suboptimal myocardial revascularization, are of considerable importance indetermining the immediate need for inotropicmedications after CPB, especially in patientswith normal preoperative LV function. This maybe due to the deterioration of biventricular function after revascularization procedures in patients, regardless of preoperative LV function.'However, the requirement for inotropic supportin the intensive care unit following CABG maybe expected to be higher in patients with impaired LV function, as observed by Goenen et a1.2
This is probably because patients with normalLV function have recovery of biventricular depression to 90% of control within 4 hours following revascularization, whereas patients with depressed LV function (ejection fraction < 0.45)have depressed biventricular function that persists for 24 hours after revascularization.'
Compared with group 1, fewer group 2patients required direct-acting vasoconstrictorsalone after CPB. This may be because patientswith moderate-severe LV dysfunction were lesslikely to have a combination of increased CO andlow MAP and SVR during emergence fromCPB, which. were the primary indications foradministering phenylephrine alone. It can bespeculated that the administration of a-adrenergic agonist agents to group 2 patients may haveincreased SVR to a point at which this couldhave decreased forward flow of blood from theimpaired LV. Indeed, group 2 patients were morelikely to be treated with a combination of vasopressors and inotropes compared with group 1(15% v 9%), although this difference was notstatistically significant.
In summary, following CABG, patientswith moderate-severe LV dysfunction may require higher doses of a-adrenoceptor agonistscompared with patients with normal or mildlyimpaired LV function. This decreased a-adrenergic responsiveness may be due to differences ino-adrenoceptor agonist affinity and/or receptornumber.

686
REFERENCES
SMITH ET AL
1. Mangano DT: Biventricular function after myocardial revascularization in humans: Deterioration and recoverypatterns during the first 24 hours. Anesthesiology 62:571577,1985
2. Goenen M, Jacquemart JL, Galvez S, et al: Preoperative left ventricular dysfunction and operative risks incoronary bypass surgery. Chest 92:804-806, 1987
3. Schwinn DA, McIntyre RW, Hawkins ED, et al:aI-Adrenergic responsiveness during coronary artery bypasssurgery: Effect of preoperative ejection fraction. Anesthesiology 69:206-217, 1988
4. Tinker JH, Roberts SL: Management of cardiopulmonary bypass, in Kaplan JA (ed): Cardiac Anesthesia.Philadelphia, PA, Grune & Stratton, 1987, pp 895-926
5. Arkin DB, Saidman LJ, Benumof JL: Case historynumber 98: Hypotension following cardiopulmonary bypass.Anesth Analg 56:720-724,1977
6. Bevan JA, Oriowo MA, Bevan RD: Physiologicalvariation in o-adrenoceptor-mediated arterial sensitivity:Relation to agonist affinity. Science 234:196-197,1986
7. Bevan JA: Control of peripheral vascular resistance: Evidence based on the in vitro study of resistancearteries. Clin Invest Med 10:568-572, 1987
8. McGrath JC: Evidence for more than one type ofpostjunctional o-adrenoceptor. Biochem Pharmacol 31:467484, 1982
9. Estafanous FG, Sheng Z, Pedrinelli R, et al:Hemodilution affects the pressor response to norepinephrine.J Cardiothorac Anesth 1:36-41, 1987
10. Guyton AC: Local control of blood flow by thetissues and nervous and humoral regulation, in Textbook ofMedical Physiology (ed 6). Philadelphia, PA, Saunders,1981, pp 232-245
II. Massagee JT, McIntyre RW, Kates RA, et al:Effects of preoperative calcium entry blocker therapy ona-adrenergic responsiveness in patients undergoing coronaryrevascularization. Anesthesiology 67:485-491, 1987
12. Barbee JH: The effect of temperature on therelative viscosityof human blood. Biorheology 10:1-5, 1973
13. van Zwieten PA, Timmermans PBMWM,Thoolen MJMC, et al: Calcium dependency of vasoconstriction mediated by (Xl- and a2-adrenoceptors. J CardiovascPharmacoI7:S113-S120, 1985 (suppI6)
14. Vanhoutte PM: Heterogeneity of postjunctionalvascular a-adrenoceptors and handling of calcium. J Cardiovase Pharmacol 4:S91-S96, 1982 (suppl 1)
15. van Zwieten PA, Van Meel JCA, TimmermansPBMWM: Calcium antagonists and a2-adrenoceptors; possible role of extracellular calcium ions in a2-adrenoceptormediated vasoconstriction. J Cardiovasc Pharmacol 4:273279,1982
16. Maze M, Prokocimer P, Spiss CK, etal: Adrenergic hyporesponsiveness of vascular contractility followingepinephrine infusion. Anesthesiology 63:A116, 1985
17. Zucker JR, Amory DW: Platelet a-adrenergicreceptors are not down-regulated during cardiopulmonarybypass. Anesthesiology 63:449-451, 1985
18. Bristow MR, Minobe W, Rasmussen R, et al:aI-Adrenergic receptors in the nonfailing and failing humanheart. J Pharmacol Exp Ther 247:1039-1045,1988
19. Hochberg MS, Parsonnet V, Gielchinsky I, et al:Coronary artery bypass grafting in patients with ejectionfractions below forty percent. J Thorac Cardiovasc Surg86:519-527,1983
20. Hung J, Kelly DT, Baird DK, et al: Aortocoronary bypass grafting in patients with severe left ventriculardysfunction. J Thorac Cardiovasc Surg 79:718-723, 1980
21. Alderman EL, Fisher LD, Litwin P, et al: Resultsof coronary artery surgery in patients with poor left ventricular function (CASS). Circulation 68:785-795,1983
22. Kennedy JW, Kaiser GC, Fisher LD, et al:Multivariate discriminant analysis of the clinical and angiographic predictors of operative mortality from the collaborative study in coronary artery surgery (CASS). J ThoracCardiovasc Surg 80:876-887,1980