Guide to the interpretation of Cardiopulmonary Exercise ...
21
Guide to the interpretation of Cardiopulmonary Exercise Testing Dr. Ines Frederix December 2014
Transcript of Guide to the interpretation of Cardiopulmonary Exercise ...

Guide to the interpretation of
Cardiopulmonary Exercise Testing
Dr. Ines Frederix December 2014

Copyright: Ines Frederix

Copyright: Ines Frederix
1 Ergospirometry: parameter description .............................................................................. 5
1.1 Cardiovascular parameters .......................................................................................... 5
1.1.1 Heart rate (HR) ..................................................................................................... 5
1.1.2 Blood pressure (BP) ............................................................................................. 5
1.1.3 Oxygen consumption (VO2) ................................................................................. 5
1.1.4 Oxygen pulse (π O2) ............................................................................................. 5
1.2 Metabolic parameters .................................................................................................. 6
1.2.1 Respiratory exchange ratio (RER) ....................................................................... 6
1.2.2 (First) Anaerobic threshold (AT1, VT1) .............................................................. 6
1.2.3 (Second) Anaerobic threshold (AT2, VT2, RCP) ................................................ 6
1.3 Ventilatory and pulmonary gas exchange parameters ................................................. 6
1.3.1 Minute ventilation (VE) ....................................................................................... 6
1.3.2 Carbon dioxide output (VCO2) ............................................................................ 6
1.3.3 Tidal volume (VT) and breathing frequency (fR) ................................................ 7
1.3.4 VD/VT .................................................................................................................. 7
1.3.5 Oxygen saturation (SaO2) .................................................................................... 7
1.3.6 Carbon dioxide respiratory equivalent (VE/VCO2) ............................................. 7
1.3.7 Oxygen respiratory equivalent (VE/VO2) ........................................................... 7
1.3.8 PET O2 and PET CO2 ......................................................................................... 7
1.3.9 VE/VCO2 slope .................................................................................................... 7
1.3.10 1.3.10 Ventilatory reserve (VR) ........................................................................... 7
2 Typical ergospirometry patterns, associated with specific pathologies/conditions ........... 9
2.1 Cardiovascular pathologies .......................................................................................... 9
2.1.1 Heart failure (HF), diagnostic evaluation ............................................................. 9
2.1.2 Heart Failure (HF), prognostic evaluation ........................................................... 9
2.1.3 Coronary artery disease ...................................................................................... 10
2.2 Respiratory pathologies ............................................................................................. 10
2.2.1 Chronic Obstructive Pulmonary Disease (COPD) ............................................. 10
2.2.2 Interstitial Lung Disease (ILD) .......................................................................... 11
2.2.3 Pulmonary Vascular Disease (PVD) .................................................................. 11
2.3 Neuromuscular pathologies ....................................................................................... 13
2.3.1 Mitochondrial myopathy .................................................................................... 13
2.4 Other pathologies/conditions ..................................................................................... 13
2.4.1 Deconditioning ................................................................................................... 13
2.4.2 Hyperventilation syndrome/Anxiety .................................................................. 13
2.4.3 Obesity ............................................................................................................... 14
2.4.4 Poor effort and malingering ............................................................................... 14

Copyright: Ines Frederix
2.5 Summary of pathology specific ergosprimetry patterns ............................................ 15
3 Algorithm for ergospirometry analysis ............................................................................ 16
3.1 What is the indication for the ergospirometry? ......................................................... 16
3.2 Assess patient’s history, clinical examination, other examinations (RxTx, ECG,
PFTs, etc.) ............................................................................................................................ 16
3.3 Was the ergospirometry maximal? ............................................................................ 16
3.4 Is aerobic capacity (VO2 max) normal? .................................................................... 16
3.5 Does cardiovascular function contribute to exercise limitation? ............................... 16
3.6 Does ventilatory function (respiratory mechanics) contribute to exercise limitation?
16
3.7 Does pulmonary gas exchange (hypoxemia, inefficient ventilation, increased dead
space ventilation) contribute to exercise limitation? ............................................................ 17
3.8 Integrate all results in final conclusion(s) .................................................................. 17
4 Reference values .............................................................................................................. 19
5 Graphic representation of cardiopulmonary exercise response in healthy person ........... 20
6 References ........................................................................................................................ 21

Ines Frederix 5
1 Ergospirometry: parameter description
1.1 Cardiovascular parameters
1.1.1 Heart rate (HR)
In healthy subjects, HR increases nearly linearly with increasing VO2; initially due to vagal
withdrawal and subsequently due to increased sympathetic activity. Achievement of age-
predicted values for maximal HR during exercise is often used as one of the markers to define
a maximal ergospirometry test (and hence VO2 max). The most widely used reference value
equation for maximal HR is: HR max predicted = 220-age (years). The difference between the
age-predicted maximal HR and the maximal HR achieved during ergospirometry is called the
Heart Rate Reserve (HRR). Normally HRR < 15 beats/min; in case of a maximal exercise
test. When the HRR is zero, there is cardiovascular limitation to exercise (in healthy subjects
cardiovascular, rather than ventilatory limitation is mostly observed). When the HR max <
85% HR max predicted; there is chronotropic incompetence.
Note: the effect of beta-blockers on HR.
1.1.2 Blood pressure (BP)
Systolic BP typically rises progressively during incremental exercise, diastolic BP remains
constant or slightly declines. If systolic BP does not increase with exercise, or in fact declines;
the exercise test should be terminated since this could indicate a serious abnormality such as
HF, ischemia, aortic stenosis, … . Maximal BP’s during exercise testing are 220/90 mmHg.
1.1.3 Oxygen consumption (VO2)
VO2 is defined as the volume of O2 extracted from inspired air in a given period of time. It
can be expressed by the Fick equation, that is: VO2= Qc x C(a-v)O2. This VO2 max is
defined during incremental exercise testing, as the VO2 attained during the VO2 plateau
phase; when the VO2 plateaus despite work rate continuing to increase. The VO2 max is the
gold standard to define a patient’s aerobic capacity. It is influenced by cardiovascular
(central), pulmonary (central) and muscular (peripheral) function.
To calculate VO2 for a maximal incremental cycle exercise test, we use the following
formula:
Male: W (predicted weight ie. 0,79xH – 60,7) x [50,75-0,372 (A)]
Female: (W (predicted weight ie. 0,65xH -42,8) + 43) x [22,78 – 0,17 (A)]
W(eight) in kg, H(eight) in centimeters, A(ge) in years
Normal value for VO2 max: VO2 max > 84% predicted (Ref. 1), > 100% predicted (Ref. 2).
1.1.4 Oxygen pulse (π O2)
The π O2 is defined as: π O2= VO2/HR=SV x C (a-v)O2. The basic profile for the π O2 is to
initially increase in a hyperbolically fashion, followed by a slow approach to an asymptotic

Ines Frederix 6
value. A low, unchanging or flat π O2; with increasing work rate may be interpreted as
resulting from a reduced SV. The normal absolute value of π O2 is > 80%.
1.2 Metabolic parameters
1.2.1 Respiratory exchange ratio (RER)
The RER is defined as : RER= VCO2/VO2. The RER is determined by the fuels used for
metabolism. RER is 1 for carbohydrates; RER is 0,7 for lipids and RER is 0,85 for
carbohydrates and lipids. A RER > 1,1 is one of the criteria to define a maximal exercise test.
1.2.2 (First) Anaerobic threshold (AT1, VT1)
The AT1 is defined as the moment when there is a transition between no or little lactate
accumulation; to a sustained increase in lactate accumulation. It corresponds to the VO2
above which anaerobic energy production substantially supplements aerobic energy
production. It is valuable in setting the intensity for exercise prescription in a highly
individualized manner. Normally AT1 equals > 40% VO2 max predicted (wide range of
normal 40-80%).
AT1 can be determined in different ways:
1. V-slope method: AT1 is identified as the VO2 at which the change in slope of the
relationship of VO2 to VCO2 occurs.
2. Respiratory equivalent method: AT1 is defined as the VO2 at which there is
significant increase in the VO2 respiratory equivalent, without concomitant increase in
the VCO2 respiratory equivalent.
3. PET method: AT1 corresponds to the increase in PET O2 (because of
hyperventilation) with no simultaneous decrease in PET CO2.
1.2.3 (Second) Anaerobic threshold (AT2, VT2, RCP)
AT2 is defined as the VO2 (% VO2 max) at which the carbon dioxide respiratory equivalent
starts to increase (after an initial decrease). AT2 marks the onset of hyperventilation
(“respiratory compensation”) during incremental exercise. It physiologically reflects the
failing of the body’s buffering mechanisms; which leads to metabolic (lactic) acidosis.
Normally AT2 is 60-90% VO2 max predicted.
1.3 Ventilatory and pulmonary gas exchange parameters
1.3.1 Minute ventilation (VE)
VE is the volume of expired air exhaled from the lungs in 1 minute . The VE is calculated as:
VE = VT x fB. With incremental exercise testing; VE increases progressively. The rise in VE
with exercise is primarily associated with an increase in VT during low levels of exercise. As
exercise progresses, both VT and fB increase until 70-80% of peak exercise; thereafter fB
predominates.
1.3.2 Carbon dioxide output (VCO2)
VCO2 is defined as the amount of CO2 exhaled from the body per unit of time.

Ines Frederix 7
1.3.3 Tidal volume (VT) and breathing frequency (fB)
See I.3.1. Normally the maximal fB is <60 breaths/min.
1.3.4 VD/VT
The VD/VT ratio is an index of gas exchange efficiency. An increase in VD/VT reflects an
increased inefficiency of ventilation; due to V/Q mismatching or a right-to-left shunt.
Normally VD/VT is 0,30-0,40 in rest. The ratio typically decreases initially with increasing
exercise intensity due to increasing VT. Patients with respiratory disease may have at rest
either normal or elevated values that fail to decrease normally or may even increase during
exercise.
1.3.5 Oxygen saturation (SaO2)
SaO2 is the actual amount of O2 bound to hemoglobin in a given volume of arterial blood.
1.3.6 Carbon dioxide respiratory equivalent (VE/VCO2)
VE/VCO2 corresponds to the number of liters of air that are being breathed to eliminate 1
liter of CO2. Normally minimal VE/VCO2 equals < 30.
1.3.7 Oxygen respiratory equivalent (VE/VO2)
VE/VO2 corresponds to the number of liters of air that are being breathed for each liter of O2
uptake.
Note: The normal pattern of change in VE/VO2 is a drop early in exercise to its nadir near the
AT1, and then an increase as maximal exercise capacity is approached. The VE/VCO2 also
decreases hyperbolically as work rate increases. For incremental tests, the increase in
VE/VO2, that typically occurs in concert with the development of metabolic acidemia (AT1)
occurs at a time when VE/VCO2 has not yet increased. It is this profile that separates this
response from the onset of hyperventilation from other causes (e.g. anxiety), in which case
both VE/O2 and VE/VCO2 would increase in concert. The normal subsequent increase in
VE/VCO2 reflects the onset of frank compensatory hyperventilation for metabolic acidosis,
with concomitant reduction in PET CO2.
1.3.8 PET O2 and PET CO2
End-tidal PO2 and PCO2.
1.3.9 VE/VCO2 slope
During normal incremental exercise testing; VE correlates closely with VCO2 in a linear
fashion. The slope of this relationship in normal subjects is 23-25 (Ref. 1), < 30 (Ref. 2).
1.3.10 Ventilatory reserve (VR)
The VR is the difference between the ventilatory capacity and the ventilatory demand. The
ventilatory capacity is defined by the MVV (Maximal Voluntary Ventilation). MVV is
calculated as: MVV= FEV1 x 35-40. The ventilatory demand is defined by the VE max. To
calculate the VR; we use the following formula: VR= VEmax/MVV. Normally during
maximal exercise testing; the VE/MVV ratio is 72 ± 15% (Ref. 1), ≤ 80% (Ref. 2). Patients
with pulmonary disease characteristically have reduced VR; in contrary to healthy people

Ines Frederix 8
where the exercise test is usually ended by cardiovascular limitation. Thus, VE/MVV has
diagnostic utility in determining if unexplained exertional dyspnea is related to a pulmonary
mechanism.

Ines Frederix 9
2 Typical ergospirometry patterns, associated with specific
pathologies/conditions
2.1 Cardiovascular pathologies
2.1.1 Heart failure (HF), diagnostic evaluation
For the cardiovascular parameters:
VO2 max: The VO2 max is reduced, reflecting an insufficient increase in cardiac output
during exercise.
∆VO2/∆W slope: In heart failure this slope is typically decreased due to circulatory
insufficiency.
πO2: Flattening of the πO2 during incremental exercise, reflects the fall in SV.
For the ventilatory parameters:
VE/MVV: In general, for patients with heart failure, the cardiopulmonary exercise tests
usually are not ventilatory limited. The presence of VE/MVV approaching or exceeding
100% of predicted (reduced VR), signals the presence of combined cardiovascular and
respiratory limitation and may suggest concurrent pulmonary disease.
VD/VT: The VD/VT is increased due to reduced cardiac output for the metabolic rate; and
hence V/Q mismatching.
VE/VCO2: The VE/VCO2 is increased due to abnormal V/Q relationships due to low
cardiac output for the metabolic rate, subclinical interstitial pulmonary edema,….. .
VE/VCO2 slope > 30 suggests increased filling pressures. Specifically for patients with
heart failure with a preserved EF (HFpEF), exercise-induced pulmonary hypertension is
characterized by high VE/VCO2’s.
For the metabolic parameters
AT1: The AT1 is usually decreased; reflecting the circulatory insufficiency and early onset
of lactic acid metabolism.
2.1.2 Heart Failure (HF), prognostic evaluation
Prognostic markers in patients with HF
VO2 max: The VO2 max is considered one of the most robust prognostic markers in
chronic heart failure. A VO2 max of 11 mL/min/kg seems to be the lower threshold for an
unfavorable prognosis.
VE/VCO2 slope: The VE/VCO2 slope provides additional prognostic information in
chronic heart failure patients; The higher the slope, the worse the prognosis.
Respiratory oscillations: The presence of respiratory oscillations is a negative prognostic
marker. It reflects advanced disease severity and poor prognosis in patients with heart
failure.

Ines Frederix 10
Table 1: Indicates the prognostic and diagnostic stratification for patients with heart
failure.
Heart Failure
VE/VCO2 slope Peak VO2
(mL/kg x min)
Respiratory
oscillations
Blood pressure
< 30:
Ventilatory Class I
>20:
Weber Class A
Not present
Rise in systolic BP
during CPET
30-36:
Ventilatory Class II
16-20:
Weber Class B
Not present
Flat systolic BP response
during CPET
36-45:
Ventilatory Class III
10-16:
Weber Class C
Present
Flat systolic BP response
during CPET
≥ 45:
Ventilatory Class IV
< 10:
Weber Class D
Present
Drop in systolic BP
during CPET
2.1.3 Coronary artery disease
During exercise testing; the onset of myocardial ischemia impairs ventricular contraction and
relaxation functions, thereby reducing the increase in cardiac output during exercise and
raising filling pressures.
For the cardiovascular parameters:
∆VO2/∆W slope: The ∆VO2/∆W slope typically starts to flatten and/or decline in case of
myocardial ischemia. The normal average slope is 10 mL/min x W.
πO2: Flattening of the πO2 during exercise, reflects the inability to adequately increase SV
due to myocardial ischemia. Concurrent compensatory more rapid increase in heart rate with
respect to work load is often noted.
For the ventilatory parameters:
VE/VCO2: An increased VE/VCO2 reflects increased filling pressures with exercise.
2.2 Respiratory pathologies
2.2.1 Chronic Obstructive Pulmonary Disease (COPD)
For the cardiovascular parameters:
VO2 max: The VO2 max is reduced in case of severe COPD, and is normal in mild
COPD.

Ines Frederix 11
∆VO2/∆W slope: This slope is usually normal, in contrary to cardiovascular pathologies
(HF, coronary artery disease).
HRR: There is usually a significant HRR, a reflection that the cardiovascular system has
been relatively unstressed.
For the ventilatory parameters:
VE/MVV: One of the distinguishing features of many patients with moderate to severe
COPD is a reduced VR (VE/VMM approaching or exceeding 100%), signaling a
significant ventilatory contribution to exercise limitation.
VD/VT and VE/VCO2: Both are abnormal reflecting ventilatory inefficiency, due to
increased dead space ventilation.
PaO2: Patients with COPD usually have low PaO2 values at rest. During exercise PaO2
may increase, decrease or remain the same; but is more likely to be reduced in patients
with moderate to severe COPD.
For the metabolic parameter:
AT1: The AT1 response may be normal, low or indeterminate. A low AT1 may reflect
deconditioning due to physical inactivity and/or skeletal muscle dysfunction.
2.2.2 Interstitial Lung Disease (ILD), Restrictive Lung Disease
For the cardiovascular parameters:
VO2 max: The VO2 max is typically reduced.
HRR: The HRR may be increased or normal, since exercise shows ventilatory limitation.
For the ventilatory parameters:
VE/MVV: A reduced VR (high VE/MVV) and ventilatory limitation to exercise are often
seen; primarily reflecting deranged pulmonary mechanics.
VD/VT and VE/VCO2: Inefficient ventilation (increased VE/VCO2 responses) due
primarily to increased VD/VT and also hyperventilation due to hypoxemia and
mechanoreceptor stimulation are usually observed throughout exercise.
PaO2: During exercise, in most patients with significant ILD, impressive arterial
desaturation and abnormal increases in P(A-a)O2 are observed.
For the metabolic parameter:
AT1: The AT1 response can be normal, although a low AT1 commonly occurs and may be
due to pulmonary circulatory and/or RV dysfunction (O2 delivery) and/or skeletal muscle
dysfunction and deconditioning (O2 utilization).
2.2.3 Pulmonary Vascular Disease (PVD)
For the cardiovascular parameters:
VO2 max: The O2 max is usually reduced. These patients’ their exercise tests are usually
cardiovascular limited.

Ines Frederix 12
πO2: The πO2 is often reduced, reflecting the heart’s inability to maintain adequate
cardiac output (CO=SV x HR), in the face of increased pulmonary vascular resistance and
consequent RV afterload.
For the ventilatory parameters:
VE/MVV: As stated above, in PVD patients the exercise test is usually cardiovascular
limited. Hence, there is usually VR at peak exercise.
VD/VT: The VD/VT is usually increased.
VE/VCO2: The VE/VCO2 is typically increased, reflecting inefficient ventilation.
For the metabolic parameter:
AT1: There is usually an early-onset metabolic acidosis (analogous to heart failure and
circulatory insufficiency).
Table 2: depicts the diagnostic and prognostic stratification of patients with PVD.
Pulmonary Vascular Disease
VE/VCO2 slope
Peak VO2
(mL/kg x min)
PET CO2
apex during
exercise
Blood pressure
SaO2
< 30:
Ventilatory Class I
>20:
Weber Class A
> 37 mmHg
Rise in systolic BP
during CPET
No ∆SaO2
30-36:
Ventilatory Class II
16-20:
Weber Class B
36-30 mmHg
Flat systolic BP
response during CPET
> 5% ↓ from
baseline
36-45:
Ventilatory Class III
10-16:
Weber Class C
29-20 mmHg
Flat systolic BP
response during CPET
> 5% ↓ from
baseline
≥ 45:
Ventilatory Class IV
< 10:
Weber Class D
< 20 mmHg
Drop in systolic BP
during CPET
> 5% ↓ from
baseline
(PET CO2 apex achieved at submaximal levels, typically immediately proceeds ventilatory
threshold)

Ines Frederix 13
2.3 Neuromuscular pathologies
2.3.1 Mitochondrial myopathy
In mitochondrial myopathy, a number of genetic mutations can lead to inefficient oxygen
utilization by muscle tissue. If mitochondrial myopathy is suspected, a muscle biopsy would
be warranted to confirm the diagnosis.
For the cardiovascular parameters:
VO2 max: The degree of impairment in VO2 max appears to correlate to the severity of
genetic mutation.
∆VO2/∆W slope: This slope is typically reduced, reflecting the inefficient use of oxygen
by the muscle tissue.
∆Q/∆VO2: In normal circumstances, where oxygen utilization and delivery are well
matched, the ∆Q/∆VO2 slope is 5 L/min. In subjects with mitochondrial myopathies, this
slope is much higher (≥ 7) as oxygen delivery far exceeds the capacity for utilization.
For the ventilatory parameters:
VE/VO2: The VE/VO2 at peak exercise is typically increased, as the ventilatory cost of
VO2 dramatically rises due to aerobic inefficiency by affected skeletal muscle.
For the metabolic parameter:
RER: High RER’s during cardiopulmonary exercise testing are seen in case of
mitochondrial myopathy.
2.4 Other pathologies/conditions
2.4.1 Deconditioning
For the cardiovascular parameters:
VO2 max: The VO2 max is usually normal. However it can be low or at the lower limit of
normal in subjects who are very deconditioned.
πO2: πO2 is typically decreased.
For the ventilatory parameters:
VE/MVV: There is usually a significant ventilatory reserve.
VD/VT and VE/VCO2: The ventilatory response to low levels of exercise is usually
normal. However, increased submaximal VE is observed at any level of VO2 above the
AT1 as a reflection of increased metabolic acidosis, compared with normal subjects.
VD/VT responses are normal, as is the VE/VCO2 slope.
For the metabolic parameter:
AT1: Typically there is early onset of AT1, due to rapid activation of anaerobic
metabolism.
2.4.2 Hyperventilation syndrome/Anxiety
For the cardiovascular parameters:

Ines Frederix 14
VO2 max: These patients have a normal VO2 max.
For the ventilatory parameters:
VE/VCO2: The basic mechanism is increased ventilation as evidenced by abnormal
increases in VE, VE/VCO2, respiratory frequency and respiratory alkalosis (evidenced by
decreased PET CO2 and PaCO2). As an increased VE/VCO2 may reflect inappropriate
ventilation and/or dead space ventilation; arterial PCO2 sampling is recommended. In
contrast to the usual gradual increase in respiratory frequency seen during progressive
exercise, subjects with psychogenic disorders may have an abrupt “turned on” onset of
regular, rapid and shallow breathing disproportionate to the metabolic stress. Also, at the
start of exercise testing, these patients often show an increased breathing frequency (> 20
breaths/min), when compared to normal patients (±10 breaths/min).
2.4.3 Obesity
For the cardiovascular parameters:
VO2 max: VO2 max may be decreased when expressed per kilogram of actual body
weight; or normal when expressed per kilogram of ideal body weight.
πO2: The πO2 is usually normal.
VO2/W slope: in severe obesity, the VO2/W slope is typically increased due to increased
oxygen consumption for a given work load, reflecting the increased metabolic need to
move the bulky legs.
For the ventilatory parameters:
VE/MVV: VE/MVV is usually normal, but may be increased in extreme obesity.
VD/VT and VE/VCO2: These parameters are usually normal in obesity.
Note: in severe obesity, initial pulmonary function tests can show a restrictive pattern.
During exercise testing relatively small tidal volumes (reflecting rapid and superficial
breathing) can be noted.
For the metabolic parameter:
AT1: The AT1 is usually normal.
2.4.4 Poor effort and malingering
This should be suspected in case of early cessation of exercise and a reduced VO2 peak; a
normal or unattained AT1, a low RER value at exercise cessation and a substantial HRR and
VR with no readily apparent peripheral abnormality.

Ines Frederix 15
2.5 Summary of pathology specific ergosprimetry patterns
Table 3: summarizes the most important ergospirometric findings for each of the pathologies discussed in chapter II “Typical ergospirometry
patterns, associated with specific pathologies/conditions”. NA: Not available.
Cardiovascular
Ventilatory
Metabolic
VO2 max or
VO2 peak Peak HR πO2
(VE/MVV)
x100= VR VD/VT
VE/VCO2
(at AT1) PaO2 AT1
Pathology
Cardiovascular
Heart Failure Decreased Variable Decreased Normal or
decreased Increased Increased Normal Decreased
Coronary artery
disease Decreased NA Decreased NA NA Normal/increas
ed
Normal Normal/decreased
Respiratory
COPD Decreased Decreased, normal
in mild
Normal (or decreased) Increased Increased Increased Variable Normal
(decreased/intermediat
e)
ILD Decreased Decreased Normal (or decreased) Normal or
increased
Increased Increased Decreased Normal (or decreased)
PVD Decreased Normal or slightly
decreased (Normal) or
decreased
Normal Increased Increased Decreased Decreased
Neuromuscular
Other
Deconditioning Decreased Normal or slightly
decreased Decreased Normal Normal Normal Normal Normal or decreased
HV Normal Normal Normal NA NA Increased Normal Normal
Obesity Decreased for
actual (normal
for ideal weight)
Normal or slightly
decreased
Normal Normal (or
increased)
Normal Normal Normal Normal (or decreased)

Ines Frederix 16
3 Algorithm for ergospirometry analysis
3.1 What is the indication for the ergospirometry?
Before starting the interpretation of the cardiopulmonary exercise test; it is of primordial
importance to know the exact indication for the test. The main indications for
cardiopulmonary exercise testing are the following:
1. Evaluation of exercise intolerance
- Determination of functional impairment or capacity (VO2 peak)
- Determination of exercise-limiting factors and pathophysiologic mechanisms
2. Evaluation of patients with cardiovascular disease
- Functional evaluation and prognosis in patients with heart failure
- Selection for cardiac transplantation
- Exercise prescription and monitoring response to exercise training for cardiac
rehabilitation
3. Evaluation of patients with respiratory disease
4. Specific clinical applications
3.2 Assess patient’s history, clinical examination, other examinations
(RxTx, ECG, PFTs, etc.)
3.3 Was the ergospirometry maximal?
Patient effort during cardiovascular exercise testing can be considered to be maximal if one or
more of the following occur:
1. The patient achieves predicted peak VO2 and/or a plateau on the VO2 curve is
observed
2. The predicted maximal work rate is achieved
3. The achieved HR is > 85% HR max predicted (cardiovascular limitation)
4. The VE max approaches or exceeds MVV (ventilatory limitation)
5. RER achieved is > 1,1
6. Patient exhaustion/Borg scale rating of 9-10 on a 0-10 scale
3.4 Is aerobic capacity (VO2 max) normal?
Normally, the observed VO2max > 84% VO2 max predicted (Ref. 1), >100% VO2 max
predicted (Ref. 2). The distinction between (ab)normal VO2 max guides the clinician in a first
direction regarding possible underlying pathology (ies).
3.5 Does cardiovascular function contribute to exercise limitation?
The cardiopulmonary exercise test is considered cardiovascular limited in case of reduced
HRR with normal or increased VR. In healthy people, cardiopulmonary exercise test are
usually cardiovascular limited.
3.6 Does ventilatory function (respiratory mechanics) contribute to exercise
limitation?

Ines Frederix 17
The cardiopulmonary exercise test is considered ventilatory limited, in case the VE max
approaches or exceeds VMM in the presence of increased HRR.
3.7 Does pulmonary gas exchange (hypoxemia, inefficient ventilation,
increased dead space ventilation) contribute to exercise limitation?
Exercise hypoxemia most often reflects intrinsic pulmonary gas exchange limitation. A fall in
SaO2 (∆SaO2) of ≥ 4%, SaO2 ≤ 88%, or PaO2 ≤ 55 mmHg during cardiopulmonary exercise
testing is usually considered clinically significant.
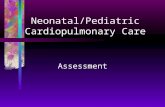
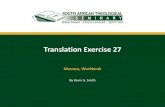
3.8 Integrate all results in final conclusion(s)
The observed ergospirometric patterns can help guide the clinician in his
diagnostic/therapeutic thinking. However, frequently different pathophysiologic mechanisms
contribute concomitantly to the patient’s symptoms/exercise intolerance. Therefore, an
integrative approach considering all ergospirometric parameters and also the patient’s history,
clinical examination and static examinations is highly encouraged.
Figure 1: depicts the basic strategy for the interpretation of peak cardiopulmonary exercise
test results.

Ines Frederix 18

Ines Frederix 19
4 Reference values Table 4: depicts the formula and reference values for the most important cardiovascular,
ventilatory and metabolic parameters; given a maximal cardiopulmonary exercise test (as
defined in section 3.3).
Parameter Formula (max ErgoSx) Reference values
Cardiovascular
Heart rate HR max= 220 -age > 85% age predicted
HRR HRR= HR pred - HR max < 15 beats/min
VO2 max VO2 max= Qc x c(a-v)max > 84% (Ref. 1), > 100% (Ref. 2) predicted
πO2 πO2= SV x C(a-v)O2 > 80%
∆VO2/∆W / Normal average slope is 10
Ventilatory
VE VE= VT x fB /
fB fB= VE/VT < 60 breaths/min
VD/VT /
< 0,28 for age < 40 years; < 0,30 for age >
40 years
VE/VCO2 slope ∆VE/∆VCO2 23-25 (Ref 1.), < 30 (Ref. 2)
VE/VCO2 (at
AT1) / < 34
∆SaO2 / < 4% (Ref. 1), < 5% (Ref. 2)
Minimal SaO2 / Should be ≥ 95% throughout exercise
VR VR= VEmax/VMM 72 ± 15% (Ref. 1), ≤ 80% (Ref. 2)
Metabolic
RER RER= VCO2/VO2 > 1,1
AT1 /
40-80% VO2 max predicted (Ref. 1); 40-
60% VO2 max predicted (Ref. 2)
AT2 (RCP) / 60-90 % VO2 max predicted (Ref. 2)

Ines Frederix 20
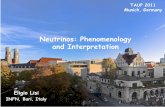
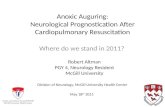
5 Graphic representation of cardiopulmonary exercise response
in healthy person
Figure 2: depicts a graphic representation of the maximal, incremental cardiopulmonary
exercise response of a healthy aged person.

Ines Frederix 21
6 References ATS/ACCP Statement on Cardiopulmonary Exercise Testing. Am J Respir Crit Care Med
2003; 167: 211-277.
Milani R, Lavie C, Mehra M, et al. Understanding the Basics of Cardiopulmonary Exercise
Testing. Mayo Clin Proc. 2006; 81: 1603-1611.
Mezzani A, Agostoni P, Cogen-Solal A, et al. Standards for the use of cardiopulmonary
exercise testing for the functional evaluation of cardiac patients: a report from the Exercise
Physiology Section of the European Association for Cardiovascular Prevention and
Rehabilitation. Eur J cardiovasc prev rehabil 2009; 16: 249-267.
Guazzi M, Adams V, Conraads V, et al. Clinical recommendations for cardiopulmonary
exercise testing data assessment in specific patient populations. Eur Heart J 2012; 1-22.
Dubowy K, Baden W, Bernitzki S, et al. A practical and transferable new protocol for
treadmill testing of children and adults. Cardiol Young 2008; 18: 615-623.
Gläser S, Friedrich N, Koch B, et al. Exercise Blood Pressure and Heart Rate Reference
Values. Heart, Lung and Circulation 2013; 22: 661-667.
Paap D, Takken T. Reference values for cardiopulmonary exercise testing in heathy adults: a
systematic review. Expert Rev. Cardiovasc. Ther. 2014; 12: 1439-1453.
Koch B, Schäper C, Itterman T, et al. Reference values for cardiopulmonary exercise testing
in healthy volunteers: the SHIP study. Eur Respir J 2009; 33: 389-397.
Cohen-Solal A, Carré F. Practical Guide to Cardiopulmonary Exercise Testing. Elsevier
Masson pp. 1-168.