Ventricular Structure and Function -...
13
1 D iastolic dysfunction plays a role in heart failure with pre- served ejection fraction. 1–3 Traditionally, diastolic func- tion (DF) has been evaluated invasively by measuring left ventricular (LV) end-diastolic or diastatic pressure–volume relations and/or τ, the time constant of isovolumic relaxation. During early rapid filling, determinants of LV pressure include relaxation and passive chamber properties. 4–6 In early diastole, relaxation usually dominates (passive) stiffness effects and their modification strongly influences DF. 5,6 See Clinical Perspective However, invasive methods can be complemented by echocardiography to characterize additional aspects of fill- ing. 7 Doppler echocardiography has become the standard and preferred noninvasive clinical quantitative DF assess- ment method. Selected aspects of LV filling dynamics can be assessed from features of the Doppler transmitral (E- and A-wave) and mitral annular (E′-wave) velocity waveforms approximated as triangles. The 3 major abnormal transmitral flow patterns, associated with dysfunction are impaired relax- ation, pseudonormal, and restrictive. 8 The inflow patterns and related cardiac fluid dynamic mechanisms, including the dynamics of atrioventricular valve plane motion, DF altera- tions accompanying chamber enlargement, and failure, have been previously investigated. 4 The pressure gradient between left atrium and LV deter- mines E-waves directly, whereas E′ reflects longitudinal chamber volume accommodation. The peak early rapid filling to peak late filling (E/A) and peak E to peak mitral annulus velocity (E/E′) ratios are common DF correlates. In normal filling, E/A>1 and peak E′ is >10 cm/s (or E/E′<8). 9 Mathematical models have been effective in promoting an understanding of DF and alteration of chamber proper- ties in selected cardiovascular diseases. 4,5,10 One such model is the parametrized diastolic filling (PDF) formalism that can assess DF quantitatively by subjecting E-waves to model- based analysis. 11 The PDF formalism models the kinematics of suction-initiated filling in analogy to the recoil from rest, Background—Pseudonormal Doppler E-wave filling patterns indicate diastolic dysfunction but are indistinguishable from the normal filling pattern. For accurate classification, maneuvers to alter load or to additionally measure peak E′ are required. E-wave deceleration time (DT) has been fractionated into its stiffness (DT s ) and relaxation (DT r ) components (DT=DT s +DT r ) by analyzing E-waves via the parametrized diastolic filling formalism. The method has been validated with DT s and DT r correlating with simultaneous catheterization-derived stiffness (dP/dV) and relaxation (τ) with r=0.82 and r=0.94, respectively. We hypothesize that DT fractionation can (1) distinguish between unblinded (E′ known) normal versus pseudonormal age-matched groups with normal left ventricular ejection fraction, and (2) distinguish between blinded (E′ unknown) normal versus pseudonormal groups, based solely on E-wave analysis. Methods and Results—Data (763 E-waves) from 15 age-matched, pseudonormal (elevated E/E′) and 15 normal subjects were analyzed. Conventional echocardiographic and parametrized diastolic filling stiffness (k) and relaxation (c) parameters and DT s and DT r were compared. Conventional diastolic function parameters did not differentiate between unblinded groups, whereas k, c (P<0.001) and DT s , DT r (P<0.001) did. Independent, blinded (E′ not provided) analysis of 42 subjects (30 subjects from unblinded training set and 12 additional subjects from validation set, 581 E-waves) showed that R (=DT r /DT) had high sensitivity (0.90) and specificity (0.86) in differentiating pseudonormal from normal once E′ revealed actual classification. Conclusions—Parametrized diastolic filling–based E-wave analysis (k, c or DT s and DT r ) can differentiate normal versus pseudonormal filling patterns without requiring knowledge of E′. (Circ Cardiovasc Imaging. 2015;8:e002177. DOI: 10.1161/CIRCIMAGING.114.002177.) Key Words: diastole ◼ Doppler echocardiography ◼ left ventricle ◼ relaxation ◼ stiffness © 2015 American Heart Association, Inc. Circ Cardiovasc Imaging is available at http://circimaging.ahajournals.org DOI: 10.1161/CIRCIMAGING.114.002177 Received May 9, 2014; accepted November 10, 2014. From the Cardiovascular Biophysics Laboratory, Cardiovascular Division (S.M., S.Z., S.J.K), Department of Physics (S.M., S.Z., S.J.K.), and Department of Medicine, Cardiovascular Division (S.J.K), Washington University School of Medicine, St. Louis, MO. The Data Supplement is available with this article at http://circimaging.ahajournals.org/lookup/suppl/doi:10.1161/CIRCIMAGING.114.002177/-/DCI. Correspondence to Sándor J. Kovács, PhD, MD, Cardiovascular Biophysics Laboratory, Washington University Medical Center, 660 South Euclid Ave, Box 8086, St Louis, MO 63110. E-mail [email protected] Fractionating E-Wave Deceleration Time Into Its Stiffness and Relaxation Components Distinguishes Pseudonormal From Normal Filling Sina Mossahebi, PhD; Simeng Zhu, BA; Sándor J. Kovács, PhD, MD Ventricular Structure and Function by guest on May 2, 2018 http://circimaging.ahajournals.org/ Downloaded from by guest on May 2, 2018 http://circimaging.ahajournals.org/ Downloaded from by guest on May 2, 2018 http://circimaging.ahajournals.org/ Downloaded from by guest on May 2, 2018 http://circimaging.ahajournals.org/ Downloaded from by guest on May 2, 2018 http://circimaging.ahajournals.org/ Downloaded from by guest on May 2, 2018 http://circimaging.ahajournals.org/ Downloaded from
-
Upload
doannguyet -
Category
Documents
-
view
217 -
download
0
Transcript of Ventricular Structure and Function -...

1
Diastolic dysfunction plays a role in heart failure with pre-served ejection fraction.1–3 Traditionally, diastolic func-
tion (DF) has been evaluated invasively by measuring left ventricular (LV) end-diastolic or diastatic pressure–volume relations and/or τ, the time constant of isovolumic relaxation. During early rapid filling, determinants of LV pressure include relaxation and passive chamber properties.4–6 In early diastole, relaxation usually dominates (passive) stiffness effects and their modification strongly influences DF.5,6
See Clinical Perspective
However, invasive methods can be complemented by echocardiography to characterize additional aspects of fill-ing.7 Doppler echocardiography has become the standard and preferred noninvasive clinical quantitative DF assess-ment method. Selected aspects of LV filling dynamics can be assessed from features of the Doppler transmitral (E- and A-wave) and mitral annular (E′-wave) velocity waveforms approximated as triangles. The 3 major abnormal transmitral
flow patterns, associated with dysfunction are impaired relax-ation, pseudonormal, and restrictive.8 The inflow patterns and related cardiac fluid dynamic mechanisms, including the dynamics of atrioventricular valve plane motion, DF altera-tions accompanying chamber enlargement, and failure, have been previously investigated.4
The pressure gradient between left atrium and LV deter-mines E-waves directly, whereas E′ reflects longitudinal chamber volume accommodation. The peak early rapid filling to peak late filling (E/A) and peak E to peak mitral annulus velocity (E/E′) ratios are common DF correlates. In normal filling, E/A>1 and peak E′ is >10 cm/s (or E/E′<8).9
Mathematical models have been effective in promoting an understanding of DF and alteration of chamber proper-ties in selected cardiovascular diseases.4,5,10 One such model is the parametrized diastolic filling (PDF) formalism that can assess DF quantitatively by subjecting E-waves to model-based analysis.11 The PDF formalism models the kinematics of suction-initiated filling in analogy to the recoil from rest,
Background—Pseudonormal Doppler E-wave filling patterns indicate diastolic dysfunction but are indistinguishable from the normal filling pattern. For accurate classification, maneuvers to alter load or to additionally measure peak E′ are required. E-wave deceleration time (DT) has been fractionated into its stiffness (DT
s) and relaxation (DT
r) components
(DT=DTs+DT
r) by analyzing E-waves via the parametrized diastolic filling formalism. The method has been validated
with DTs and DT
r correlating with simultaneous catheterization-derived stiffness (dP/dV) and relaxation (τ) with r=0.82
and r=0.94, respectively. We hypothesize that DT fractionation can (1) distinguish between unblinded (E′ known) normal versus pseudonormal age-matched groups with normal left ventricular ejection fraction, and (2) distinguish between blinded (E′ unknown) normal versus pseudonormal groups, based solely on E-wave analysis.
Methods and Results—Data (763 E-waves) from 15 age-matched, pseudonormal (elevated E/E′) and 15 normal subjects were analyzed. Conventional echocardiographic and parametrized diastolic filling stiffness (k) and relaxation (c) parameters and DT
s and DT
r were compared. Conventional diastolic function parameters did not differentiate between
unblinded groups, whereas k, c (P<0.001) and DTs, DT
r (P<0.001) did. Independent, blinded (E′ not provided) analysis
of 42 subjects (30 subjects from unblinded training set and 12 additional subjects from validation set, 581 E-waves) showed that R (=DT
r/DT) had high sensitivity (0.90) and specificity (0.86) in differentiating pseudonormal from normal
once E′ revealed actual classification.Conclusions—Parametrized diastolic filling–based E-wave analysis (k, c or DT
s and DT
r) can differentiate normal versus
pseudonormal filling patterns without requiring knowledge of E′. (Circ Cardiovasc Imaging. 2015;8:e002177. DOI: 10.1161/CIRCIMAGING.114.002177.)
Key Words: diastole ◼ Doppler echocardiography ◼ left ventricle ◼ relaxation ◼ stiffness
© 2015 American Heart Association, Inc.
Circ Cardiovasc Imaging is available at http://circimaging.ahajournals.org DOI: 10.1161/CIRCIMAGING.114.002177
Received May 9, 2014; accepted November 10, 2014.From the Cardiovascular Biophysics Laboratory, Cardiovascular Division (S.M., S.Z., S.J.K), Department of Physics (S.M., S.Z., S.J.K.), and Department
of Medicine, Cardiovascular Division (S.J.K), Washington University School of Medicine, St. Louis, MO.The Data Supplement is available with this article at http://circimaging.ahajournals.org/lookup/suppl/doi:10.1161/CIRCIMAGING.114.002177/-/DCI.Correspondence to Sándor J. Kovács, PhD, MD, Cardiovascular Biophysics Laboratory, Washington University Medical Center, 660 South Euclid Ave,
Box 8086, St Louis, MO 63110. E-mail [email protected]
Fractionating E-Wave Deceleration Time Into Its Stiffness and Relaxation Components Distinguishes Pseudonormal
From Normal FillingSina Mossahebi, PhD; Simeng Zhu, BA; Sándor J. Kovács, PhD, MD
Ventricular Structure and Function
by guest on May 2, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from
by guest on May 2, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from
by guest on May 2, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from
by guest on May 2, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from
by guest on May 2, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from
by guest on May 2, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from

2 Mossahebi et al E-waves Distinguish Pseudonormal vs. Normal Filling
of an equivalent damped oscillator. Model-predicted fit to the clinical E-wave is excellent, and the fitting process yields 3 unique parameters for each analyzed E-wave: k is the stiff-ness constant; c is the viscoelasticity/relaxation constant; and x
0 is the load. Using a clinical E-wave contour as input and
suitable mathematical methods, unique k, c, and x0 param-
eters are generated as output for each E-wave.12 The PDF parameters also generate indexes with rigorous physiological analogues, such as the peak instantaneous pressure gradient (kx
0) and the potential energy driving the recoil/suction pro-
cess (1/2kx0
2).13,14 The details and the required tools to carry out PDF-based analysis of E-waves for DF quantification are available at Journal of Visualized Experiments.15
Prior work by Little et al16 predicted that Doppler E-wave DT is determined by stiffness alone. E-wave analysis via PDF revealed that DT is actually jointly determined by stiff-ness (PDF parameter k) and relaxation (PDF parameter c).17 Using PDF-based analysis, we have predicted and validated that E-wave DT can be decomposed into its stiffness (DT
s)
and relaxation (DTr) components such that DT=DT
s+DT
r.18,19
The predicted causal relationship between DTs and DT
r and
stiffness (ΔP/ΔV) and relaxation (τ) was validated using simultaneous, high fidelity hemodynamic and echocardio-graphic data, by the high, observed correlation (r=0.82 and r=0.94, respectively).18,19
The effect of delayed relaxation (lengthens E-wave) can be masked by increased stiffness (shortens E-wave) by generating increased atrial pressure and thereby increas-ing E-wave amplitude.5,6 In pseudonormal filling, LV and left atrial pressures are increased, and relaxation is slower.7 Although inscribed at a higher absolute pressure, the early diastolic pressure gradient is similar to normal filling, result-ing in indistinguishable E-wave shapes and E/A ratios. With progressive impairment of relaxation, the E′ peak is reduced and delayed.20 Thus, pseudonormal can be distinguished from normal by a reduced and delayed E′ and increase in the E/E′ ratio or by respiratory maneuvers (straining) that transiently alter load.7,9
In this work, we test 2 hypotheses: (1) that PDF-based E-wave analysis suffices to differentiate pseudonormal from normal filling in unblinded groups, that is, where E′ is known in advance, and (2) that PDF analysis can differentiate pseudonormal from normal filling in blinded groups, when E′ is not known in advance. We fractionate DT into its stiffness and relaxation components and determine whether they can distinguish between normal and pseudonormal filling patterns in unblinded and blinded age-matched groups having normal E-wave patterns and indistinguishable E
peak, DT, and E
dur.
Methods
Subject Selection
Unblinded Analysis GroupThirty data sets (mean age 59, 16 men) were selected from the Cardio-vascular Biophysics Laboratory database.21 All participants provided informed consent before the procedure using a protocol approved by the Washington University Human Research Protection Office.
Fifteen normal filling pattern data sets were selected so that they were age-matched with the 15 pseudonormal filling data sets ac-cording to American Society of Echocardiography9 criteria. In both
groups, 0.8<E/A<1.5 and 160<DT<200 ms. Selection criteria for the normal group were no active ischemia, normal valvular function, nor-mal LV ejection fraction (≥50%), no history of myocardial infarction or peripheral vascular disease or bundle branch block, and clear dia-static intervals after E-waves. Among the 15 normal filling data sets, 12 had normal end-diastolic pressure (LVEDP<14 mm Hg) and 3 had 14<LVEDP<16 mm Hg. These 3 subjects were included in normal group because they had normal relaxation (τ<50 ms). The distribu-tions of LVEDPs in the 15 pseudonormal filling data sets were 6 with 15<LVEDP<20 mm Hg and 9 with LVEDP>21 mm Hg. Selection cri-teria for the pseudonormal group9,22,23 were indistinguishable E-wave peak, DT, and E-wave duration compared with the normal group, nor-mal LV function (ejection fraction >50%) with impaired annular peak velocity (lateral E′<10) and prolonged τ (>50 ms). The pseudonormal data sets were age-matched with the normal group because DF de-pends on age.24 Because E-waves vary in response to respiration and load,25 ≥10 to 15 cardiac cycles per subject are analyzed, assuring that the physiology is accurately reflected, accordingly a total of 763 cardiac cycles from 30 subjects were analyzed. Age matching was achieved by selecting the pseudonormal group and using frequency age-matching by 5-year intervals to select normal subjects. The nor-mal data sets were also selected so that none were older (or younger) than the oldest (or the youngest) in pseudonormal group. The clinical descriptors of the 30 subjects and their hemodynamic and echocar-diographic indices are shown in Tables 1 and 2.
Blinded Analysis GroupThe 30 data sets from the unblinded training set were combined with 12 additional data sets as a validation set (42 total) meeting inclu-sionary criteria from the Cardiovascular Biophysics Laboratory da-tabase21 and subjected to a de novo blinded analysis by a member (S. Zhu) of our research group. In this blinded study, 42 data sets consist-ing only of E-waves were provided for analysis to the independent collaborator (S. Zhu). The clinical descriptors of the blinded group are shown in Table 3.
Data AcquisitionThe database is a repository of high fidelity, simultaneous echocar-diographic transmitral flow and pressure–volume data using standard recording methods that have been previously detailed.11,13,14,20,21,26 Briefly, immediately before arterial access, a complete 2D echo-Doppler study is performed with subjects in supine position using a Philips (Andover, MA) iE33 system according to American Society of Echocardiography criteria.9,27
Doppler E-Wave AnalysisFor each subject, ≥1 to 2 minutes of simultaneous hemodynamic and continuous transmitral flow data were recorded in the pulsed-wave Doppler mode. In accordance with convention, the apical 4-chamber
Table 1. Clinical Descriptors of Normal and Pseudonormal Groups in Unblinded* Analysis
Clinical Descriptors
Normal Filling Group
Pseudonormal Filling Group Significance
N 15 15 NA
Age, y 59±8 59±9 0.87
sex (M/F) 8/7 8/7 NA
Heart rate, bpm 68±7 66±7 0.47
LVEF, % 71±8 71±8 0.81
Height, cm 170±11 165±8 0.16
Weight, kg 88±16 86±15 0.78
Data are presented as mean±standard deviation.LVEF indicates left ventricular ejection fraction (via calibrated ventricu
lography); and NA, not applicable.*Unblinded is defined as E′ and τ are known to the person doing the analysis.
by guest on May 2, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from

3 Mossahebi et al E-waves Distinguish Pseudonormal vs. Normal Filling
view was used for Doppler E-wave recording with the sample volume located at the leaflet tips.
Doppler transmitral flow velocity contours and mitral annular E′-waves were analyzed using the conventional, triangle-shape ap-proximation,28,29 yielding peak E-wave velocity (E), acceleration time (AT), DT, velocity-time integral, peak A-wave velocity (A), E/A ratio, peak E′-wave velocity (E′), and E/E′ ratio.
Each E-wave was also analyzed via the PDF formalism (see Appendix 1 in the Data Supplement) to yield mathematically unique PDF parameters (x
0, c, k) for each E-wave.15,20,30,31 Stiffness (DT
s) and
relaxation (DTr) components of DT were computed via the previ-
ously validated fractionation method18 (see Appendix 2 in the Data Supplement) such that DT=DT
s+DT
r (Figure 1), where total DT was
determined using the conventional method. Alternatively, DT can be determined via the PDF method solely as detailed in Ref. [18]. The conclusions are unaffected by the method of DT determination. By normalizing DT and rewriting DT=DT
s+DT
r as 1=S+R, where
S=DTs/DT and R=DT
r/DT, S and R provide the fractional compo-
nents of total DT. Sensitivity and specificity were determined using the logistic regression model (receiver operator characteristic analy-sis) to compare the diagnostic performance of parameter R (or S) over a range of thresholds by classifying normal and pseudonormal groups, where normal and pseudonormal groups were defined and categorized based on E/E′ and τ values. Using the logistic regression model, the cut point was selected from the data shown in Table 4 from the N=30 unblinded analysis (E/E′ and τ known to classify normal versus pseudonormal) as that value of R that maximized both sensitivity and specificity (where the sensitivity and specificity curves versus all possible cutpoints cross) with the highest likeli-hood ratio.32
Blinded AnalysisA total of 581 cardiac cycles from the 42 data sets were analyzed by one author (S. Zhu) blinded to E′ and τ. PDF parameters, stiffness, and relaxation components of DT (DT
s and DT
r) and the fraction of
DT as a result of stiffness and relaxation (S and R) were computed for each E-wave. Based on the selected cut point for R (or S) from the N=30 unblinded study, sensitivity and specificity in 12 additional subjects as a validation set was performed. In addition, all 42 subjects (30 from training set and 12 from validation set) were independently analyzed in a blinded fashion (E′ and τ not known to S. Zhu) to deter-mine interobserver variation in determining R and ability to classify normal versus pseudonormal filling.
Statistical AnalysisContinuous variables (hemodynamic indexes, echocardiographic, and PDF parameters) were presented as mean and SDs from an av-erage of 25 cycles per subject in the unblinded study and 14 car-diac cycles per subject in the blinded study. Comparisons between normal and pseudonormal were performed using t test. P values of <0.05 were considered significant. Logistic regression analysis used a univariate model using the parameter R (=DT
r/DT) to determine
how well it differentiated pseudonormal from normal (defined by τ and E/E′). All statistical analyses and comparisons were performed using Microsoft Excel 2010 Version 14.0.7128.5000 (Microsoft Corporation, Redmond WA) and GraphPad Prism/StatMate 2009 ver-sion 5.03 (Graphpad Software Inc., La Jolla CA).
Results
Hemodynamics in Normal and PseudonormalAs expected, LVEDP and τ were significantly higher in pseudonormal than that in normal filling group (LVEDP: 20±4 mm Hg versus 13±2 mm Hg, P<0.001; τ: 65±5 ms ver-sus 46±2 mm Hg, P<0.001). The LV end-systolic volume and LVEDV are similar in both groups (LV end-systolic volume: 36±12 mL for pseudonormal versus 39±17 mL for normal, P=0.63 and LVEDV: 128±38 mL for pseudonormal versus 134±43 mL for normal, P=0.66).
Table 2. Hemodynamic and Echocardiographic Data in Normal Filling and Pseudonormal Filling Groups
Normal Filling
Pseudonormal Filling Significance
Hemodynamic Parameters
LVEDP, mm Hg 13±2 20±3 <0.001
LVESV, mL 39±17 36±12 0.63
LVEDV, mL 134±43 128±38 0.66
τ, ms 46±2 65±5 <0.001
Echocardiographic Parameters
Peak Ewave velocity (E), cm/s 82±6 83±13 0.62
Ewave deceleration time (DT), ms 180±16 185±13 0.31
Ewave duration time (Edur
), ms 262±17 258±23 0.60
EVTI, cm 10.5±1.9 11.1±1.9 0.35
Peak Awave velocity (A), cm/s 72±9 73±15 0.82
E/A (dimensionless) 1.2±0.1 1.2±0.4 0.49
Peak E′wave velocity (E′), cm/s 15±3 8±1 <0.001
E/E′ (dimensionless) 5.1±0.9 10.9±1.4 <0.001
k, 1/s2 212±17 263±28 <0.001
c, 1/s 15.7±1.6 23.9±6.0 <0.001
DTr, ms 44±12 64±14 <0.001
DTs, ms 136±8 121±11 <0.001
R=DTr/DT, % 24±5 34±6 <0.001
S=DTs/DT, % 76±5 66±6 <0.001
Data are presented as mean±standard deviation.c indicates PDF relaxation parameter; DT
r, relaxation component of DT; DT
s,
stiffness component of DT E/A, ratio of peak Ewave and peak Awave; E/E′, ratio of peak Ewave and peak E′wave; EVTI, Ewave velocitytime integral; k, PDF stiffness parameter; LVEDP, left ventricular enddiastolic pressure; LVEDV, left ventricular enddiastolic volume; LVESV, left ventricular endsystolic volume; and τ, time constant of isovolumic relaxation.
Table 3. Clinical Descriptors of Normal Filling and Pseudonormal Filling Groups in Blinded* Analysis
Clinical Descriptors
Normal Filling Group
Pseudonormal Filling Group Significance
N 21 21 N.A.
Age, y 59±8 59±10 0.84
Sex (M/F) 11/10 13/8 0.53
Heart rate, bpm 67±7 66±7 0.77
LVEF, % 73±8 71±8 0.52
Height, cm 171±10 165±9 0.10
Weight, kg 85±18 87±15 0.67
Data are presented as mean±standard deviation.LVEF indicates left ventricular ejection fraction (via calibrated ventricu
lography); and NA, not applicable.*Blinded is defined as normal or pseudonormal status is unknown to the
person doing the analysis (E′ and τ unknown).
by guest on May 2, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from

4 Mossahebi et al E-waves Distinguish Pseudonormal vs. Normal Filling
Conventional E-Wave, A-Wave, and E′-Wave Features in Normal and PseudonormalPeak E-wave velocity (E), E-wave DT, E-wave duration (E
dur), and E-wave velocity-time integral do not significantly
differ between normal and pseudonormal filling groups (E: 82±6 cm/s versus 83±13 cm/s, P=0.62; DT: 180±16 ms versus 185±13 ms, P=0.31; E
dur: 262±17 ms versus 258±23
ms, P=0.60; E-wave velocity-time integral: 10.5±1.9 cm ver-sus 11.1±1.9 cm, P=0.35).
Peak A-wave velocity (A) and E/A ratio do not significantly differ between groups (A: 72±9 cm/s versus 73±15 cm/s, P=0.82; E/A: 1.2±0.1 versus 1.2±0.4, P=0.49). As expected, peak E′-wave velocity (E′) is significantly lower in pseudo-normal than normal filling (E′: 8±1 cm/s versus 15±3 cm/s, P<0.001). E/E′ is higher in pseudonormal than in normal fill-ing (E/E′: 10.9±1.4 versus 5.1±0.9, P<0.001).
PDF Parameters in Normal and PseudonormalPDF analysis reveals that PDF stiffness parameter (k) and PDF relaxation parameter analysis reveals that PDF stiff-ness parameter (c) in pseudonormal group are higher (worse) than normal group (k: 263±28 1/s2 versus 212±17 1/s2, P<0.001; c: 23.9±6.0 1/s versus 15.7±1.6 1/s, P<0.001).
Fractionation of Deceleration Time into Stiffness and Relaxation Components in Normal and PseudonormalRelaxation component of DT (DT
r) in pseudonormal group is
longer than normal group (DTr-pseudonormal
=64±14 ms versus DTr-
normal=44±12 ms, P<0.001). The longer DT
r in pseudonormal and
the direct correlation between DTr and the time constant of iso-
volumic relaxation (τ) and isovolumic relaxation time show that relaxation is impaired in pseudonormal compared with normal filling. Stiffness component of DT (DT
s) in pseudonormal group
(inversely related to chamber stiffness) is shorter (stiffer) than normal group (DT
s-pseudonormal=121±11 ms versus DT
s-normal=136±8
ms, P<0.001). The shorter DTs in pseudonormal quantifies the
extent to which pseudonormal chambers are stiffer than normal. For the 15 normal data sets, S=0.76 and R=0.24; hence, 76% of total DT is caused by stiffness and 24% is caused by relaxation. For the 15 pseudonormal data sets, S=0.66 and R=0.34; hence, 66% of DT is caused by stiffness and 34% is caused by relax-ation. These differences are significant (P<0.001).
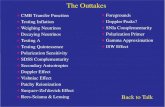
Figure 2 shows receiver operator characteristic curve for R (=DT
r/DT) in the unblinded study of 30 subjects. Receiver
operator characteristic analysis demonstrates that R (R=0.28 as a cutpoint) can differentiate pseudonormal versus normal subjects with high sensitivity (0.93) and specificity (0.93). The area under receiver operator characteristic curve (area under curve) is 0.98. The raw data showing R values of the 30 subjects used for plotting Figure 2 is given in Table 4.
Repeat determination of R using the entire data set (N=42) via unblinded analysis comprising N=21 normal and N=21 pseudonormal yielded R=0.28, independently reaffirming it as the cutpoint.
Blinded AnalysisR=0.28 (from the N=30 unblinded study) applied to the vali-dation set (12 subjects) in a blinded fashion predicted 5 of 6
Table 4. The Relaxation Fraction R for All Subjects in the Unblinded Study
SubjectR=DT
r/DT
(Normal)R=DT
r/DT
(Pseudonormal)
1 0.270 0.324
2 0.276 0.289
3 0.286 0.365
4 0.272 0.310
5 0.220 0.348
6 0.225 0.321
7 0.249 0.298
8 0.212 0.293
9 0.192 0.471
10 0.173 0.274
11 0.257 0.285
12 0.158 0.449
13 0.276 0.400
14 0.212 0.356
15 0.240 0.363
Individual R=DTr/DT values for 30 subjects of normal and pseudonormal
groups in unblinded study used to plot the ROC curve in Figure 2.DT indicates Ewave deceleration time; and DT
r, relaxation component of DT.
1.5
2.0
2.5
Time (s)
1.0
0.5
A B C D
AT DT
Mitr
al fl
ow v
eloc
ity (m
/s)
0.2 0.40 0.6 0.2 0.40 0.6
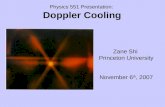
Figure 1. Overview of DTs and DTr computation. A, Typical Doppler velocity profile. B, Acceleration time (AT), DT, Edur determination using triangle approx-imation to E-wave contour. C, Parametrized diastolic filling (PDF) model fit to E-wave (green) provides PDF parameters c=22.7/s, k=217/s2, x0=14.8 cm. D, DTr is determined by setting c=0, thereby generating an ideal, model predicted E-wave (red curve), with same x0, k as original E-wave (green curve). DTr is defined as the time difference between duration of the actual E-wave (green curve) using triangle method and the ideal (c=0) E-wave (red curve). DTs is then determined by subtracting DTr from total DT (DTs=DT−DTr). DT=202 ms, DTr=77 ms, and DTs=125 ms. c indicates PDF chamber relaxation parameter; DT, E-wave deceleration time; DTr, relaxation component of E-wave deceleration time; DTs, stiffness component of E-wave deceleration time; Edur, E-wave duration; k, PDF chamber stiffness parameter; and xo, PDF load parameter. See text for details.
by guest on May 2, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from

5 Mossahebi et al E-waves Distinguish Pseudonormal vs. Normal Filling
normal subjects correctly and 5 of 6 pseudonormal subjects correctly demonstrating the ability of R (DT
r/DT) to differen-
tiate pseudonormal versus normal with high sensitivity (0.83) and specificity (0.83). The repeated interobserver variability study performed in a blinded fashion by S. Zhu of all 42 data sets demonstrated that R was observer independent and it dif-ferentiated pseudonormal versus normal filling subjects with high sensitivity (0.90) and specificity (0.86).
DiscussionDiastolic Function EvaluationEchocardiography is the primary and preferred noninva-sive method of DF evaluation. E-wave amplitude and shape reflects global volume accommodation, whereas E′ reflects the longitudinal component of volume accommodation. E′ is known to be impaired in dysfunction, and E/E′ is known to correlate with filling pressures, that is, pulmonary capillary wedge based on established physiological mechanisms.9,33,34
Pseudonormal FillingBoth impaired relaxation and restrictive patterns (grade 1 and 3 diastolic dysfunction) can be distinguished from normal using mitral inflow pattern features (E/A ratio). Maintenance of similar atrioventricular pressure gradient in pseudonor-mal and normal setting generates E-waves that are indistin-guishable using conventional metrics, such as E
peak, E
dur, DT,
velocity-time integral, and E/A (as shown in Figure 3). Thus, distinguishing pseudonormal filling (grade 2 of diastolic dys-function) from normal filling requires additional informa-tion, such as E′ or response to respiratory (strain) maneuvers. Pseudonormal can be distinguished from normal filling by reduced E′ and increased E/E′. Cardiac catheterization indi-cates that in the pseudonormal filling pattern, both LV and left atrium pressures are increased and are associated with stiffer chambers compared with normal. E/E′>15 indicates elevated pulmonary capillary wedge pressure, whereas E/E′<8 is asso-ciated with normal left atrium pressures.35
PDF Analysis of E-Waves, Diastolic Function, and DT FractionationThe PDF method has previously shown that the cham-ber relaxation parameter c was significantly higher in hypertensive compared with nonhypertensive controls.25 Furthermore, the PDF relaxation parameter c differenti-ated between diabetic versus control subjects, whereas conventional indexes, such as DT, E
peak, and τ, failed
to do so.36 The peak atrioventricular pressure gradient, obtained from the PDF parameters as kx
0,13 was signifi-
cantly higher in the diabetic group. The PDF formalism has also characterized mitral annular oscillations after the E′-wave and showed that the absence of mitral annular oscillations indicates relaxation-related diastolic dysfunc-tion.37 The physiological role of E′ as a longitudinal vol-ume accommodation index has been elucidated in terms of impedance.33
An additional PDF-based mechanistic advance in under-standing DF includes the insight that during diastasis, the ventricle is in (transient) static equilibrium, such that atrial and ventricular pressures are equal (forces are balanced, but not zero) and transmitral flow is absent, although residual vortices may be present.5,38 Accordingly, the pas-sive, in vivo equilibrium volume of the (fully relaxed) LV is its volume at diastasis.39 Beat-to-beat variation in dia-static volume and pressure generates a locus of P, V points whose slope via linear regression defines in vivo pas-sive chamber stiffness,39 easily determined directly from E-wave analysis.40
Although pioneering work indicated that DT and stiff-ness16 are inversely related, subsequent PDF analysis has refined that view by showing that E-wave DT is deter-mined jointly by stiffness and relaxation (k and c PDF
Figure 2. Receiver operator characteristic curve for the percent-age of normalized DT as a result of relaxation (R=DTr/DT) in unblinded study demonstrates the ability of parameter R (R=0.28 as a cutpoint) in differentiating pseudonormal vs normal subjects with high sensitivity (0.93) and specificity (0.93), yielding an area under curve (AUC) of 0.98. DT indicates E-wave deceleration time; and DTr, relaxation component of DT. See text for details.
Subject 2
500 msec
Subject 1
500 msec
1 m/s
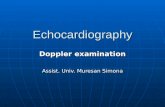
Figure 3. E-waves of 2 selected subjects (normal pattern, pseudonormal pattern) with indistinguishable E-wave duration, Epeak, E/A ratio but significantly different values for PDF parame-ters (k and c) and stiffness and relaxation components of DT (DTs and DTr). Normal: Edur=261 ms, Epeak=0.95 m/s, E/A=1.3. c=17 1/s, k=202 1/s2. DTs=137 ms, DTr=40 ms. Pseudonormal: Edur=258 ms, Epeak=0.93 m/s, E/A=1.1. c=25 1/s, k=295 1/s. DTs=107 ms, DTr=76 ms. c indicates PDF chamber relaxation parameter; DTr, relaxation component of E-wave deceleration time; DTs, stiffness component of E-wave deceleration time; Edur, E-wave duration; Epeak, peak E-wave velocity; and k, PDF chamber stiffness param-eter. See text for details.
by guest on May 2, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from

6 Mossahebi et al E-waves Distinguish Pseudonormal vs. Normal Filling
parameters) rather than stiffness alone.17 Because indistin-guishable E-waves having the same DT have been shown to have different chamber stiffness (dP/dV) and relaxation (τ) on simultaneous hemodynamic recording, it follows that E-wave DT may not provide an accurate determination of LV chamber stiffness if LV relaxation remains unknown. Based on these principles, we have previously derived and validated a method by which E-wave DT can be fractionated into stiffness (DT
s) and relaxation (DT
r) components18,19
such that DT=DTs+DT
r.
Using PDF analysis and the DT fractionation method, we have recently shown19 that atrial fibrillation chambers have increased diastatic passive chamber stiffness compared with normal sinus rhythm chambers at diastasis. Additionally, compared with normal sinus rhythm, a larger percentage of DT is because of stiffness than of relaxation in atrial fibrillation.
In the current study, we analyzed E-waves via the PDF formalism and fractionated them into their stiffness and relaxation components in age-matched normal and pseudo-normal groups. Figure 3 illustrates normal and pseudonormal E-waves, showing their indistinguishability using conven-tional metrics (E
peak, E
dur, and E/A), whereas generating sig-
nificantly different PDF parameters (k and c) and stiffness and relaxation components of DT (DT
s and DT
r). The higher
PDF stiffness parameter k and shorter DTs (inversely related
to stiffness) in the pseudonormal group compared with nor-mal group (P<0.001) established the increased chamber stiffness associated with pseudonormal patterns. Similarly, higher PDF (worse) relaxation parameter c and longer DT
r
observed in the pseudonormal group compared with normal group (P<0.001) established impaired relaxation compared with normal group. Shorter DT
s (higher PDF stiffness param-
eter k) with longer DTr (higher [worse] relaxation parameter
c) in pseudonormal than in normal reveals how simultane-ously increased stiffness and impaired relaxation oppose each other in generating pseudonormal E-waves that conventional analysis cannot distinguish from normal. The fraction of DT accounted for by relaxation (R) in the pseudonormal group is significantly higher than in the normal group (P<0.001). These results quantify the simultaneous increase in stiffness (that shortens DT) and impairment in relaxation (that length-ens DT) that oppose each other to generate E-waves that are indistinguishable from normal. Furthermore, PDF analysis and fractionation of DT to its stiffness and relaxation com-ponents distinguishes pseudonormal from normal without requirement for load varying respiratory maneuvers or mea-surement of E′. By using subjects as their own controls and trending their progress echocardiographically, the method is well suited to assess the beneficial or adverse chamber remodeling consequences of alternative pharmacological approaches on DF in all subjects. In the blinded study (no E′-wave or LVEDP information), the cut point selection of R=0.28 from unblinded study yielded high sensitivity (0.90) and specificity (0.86) in differentiating normal and pseudo-normal groups.
Limitations
Sample SizeAlthough the total number of data sets subjected to blinded analysis (n=42) by an independent observer, based on the initial 30 unblinded and 12 additional blinded (for initial comparison to the 30 unblinded datasets), is modest and may be viewed as a potential statistical limitation, the total number of E-waves analyzed (n=931) mitigates the sample size limitation to an acceptable degree. The sample size limitation is also mitigated by the demonstrated high sensi-tivity and specificity achieved by the blinded study in differ-entiating pseudonormal from normal filling. The unblinded (30 subjects) and blinded (42 subjects) studies had power of >90% to detect a true difference of DT
s, DT
r, R, and S
parameters between pseudonormal and normal group with a significance level of 0.01.
Effect of Heart RateAlthough the PDF formalism is applicable to all E-waves, robust analysis is achieved for E-waves that have a clear ter-mination followed by diastasis. E-wave analysis becomes less reliable when the A-wave merges with the E-wave and covers more than two-thirds of the E-wave deceleratio por-tion. This typically occurs at heart rate (HR) >90 bpm.41,42 In the present study, our inclusion criteria required use of data sets with clearly discernible E-waves followed by a dia-static interval; hence, variation in HR among our subjects should not affect our results. It was previously shown41,42 that for a 100% increase in HR (from 50 to 100 bpm), E-wave durations decrease by ≈15% (from ≈300 to 255 ms). PDF stiffness and relaxation parameters (k and c) as well as DT components (DT
r and DT
s) change only slightly (≈10%) as
the HR increases to levels where E- and A-waves merge, as diastasis is eliminated. Hence, if E-waves at those higher HRs were to be analyzed, we expect similar DT
r and R=DT
r/
DT, DTs and S=DT
s/DT, changes in keeping with the 10%
change in PDF parameters.
Interobserver LimitationThe fact that interobserver-variability/blinded analysis achieved 90% rather than 100% sensitivity and specificity in predicting normal versus pseudonormal is in part caused by the known interobserver variability of PDF method and variation of E-wave image quality, determination of E-wave contour features, such as amplitude, duration, and curvature. In spite of the 10% interobserver variability, the value of R remained unchanged.
ConclusionsDF was assessed via the PDF formalism by fractionating E-wave DT into its stiffness (DT
s) and relaxation (DT
r) com-
ponents in age-matched, pseudonormal and normal filling pattern groups in both unblinded and blinded groups. Both the PDF parameters by themselves and DT
s, DT
r differenti-
ated normal versus pseudonormal groups. Based on the cut point value of R=0.28 from the unblinded study, the blinded study yielded excellent sensitivity (0.90) and specificity (0.86) in predicting pseudonormal versus normal based on
by guest on May 2, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from

7 Mossahebi et al E-waves Distinguish Pseudonormal vs. Normal Filling
E-wave analysis alone. The method revealed and quantified the opposing effects of stiffness (shortens DT) versus relax-ation (lengthens DT) on total DT, resulting in total DT being indistinguishable from normal. The method is well suited to assess the natural history of heart failure with preserved ejec-tion fraction and the beneficial or adverse chamber remodel-ing consequences of alternative pharmacological approaches on DF in all subjects.
AcknowledgmentsWe thank sonographer Peggy Brown for expert echocardiographic data acquisition and the staff of Barnes Jewish Hospital Cardiovascular Procedure Center’s Cardiac Catheterization Laboratory for their assistance. Discussions with Leonid Shmuylovich are gratefully acknowledged.
Sources of FundingThis work was supported in part by the Alan A. and Edith L Wolff Charitable Trust, St. Louis, and the Barnes-Jewish Hospital Foundation. Sina Mossahebi was supported in part by a teaching assistantship from the Physics Department, Washington University College of Arts and Sciences. Simeng Zhu was supported by the Washington University Compton Scholars Program.
DisclosuresNone.
References 1. Sharma K, Kass DA. Heart failure with preserved ejection fraction: mech-
anisms, clinical features, and therapies. Circ Res. 2014;115:79–96. doi: 10.1161/CIRCRESAHA.115.302922.
2. Maeder MT, Kaye DM. Heart failure with normal left ventricular ejec-tion fraction. J Am Coll Cardiol. 2009;53:905–918. doi: 10.1016/j.jacc.2008.12.007.
3. Zile MR, Brutsaert DL. New concepts in diastolic dysfunction and diastol-ic heart failure: Part I: diagnosis, prognosis, and measurements of diastolic function. Circulation. 2002;105:1387–1393.
4. Pasipoularides A. Evaluation of right and left ventricular diastol-ic filling. J Cardiovasc Transl Res. 2013;6:623–639. doi: 10.1007/s12265-013-9461-4.
5. Pasipoularides A. Heart’s Vortex: Intracardiac Blood Flow Phenomena. Shelton, CT: People’s Medical Publishing House; 2010.
6. Pasipoularides A. Right and left ventricular diastolic pressure-volume re-lations: a comprehensive review. J Cardiovasc Transl Res. 2013;6:239–252. doi: 10.1007/s12265-012-9424-1.
7. Little WC, Oh JK. Echocardiographic evaluation of diastolic function can be used to guide clinical care. Circulation. 2009;120:802–809. doi: 10.1161/CIRCULATIONAHA.109.869602.
8. Redfield MM, Jacobsen SJ, Burnett JC Jr, Mahoney DW, Bailey KR, Rodeheffer RJ. Burden of systolic and diastolic ventricular dysfunction in the community: appreciating the scope of the heart failure epidemic. JAMA. 2003;289:194–202.
9. Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK, Smiseth OA, Waggoner AD, Flachskampf FA, Pellikka PA, Evangelista A. Recommendations for the evaluation of left ventricular diastolic function by echocardiography. J Am Soc Echocardiogr. 2009;22:107–133. doi: 10.1016/j.echo.2008.11.023.
10. Mirsky I, Pasipoularides A. Clinical assessment of diastolic function. Prog Cardiovasc Dis. 1990;32:291–318.
11. Kovács SJ, Setser R, Hall AF. Left ventricular chamber stiffness from model-based image processing of transmitral Doppler E-waves. Coron Artery Dis. 1997;8:179–187.
12. Hall AF, Kovács SJ. Automated method for characterization of diastolic transmitral Doppler velocity contours: early rapid filling. Ultrasound Med Biol. 1994;20:107–116.
13. Bauman L, Chung CS, Karamanoglu M, Kovács SJ. The peak atrioven-tricular pressure gradient to transmitral flow relation: kinematic model
prediction with in vivo validation. J Am Soc Echocardiogr. 2004;17:839–844. doi: 10.1016/j.echo.2004.04.017.
14. Mossahebi S, Shmuylovich L, Kovács SJ. The thermodynamics of dias-tole: kinematic modeling-based derivation of the P-V loop to transmitral flow energy relation with in vivo validation. Am J Physiol Heart Circ Physiol. 2011;300:H514–H521. doi: 10.1152/ajpheart.00814.2010.
15. Mossahebi S, Zhu S, Chen H, Shmuylovich L, Ghosh E, Kovács SJ. Quantification of global diastolic function by kinematic modeling-based analysis of transmitral flow via the Parametrized Diastolic Filling formal-ism. J Vis Exp. 2014; 91:e51471. doi: 10.3791/51471.
16. Little WC, Ohno M, Kitzman DW, Thomas JD, Cheng CP. Determination of left ventricular chamber stiffness from the time for deceleration of early left ventricular filling. Circulation. 1995;92:1933–1939.
17. Shmuylovich L, Kovács SJ. E-wave deceleration time may not provide an accurate determination of LV chamber stiffness if LV relaxation/viscoelas-ticity is unknown. Am J Physiol Heart Circ Physiol. 2007;292:H2712–H2720. doi: 10.1152/ajpheart.01068.2006.
18. Mossahebi S, Kovács SJ. Decomposition of transmitral flow (E-wave) de-celeration time into stiffness and relaxation components: model-based pre-diction with in-vivo validation. Cardiovasc Eng Technol. 2014; 5:25–34.
19. Mossahebi S, Kovács SJ. Diastolic function in normal sinus rhythm vs. chronic atrial fibrillation: comparison by fractionation of E-wave decelera-tion time into stiffness and relaxation components. J AFIB. 2014;6:13–19.
20. Lisauskas JB, Singh J, Bowman AW, Kovács SJ. Chamber properties from transmitral flow: prediction of average and passive left ventricular dia-stolic stiffness. J Appl Physiol (1985). 2001;91:154–162.
21. Chung CS, Ajo DM, Kovács SJ. Isovolumic pressure-to-early rapid fill-ing decay rate relation: model-based derivation and validation via si-multaneous catheterization echocardiography. J Appl Physiol (1985). 2006;100:528–534. doi: 10.1152/japplphysiol.00617.2005.
22. Ohno M, Cheng CP, Little WC. Mechanism of altered patterns of left ventricular filling during the development of congestive heart failure. Circulation. 1994;89:2241–2250.
23. Sohn DW, Chai IH, Lee DJ, Kim HC, Kim HS, Oh BH, Lee MM, Park YB, Choi YS, Seo JD, Lee YW. Assessment of mitral annulus velocity by Doppler tissue imaging in the evaluation of left ventricular diastolic func-tion. J Am Coll Cardiol. 1997;30:474–480.
24. Klein AL, Burstow DJ, Tajik AJ, Zachariah PK, Bailey KR, Seward JB. Effects of age on left ventricular dimensions and filling dynamics in 117 normal persons. Mayo Clin Proc. 1994;69:212–224.
25. Kovács SJ, Rosado J, Manson McGuire AL, Hall AF. Can trasmi-tral Doppler E-waves differentiate hypertensive hearts from normal? Hypertension. 1997;30:788–795.
26. Kovács SJ, Meisner JS, Yellin EL. Modeling of diastole. Cardiol Clin. 2000;18:459–487.
27. Gottdiener JS, Bednarz J, Devereux R, Gardin J, Klein A, Manning WJ, Morehead A, Kitzman D, Oh J, Quinones M, Schiller NB, Stein JH, Weissman NJ; American Society of Echocardiography. American Society of Echocardiography recommendations for use of echocardiog-raphy in clinical trials. J Am Soc Echocardiogr. 2004;17:1086–1119. doi: 10.1016/j.echo.2004.07.013.
28. Appleton CP, Firstenberg MS, Garcia MJ, Thomas JD. The echo-Doppler evaluation of left ventricular diastolic function. A current perspective. Cardiol Clin. 2000;18:513–46, ix.
29. Feigenbaum H. Echocardiography. Philadelphia, PA: Lippincott Williams & Wilkins; 2005.
30. Kovács SJ Jr, Barzilai B, Pérez JE. Evaluation of diastolic function with Doppler echocardiography: the PDF formalism. Am J Physiol. 1987;252(1 Pt 2):H178–H187.
31. Kovács SJ, McQueen MD, Peskin CS. Modelling cardiac fluid dynamics and diastolic function. Phil Trans R Soc Lon (A). 2001;359:1299–1314.
32. Hosmer DW, Lemeshow S. Applied Logistic Regression, 2nd ed. New York: John Wiley & Sons. 2000:160–162.
33. Ghosh E, Kovács SJ. Early left ventricular diastolic function quantitation using directional impedances. Ann Biomed Eng. 2013;41:1269–1278. doi: 10.1007/s10439-013-0756-z.
34. Lisauskas J, Singh J, Courtois M, Kovács SJ. The relation of the peak Doppler E-wave to peak mitral annulus velocity ratio to diastolic function. Ultrasound Med Biol. 2001;27:499–507.
35. Ommen SR, Nishimura RA, Appleton CP, Miller FA, Oh JK, Redfield MM, Tajik AJ. Clinical utility of Doppler echocardiography and tissue Doppler imaging in the estimation of left ventricular filling pressures: a comparative simultaneous Doppler-catheterization study. Circulation. 2000;102:1788–1794.
by guest on May 2, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from

8 Mossahebi et al E-waves Distinguish Pseudonormal vs. Normal Filling
36. Riordan MM, Chung CS, Kovács SJ. Diabetes and diastolic function: stiffness and relaxation from transmitral flow. Ultrasound Med Biol. 2005;31:1589–1596. doi: 10.1016/j.ultrasmedbio.2005.07.015.
37. Riordan MM, Kovács SJ. Quantitation of mitral annular oscillations and longitudinal “ringing” of the left ventricle: a new window into longitu-dinal diastolic function. J Appl Physiol (1985). 2006;100:112–119. doi: 10.1152/japplphysiol.00844.2005.
38. Pasipoularides A, Shu M, Shah A, Womack MS, Glower DD. Diastolic right ventricular filling vortex in normal and volume overload states. Am J Physiol Heart Circ Physiol. 2003;284:H1064–H1072.
39. Zhang W, Chung CS, Shmuylovich L, Kovács SJ. Is left ventricular volume during diastasis the real equilibrium volume, and what is its relationship
to diastolic suction? J Appl Physiol (1985). 2008;105:1012–1014. doi: 10.1152/japplphysiol.00799.2007.
40. Mossahebi S, Kovács SJ. Kinematic modeling-based left ventricular dia-static (passive) chamber stiffness determination with in-vivo validation. Ann Biomed Eng. 2012;40:987–995. doi: 10.1007/s10439-011-0458-3.
41. Chung CS, Karamanoglu M, Kovács SJ. Duration of diastole and its phases as a function of heart rate during supine bicycle exercise. Am J Physiol Heart Circ Physiol. 2004;287:H2003–H2008. doi: 10.1152/ajpheart.00404.2004.
42. Chung CS, Kovács SJ. Consequences of increasing heart rate on decelera-tion time, the velocity-time integral, and E/A. Am J Cardiol. 2006;97:130–136. doi: 10.1016/j.amjcard.2005.07.116.
CLINICAL PERSPECTIVEEchocardiographic imaging–based assessment of diastolic function has relied on phenomenologic and correlation-based global indexes, such as E/A, E/E′, E-wave DT, and so on rather than causality-based indexes that directly stem from the chamber’s role as a mechanical suction pump in early diastole. Because suction-initiated early rapid filling operates mecha-nistically the same way in all hearts, it is governed by Newton’s Law, that is, an equation of motion. E-wave contours predicted by solution of the equation of motion show excellent agreement with clinical E-wave contours. Hence, what quan-titatively differentiates diastolic function in one heart from another are the parameters (stiffness, relaxation, and load) of the equation. The parametrized diastolic filling formalism provides those parameters by validated analysis of E-wave contours. Accordingly, parametrized diastolic filling analysis of E-waves and fractionation of E-wave DT to its stiffness (DT
s) and
relaxation (DTr) components as detailed here distinguishes PN from NL without requirement for load varying respiratory
maneuvers or measurement of E′. By using subjects as their own controls and trending their progress via echocardiography, the method is ideally suited to assess the beneficial or adverse chamber remodeling consequences of alternative pharmaco-logical regimens on diastolic function. This novel method and these results allow clinicians to track DT
s and DT
r not only as
diastolic function determinants, but also as determinants of prognosis and rehospitalization for heart failure as well.
by guest on May 2, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from

Sina Mossahebi, Simeng Zhu and Sándor J. KovácsDistinguishes Pseudonormal From Normal Filling
Fractionating E-Wave Deceleration Time Into Its Stiffness and Relaxation Components
Print ISSN: 1941-9651. Online ISSN: 1942-0080 Copyright © 2015 American Heart Association, Inc. All rights reserved.
Dallas, TX 75231is published by the American Heart Association, 7272 Greenville Avenue,Circulation: Cardiovascular Imaging
doi: 10.1161/CIRCIMAGING.114.0021772015;8:Circ Cardiovasc Imaging.
http://circimaging.ahajournals.org/content/8/1/e002177World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circimaging.ahajournals.org/content/suppl/2015/01/16/CIRCIMAGING.114.002177.DC1Data Supplement (unedited) at:
http://circimaging.ahajournals.org//subscriptions/
is online at: Circulation: Cardiovascular Imaging Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
requested is located, click Request Permissions in the middle column of the Web page under Services. FurtherCenter, not the Editorial Office. Once the online version of the published article for which permission is being
can be obtained via RightsLink, a service of the Copyright ClearanceCirculation: Cardiovascular Imagingin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on May 2, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from

Supplemental Material
Appendix 1
The PDF Formalism
Suction initiated filling is modeled via the Parametrized Diastolic Filling (PDF) formalism. The
model uses a linear, bi-directional spring to approximate the kinematics of early filling in
analogy to the recoil from rest of a damped, simple harmonic oscillator [1]. In accordance with
Newton’s second law, the equation of motion is:
[A.1]
Because the E-wave has zero initial velocity, the model’s initial velocity is zero (v(0)=0).
However, the simple harmonic oscillator (SHO) has a non-zero initial spring displacement, xo.
Systole stores elastic strain in tissue, which at mitral valve opening, is available to power
mechanical recoil and the ventricular suction process. Equation 1 allows calculation of
parameters c and k per unit mass. The predicted contour of the clinical E-wave is obtained from
the solution for the SHO velocity, which for underdamped (c2<4k) kinematics is:
[A.2]
where . The determination of PDF parameters from each E-wave generates a
unique set of xo, c, and k [2] values for each contour. The three parameters xo, c, and k encompass
the (lumped) physiologic determinants of all E-wave contours. The initial oscillator displacement
xo (cm) is linearly related to the velocity-time integral (VTI) of the E-wave [3]. Chamber
stiffness (dP/dV) is linearly related to the spring constant k (g/s2) [3,4], while the chamber
viscoelasticity/relaxation index c (g/s) characterizes the resistance of the process [3,5]. PDF
d 2x
dt2 c
dx
dt kx 0
)sin()2/exp()( tctkx
tv o
2/4 2ck

analysis of Doppler E-waves can accurately determine diastatic (passive) LV chamber stiffness
[6]. E-waves with long concave up deceleration portions (‘delayed relaxation pattern’) are fit by
the ‘overdamped’ solution (c2>4k) and have higher c values, while E-waves that resemble the
first half of a sine wave are fit by the underdamped solution and have lower c values [7].
Briefly, echocardiographic images are cropped, the mitral E-wave maximum velocity envelopes
are identified and fit by the PDF generated solution using the Levenberg-Marquardt algorithm to
yield the best-fit PDF parameter xo, c, and k, values. The process is achieved using a custom Lab
VIEW (National Instruments, Austin, TX) interface [2]. In addition to providing parameter
values the algorithm also provides a simultaneous measure of goodness of fit. The details of
methods are available at Journal of Visualized Experiments [8]. These algorithms are available
for download for any user on our website: http://CBL1.wustl.edu

Appendix 2
Determination of stiffness and relaxation components of E-wave deceleration time
PDF model predicts that E-wave deceleration time (DT) is a function of both stiffness and
relaxation [7]. PDF-based E-wave analysis provides a method for fractionating total DT into its
stiffness (DTs) and relaxation (DTr) components such that DT=DTs+DTr. The fractionation
method has been validated with DTs and DTr correlating with simultaneous stiffness (dP/dV) and
relaxation (tau) with r=0.82 and r=0.94 respectively [9].
The duration of the E-wave, AT, and DT are measured as usual from Doppler echo
images using the conventional triangle approximation to E-wave shapes (Figure 1). The effect of
delayed relaxation on an ideal (generated by recoil only) E-wave is to decrease its peak
amplitude and lengthen its DT. Accordingly, DTr is determined by using the same xo and k as the
original E-wave but setting c=0 and thereby providing the PDF generated ideal contour.
Subtracting the ideal E-wave’s shorter duration from actual total duration yields DTr (See Figure
1). Therefore, E-wave DT is decomposed into its components as DT = DTs + DTr. It is known
that DTs, DTr are only weakly load and heart rate dependent [9]. Fractionation is achieved by
dividing by DT yielding 1= S + R, where S is the fraction of total DT due to stiffness and R is the
fraction of total DT due to relaxation. Hence, S=DTs/DT, and R=DTr/DT.

References
1. Kovács SJ Jr, Barzilai B, Pérez JE. Evaluation of diastolic function with Doppler echocardiography: the PDF formalism. Am J Physiol. 1987; 252:H178-H187.
2. Hall AF, Kovács SJ. Automated method for characterization of diastolic transmitral Doppler velocity contours: early rapid filling. Ultrasound Med Biol. 1994; 20:107-116.
3. Kovács SJ, Sester R, Hall AF. Left ventricular chamber stiffness from model-based image processing of transmitral Doppler E-waves. Cor Art Dis. 1997; 8:179-187.
4. Lisauskas JB, Singh J, Bowman AW, Kovács SJ. Chamber properties from transmitral flow: prediction of average and passive left ventricular diastolic stiffness. J Appl Physiol. 2001; 91:154–162.
5. Kovács SJ, Meisner JS, Yellin EL. Modeling of diastole. Cardiology Clinics. 2000; 18:459-487.
6. Mossahebi S, Kovács SJ. Kinematic modeling-based left ventricular diastatic (passive) chamber stiffness determination with in-vivo validation. Ann Biomed Eng. 2012; 40:987-995.
7. Shmuylovich L, Kovács SJ. E-wave deceleration time may not provide an accurate determination of left ventricular chamber stiffness if left ventricular relaxation/viscoelasticity is unknown. Am J Physiol, Heart Circ Physiol. 2007; 292:H2712-H2720.
8. Mossahebi S, Zhu S, Chen H, Shmuylovich L, Ghosh E, Kovács SJ. Quantification of global diastolic function by kinematic modeling-based analysis of transmitral flow via the Parametrized Diastolic Filling formalism. J Vis Exp. 2014; 91:e51471.
9. Mossahebi S, Kovács SJ. Decomposition of transmitral flow (E-wave) deceleration time into stiffness and relaxation components: Model-based prediction with in-vivo validation. Cardiovascular Engineering & Technology. 2014; 5:25-34.