Ultrasonographic diagnosis of a large placental intervillous thrombosis associated with elevated...
3
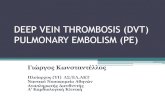
Ultrasonographic diagnosis of a large placental intervillous thrombosis associated with elevated maternal serum a -fetoprotein level Eric Jauniaux, MD,* Donald Gibb, MD, Gonzalo Moscoso, MD, and Stuart Campbell, FRCOG London, England A placental lesion associated with elevated maternal serum a-fetoprotein level and a positive Kleihauer-Betke test is reported. Serial ultrasonograms showed a progressive increase in the echogenicity of the lesion that corresponded to a large intervillous thrombosis after delivery. This case illustrates the importance of detailed ultrasonographic and pathologic placental investigations in pregnancies with unexplained elevated levels of a-fetoprotein. (AM J OasTET GVNECOL 1990;163:1558-60.) Key words: Prenatal diagnosis, u-fetoprotein, placenta, ultrasonography From the Obstetric Ultrasound Unit, Department of Obstetrics and Gynecology, and the Fetal and Perinatal Pathology Unit, King's Col- lege Hospital School of Medicine and Dentistry, University of London. Received for publication February 8,1990; revised May 4,1990; accepted May 18, 1990. Reprint requests: Eric Jauniaux, MD, Department of Obstetrics and Gynecology, Academic Hospital Erasme, 808 Route de Lennik, 1070 Brussels, Belgium. *Research fellow from the Free University of Brussels (ULB), Bel- gium, supported by the British Council (Sir Alexander Fleming Award, 1989). 6/1122485 Fig. 1. Composite compound scan of uterus (U) and placenta (P) shows heterogeneous and hypo- echoic placental lesion (asterisk) at 17 (A) and 22 (B) weeks' gestation. For comparison, C, a retro- placental hematoma (star) at 32 weeks, 2 weeks after an invasive procedure, and D, a recent marginal hematoma (star) at 18 weeks. 1558
Transcript of Ultrasonographic diagnosis of a large placental intervillous thrombosis associated with elevated...

Ultrasonographic diagnosis of a large placental intervillous thrombosis associated with elevated maternal serum a -fetoprotein level
Eric Jauniaux, MD,* Donald Gibb, MD, Gonzalo Moscoso, MD, and Stuart Campbell, FRCOG
London, England
A placental lesion associated with elevated maternal serum a-fetoprotein level and a positive Kleihauer-Betke test is reported. Serial ultrasonograms showed a progressive increase in the echogenicity
of the lesion that corresponded to a large intervillous thrombosis after delivery. This case illustrates the importance of detailed ultrasonographic and pathologic placental investigations in pregnancies with unexplained elevated levels of a-fetoprotein. (AM J OasTET GVNECOL 1990;163:1558-60.)
Key words: Prenatal diagnosis, u-fetoprotein, placenta, ultrasonography
From the Obstetric Ultrasound Unit, Department of Obstetrics and Gynecology, and the Fetal and Perinatal Pathology Unit, King's College Hospital School of Medicine and Dentistry, University of London. Received for publication February 8,1990; revised May 4,1990; accepted May 18, 1990. Reprint requests: Eric Jauniaux, MD, Department of Obstetrics and
Gynecology, Academic Hospital Erasme, 808 Route de Lennik, 1070 Brussels, Belgium. *Research fellow from the Free University of Brussels (ULB), Belgium, supported by the British Council (Sir Alexander Fleming Award, 1989). 6/1122485
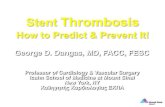
Fig. 1. Composite compound scan of uterus (U) and placenta (P) shows heterogeneous and hypoechoic placental lesion (asterisk) at 17 (A) and 22 (B) weeks' gestation. For comparison, C, a retroplacental hematoma (star) at 32 weeks, 2 weeks after an invasive procedure, and D, a recent marginal hematoma (star) at 18 weeks.
1558

Volume Iti:{ "umber 5. Part I
Prenatal diagnosis of placental intervillous thrombosis 1559
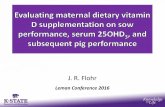
Fig. 2. A, Transverse and longitudinal ultrasonogram of placenta shows placental lesion at 35 weeks (asterisk). B, Lesion is isoechoic and surrounded by sonolucent spaces containing turbulent blood flow on real-time imaging. C, Macroscopic view of lesion (asterisk) corresponds histologically to an old intervillous thrombosis.
Maternal serum a-fetoprotein (AFP) concentrations are routinely performed between 16 and 20 weeks' gestation as a screening test for different fetal anomalies. Elevated AFP levels can also be found in association with well-defined placental lesions without associated fetal anomalies such as chorioangiomas l or in combined fetoplacental pathologic conditions such as triploidy." We described an unusual placental lesion that ultrasonographically resembled a hematoma or a chorioangioma and was associated with an elevated maternal serum AFP level.
Case report
A 29-year-old healthy nonsmoking primigravid woman was referred because of elevated maternal serum AFP levels (4.5 and 4.8 multiples of the median). At 18 weeks' gestation ultrasonography showed a singleton and anatomically normal fetus with measurements consistent with the estimated gestation. The placenta was fundal and contained a 3.1 x 3.5 em heterogeneous and hypoechoic lesion (Fig. 1, A). A hematoma or a chorioangioma was suspected and ultrasonographic follow-up of the pregnancy was started. At that time a Kleihauer-Betke test had positive results.
At 22 weeks the lesion was larger, well demarcated
(Fig. 1, B), and contained turbulent blood flow on realtime scanning. Weak flow velocity waveforms with maternal characteristics were detected at the level of the lesion on color Doppler flow imaging. These findings were compared with the ultrasonographic features of a retroplacental hematoma and of a subchorionic (marginal) hematoma, both of which were subsequently confirmed after delivery. In these two cases no blood How was found in the lesion. These lesions were hyperechoic to isoechoic in the acute stage (Fig. 1, D) and hypoechoic to sonolucent within 2 weeks (Fig. 1, C).
At 29 weeks slow fetal growth (5th percentile) and reduced amniotic fluid volume were noted. Fetal and uteroplacental Doppler studies were within our normal ranges. The placental lesion was homogeneous, isoechoic (Fig. 2, A), and surrounded by small sonolucent spaces (Fig. 2, B) that contained turbulent flow. Similar antepartum features were observed until term. Because of breech presentation and poor fetal growth, the patient was delivered by cesarean section of a healthy female infant weighing 2230 gm. The postpartum course was uneventful.
The placenta weighed 410 gm. Examination of the slices showed a white lesion of 3 x 3 x 4 em, composed histologically oflaminated fibrin surrounded by several groups of infarcted villi (Fig. 2, C). There was no evidence of a retroplacental hematoma.

Jauniaux et al.
Comment
Ultrasonographic investigation of the placenta in patients with elevated maternal serum AFP levels has shown a high incidence of retroplacental or subchorionic placental hemorrhage. I However, in this study serial ultrasonographic examination and pathologic correlation were not performed.
The placenta is a dynamic organ. As demonstrated in this case, the ultrasonographic appearances are dependent on gestational age and the evolution of the lesion. At the time of AFP screening, the lesion was hypoechoic and contained turbulent blood flow. Six weeks later the lesion was more echogenic. In contrast, resolving hematomas become sonolucent and do not demonstrate blood flow. A placental chorioangioma was also unlikely because color Doppler flow studies of the lesion only detected maternal flow velocity waveforms.
The association of an increased maternal serum AFP level with a positive Kleihauer-Betke test is suggestive
November 1990 Am J Obstet Gynecol
of a breakdown of the placental barrier2 and should lead to detailed assessment of placental appearance.
Elevated maternal serum AFP levels, combined with abnormal placental ultrasonographic features, may be an early indication of subsequent perinatal complications, particularly fetal intrauterine growth retardation. Further placental ultrasonographic and pathologic investigations in a prospective manner are needed to validate the relationship between the development of placental lesion, elevated maternal serum AFP, and fetal outcome.
REFERENCES
1. Fleischer AC, Kurtz AB, Wapner RJ, et al. Elevated alphafetoprotein and a normal fetal sonogram: association with placental abnormalities. AJR 1988;150:881-3.
2. Berkeley AS, Killackey MA, Cederqvist LL. Elevated maternal serum a-fetoprotein levels associated with breakdown in fetal-maternal-placental barrier. AM J OBSTET GyNECOL 1983;146:859-61.
Direct ultrasonographic measurement of fetal lung length in normal pregnancies and pregnancies complicated by prolonged rupture of membranes
Alistair B. Roberts, MD, and Jennifer M. Mitchell, DMU
Auckland, New Zealand
Fetal lung length was measured directly with ultrasonography in 20 patients with prolonged rupture of membranes, commencing before 25 weeks' gestation. Measurements were made weekly and compared with data collected from 310 normal pregnancies. Measurement of fetal lung length by ultrasonography was a good predictor of pulmonary hypoplasia, predicting >90% of cases. There was a good correlation between lung size assessed by the last ultrasonographic examination and lung weight postmortem (r = 0.783, P < 0.05). Lung length measurements were superior to fetal chest circumference measurements in the identification of pulmonary hypoplasia. There was a significant negative association between the amount of amniotic fluid and pulmonary hypoplasia (p < 0.05). There were fetuses with pulmonary hypoplasia that had respiratory movements seen at the majority of ultrasonographic examinations. (AM J easlET GYNECOL 1990;163:1560-6.)
Key words: Fetal lung, fetal breathing, oligohydramnios, pulmonary hypoplasia, ultrasonography
From the Department of Obstetrics, Auckland University Medical School, National Women's Hospital. Received for publication january 31, 1990; revised May 18, 1990; accepted july 27, 1990. Reprint requests: A. B. Roberts, MD, Department of Obstetrics and Gynecology, Auckland University Medical School, National Women's Hospital, Claude Road, Auckland, New Zealand. 6/1/24145
1560
Fetal pulmonary hypoplasia is a significant contributor to neonatal death. I It occurs as a consequence of prolonged rupture of membranes,2 renal agenesis, diaphragmatic hernia, pleural effusions, and skeletal dysplasias.3
.5 Antepartum prediction of pulmonary hypo
plasia has been elusive.6
Ultrasonography has contributed by use of mea-