
Stent Thrombosis - Livemedia.grstatic.livemedia.gr/hcs2/documents/al18822_us41...Early stent...
43
George D. Dangas, MD, FACC, FESC Professor of Cardiology & Vascular Surgery Icahn School of Medicine at Mount Sinai New York, NY Καθηγητής Καρδιολογίας ΕΚΠΑ Stent Thrombosis How to Predict & Prevent It!
Transcript of Stent Thrombosis - Livemedia.grstatic.livemedia.gr/hcs2/documents/al18822_us41...Early stent...
-
George D. Dangas, MD, FACC, FESC
Professor of Cardiology & Vascular Surgery Icahn School of Medicine at Mount Sinai
New York, NY Καθηγητής Καρδιολογίας ΕΚΠΑ
Stent Thrombosis How to Predict & Prevent It!
-
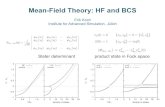
History of Stent Thrombosis
1. Schatz RA et al. Circulation.1991;83:148; 2. Fischman DL et al. N Engl J Med. 1994;331496; 3 Colombo A et al. Circulation.1995;91:1676; 4. Schömig A et al.Circulation.1994,90:2716; 5. Leon M et al. N Engl J Med. 1998;339:1665; Joner M et al. J Am Coll Cardiol. 2006;48:193
0
4
8
12
16
1 2 3 4 5PS1 1991
STRESS2 1993
Colombo3 1995
STARS5 1997
Sten
t thr
ombo
sis
(%)
16%
3.5%1.4%
0.6%0.8%
ISAR4 1996
CoumadinHigh-pressure balloons
and DAPT
-
Very Late
> 1 year
Late
Subacute 24 hours to 30 days
24 Hours
Timing of ST After Stent Implantation
Acute ST
>30 days (but within 1 year)
Cutlip DE et al. Circulation. 2007;115:2344-51
“Early”
-
Procedure
Predictors of Stent Thrombosis The good (Patient), the bad (Procedure) and the ugly (Device)
Stent Thrombosis
Patient
Device• Type of stent • Polymer integrity and
reactions • Drug effects • Covered Stents • Incomplete Vascular Healing
and / or Inadequate Neointimal Coverage
• Hypersensitivity to drug coating or polymer
• Neoatherosclerosis
• Residual Edge Dissection Dissection
• Lesion / Stent Length • Vessel / Stent Diameter • Complex Lesions • Incomplete Stent Apposition
• ACS / STEMI • Diabetes Mellitus • Chronic Kidney Disease • LV Dysfunction • Saphenous Vein Graft
• Platelet Reactivity • Premature cessation of
DAPT • APT Non-Responsiveness • Malignancy
-
Stent Thrombosis With Drug-Eluting Stents and Bioresorbable Scaffolds Evidence From a Network Meta-Analysis of 147 Trials
A total of 147 trials including 126,526 patients
Kang S et al., J Am Coll Cardiol Intv. 2016;9(12):1203-1212
-
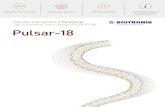
0
1,8
ML VISION (81 µm) TS Vision (162 µm) Xience V (96,6 µm)
0,8
1,5
1,0
Impact of strut thickness
Kolandaivelu K et al., Circulation 2011; 123:1400-1409
Relative ex vivo thrombogenicityLD
H A
dsor
banc
e fo
r Ste
nt F
orm
ulat
ion
/ LD
H A
bsor
banc
e fo
r ML
Visi
on (8
1µm
)
Hematotoxilin and eosin staining, 3 days
after implantation
Computational models depicting flow
alterations
-
Pathobiology of ST with DES
-
INCOMPLETE STENT APPOSITION
Attizzani GF et al., J Am Coll Cardiol. 2014 Apr 15;63(14):1355-67
Positive Vessel Remodeling
Thrombus Dissolution
Stent – Vessel Size Mismatch
Cook S et al., Circulation. 2007;115:2426-2434
-
Stent Underexpansion Poses a ST Risk
-
Adjusted risk of definite or probable stent thrombosis across complex PCI
components
Giustino G et al; J Am Coll Cardiol. 2016 Aug 25. pii: S0735-1097(16)34935-X
-
429 Healthy Amish after Clopidogrel 75
mg X 7dP=1.5 X 10-13
Shuldiner AR et al., JAMA 2009;302(8):849-858
CPY2C19*2 explained 12% of variance in Clopidogrel Response
CYP2C19 and Clopidogrel Responsiveness
-
Combined clinical and genetic model for ST risk prediction
Cayla G. et al., JAMA. 2011;306:1765-1774.
Genetic Model – AUC: 0.68; 95% CI, 0.62-0.74; P < 0.001
Clinical Model – AUC: 0.73; 95% CI, 0.67-0.78; P < 0.001
Combined Model – AUC: 0.78; 95% CI: 0.73-0.83; P < 0.001
-
* Log-rank P values adjusted for multiple comparisons
N=3041
Q1 taken as referent
Meta-Analysis of OTR and Ischemic Events Post-PCI Increasing Risk With Greater Residual Reactivity
Brar S et al, J Am Coll Cardiol. 2011 Nov 1;58(19):1945-54
-
ADAPT-DES: Unadjusted and
Adjusted ST Rates According to PRU
Stone G et al - Lancet 2013; 382: 614–23
-
ADAPT-DES IVUS SUBSTUDY: IVUS Planar Analysis
A. Maehara – TCT 2014
-
Use of IVUS Reduces Stent Thrombosis and Myocardial Infarction Results from the Prospective, Multicenter
ADAPT-DES Study
A. Maehara – TCT 2014
-
STENT THROMBOSIS -Pharmacotherapy-
-
2277923
2253 2143 2088 2027 1684898 847 835 801 673
Number at riskP-R HeparinNo P-R Heparin
p =
-
Clopidogrel Double vs Standard Dose
Mehta S. et al. Lancet. 2010 Oct 9;376(9748):1233-43
Clopidogrel standard dose Clopidogrel double dose
Adjusted HR 0.54 (0.39-0.74) P=0.0001
Clopidogrel standard-dose Clopidogrel double-dose
Number at risk
8703 8560
8561 8444
8482 8390
8455 8366
8438 8356
8428 8347
0 3 6 9 12 15 18 21 24 27 300%
0.6%
0.8%
1.0%
1.2%
1.4%
0.4%
0.2%Ste
nt th
rom
bosi
s (%
)
Days
Definite Stent Thrombosis (angio confirmed)
-
TRITON-TIMI-38
Wiviott S.D. et al. Lancet. 2008;371:1353-63
DAYS
HR 0.41 [0.29-0.59] P
-
PLATO Stent Thrombosis
12 M
onth
Ev
entR
ate
(%)
0
1,3
2,5
3,8
5
Definite Definite, probable or possible
2,82,1
1,3
3,62,8
1,9
Clopidogrel (n=5,649) Ticagrelor (n=5,640)
HR(95%CI) = 0.67 (0.50–0.91)
P=0.009
HR(95%CI) = 0.77 (0.62–0.95)
P=0.01
HR(95%CI) = 0.75 (0.59–0.95)
P=0.02
Wallentin L. et al. NEJM 2009;361:1045-57
-
CHAMPION-PHOENIX Stent Thrombosis reduction with Cangrelor
Bhatt DL et al ., N Engl J Med. 2013 Apr 4;368(14):1303-13
-
IPST in CHAMPION PHOENIX
Généreux P et al. JACC Vol. 63, No. 7, 2014
10,939 pts assessed by a blinded core lab Impact on 30-day mortality
-
Dangas GD et al; JACC 2012;59(20):1752-9
Mortality Following Stent Thrombosis Occurring In-Hospital versus
Out-Of-Hospital: Results from HORIZONS-AMI Mortality according to ARC timing definitions of ST
-
• Patient-level pooled analysis from HORIZONS-AMI and EUROMAX
• 30-day outcomes in 4935 patients undergoing pPCI with stent implantation at 188 international sites, randomized to either bivalirudin or UFH±GPI.
• Among patients with early ST, the propensity-adjusted risk of subsequent mortality within 30 days was determined for patients treated with bivalirudin versus heparin±GPI in a Cox multivariable model, with ST treated as a time-dependent variable; all differing baseline covariates were included in the propensity model.
Dangas GD et al. Circulation Cardiovasc Interv. 2016;9:e003272. DOI: 10.1161/CIRCINTERVENTIONS.115.003272
Early Stent Thrombosis and Mortality After Primary Percutaneous Coronary Intervention in
ST-Segment–Elevation Myocardial Infarction
A Patient-Level Analysis of 2 Randomized Trials
-
0,0
0,8
1,5
0 2 4 4 6 8 10 12 14 16 18 20 22 24
Bivalirudin 2479 2448 2436 2434 2433 2431 2431 2430 2430 2429 2429 2429 2428
Heparin ± GPI 2456 2448 2447 2447 2445 2445 2443 2442 2442 2442 2442 2442 2442
Sten
t Thr
ombo
sis
(%)
Time in Hours
BivalirudinHeparin ± GPI
1.1%
0.04%
0.4%
0.2%
Log Rank P-Value:
-
Kaplan–Meier estimates of 30-day mortality in patients with stent thrombosis (ST) according to the timing of the ST
event and regimen
Dangas GD et al. Circulation Cardiovasc Interv. 2016;9:e003272. 10.1161/CIRCINTERVENTIONS.115.003272
-
Stent Thrombosis in 2016 and the
BVS ERA
-
DAPT Cessation And 2-Year Definite / Probable Stent
Thrombosis
Mehran R et al; Lancet. 2013 Nov 23;382(9906):1714-22
-
Numbers of patients at low, intermediate, and high bleeding risk, respectively, with similar proportions observed for the different thrombotic risk categories.
Coronary Thrombosis and Major Bleeding After PCI With Drug-Eluting Stents
Baber U et al., J Am Coll Cardiol. 2016 May 17;67(19):2224-34
-
Predicting Risks for Coronary Thrombosis and Major Bleeding After PCI with DES: Risk Scores from PARIS Registry
Integer Risk Score for Major Bleeding
Parameter Score
Age, years< 50 50-59 60-69 70-79 >80
0 +1 +2 +3 +4
BMI, kg/m2 35
+2 0 +2
Current Smoking
Yes No
+2 0
AnemiaPresent Absent
+3 0
CKD*Present Absent
+2 0
3ple Therapy on discharge
Yes No+2 0
Integer Risk Score for Coronary Thrombosis
Parameter Score
Diabetes MellitusNone Non-Insulin Insulin
0 +1 +3
Acute Coronary Syndrome
No Yes, Tn (-) Yes, Tn (+)0 +1 +2
Current SmokingYes No
+1 0
CKD* CrCl < 60 mL/min/1.73 m2
Present Absent
+2 0
Prior PCI Yes No+2 0
Prior CABGYes No
+2 0
Baber U et al., J Am Coll Cardiol. 2016 May 17;67(19):2224-34
-
PCI complexity & Stent thrombosis
Complex PCI is strongly associated with increased risk of definite or probable ST with a magnitude that was comparable to that of a history of prior MI or high-risk ACS presentation.
Giustino G et al., J Am Coll Cardiol. 2016 Aug 25. pii: S0735-1097(16)34935-X
-
ST risk score (UA/nonSTEMI & STEMI) Based on ACUITY & HORIZONS datasets
Variable Calculation Integer Assignment for Stent Thrombosis Risk Score
Type of Acute Coronary
Syndrome
NSTE-ACS w/o
ST changes +1
NSTE-ACS with ST
deviation +2 STEMI+4
Current Smoking Yes: +1 No: +0
Insulin treated diabetes Yes: +2 No: +0
History of PCI Yes: +1 No: +0
Baseline Platelet Count 400K/ul: +2
Absence of pre-PCI Heparin Yes: +1 No: 0Aneurysm or Ulceration Yes: +2 No: 0
Baseline TIMI flow grade 0/1 Yes: +1 No: 0
Final TIMI flow grade < 3 Yes: +1 No: 0
Number of Vessels Treated 1 vessel: +0 2 vessels: +1 3 vessels: +2
Dangas GD et al; JACC Cardiovasc Interv. 2012 Nov;5(11):1097-105
-
Derivation cohort
Validation cohort
Dangas GD et al., JACC Cardiovasc Interv. 2012 Nov;5(11):1097-105
-
Risk of ST with 1st- and 2nd-Generation Drug-Eluting Stents According to Duration of Dual Antiplatelet Therapy
Giustino G et al., J Am Coll Cardiol. 2015 Apr 7;65(13):1298-310
-
Timing of strut reabsorption
Indolfi C et al., Nat Rev Cardiol. 2016 Sep 29. doi: 10.1038/nrcardio.2016.151
Timing of vascular scaffold reabsorption
-
Gregg SW TCT presentation 2016
-
Puricel S. et al ., J Am Coll Cardiol. 2016 Mar 1;67(8):921-31
The implantation protocol used was an independent predictor of ScT
*For a 2.5-3.0 mm and 3.5 mm scaffold respectively
BVS specific protocol
Do not accept MLD
-
Timing and Mechanism of DES Thrombosis
Nakazawa et al. J Cardiol 2011;58:84-91 Claessen BE…Dangas GD; JACC Cardiovasc Interv 2014;7:1081-92
Early (12 Mo)
Procedural Delayed healing Abnormal vascular response
Underexpansion Uncovered struts Hypersensitivity
Edge dissection Fibrin deposition Extensive fibrin deposition Residual plaque Late malapposition?
Neoatherosclerosis
-
How to Minimize Stent Thrombosis• Better Patient selection
Screening for adherence and bleeding risk / ability to tolerate DAPT No upcoming surgical procedures (6 wk for BMS, 6–12 m for DES)
• Better Stent selection and deployment Consider use of stents with proven lower stent thrombosis rates Appropriate vessel sizing, high-pressure deployment/post-dilation Ensuring absence of edge dissections and adequate inflow/outflow Avoiding the use of 2 stents in bifurcation lesions (if possible)
• Better Peri- and post-procedure care Use of more potent oral antiplatelet regimens in appropriately indicated clinical scenarios (e.g. ACS with acceptable bleeding risk) Patient education and clinical follow-up are critical Continuation of DAPT without interruption whenever possible
Kirtane AJ. et al Circulation. 2011 Sep 13;124(11):1283-7
-
2nd Generation
DES (ZES, EES)
With or without potent
antiplatelet agents
(prasugrel, ticagrelor)
Short term DAPT
Prevention of Stent Thrombosis and DAPT
Favors the stronger antiplatelet agents/regimens Is Closely related to type of stent & adherence
-
Vulnerable Stent vs Patient ??
What are we treating?
20-25% risk of “falling” again in the
next 5 yearsc/o Dominic Angiolillo















![NeutronScattering: Theory,Instrumentation, …...2 0.5 1 1.5 2 0.5 1 1.5 2 2.5 α−MnMoO4, Logarithmic scale Q=(0,K,K/2) [rlu] Energy [meV] Figure1: Inelastic neutron scattering data](https://static.fdocument.org/doc/165x107/5f07fd297e708231d41fc546/neutronscattering-theoryinstrumentation-2-05-1-15-2-05-1-15-2-25-amnmoo4.jpg)