THESIS - Denis O' Dwyer
55
1 PATH40220: BSc. Biomedical Science Research Project Cellular Sources and Glycosylated Variants of Leucine rich-α 2 Glycoprotein in Heart Failure Denis O’ Dwyer Stage 4 Biomedical Health and Life Science University College Dublin Principle Investigator: Dr. John Baugh Senior Lecturer School of Medicine & Medical Science Conway Institute University College Dublin
-
Upload
denis-p-o-dwyer -
Category
Documents
-
view
264 -
download
2
Transcript of THESIS - Denis O' Dwyer

1
PATH40220: BSc. Biomedical Science Research Project
Cellular Sources and Glycosylated Variants of Leucine rich-α2 Glycoprotein
in Heart Failure
Denis O’ Dwyer
Stage 4 Biomedical Health and Life Science University College Dublin
Principle Investigator: Dr. John Baugh Senior Lecturer
School of Medicine & Medical Science Conway Institute
University College Dublin

2
A SIGNED COPY OF THIS FORM MUST ACCOMPANY ALL SUBMISSIONS FOR ASSESSMENT. STUDENTS SHOULD KEEP A COPY OF ALL WORK SUBMITTED.
Procedures for Submission and Late Submission
Ensure that you have checked the School’s procedures for the submission of assessments.
Note: There are penalties for the late submission of assessments. For further information please see the University’s Policy on Late Submission of Coursework, (http://www.ucd.ie/registry/academicsecretariat/pol.htm) Plagiarism: the unacknowledged inclusion of another person’s writings or ideas or works, in any formally presented work (including essays, examinations, projects, laboratory reports or presentations). The penalties associated with plagiarism designed to impose sanctions that reflect the seriousness of University’s commitment to academic integrity. Ensure that you have read the University’s Briefing for Students on Academic Integrity and Plagiarism and the UCD Plagiarism Statement, Plagiarism Policy and Procedures (http://www.ucd.ie/registry/academicsecretariat/pol.htm)
Student Name
Student Number
Assessment Title
Module Title Module Co-‐ordinator
Supervisor
Date Submitted OFFICE USE ONLY Date Received
OFFICE USE ONLY
Grade/Mark
Assessment Submission Form
Denis O’ Dwyer
11304411
BSc. Biomedical Science Research Project
PATH40220: Research Project BSc. BHLS
Prof. William Watson
Dr. John Baugh
26/2/2015
Declaration of Authorship I declare that all material in this assessment is my own work except where there is clear acknowledgement and appropriate reference to the work of others. Signed………………………………………………Date……………………………

3
Summary
Heart failure (HF) is characterized by abnormalities in cardiac structure and function
resulting in a reduced oxygen supply to the body. Diastolic HF or HF with preserved
Ejection Fraction (HFpEF) is the primary concern of this thesis. HFpEF is identified
by excessive myocardial fibrosis of the interstitium leading to reduce filling volumes.
Leucine rich α2-Glycoprotein (LRG), recently shown by our lab to be upregulated in
patients with HF, suggests that it plays a role in the disease process. However, there is
scant data about LRG and its physiological role to date, which means further study is
needed on this potential novel biomarker.
The aim of this research was to identify cellular sources of LRG in disease relevant
cells and also to examine their secretion patterns. This was completed by testing both
inflammatory and structural cells present during HF for LRG.
Preliminary tests using qPCR showed low LRG mRNA expression in THP1 and
VHCF cells. But interestingly after western blot, protein expression was identified in
each cell type. Banding at different molecular weights suggests the idea of LRGs
post-translational modification (PTM). Untreated VHCF cells showed high levels of
LRG in their medium. Serum-starvation was seen to inhibit extracellular LRG levels
in THP1 cells. Differentiation of the THP1 cells into macrophage by PMA at varying
concentrations showed no change to LRG protein levels. Finally the deglycosylating
enzyme PNGase F successfully reduced the glycosylated variants of LRG in THP1
and HepG2 supernatant and lysates.
In conclusion, the data suggests that LRG is constitutively expressed and secreted in
tissue relevant cells concerning HF. The presence of serum seems necessary for the
extracellular secretion of LRG in fibroblasts and THP1 cells and finally LRG is
heavily glycosylated and consists of many different glycovariants.

4
Table of Contents
Introduction .................................................................................................................. 5 1.1 Heart Failure ........................................................................................................ 6 1.2 Pathophysiology of HF ........................................................................................ 7 1.3 Leucine rich α2-Glycoprotein ............................................................................... 9 1.4 LRG as a Possible Therapeutic .......................................................................... 10 1.5 Purpose of this study .......................................................................................... 13
Methods and Materials .............................................................................................. 14 2.1 Materials ............................................................................................................ 15 2.2 Cell culture ......................................................................................................... 15 2.3 PBMC isolation .................................................................................................. 16 2.4 Treatment of cells .............................................................................................. 16 2.5 Quantitative Polymerase Chain Reaction Method ............................................. 18 2.6 Western Blotting Methods ................................................................................. 19 2.7 Ethical Consideration ......................................................................................... 22
Results ......................................................................................................................... 23 3.1 Basal LRG expression and production in structural and inflammatory components .............................................................................................................. 24
3.1.1 LRG mRNA expression in THP1 and VHCF cells .................................... 24 3.1.2 LRG protein production in THP1, VHCF and PBMC cells ....................... 25
3.2 LRG expression in treated cardiac fibroblasts ................................................... 26 3.2.1 LRG mRNA expression in VHCFs after TGF-β treatment and serum starvation .............................................................................................................. 26 3.2.2 LRG protein expression and secretion patterns in cardiac fibroblast ......... 27
3.3 Expression and secretion patterns of LRG in human monocytes ...................... 28 3.3.1 Effects of serum on LRG protein expression in THP1 cells ....................... 28 3.3.2 LRG protein expression in macrophage like cells ...................................... 29
3.4 Confirmation of LRG within each supernatant and lysate tested. ..................... 31 3.4.1 Effect of the deglycosylating agent PNGase F on the LRG glycoprotein .. 31 3.4.2 Testing for evidence of non-specific binding to serum in media ................ 32
Discussion ................................................................................................................... 33 4.1 General Discussion ............................................................................................ 34 4.2 LRG expression and secretion patterns in cardiac fibroblasts ........................... 35 4.3 LRG expression and secretion patterns in monocytes/macrophages ................. 37 4.4 Glycosylated variants of LRG ........................................................................... 39 4.5 Future direction .................................................................................................. 40 4.6 Conclusion ......................................................................................................... 41
Acknowledgements .................................................................................................... 42
Bibliography ............................................................................................................... 43 Appendix ..................................................................................................................... 47

5
Chapter 1
Introduction

6
1.1 Heart Failure
Heart failure is a progressive disease characterized by major remodeling of cardiac
tissue with a reduced cardiac output (McMurray et al., 2012). Inadequate tissue
perfusion results in organ failure. 1-2% of the adult population suffers from HF but
the extent of the complication is most prominent in people over the age of 65 years
(McMurray and Pfeffer, 2005). With an aging population, the number of persons with
HF will continue to rise exponentially (fig. 1) (Owan and Redfield, 2005). Figueroa
and Peters (2006) acknowledge the fact that multiple studies have shown HF to be
associated with a 2-year mortality rate of between 45-50%. The European Society of
Cardiology (2013) suggests typical symptoms of HF, which include fatigue,
breathlessness and ankle swelling. At present, the gold standard for assessing and
diagnosing HF is two-dimensional transthoracic Doppler echocardiography (Oh et al.,
2006).
Figure 1. The increasing trend of HF in individuals over 65 years
(Owan and Redfield, 2005)

7
1.2 Pathophysiology of HF The primary complication underlying HF is left ventricular dysfunction (Haydock and
Cowie, 2010). HF can be categorized into two different forms: Systolic HF and
Diastolic HF. Systolic dysfunction is characterised by a reduction in myocardial
contractility leading to a reduction in left ventricular ejection fraction (Chatterjee and
Massie, 2007). Diastolic Dysfunction is characterised by insufficient filling of the left
ventricle, which occurs due to the stiffness within the chambers walls (Baicu et al.,
2005). Increase in myocardial stiffness is primarily due hypertrophy and a fibrotic
response within the thickening myocardium (Rudolph et al., 2009). Diastolic HF or
HF with preserved ejection fraction (HFpEF) and its pathophysiology is the main
interest of this thesis.
Table 1. Different characteristics between HFpEF and HFrEF, showing the
imminent need for new therapies to treat DHF (Abbate et al., 2015). Randomised
controlled trials (RCT)

8
The majority of patients presenting with HFpEF are longstanding sufferers of
hypertension (Mandinov et al., 2000). Due to this prolonged insult, the body attempts
to repair the damaged cardiac tissue by aberrantly depositing excess extracellular
matrix proteins in a process known as tissue fibrosis (Krenning et al., 2010). Intrinsic
cardiac fibroblasts are activated by specific cytokines (eg. TGF-β), which causes their
differentiation into myofibroblasts and leads to an increased expression of collagen
type 1 (Fan et al., 2012). Monocytes are also intrinsically involved, infiltrating the
injured site (Glezeva and Baugh, 2014). Through their recruitment by a chemokine
gradient they initially differentiate into pro-inflammatory M1 macrophage, which
contribute to cardiac remodeling by increasing cardiac apoptotic events (Fernandez-
Velasco et al., 2014). Through specific cytokines (IL4, IL10), the cells differentiate to
M2 pro-fibrotic macrophage (Cho et al., 2014). These cells contribute to the
resolution and fibrosis seen in patients with HF (Fernandez-Velasco et al., 2014).
Possibly targeting the initial infiltration of monocytes or inhibiting the switch to a
pro-fibrotic phenotype may alleviate constrictive symptoms within the heart.
Pressure/Volume+overload+
Chemokine+induc5on+
M2+Macrophage+Monocyte+
M1+Macrophage+
LPS,+TNFCα+
IL10,+TGFCβ+
ECM Expression Collagen Deposition
Figure 2. Inflammatory and structural components contributing to the fibrotic
phenotype during HF.
!

9
1.3 Leucine rich α2-Glycoprotein
Leucine rich α2-Glycoprotein (LRG) is a highly conserved 132 amino acid protein,
consisting of 8 consensus repeats of leucine, proline or asparagine (Shirai et al.,
2009). Initially isolated as a trace element from human serum (Haupt and Baudner,
1977), it is approximately 45kDa in size and is heavily glycosylated, showing various
glycovarients after 2D-DIGE (Watson et al., 2011). It is thought to play an important
role in protein-protein interactions but its ultimate function is to date still unknown.
In 2011, Watson et al. published new experimental data from a study they completed
on HF patients. They found increased expression of LRG in the coronary sinus (CS)
serum of asymptomatic hypertensive patients. The group further analyzed this
understudied protein by testing its validity against the already recognized biomarker
of HF, B-type natriuretic peptide (BNP). LRG was shown to significantly correlate
with BNP in patients with left ventricular diastolic dysfunction and HF (Fig. 3A). The
levels of LRG were also significantly increased through various stages of the disease
independent of age, sex and renal function (Fig. 3B). Its potential as a novel
biomarker for HF was suggested.
A B
Figure 3A. Correlation of LRG levels with BNP, a recognized biomarker for HF
(Watson et al., 2011). Figure 3B. Increasing levels of LRG with disease progression
(Watson et al., 2011).
!

10
LRG has been shown previously to be involved in chronic inflammatory processes.
Patients suffering from acute appendicitis (Kentsis et al., 2012) and rheumatoid
arthritis (Ha et al., 2014) have shown an upregulation in serum levels of the
glycoprotein and LRG been suggested as a potential biomarker in each case. Shirai et
al., (2009) further demonstrated LRGs induction at a transcriptional level acting as an
acute phase protein when treating HepG2 cells with the pro-inflammatory cytokines
IL6 and TNFα. The same cytokines were also seen to correlate with LRG levels in CS
serum of asymptomatic, hypertensive patients (Watson et al., 2011). Little is known
about the exact function of LRG but these findings propose the idea it is extensively
involved in disease pathways and may be expressed as a protective response by the
body.
1.4 LRG as a Possible Therapeutic An anti-fibrotic role of LRG has been suggested. A member of the Baugh group was
able to show by qPCR, a reduction of ASMA and collagen at a transcriptional level in
cardiac fibroblasts after treatment with LRG-rich media (Tea et al., Unpublished). An
induction of LRG through IL6 and TNF-α in fibroblasts was also seen to inhibit their
differentiation to myofibroblasts by TGF-β (Tea et al., Unpublished). With
statistically significant figures showing negligible mRNA collagen expression in LRG
induced media (fig. 4A), it suggests that the protein may act as a possible anti-fibrotic
agent. After immunohistochemistry (fig. 4B), the expression of LRG was seen within
atrial biopsies of dysfunctional hearts (Watson et al., 2011). Its presence suggests that
it is playing a functional role in the heart.

11
A paper published in Nature by Wang et al. (2013) suggested that LRG plays a role in
the promotion of new blood vessels through TGF-β signaling. LRG was initially
found to be constantly overexpressed in the microvasculature of retinal disease mouse
models (Wang et al., 2013). After proteomic analysis, human vitreous samples were
seen to have increased levels of both LRG and TGF-β (Wang et al., 2013) suggesting
that both molecules have coordinated expression. Previous work has seen active TGF-
β molecule form a tetrameric structure with the type I and type II TGF-β receptors in
endothelial cells (Lim and Zhu, 2006) causing the activation by phosphorylation of
either the ALK1 or ALK5 receptor subunits (Goumans et al., 2003). From the
incubation of LRG in specific conditioned media containing TGF-β, it was found that
the LRG only associates with ALK1 in the presence of the auxiliary protein endoglin.
This relays a signal through the TβRII onto the pro-angiogenic Smad 1/5/8 pathway.
With that said, in the absence of LRG and endoglin, a possible switch occurs with the
ALK5 unit activating the pro-fibrotic Smad 2/3 pathway which potentially drives
Ctrl.
TGF-β
LRG
LRG +
TGF-β
Figure 4A. A significant reduction in Collagen 1 mRNA levels in VHCF after LRG
induction with IL6 and TNF despite treatment with TGF-β (Tea et al., Unpublished).
Figure 4B. Right atrial biopsy from HF patient. Staining in brown shows presence
of LRG within the myocardial tissue (Watson et al., 2011).
A B

12
cardiac fibrosis. The active competition of endoglin and ALK5 for LRG suggests a
dynamic switch in deciding what will be the resulting phenotype in HFpEF. Reduced
endoglin expression has recently been shown to prevent cardiac fibrosis (Kapur et al.,
2012). This furthers the evidence of the imminent need for LRG to be present
allowing for vital vascular growth in disease settings.
A B
!Figure 5A. Signaling profile within a fibroblast through TGF-β, allowing for
expression of ECM proteins. Figure 5B. In the presence of LRG, endothelial cells
favour a pro-angiogenic state (Wang et al., 2013) !

13
1.5 Purpose of this study Given the potential role of LRG in mediating the pro-fibrotic effects of TGF-β it is
likely that LRG may modulate HF disease pathogenesis. To date most work has
studied LRG as a liver-derived serum protein but there is immunohistochemistry
evidence that LRG is expressed within the heart (fig. 4B) (Watson et al., 2011).
The overall hypothesis of this project is that disease-relevant cells within the heart
express LRG.
In order to test this hypothesis the following aims were conducted:
i) Measure LRG expression in human monocytes/macrophages, primary
human and mouse fibroblasts
ii) Assess secretion patterns of LRG in cells supernatant.

14
Chapter 2
Methods and Materials

15
2.1 Materials All reagents used and their respective product codes are outlined in Appendix 1.
2.2 Cell culture Cell lines used:
1. Ventricular Human Cardiac Fibroblasts (VHCF)
2. Murine Primary Cardiac Fibroblasts
3. Human Liver Hepatocellular Carcinoma (HepG2) cells
4. Human Monocytic (THP1) cells
Culturing of cells was carried out to the manufacturer’s specifications. Cultures were
grown in a 37°C humidified incubator containing 5% CO2 and 21% oxygen. Cells
were cultured in conditioned DMEM media containing 10% FCS, 1% L-Glutamine
and 1% Penicillin/Streptomycin. THP1s were cultured in RPMI also containing the
same concentrations of FCS, L-Glutamine and Penicillin/Streptomycin. In a number
of experiments, Serum-starved media was used (media without addition of 10% FCS).
At 65-70% confluency of HepG2 and VHCFs, media was removed from flasks and
washed with PBS. Trypsin-EDTA was then added to the flask and incubated at 37°C.
After cell detachment, the medium was neutralized and centrifuged for 5 minutes at
300Xg. Supernatant were discarded and pellets resuspended in fresh media. A cell
count was completed using a haemocytometer. Cells were then further passaged or
seeded onto a 6 well plate at 250,000 cells/cm3. All culturing took place under
laminar flow.

16
2.3 PBMC isolation A human blood sample was obtained and peripheral Blood-mononuclear cells
(PBMC) were carefully isolated by density centrifugation as described from the
MACS isolation kit (Miltenyi Biotec, Germany) as shown in Fig. 6.
2.4 Treatment of cells Serum-starved and TGF- β treated fibroblasts
VHCFs and murine cardiac fibroblasts were seeded and once confluent, cell were
either serum-starved or treated with a 10ng/µl TGF-β solution. These conditions were
present for 72hrs.
Figure 6: Density gradient of blood components after centrifugation
!!!
Figure 7: Seeding and treatment of VHCF cells !!!

17
THP1 cells response to changeable serum levels THP1 cells were seeded onto a 6 well plate with ~0.4 million cells in each well. Cells
in each well were treated with varying degrees of serum in RPMI medium and left for
72hrs (Table 2).
Effect of PMA on THP1 expression of LRG THP1 cells were seeded onto a 6 well plate with ~0.5 million cells in each well and
maintained in 10% RPMI. Each well was treated with different concentrations of
PMA and exposed for 24hrs (Table 3).
Table 2: Varying degrees of serum concentration in each well
Table 3: Concentration of PMA treatment on THP1 cells

18
Table 4: Final Mastermix (per sample) !
2.5 Quantitative Polymerase Chain Reaction (qPCR) Method The Promega ReliaPrep RNA Cell Kit was used and its protocol was followed for
RNA extraction and purification. BLTG buffer was applied to each well and the
lysate was collected. Isopropanol was added to each sample. These samples were
placed in spin column tubes and treated with RNA Cell kit solutions (RNA wash
solution, a DNase solution and a column wash solution). The RNA lysate was placed
in an eppendorf with 30µl of RNase free H2O and stored at -80°C.
RNA in each sample was quantified using a Nanodrop ND-2000 (Thermo Scientific),
The conversion of RNA to cDNA was carried out following the Invitrogen guidelines.
Briefly, Mastermix solutions and a superscript mix (appendix) were added to the
RNA samples. After a 1:10 dilution with dH2O, the cDNA was stored at -20°C.
To complete the qPCR preparation process, a final mastermix was made. The
following reagents were included:
Final Mastermix solution (Table 4) containing primers for Lrg1 (See appendix) was
added to the cDNA samples. Replicates (n=2) of each sample were carried out. B2M
was used as the housekeeper gene.

19
Table 5: Thermal profile of qPCR !
Table 6: Creation of Polyacrylamide gel for western blot !
The thermal profile (Table 5), the following thermal profile was used to allow for
appropriate amplification and Ct values were obtained from MX 3000p (Stratagene)
After completion, figures were given for each samples cycle threshold derived from
amplification plots. This allowed for fold changes to be formulated.
2.6 Western Blotting Methods Extraction of the protein contents carried out using a 100µl 1X RIPA buffer (see
appendix). Cell lysates were obtained and placed in 0.5ml eppendorfs. The samples
were stored in the -80°C freezer.
Protein samples were quantified using the bicinchoninic acid (BCA) assay kit.
Standards were prepared and diluted accordingly by RIPA PI. Absorbance values
were recorded at 562nm and the Softmax-pro software was used to find the unknown
protein concentrations. The manufacturers protocol was closely followed throughout.
10% polyacrylamide gel was made up using reagents mentioned in Table 6.

20
A loading dye was made from 2X laemmli buffer and BME in a 1:20 dilution and was
added in a 1:1 ratio to eluents of the quantified protein. Samples in their respective
eppendorfs were then exposed to 95oC on a heating block for 5 minutes to allow for
protein denaturation. SeeBlue Protein ladder is a pre-stained standard that was loaded
(10µl) into the first lane of each gel.
The gel was run for 15 minutes at 80mV to allow all the samples to be in a linear
arrangement at the bottom of the stacking layer. Voltage was increased to 120mV and
the samples were seen to take 45/60 minutes to run through the separating layer. A 1X
Running Buffer facilitated the running of the gel in a BioRad Minicell apparatus.
Proteins were transfered onto a Polyvinylidene Fluoride (PVDF) membrane, first
activated in 100% methanol for 30 seconds. A transfer sandwich was prepared (Fig.
8) and then placed in the electroblotting apparatus filled with 1X transfer buffer
containing 10% methanol, kept on ice. This was run at 110mV for 90 minutes.
Figure 8: Membrane sandwich at transfer phase to allow correct transfer
of proteins to PVDF membrane

21
Immediately after the transfer, the PVDF was blocked in 5ml of blocking buffer to
prevent non-specific binding. It was rotated for 60 minutes in a 50ml falcon. Exposure
to the primary antibody was then completed overnight in the 4°C cold room on a
rotator. The PVDF was washed with a TBS-Tween substrate 3X10 minutes after each
exposure to an antibody. The secondary antibody exposure was carried out for 60-90
minutes on the rotator and was followed by another wash step.
The membrane was finally rotated for 5 minutes in HRP substrate. In the dark room,
Fuji Medical X-ray film was placed over the PVDF and was developed to show
specific patterns of banding from the protein of interest.
Preparation for use of PNGase F deglycosylating agent
The PNGase F protocol was used to deglycosylate the protein lysates. Briefly, 1µl of
10X Glycoprotein Denaturing Buffer was added to the protein samples followed by
denatured on a 95oC heating block for 5 minutes. Samples were then centrifuged and
2µl of 10X G7 Reaction Buffer and 2µl of 10% NP-40 were added to the eppendorfs.
1µl of PNGase F was added to each eppendorf, followed by incubation at 37oC for
one hour. Deglycosylated samples were then loaded onto the gel.
Table 7: Functional dilution factors of antibodies !

22
Reprobing the membrane
10ml of a hot stripping buffer containing βME (see appendix) was placed into a
falcon tube with the membrane facing inwards. After 30 minutes incubation at 37°C,
the membrane was again washed in a 3X10 minute TBS-Tween wash. The membrane
was rotated in a GapDH primary antibody followed by a wash step. Goat anti-Mouse
is used as the secondary antibody. GapDH expression was developed on Fuji Medical
film following exposure to HRP substrate.
2.7 Ethical Consideration The blood sample during the isolation of PBMC’s was acquired from an alternative
study, which had been previously approved by the HREC (Human Research Ethics
Committee) within UCD.

23
Chapter 3
Results

24
3.1 Basal LRG expression and production in structural and inflammatory
components
Initial experimentation was to identify whether disease-‐relevant cells within the
heart express LRG. qPCR was the first experimental procedure used to test for
cells mRNA expression. This was followed by western blot. Data on the cells
protein expression was thought to be more reliable and qualitative, and is the
reason why westerns were the major form of experimentation.
3.1.1 LRG mRNA expression in THP1 and VHCF cells (n=1)
To investigate if LRG was present at a transcriptional level, a qPCR was carried out.
HepG2 cells were used as a positive control as LRG mRNA expression has previously
been shown to be abundantly expressed within them (Shirai et al., 2009). VHCFs
made up the structural component due to their known fibrotic action and a monocytic
cell type (THP1) was tested to form the inflammatory component.
Ct values are an expression of how many cycles had to be carried out before a
threshold fluorescent signal was detected. Ct values are inversely proportional to the
quantity of target transcript in the sample. A low Ct means that there is a relatively
high expression of the RNA within the cell. B2M was used as the housekeeper gene.
The fold change was the difference between the housekeeper and the sample of
interest. This shows the variation in expression between the 2 genes. The sub control
values normalises the figures with the actual control and allows for the fold change to
be extrapolated as seen under the heading fold change.

25
Table 8: Basal LRG mRNA expression in VHCF, HepG2s & THP1 cells with Cts, ΔCts
and fold change. B2M used as a housekeeper gene."!!
HepG2 (CTRL) VHCF THP10.00
0.25
0.50
0.75
1.00
LRG Gene mRNA Expression
Rel
ativ
e m
RN
A F
old
Cha
nge
Figure 9: Basal LRG mRNA fold change between HepG2, VHCF and THP1 cells. !
As expected, high expression of LRG was identified in HepG2 cells. Expression was
detectable in THP1 and VHCF cells but much lower than the control sample (fig. 9).
3.1.2 LRG protein production in THP1, VHCF and PBMC cells (n=2). The cell lysates of PBMC, THP1 and VHCF samples were loaded onto a
polyacrylamide gel. HepG2 was also loaded acting as a positive control with its
protein expression of LRG seen previously in the lab (Tea et al., Unpublished). A
serum-starved HepG2 supernatant sample was also loaded. Historically, the lab had
shown an induction of LRG production and secretion after culturing HepG2s in 0%
DMEM medium.

26
LRG was seen to be present in the cell types. The HepG2 control showed 3 variable
bands with a strong signal at ~45kDa (fig. 10). The HepG2 supernatant gave an
extremely strong signal with a concentrated region at ~55kDa. Banding was also seen
at the same weight for PBMC, VHCF and THP1 lysate with the THP1 sample also
having a concentrated LRG expression at ~45kDa.
3.2 LRG expression in treated cardiac fibroblasts
3.2.1 LRG mRNA expression in VHCFs after TGF-β treatment and starvation
(n=1)
qPCR was again the method of preliminary testing for LRG expression in fibroblasts.
Low fold changes were recorded in each VHCF sample when compared against the
positive control. A slight increase in mRNA expression was seen in the serum-starved
sample, but due to the relatively low levels, nothing could be concluded.
Figure 10: Basal LRG protein expression in HepG2 (supernatant and Lysate),
PBMC, VHCF and THP1 cells. GapDH used as the loading control.

27
Table 9: VHCF mRNA expression after treatment with TGF-β and serum
starvation showing Cts, ΔCts and Fold change. B2M used as a housekeeper gene."!!
3.2.2 LRG protein expression and secretion patterns in cardiac fibroblast (n=2)
After VHCFs were treated with TGF-β and/or serum-starved accordingly over a 72-
hour period, their supernatants and lysates were loaded for blotting. HepG2 lysate was
the positive control. Extensive levels of LRG were seen to be present in the non-
treated and TGF-β treated supernatants (fig. 11). Serum-starvation caused cells to
have a noticeably less LRG protein expression in their supernatant. Although levels of
LRG were seen in the lysates of the serum-starved samples. The identification of
variable banding patterns was seen again between supernatants and lysates with
values above and below 50kDa.
Figure 11: Effect of TGF-β and serum starvation (SS) on LRG protein expression and
secretion in VHCF. Cells treated accordingly. Supernatants (sup) and lysates (lys) loaded.
GapDH used as the loading control. Blot is representative of an n=2.

28
A sample of murine cardiac fibroblasts was also run on a gel. Clear levels of LRG
protein expression were seen above and below the 50kDa molecular weight mark (fig.
12). Heavy bands for LRG were observed in the lysates of the non-treated and TGF-β
treated cells. In the absence of serum, banding of the lysates reduced to a size of
~50kDa.
3.3 Expression and secretion patterns of LRG in human monocytes
3.3.1 Effects of serum on LRG protein expression in THP1 cells (n=3)
To examine if monocytes produce and secrete LRG, THP1 cells were treated with
varying concentrations of FCS for 48 hours prior to analysis with western blot (Fig
13). HepG2 supernatant and lysate, again used as the positive control, showed the
variable migration pattern of the suspected LRG protein. LRG was absent from the
GapDH control
37kDa
Figure 12: Effect of TGF-β and serum starvation (SS) on LRG protein expression
in murine primary cardiac fibroblast lysates. GapDH used as loading control. Blot
is representative of an n=2.
!

29
supernatant of the THP1 cells treated with a FCS concentration below 5%. The
antibody gave an extremely strong signal for LRG within each lysate at ~45kDa. The
blotchy appearance of the bands is an unclear indication of protein size or type.
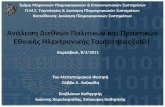
3.3.2 LRG protein expression in macrophage like cells (n=2) After differentiation of THP1 cells to a macrophage like phenotype using the phorbol
ester PMA (fig. 14), LRG protein levels in the lysastes were reduced. Variable
banding patterns can again be seen between supernatants and lysates showing
expression of LRG (fig. 15). . Blotchy patterns were observed for each supernatant
loaded, regardless of what PMA concentration was used. It was suspected that non-
specific binding was occurring or multiple different glycovariants of LRG exist.
Figure 13: Effect of a FCS concentration response on THP1 cells LRG protein
expression and secretion. Cells exposed to varying degrees of serum. Both
supernatants (sup) and lysates (lys) loaded. GapDH used as a loading
control. Blot is representative of an n=3. !

30
Figure 15: Effect of a PMA dose response on THP1 cells showing LRG protein
expression and secretion patterns. Both supernatants (sup) and lysates (lys)
loaded. GapDH used as loading control. Blot is representative of an n=2. !
Figure 14A: THP1 cells in culture before treatment with PMA. They present with
a clear circular morphology in clusters. Figure 14B: THP1 cells differentiation
into a macrophage like phenotype. The cells adhere to the flask and are spindly in
appearance. !
A B

31
3.4 Confirmation of LRG within each supernatant and lysate tested.
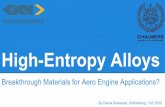
3.4.1 Effect of the deglycosylating agent PNGase F on the LRG glycoprotein
(n=2)
PNGase F, an enzyme that cleaves N-linked glycans, was utilised to determine
whether the varied MW banding patterns in the different samples was due to
glycovariation of LRG or non-specific antibody binding. Treatment of supernatants
and lysates of THP1 and HepG2 cells reduced the detected LRG band size suggesting
that the varied molecular weight was at least in part due to glycosylation (Fig 16). The
LRG bands in enzyme treated lysates were brought down to a banding level MW of
~35kDa and the supernatant bands were decreased to a MW of ~38kDa. The enzyme
treated THP1 supernatant did not completely deglycosylate but a small amount of a
lower MW species of LRG appeared at ~38kDa. Nevertheless the experiment
confirmed the presence of LRG in each cell type tested and that the protein consists of
multiple glycovariants.
Figure 16: Application of the deglycosylating agent PNGase F on HepG2 and THP1
supernatant (sup) and lysates (lys) to identify LRG. GapDH used as a loading
control. Blot is representative of an n=2. !

32
3.4.2 Testing for evidence of non-specific binding to serum in media (n=1) After observing bands previously in media with serum present, there was a suggestion
that the antibody being used was binding non-specifically to a component in FCS. A
sample of neat FCS along with the DMEM and RPMI media were ran on a blot to test
this. A PNGase F treated and non-treated human serum sample was loaded to confirm
the binding capabilities of the Abcam antibody to LRG. The absence of bands seen in
the FCS positive media implied non-specific binding was not occurring (fig. 17). The
presence of LRG was seen as expected within the human serum sample with
successful deglycosylation when treated with PNGase F.
Figure 17:Negative identification of non-specific binding occurring
due to presence of FCS in media. LRG within a human serum sample
successfully deglycosylated by PNGase F. !

33
Chapter 4
Discussion

34
4.1 General Discussion HFpEF is emerging as a major health concern with rapidly increasing prevalence
driven by the ageing population and increased incidence of hypertension, diabetes,
and obesity. Despite this increase in prevalence there is still much to learn about
disease pathogenesis and there is a need for the development of therapeutic and
diagnostic strategies to treat the condition. The present recognized biomarker BNP is
somewhat useful in identifying patients suffering from HF but unfortunately it is
extremely variable between individuals and levels fluctuate depending on patient
characteristics; age, sex and renal function (O'Hanlon et al., 2007). Echocardiography
confirms diagnosis but in most cases, the disease has progressed to a late stage where
considerable remodeling of the myocardium and extensive fibrosis of the interstitium
means that intervention is challenging. There is currently no therapeutics that can
reverse or delay disease progression.
After the identification of LRG’s upregulation in patients suffering from HF and
subsequently showing it to be a stronger diagnostic than BNP (Watson et al., 2011),
its use as a clinical biomarker was suggested. Wang et al., (2013) identified a possible
functional role of LRG through TGF-β signaling in endothelial cells. LRG, in the
presence of endoglin, was seen to cause a switch in Smad signaling from a pro-
fibrotic phenotype to promote neovascularization. This suggested that LRG was
potentially playing a modulatory role and inhibiting the pro-fibrotic response.
Immunostaining within our lab has shown LRG’s presence within cardiac tissue
sections (fig. 4B) (Watson et al., 2011). It is hypothesized that LRG production within
the heart is a protective mechanism that inhibits TGF-β-induced fibroblast activation.

35
The purpose of this study was to identify the specific cells responsible for the
production and secretion of LRG. By determining the cellular sources of the
glycoprotein, a better understanding of its role in a failing heart can be formed.
4.2 LRG expression and secretion patterns in cardiac fibroblasts One of the major hallmarks of HF is chronic fibrosis. The secretion of fibrillar
collagen by TGF-β activated tissue-resident fibroblasts causes ventricular stiffness,
which drives diastolic dysfunction. Given the potential role of LRG in modulating
TGF-β signaling initial experiments were conducted to assess fibroblast expression of
LRG. Low levels of LRG mRNA were detectable by qPCR, with an approximately 50
fold lower expression than in the positive control (HepG2s). Rather than continuing
with PCR, a Western Blot approach was used to determine whether these relatively
low levels of LRG transcript were being translated into detectable protein. Initial
analysis of VHCF lysates revealed a protein band for LRG at ~55kDa. This was a
higher MW than expected, raising concerns as to whether this really was LRG or
perhaps non-specific binding of the antibody. After repeating the experiment and
showing basal “heavy” LRG expression in VHCF cells, a comparison was then made
with other cell supernatants and lysates.
VHCF cells were treated with TGF-β and/or serum-starved. Their differentiation into
activated myofibroblasts, the major cell type causing in ECM deposition, was
achieved by treatment with TGF-β (Fan et al., 2012). Serum-starvation was studied as
it had been previously shown to cause increased LRG protein production in HepG2
cells (Tea et al., Unpublished). An exploratory qPCR was completed on the treated
and non-treated cells. The results again showed relatively low LRG expression in
each cell sample. Serum-starvation did cause an increase in LRG transcription but this
was inconclusive due to lack of repeats and possible technical errors.

36
A western blot of the same experiment was carried out to look at the protein
expression and secretion patterns of the fibroblasts. A considerable level of LRG
protein was seen at ~55kDa in the non-treated and TGF-β treated VHCF supernatants.
This proposes that LRG is being secreted from cardiac fibroblasts in abundance with
the suggestion that the cytokine TGF-β is causing an induction. The lysates only
showed banding for the TGF-β and serum-starved samples. Nothing was detectable
for the non-treated lysate. This seems to infer that is necessary for the secretion of
LRG. Without, LRG is possibly in a native or immature form and cannot be expelled
from the cell.
Murine cardiac fibroblasts were kindly donated within the group and after treatment
and testing, they gave similar results. The non-treated and TGF-β treated lysates
showed strong banding patterns at ~55kDa and serum-starvation causing a reduction
to ~50kDa. The amount of LRG present again seemed to suggest that serum
starvation inhibits the production of LRG. This conclusion is speculative due to the
experiment only an n=2.
Serum is vital for mitotic division of cells but also to supply appropriate nutrients to
allow for their growth and survival (Brunner et al., 2010). When absent, the cells are
unable to multiply efficiently, as observed under a light microscope, thus leading also
to a possible reduction in protein production.
VHCF cells culturing in a 2cm3 well for 72 hours become extremely confluent. Their
dense meshwork may be compared to the remodeling, which occurs in the interstitial
spaces during HF. Speculative evidence suggests that due to their high confluency,
the cells react accordingly by secreting LRG in an attempt to modulate the aggressive

37
proliferation of cells. When fibroblast division is inhibited due to serum starvation it
is perhaps not necessary for the cells to secrete active LRG forms.
4.3 LRG expression and secretion patterns in monocytes/macrophages HFpEF is in 60-80% of cases brought about by a hypertensive insult (Owan and
Redfield, 2005). The body attempts to respond accordingly due to the pressure
overload by initially increasing the number of activated inflammatory cells in the
heart. Previously LRG expression was found to increase early in inflammatory
responses through granulocytic differentiation (O'Donnell et al., 2002). Monocytes in
particular are key of early inflammation through their release of pro-inflammatory
cytokines such as MCP1 and TNF-α (Fernandez-Velasco et al., 2014). Their
differentiation to macrophages once inside the vessel wall is an attempt to resolve the
underlying complication. Unfortunately due to sustained injury, uncontrolled
inflammation is the result with constantly activated macrophage promoting aberrant
tissue remodeling (Glezeva and Baugh, 2014). These cells inherent role during the
pathophysiology of HFpEF means their experimentation for the presence of LRG may
be beneficial.
THP1, a human monocytic cell line was the main cell type tested. Peripberal blood
mononuclear cells (PBMCs), a primary cell type, which includes approximately 30%
monocytes, was another inflammatory subtype briefly tested for basal expression of
LRG. An initial qPCR showed evidence of LRG at the mRNA level in THP1s.
Western blotting of its protein lysate showed a strong banding pattern for LRG at
~45kDa with heavier banding patterns also seen at ~55kDa. The variable banding
patterns seen from the blot suggested possible non-specific binding of the antibody
but with the HepG2 control lysate also showing variable banding patterns,
glycovariants of the protein was speculated. Most interesting to note was the fact that

38
THP1’s seemed to have a larger expression than the HepG2s under visual observation
of the bands. The PBMC lysate seemed to have low LRG protein expression with a
weak band seen again at ~55kDa.
A serum concentration response was next prepared in an attempt to identify if serum
is truly necessary for the production/secretion of heavier LRG forms. This was
confirmed after western blotting of supernatants and lysates with heavy forms of LRG
only present in the 5% and 10% serum treated cells samples at ~55kDa. The absence
of serum from each medium did not inhibit LRG’s intracellular production with large
signals seen in each lysate.
Macrophages are in many respects a dynamic cell type, promoting either a pro-
fibrotic or pro-inflammatory phenotype (Glezeva and Baugh, 2014). The
differentiation of THP1 cells to macrophage was completed through the phorbol ester
PMA at different concentrations. Identification of a visible induction of LRG after
differentiation was postulated but the results returned negative. There was a
noticeable reduction in protein levels after PMA treatment in the lysates. Speculative
evidence suggests that the cells were differentiated into a M2 type macrophage that
are known to promote cardiac repair and mediate pro-fibrotic responses (Fernandez-
Velasco et al., 2014). The supernatants showed some extremely strange banding
patterns in each sample. This may be artifact due to overloading of the wells. It is
possible that there may have been too much protein in each sample retarding the
migration.

39
4.4 Glycosylated variants of LRG It was suggested that the variable banding pattern initially seen between the HepG2
supernatant and lysate was due to extensive glycosylation of the LRG structure. This
suggestion is supported by a previous study, which showed an increase in LRG
glycosylation in pancreatic cancer (Patwa et al., 2006). The secretion patterns of
cardiac fibroblasts and monocytes/macrophage had the same heavy banding
arrangement. There was concern that the Abcam LRG antibody was binding non-
specifically to serum present in the media. An experiment was set up to test this by
using the deglycosylating agent PNGase F in an attempt to reduce the molecular
weight observed previously.
The enzyme was successful in reducing the MW for the suspected LRG glycovariants
in THP1 and HepG2 supernatant and lysates. Suggestive incomplete deglycosylation
occurred for both supernatants reducing to a size of ~37kDa in comparison to the
lysates which was reduced further to ~35kDa. LRG consists of 4 N-linked and 1 O-
linked glycan bonds (Nextprot.org, 2015). PNGase F has the limited ability to cleave
only N-glycans from glycoproteins meaning that the last O-glycan bond possibly
remains in supernatants (as seen in the banding patterns of the supernatants). This
furthers the suggestion that the post-translational modification (PTM) is necessary for
the cells ability to secrete LRG. After 2D-DIGE, differential expression of LRG in
asymptomatic hypertensive patients was seen for the two heaviest spots (Watson et
al., 2011). The presence of this large glycosylated form of LRG proposes the idea that
it has a physiological function in a dysfunctional heart.
The absence of bands for RPMI, DMEM and neat FCS after being loaded onto a blot
confirmed that non-specific binding to the serum was not occurring and this acted as
an appropriate control.

40
4.5 Future direction After observing the protein expression of LRG in both cardiac fibroblasts and THP1
cells, what’s causing its induction needed elucidation. THP1 and PBMC cells
previously treated with various inflammatory products in lysates and their
supernatants were run on a blot (appendix 6). In both cell types, each factor seemed to
cause an induction of intracellular LRG, which offers the idea that LRG is extensively
involved during the inflammatory stage of diastolic dysfunction. LPS and TNF-α
were seen to cause an increase in heavy secreted forms of LRG in THP1 cells. This is
possibly due to their ability to differentiate the monocytes to a M1 type macrophage
(Fernandez-Velasco et al., 2014). Speculation that the heavier form of LRG as the
most functionally active means that the future uses of both factors may be beneficial.
TGF-β also needs to be further tested to elucidate the exact combinatorial signaling
profile that occurs between it and LRG in switching to an anti-fibrotic phenotype.
Attempted optimization of the LRG antibody used by the London group in the Wang
et al,. (2013) study was unsuccessful. No conclusive result was given and it was
thought that an incorrect dilution factor might have been used. Further testing with
this antibody is needed to confirm the true presence of LRG.
After successful identification of what causes the induction and secretion of the heavy
LRG form, its isolation is necessary and then to treat heart tissue sections. If after
treatment, collagen production is inhibited in fibroblasts/myofibroblasts, this will
further add to the existing evidence suggesting that LRG is acting as an anti-fibrotic.
The switch to Smad 1/5/8 signaling can be established in disease relevant cells using a
luciferase reporter vector (Zhang, 2009).

41
4.6 Conclusion The results acquired suggest that LRG production may be stimulated during early
heart dysfunction by a local source within the heart. Acknowledging that LRG is
extensively expressed in liver cells, it seems more plausible that cells elicit their
actions directly at the site of injury. For the first time cardiac fibroblasts were shown
to secrete LRG in abundance from the cell. There is a suggestion that their
differentiation to myofibroblats through TGF-β causes an even larger secretion
pattern but this needs to be tested further and quantified by densitometry.
After establishing that THP1 cells also produce and secrete LRG, it was supposed that
the inflammatory response during HFpEF is vital in preventing a pro-fibrotic
response. Although the macrophage tested did not show an increase in LRG, it is still
hypothesized that these cells are the major component in determining the fate of the
heart.
The dominant finding from this study was the recognition of LRG as being an
extremely glycosylated protein, that’s expression varies depending on its
environment. As already mentioned, future testing on LRG and its variant forms
needs to be completed in order to establish whether the proteins expression is a
protective response during the pathophysiology of HFpEF.
Restricted word count: 5990

42
Acknowledgements I would like to take this opportunity to sincerely thank my Principal investigator, Dr.
John Baugh for his continual support and guidance throughout my project. His
unending patience and good humour meant approaching him about any issue I had
was no problem. I would also like to kindly thank his strong team, including Dr. Chris
Watson, Dr Nadia Glezeva, Adam Russell-Hallinan, James O’Reilly and Roisin
Neary. A special mention to Eugene McNamara for his fantastic supervision and help
throughout my thesis. I gratefully acknowledge the Irish Health Research Board for
their financial support in allowing me to complete my project. I thank the Conway
Institute for allowing me to complete my study within their lab and the use of their
equipment. Kind regards to Dr. Anna Alucino and Dr. Eoin Cummins for their
donation of the THP1 cells. Finally a massive thank you to my family for their
unending love and encouragement throughout my study at UCD. None of this would
have been possible without you.

43
Bibliography

44
ABBATE, A., ARENA, R., ABOUZAKI, N., VAN TASSELL, B. W., CANADA, J., SHAH,
K., BIONDI-‐ZOCCAI, G. & VOELKEL, N. F. 2015. Heart failure with preserved ejection fraction: Refocusing on diastole. Int J Cardiol, 179c, 430-‐440.
BAICU, C. F., ZILE, M. R., AURIGEMMA, G. P. & GAASCH, W. H. 2005. Left ventricular systolic performance, function, and contractility in patients with diastolic heart failure. Circulation, 111, 2306-‐12.
BRUNNER, D., FRANK, J., APPL, H., SCHOFFL, H., PFALLER, W. & GSTRAUNTHALER, G. 2010. Serum-‐free cell culture: the serum-‐free media interactive online database. Altex, 27, 53-‐62.
CHATTERJEE, K. & MASSIE, B. 2007. Systolic and diastolic heart failure: differences and similarities. J Card Fail, 13, 569-‐76.
CHO, D.-‐I., KIM, M. R., JEONG, H.-‐Y., JEONG, H. C., JEONG, M. H., YOON, S. H., KIM, Y. S. & AHN, Y. 2014. Mesenchymal stem cells reciprocally regulate the M1/M2 balance in mouse bone marrow-‐derived macrophages. Experimental & molecular medicine, 46, e70.
FAN, D., TAKAWALE, A., LEE, J. & KASSIRI, Z. 2012. Cardiac fibroblasts, fibrosis and extracellular matrix remodeling in heart disease. Fibrogenesis Tissue Repair, 5, 15.
FERNANDEZ-‐VELASCO, M., GONZALEZ-‐RAMOS, S. & BOSCA, L. 2014. Involvement of monocytes/macrophages as key factors in the development and progression of cardiovascular diseases. Biochem J, 458, 187-‐93.
FIGUEROA, M. S. & PETERS, J. I. 2006. Congestive heart failure: Diagnosis, pathophysiology, therapy, and implications for respiratory care. Respir Care, 51, 403-‐12.
GLEZEVA, N. & BAUGH, J. A. 2014. Role of inflammation in the pathogenesis of heart failure with preserved ejection fraction and its potential as a therapeutic target. Heart Fail Rev, 19, 681-‐94.
GOUMANS, M. J., LEBRIN, F. & VALDIMARSDOTTIR, G. 2003. Controlling the angiogenic switch: a balance between two distinct TGF-‐b receptor signaling pathways. Trends Cardiovasc Med, 13, 301-‐7.
HA, Y. J., KANG, E. J., LEE, S. W., LEE, S. K. & PARK, Y. B. 2014. Usefulness of serum leucine-‐rich alpha-‐2 glycoprotein as a disease activity biomarker in patients with rheumatoid arthritis. 29, 1199-‐204.
HAUPT, H. & BAUDNER, S. 1977. [Isolation and characterization of an unknown, leucine-‐rich 3.1-‐S-‐alpha2-‐glycoprotein from human serum (author's transl)]. Hoppe Seylers Z Physiol Chem, 358, 639-‐46.
HAYDOCK, P. M. & COWIE, M. R. 2010. Heart failure: classification and pathophysiology. Medicine, 38, 467-‐472.
KAPUR, N. K., WILSON, S., YUNIS, A. A., QIAO, X., MACKEY, E., PARUCHURI, V., BAKER, C., ARONOVITZ, M. J., KARUMANCHI, S. A., LETARTE, M., KASS, D. A., MENDELSOHN, M. E. & KARAS, R. H. 2012. Reduced endoglin activity limits cardiac fibrosis and improves survival in heart failure. Circulation, 125, 2728-‐38.
KENTSIS, A., AHMED, S., KUREK, K., BRENNAN, E., BRADWIN, G., STEEN, H. & BACHUR, R. 2012. Detection and diagnostic value of urine leucine-‐rich

45
alpha-‐2-‐glycoprotein in children with suspected acute appendicitis. Ann Emerg Med, 60, 78-‐83.e1.
KRENNING, G., ZEISBERG, E. M. & KALLURI, R. 2010. The Origin of Fibroblasts and Mechanism of Cardiac Fibrosis. Journal of cellular physiology, 225, 631-‐637.
LIM, H. & ZHU, Y. Z. 2006. Role of transforming growth factor-‐beta in the progression of heart failure. Cell Mol Life Sci, 63, 2584-‐96.
MANDINOV, L., EBERLI, F. R., SEILER, C. & HESS, O. M. 2000. Diastolic heart failure.
MCMURRAY, J. J., ADAMOPOULOS, S., ANKER, S. D., AURICCHIO, A., BOHM, M., DICKSTEIN, K., FALK, V., FILIPPATOS, G., FONSECA, C., GOMEZ-‐SANCHEZ, M. A., JAARSMA, T., KOBER, L., LIP, G. Y., MAGGIONI, A. P., PARKHOMENKO, A., PIESKE, B. M., POPESCU, B. A., RONNEVIK, P. K., RUTTEN, F. H., SCHWITTER, J., SEFEROVIC, P., STEPINSKA, J., TRINDADE, P. T., VOORS, A. A., ZANNAD, F., ZEIHER, A., BAX, J. J., BAUMGARTNER, H., CECONI, C., DEAN, V., DEATON, C., FAGARD, R., FUNCK-‐BRENTANO, C., HASDAI, D., HOES, A., KIRCHHOF, P., KNUUTI, J., KOLH, P., MCDONAGH, T., MOULIN, C., POPESCU, B. A., REINER, Z., SECHTEM, U., SIRNES, P. A., TENDERA, M., TORBICKI, A., VAHANIAN, A., WINDECKER, S., MCDONAGH, T., SECHTEM, U., BONET, L. A., AVRAAMIDES, P., BEN LAMIN, H. A., BRIGNOLE, M., COCA, A., COWBURN, P., DARGIE, H., ELLIOTT, P., FLACHSKAMPF, F. A., GUIDA, G. F., HARDMAN, S., IUNG, B., MERKELY, B., MUELLER, C., NANAS, J. N., NIELSEN, O. W., ORN, S., PARISSIS, J. T. & PONIKOWSKI, P. 2012. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail, 14, 803-‐69.
MCMURRAY, J. J. & PFEFFER, M. A. 2005. Heart failure. Lancet, 365, 1877-‐89. NEXTPROT.ORG, (2015). LRG1 - Leucine-rich alpha-2-glycoprotein - human
protein (Proteomics). [online] Available at: http://www.nextprot.org/db/entry/NX_P02750/proteomics [Accessed 2 Feb. 2015]
O'DONNELL, L. C., DRUHAN, L. J. & AVALOS, B. R. 2002. Molecular characterization and expression analysis of leucine-‐rich alpha2-‐glycoprotein, a novel marker of granulocytic differentiation. J Leukoc Biol, 72, 478-‐85.
O'HANLON, R., O'SHEA, P., LEDWIDGE, M., O'LOUGHLIN, C., LANGE, S., CONLON, C., PHELAN, D., CUNNINGHAM, S. & MCDONALD, K. 2007. The biologic variability of B-‐type natriuretic peptide and N-‐terminal pro-‐B-‐type natriuretic peptide in stable heart failure patients. J Card Fail, 13, 50-‐5.
OH, J. K., HATLE, L., TAJIK, A. J. & LITTLE, W. C. 2006. Diastolic heart failure can be diagnosed by comprehensive two-‐dimensional and Doppler echocardiography. J Am Coll Cardiol, 47, 500-‐6.
OWAN, T. E. & REDFIELD, M. M. 2005. Epidemiology of diastolic heart failure. Prog Cardiovasc Dis, 47, 320-‐32.
PATWA, T. H., ZHAO, J., ANDERSON, M. A., SIMEONE, D. M. & LUBMAN, D. M. 2006. Screening of glycosylation patterns in serum using natural glycoprotein microarrays and multi-‐lectin fluorescence detection. Anal Chem, 78, 6411-‐21.
RUDOLPH, A., ABDEL-‐ATY, H., BOHL, S., BOYÉ, P., ZAGROSEK, A., DIETZ, R. & SCHULZ-‐MENGER, J. 2009. Noninvasive Detection of Fibrosis Applying Contrast-‐Enhanced Cardiac Magnetic Resonance in Different Forms of

46
Left Ventricular Hypertrophy: Relation to Remodeling. Journal of the American College of Cardiology, 53, 284-‐291.
SHIRAI, R., HIRANO, F., OHKURA, N., IKEDA, K. & INOUE, S. 2009. Up-‐regulation of the expression of leucine-‐rich α2-‐glycoprotein in hepatocytes by the mediators of acute-‐phase response. Biochemical and Biophysical Research Communications, 382, 776-‐779.
WANG, X., ABRAHAM, S., MCKENZIE, J. A., JEFFS, N., SWIRE, M., TRIPATHI, V. B., LUHMANN, U. F., LANGE, C. A., ZHAI, Z., ARTHUR, H. M., BAINBRIDGE, J. W., MOSS, S. E. & GREENWOOD, J. 2013. LRG1 promotes angiogenesis by modulating endothelial TGF-‐beta signalling. Nature, 499, 306-‐11.
WATSON, C. J., LEDWIDGE, M. T., PHELAN, D., COLLIER, P., BYRNE, J. C., DUNN, M. J., MCDONALD, K. M. & BAUGH, J. A. 2011. Proteomic analysis of coronary sinus serum reveals leucine-‐rich alpha2-‐glycoprotein as a novel biomarker of ventricular dysfunction and heart failure. Circ Heart Fail, 4, 188-‐97.
ZHANG, Y. E. 2009. Non-‐Smad pathways in TGF-‐[beta] signaling. Cell Res, 19, 128-‐139.

47
Appendix

48
Appendix 1 Materials
Material Company Code 10% NP-40 Millipore #B2704S 100% Methanol Sigma-Aldrich #24229-25L-R 10X G7 Reaction Buffer Millipore #B3704S BME EMD millipore #M6250 Bovine Serum Albumin (BSA)
Sigma-Aldrich #BPE9701-100
Chemiluminescent HRP Substrate
NEB #P90720
Dimethyl Sulfoxide (DMSO) Dulbeccos Modified Eagle Medium (DMEM)
Promo Kine #BE12-614F
Foetal Calf Serum (FCS) Relaprep RNA #10270-106 GapDH primary Ab Sigma-Aldrich #MAB374 Glycoprotein Denaturing Buffer
Millipore #B1704S
HRP Substrate SuperSignal West Pico Chemiluminescent Substrate
NEB #WBKL50500
Human Liver Hepatocellular Carcinoma Cells
ATCC #HB-8065
L-Glutamine Santa Cruz Biotechnologies
#25030
Lamelli Buffer Bio-Rad #161-0737 Penicillin/Streptomycin Sigma-Aldrich #1514 Phorbol 12-myristate 13-acetate (PMA)
Fisher Scientific #P8139
Phosphate Buffered Saline (PBS)
Lonza #17-513F
PNGase F NEB #P0704S Polyvinylidine Fluoride (PVDF) Membrane
NEB #IPVH00010
Quantitative polymerase chain reaction (qPCR)
Gibco #Z6012
Random Primers Invitrogen #18064 SeeBlue Plus2 Pre-stained Standard Protein Ladder
Promokine #LC5925
Superscript II Reverse Transcriptase (SIIRT)
Invitrogen #906161
Tetramethylethylenediamine Cell signalling technologies
T9281
THP1 cells Worthington #TIB-202 Transforming Growth Factor β (TGFβ)
Promokine #C-63503
Trypsin Sigma-Aldrich #25200-056 Ventricular Human Cardiac Fibroblasts (VHCFs)
ScienCell HCF-AV #6310
β-2-Mercaptoethanol (βME) Gibco #M6250-100ML

49
Appendix 2 List of Abbreviations
% Percentage °C Degree Celsius ~ Approximately AMPS Ammonium Persulfate ASMA Alpha Smooth Muscle Actin βME Beta-2-Mercaptoethanol B2M Beta-2 microglobulin BSA Bovine Serum Albumin CAD Coronary Artery Disease Ct Cycle Threshold DNA Deoxyribonucleic Acid DHF Diastolic Heart Failure DMEM Dulbeccos Modified Eagle Medium EC Endothelial Cells ECM Extracellular Matrix FCS Foetal Calf Serum GS Glucose Solution GapDH Glyceraldehyde-3-Phosphate Dehydrogenase g Grams G G-force HRP Horseradish Peroxidase HepG2 Human Liver Hepatocellular Carcinoma Interleukin

50
HFpEF Heart Failure with Preserved Ejection Fraction IL Interleukin kDa Kilodaltons LPS Lipopolysaccharide LVDD Left Ventricular Diastolic Dysfunction LRG Leucine rich α2-Glycoprotein MCP Monocyte Chemoattractant Protein mRNA Messenger Ribonucleic Acid MM Mastermix µg Micrograms µl Microlitres ml Millilitres mM Millimolar mV Millivolts M Molar ng Nanograms PBMC Peripheral Blood Mononuclear Cells % Percentage PBS Phosphate Buffered Saline PMA Phorbol 12-myristate 13-acetate PTM Post-‐translational Modification PVDF Polyvinylidine Fluoride qPCR Quantitative Polymerase Reaction RCT Randomised controlled trials RIPA Radioimmunoprecipitation

51
Appendix 3
Reagents Quantity (per sample) Yellow Core Buffer 24µl MnCl2 3µl Dnase I 3µl
DNase solution mix
Reagents Amounts 100ng Random Primers 1µl dNTP mix 1µl RNA Samples 10µl
Mastermix 1 (per sample)
Reagents Amounts First strand buffer 4µl 0.1M DTT 2µl RNase out 1µl
RPMI Roswell Park Memorial Institute Media n Sample Number SDS-PAGE Sodium Dodecyl Sulfate Polyacrylamide Gel
Electrophoresis s Seconds SS Serum Starvation THP1 Human monocytic cell SIIRT Superscript II Reverse Transcriptase SHF Systolic Heart Failure TEMED Tetramethylethylenediamine TGF-β Transforming Growth Factor Beta TBS Tris-Buffered Saline TNF-α Tumor Necrosis Factor Alpha VHCF Ventricular Human Cardiac Fibroblasts 2D-DIGE Two Dimensional Fluorescence Difference Gel
Electrophoresis

52
Mastermix 2 (per sample)
Gene Forward Sequence Reverse Sequence GapDH 5' -‐ ACAGTCAGCCGCATCTTCTT -‐
3' 5' -‐ ACGACCAAATCCGTTGACTC -‐ 3'
LRG1 5' -‐ CAGACAGCGACCAAAAAGC -‐ 3'
5' -‐ AGGTGGTTGACAGGAGATGG -‐ 3'
LRG and GapDH primer sequences Appendix 4
qPCR Amplification Plot
qPCR dissociation curve

53
Appendix 5
Recipies
PAGE Transfer Protein Detection 10X running buffer 20X TBS 1X Stripping Buffer
30.2g of 25mM Tris base 30.3g 0.5M Tris Base in 500ml dH2O 3.78g TrisBase in 500 ml dH2O
188g of 250mM Glycine SDS 0.4% 2.0g pH6.8 10.0g 2.0% SDS pH 2.0 10g of 0.1% SDS Add 72µL of BME 1X running buffer 1X TBS-T (0.1% Tween) Blocking Buffer
900ml dH2O 50ml 20X TBS 950ml dH2O 2.5g of skim milk powder 100ml of 10 x running buffer 1ml Tween 50 ml TBS-tween
500µL of Goat Serum
1X Separating Buffer 10X Transfer Buffer 90.8g of 1.5M Tris Base in 500ml of dH2O 144g of 192mM Glycine 2.0g of 0.4% SDS pH6.8 30g of 24.7mM Tris Base Make up to 1L with dH2O 1X Stacking Buffer 1X Transfer Buffer
30.3g of 0.5M Tris Base in 500ml of dH2O 800 ml dH2O
2.0g of 0.4% SDS pH6.8 100 ml of 10X transfer buffer
100 ml Methanol
1X RIPA Buffer Loading Dye TGF-β (0.5ng/µ l solution) 1:10 dilution of 10X RIPA 950µl of Lamellae Buffer 1µl of TGF-β 1X protease inhibitor cocktail tablet 50µl of β-ME 99µl of 0% DMEM medium

54
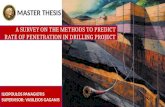
Appendix 6
Supplementary Western Blots
A
B

55