Targeting of nonlipidated, aggregated apoE with antibodies ...

Joanne Donovan, MD, PhDCatabasis Pharmaceuticals, Cambridge, MA
Targeting NF-κB with Edasalonexent for Muscle and Bone Health in Duchenne Muscular Dystrophy

2
Disclosures
This presentation contains forward-looking statements within the meaning of The Private Securities Litigation Reform Act of 1995, including statements regardingour expectations and beliefs about our business, future financial and operating performance, clinical trial plans, product development plans and prospects,including statements about future clinical trial plans including, among other things, statements about our single global Phase 3 PolarisDMD trial in Duchennemuscular dystrophy, or DMD, to evaluate the efficacy and safety of edasalonexent for registration purposes, our plans to continue to evaluate data from the open-label extension of our MoveDMD® clinical trial of edasalonexent for the treatment of DMD, and our plans to combine edasalonexent treatment with other DMDtreatments such as gene therapy and other dystrophin-targeted approaches. The words “believe”, “anticipate”, “plans,” “expect”, “could”, “should”, “will”, “would”,“may”, “intend” and similar expressions are intended to identify forward-looking statements, although not all forward-looking statements contain these identifyingwords.
The forward-looking statements contained in this presentation and in remarks made during this presentation and the following Q&A session are subject toimportant risks and uncertainties that may cause actual events or results to differ materially from our current expectations and beliefs, including: uncertaintiesinherent in the initiation and completion of preclinical studies and clinical trials and clinical development of our product candidates; availability and timing of resultsfrom preclinical studies and clinical trials; whether interim results from a clinical trial will be predictive of the final results of the trial or the results of future trials;expectations for regulatory approvals to conduct trials or to market products, including our expected target product profile for edasalonexent in DMD; availability offunding sufficient for our foreseeable and unforeseeable operating expenses and capital expenditure requirements; other matters that could affect the availabilityor commercial potential of our product candidates; and general economic and market conditions and other factors discussed in the “Risk Factors” section of ourAnnual Report on Form 10-Q for the period ended March 31, 2019, which is on file with the Securities and Exchange Commission, and in other filings that we maymake with the Securities and Exchange Commission in the future. In addition, the forward-looking statements included in this presentation represent our views asof the date of this presentation. We anticipate that subsequent events and developments will cause our views to change. However, while we may elect to updatethese forward-looking statements at some point in the future, we specifically disclaim any obligation to do so. These forward-looking statements should not berelied upon as representing our views as of any date subsequent to the date of this presentation.
Joanne Donovan is an employee of Catabasis Pharmaceuticals, Inc.
Edasalonexent is an investigational agent that is not approved in any territory.

Chen et al., Neurology 2005 65: 826Fiorillo et al., Physiol Genomics 2018 50:735 3
Activation of NF-κB in Muscular Dystrophy Is a Key Factorin Disease Progression in Skeletal and Cardiac Muscle
No Dystrophin + Mechanical Stress
Disease Progression
ActivatedNF-κB
Kumar et al., FASEB J 2003 17:386Akima et al., Neuromuscul Disord 2012 22: 16
Degeneration MuRF1/MAFbx
Control DMD
Cross section of mid-thigh muscle in 12-14 YO boys
Dystrophin and Membrane Stability
b-Dystroglycan
Actin
Dystrophin
MMP-9
miRNA
NF-κB decreases dystrophin production, suggesting inhibition could increase dystrophin with dystrophin-targeted therapies
Inflammation in Infancy
Cytokines
Fibrosis
Inflammation
Regeneration
Satellite Cell
Myoblasts
Myotube
Cyclin D1
MyoD

Edasalonexent Inhibits NF-κB, a Key Driver of Muscle Disease in DMD
‣ Inhibiting NF-κB slows disease progression in animal models of DMD
– Oral administration of edasalonexent or analog (CAT-1041) reduces muscle inflammation and improves function in mdx mice and GRMD dog
‣ Edasalonexent is an orally-administered small molecule that is not a steroid
‣ Being developed for patients with DMD regardless of mutation, both as monotherapy and potentially to be combined with dystrophin-targeted therapies
Decreased Cardiac FibrosisReduced Inflammation in mdx12 month-old GRMD
Untreated CAT-1041
Masson’s Trichrome Staining
Re
lati
ve P
rote
in C
on
ten
t (A
U)
2.5
2
1.5
1
0.5
0OPN IL-6 IL-4
p=0.02
p=0.01
p=0.04
Control
CAT-1041
Increased Diaphragm Specific Force in mdx
Sp
eci
fic
Fo
rce
(N
/cm
2)
10
8
6
4
2
0Control CAT-1041
Control
CAT-1041
p=0.02
Means + SEM
Hammers et al., 2016 JCI Insight
4

5
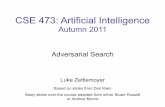
DMD Boys Are Shorter From an Early Age
3 4 5 6 7 8 9
8 0
1 0 0
1 2 0
1 4 0
S te ro id -N a iv e D M D B o y s a r e
C o n s is te n t ly S h o r te r
fo r T h e ir A g e
( 1 0t h
, 5 0t h
, a n d 9 0t h
p e r c e n t i le s )
A g e (y )
He
igh
t (c
m)
D M D (W e s t, e t . a l . )
C D C (2 0 0 0 )
‣ Normal length at birth
‣ Progressive divergence in the difference in stature (compared to healthy controls)
‣ ~5% difference in height from healthy controls
West et al., 2013 J Peds

6
‣ RANK-ligand mediated NF-κB activates osteoclast differentiation and function
– Drives bone loss
‣ NF-κB activation additionally inhibits osteoblast maturation
– Inhibits new bone growth
NF-κB Activity Mediates Inflammation-induced Bone Loss(R
ach
ne
r, e
t. a
l., L
an
cet
20
11
)
(Kru
m, e
t. a
l., N
atu
re R
ev R
heu
m 2
01
0)
Inhibition of NF-κB has the potential to reduce bone loss and enhance new bone growth in patients affected by DMD

7
‣ Inflammatory stimuli that activate NF-κB cause reduced bone lengths
– (in situ fetal mouse metatarsals)
Persistent NF-κB Activation Reduces Bone Length
Landman, et. al., Arthritis Research and Therapy 2013

8
‣ Corticosteroid molecules enhance osteoblast apoptosis and reduce ossification
‣ Steroid-induced increase in RANK-ligand and decrease in Osteoprotegerin leads to enhanced bone resorption and osteoporosis
Corticosteroid Activity Favors Bone Resorption
(Baschant et. al., Nature Rev Rheum 2012)
‣ Clinical consequence is an increased risk of fractures with minimal mechanical stress
(Joseph et. al., JAMA Neurology 2019)

9
Bone Sparing Effect of Edasalonexent in mdx MiceCompared to bone loss seen with prednisolone
‣ No bone metabolism defects in young mdx mice relative to WT (measured by peripheral quantitative CT)
‣ Prednisolone treatment (5mg/kg daily) for ~6 weeks significantly reduced bone length and density
‣ With edasalonexent treatment bone length and density are normal
Femur Length Cortical Density
**** P<0.0001 vs mdx control

10
‣ Long-term low dose corticosteroid is sufficient to induce bone loss and reduced femur lengths
Edasalonexent Maintains Bone Sparing Effect in mdx Mice AfterLong Term Treatment
3-month treatment1 mg/kg Prednisolone
6-month treatment1 mg/kg Prednisolone
Femur Length Cortical Density
W T
c t r l
m d x
c t r l
m d x
e d a s a
m d x
p r e d
0
4
8
1 2
1 6
2 0
F e m u r L e n g th
Fe
mu
r L
en
gth
(m
m)
W T
c t r l
m d x
c t r l
m d x
e d a s a
m d x
p r e d
0
4
8
1 2
1 6
2 0
F e m u r L e n g th
Fe
mu
r L
en
gth
(m
m)
N S
N S
* * *
W T
c t r l
m d x
c t r l
m d x
e d a s a
m d x
p r e d
0 .0
0 .4
0 .8
1 .2
C o rtic a l D e n s ity
Co
rti
ca
l D
en
sit
y (
mg
/mm
2)
N S
N S
* * * *
W T
c t r l
m d x
c t r l
m d x
e d a s a
m d x
p r e d
0 .0
0 .4
0 .8
1 .2
C o rtic a l D e n s ity
Co
rti
ca
l D
en
sit
y (
mg
/mm
2)
****p<0.0001, ***p<0.005

‣ Study Objectives
– Proof of concept using MRI to assess changes in muscle health
– Long-term study to enable Phase 3
‣ Key Inclusion / Exclusion criteria
– Age 4 to 8th birthday not on corticosteroids for at least 24 weeks
Design of MoveDMD, a Phase 2 Trial with Open-Label Extension
Phase 1n=17
Off-Treatment Periodn=16
Phase 2n=31
Open-Label Extensionn=31
‣ Analysis Plan
– 12-week placebo control period
– Compare changes during off-treatment control period with changes after initiation of edasalonexent
1 week ~6 months prior to Phase 2 12-week placebo-controlled period
>72 weeks
11

12
Range of Endpoints to Demonstrate Proof of Concept and Support Design of Phase 3
NF-κB Target Engagement Biomarkers Muscle MRI Functional
▸ Inhibition of
NF-κB targeted
gene set in
peripheral blood
▸ CRP, biomarker of
inflammation
▸Muscle enzymes
▸MRI T2 of upper
and lower leg
▸MRS muscle fat
▸North Star
Ambulatory
Assessment and
Timed Function
Tests

13
‣ Declines in function in natural history study were similar to those observed in the MoveDMD trial off-treatment
‣ Decreases in function correlate with increases in composite lower leg MRI T2 as well as muscle fat fraction
Steroid-Naïve Boys in Age Range 4 to 8th Birthday Are Declining in Function and Progressing on MRI
Functional Decline in Boys Not Receiving Steroids or Edasalonexent
MRI Shows Disease Progression
Finkel et al., World Muscle Society, 2018; Vandenbourne et al., World Muscle Society, 2018
An
nu
alize
d R
ate
of
Ch
an
ge
(m
s/ye
ar)
6
4
2
An
nu
alize
d R
ate
of
Ch
an
ge
(%
/ye
ar)
4
3
2
1
An
nu
alize
d R
ate
of
Ch
an
ge
(%
/ye
ar)
20
15
10
5
Lower Leg Composite MRI T2 Soleus Fat Fraction VL Fat Fraction
An
nu
alize
d R
ate
of
Ch
an
ge
(ta
sks/
s/ye
ar)
0.00
-0.05
-0.10
-0.15
10-meter walk/run 4-stair climb Time to stand
Natural History: ImagingDMD Prior to treatment: MoveDMD
Means + SEM

14
‣ Composite of 5 lower leg muscles MRI T2 used to encompass muscles at various stages of disease progression and minimize variability
‣ Following 72 weeks of edasalonexent, the rate of increase in the composite MRI T2 in the five lower leg muscles decreased as compared to the rate of increase during the off-treatment control period
In Phase 2 MoveDMD Trial and Open-Label Extension:
Edasalonexent Improved Rate of Change of MRI T2 Compared to Off-Treatment Control Period
MRI T2: Composite of 5 Lower Leg Muscles
Weeks on Edasalonexent
12 483624
* **
*
Edasalonexent
100 mg/kg
Off-treatment control
*
72
Better
An
nu
alize
d R
ate
of
Ch
an
ge
(m
se
c/ye
ar)
6
4
2
0
-4
Means + SEM; mixed model comparison with off-treatment period * Week 12: p=0.002, n=16; Week 24: p=0.004, n=14; Week 36: p=0.032, n=13; Week 48: p=0.018, n=12; Week 72: p=0.052, n=9

15
In Phase 2 MoveDMD Trial and Open-Label Extension:
All Assessments of Function Stabilized on Edasalonexent Compared to Off-Treatment Control
North Star Ambulatory Assessment
NS
AA
Sco
re
25
20
15
10
5
-36 -24 -12 0 12 24 36 48 60 72
Edasalonexent
100 mg/kg
Control Period
Sp
ee
d (
1/S
eco
nd
s)
0.4Edasalonexent
0.3
0.2
0-36 -24 -12 0 12 24 36 48 60
100 mg/kg
Control Period
0.1
4-Stair Climb
72
Tim
e (S
eco
nd
s)
5
1015
10-Meter Walk/Run
Sp
ee
d (
1/S
eco
nd
s) Tim
e (S
eco
nd
s)
0.20
0.18
0.16
0.14
0.12
5
10-36 -24 -12 0 12 24 36 48 60 72
Edasalonexent
100 mg/kg
Control Period
Better
Weeks
WeeksWeeks
Time to Stand
Sp
ee
d (
1/S
eco
nd
s)
Tim
e (S
eco
nd
s)
0.3
-36 -24 -12 0 12 24 36 48 60 72
Edasalonexent
100 mg/kg
0
0.2
0.1
5
10
Control Period
15
Weeks
Means ± SEM shown. Includes data of all boys initially started on 100 mg/kg dose (n=16) with 11 boys participating through 72 weeks.

16
In Phase 2 MoveDMD Trial and Open-Label Extension:
Muscle Enzymes Significantly Decreased on Edasalonexent, Supporting a Positive Drug Effect
Weeks on 100 mg/kg Edasalonexent
IU/m
L
0
-5000
-10000
-15000
-20000
-25000
IU/m
L
0
-50
-100
-150
-200
Alanine Aminotransferase
12 36 724824 60
IU/m
L
0
-50
-100
-150
-200
-250
Aspartate Aminotransferase
12 36 724824 60
IU/m
L
0
-200
-400
-600
-800
Lactate Dehydrogenase
12 36 724824 60
Creatine Kinase
*
12 36 724824 60
*
* *
Plasma muscle enzymes are elevated 10 to 100 fold in DMD, indicative of leakage from damaged myocytes
Means ± SEM shown; * p<0.05 for mean change from baseline after 12 weeks

17
In Phase 2 MoveDMD Trial and Open-Label Extension:
Edasalonexent Showed Potential for Cardiac Benefits in DMDB
ea
ts p
er
min
ute
0
-5
-10
-15
Heart Rate: Change from Baseline
0 20 40
Weeks on Edasalonexent
8060
* p<0.01
Thomas, et al. Pediatr Cardiol. 2012 33(7):1175-9.Hammers, et al. JCI Insight 2016 1(21): e90341Fleming, et al., Lancet 2011 377: 1011-18Means ± SEM shown;
Baseline99 beats/min
‣ Elevated resting heart rate is initial manifestation of cardiac disease in DMD
– Cardiac failure is a leading cause of mortality in DMD
– Elevated heart rate triples the risk of cardiomyopathy several years later
‣ Edasalonexent analog had positive effects on fibrosis in mdx and GRMD models
– Edasalonexent tissue levels in heart > skeletal muscle
‣ In MoveDMD trial, mean resting heart rate significantly decreased, approaching age-normative heart rate ~92 beats per minute

100
75
50
25
0
18
‣ 50+ patient years of exposure
‣ Well tolerated, with majority of adverse events mild in nature
– Most common related adverse event was diarrhea, which did not require discontinuation
– No adverse trends in chemistry, hematology, or measures of adrenal function (cortisol and ACTH)
‣ Boys on edasalonexent grew 2.1 inches/ year, similar to unaffected boys
In Phase 2 MoveDMD Trial and Open-Label Extension:
Safety: Growth Continues as Expected
Percentiles Compared to CDC Growth Charts
BMI 100
75
50
25
0
Weight 100
75
50
25
0
Height
Pe
rce
nti
le
Weeks on Edasalonexent
Means ± SEM shown
0 12 24 36 48 60 72 0 12 24 36 48 60 720 12 24 36 48 60 72

‣ Preclinical data support potential for NF-κB inhibition to support bone health in DMD
‣ In Phase 2 MoveDMD trial and open-label extension, edasalonexent, an oral NF-κB inhibitor, showed:
– MRI measures supportive of positive edasalonexent treatment effects
– Muscle MRI T2 rate of change improved with edasalonexent treatment versus off-treatment control period progression
– Well-tolerated with growth along expected growth curves
– Clinically meaningful slowing of disease progression on edasalonexent compared to off-treatment control period
– North Star Ambulatory Assessment and all timed function tests stabilized
‣ Preclinical and clinical data support design of Phase 3 registration trial
19
Targeting NF-κB with Edasalonexent Has Potential for Benefit of Skeletal and Cardiac Muscle as well as Supporting Growth and Bone Health in DMD

20
– Enrolling approximately 125 4-to-<8 year-old boys not on steroids for 6 months
– Primary endpoint: NSAA
– Secondary endpoints: age-appropriate timed functional tests
‣ Bone-related measures:
– Standardized lumbosacral spine films to assess for fractures
– DXA: bone density and body composition
‣ Top-line results anticipated in second half of 2020
Phase 3 Polaris Clinical Trial Currently Ongoing
12-month, randomized, double-blind placebo-controlled trial
Open-label extension
Edasalonexent
Primary Endpoint
Placebo
Edasalonexent 100 mg/kg

21
Acknowledgements
‣ Patients and families
‣ Patient groups
‣ Nemours Children’s Hospital
– Richard Finkel, MD
‣ ImagingDMD & University of Florida
– Krista Vandenborne, PT PhD
– H. Lee Sweeney, PhD
– Rebecca J. Willcocks, PhD
– Glenn Walter, PhD
– Sean C. Forbes, PhD
– William T. Triplett, BSc
‣ Oregon Health Sciences University
– Erika L. Finanger, MD
– William Rooney, PhD
‣ The Children’s Hospital of Philadelphia
– Gihan I. Tennekoon, MD
– Sabrina W. Yum, MD
‣ University of California
– Perry Shieh, MD PhD
‣ Catabasis Pharmaceuticals
– Maria Mancini, MHP
– Angelika Fretzen, PhD
– Pradeep Bista, PhD
– Andrew Nichols, PhD
– James MacDougall, PhD