Su1788 Iatrogenic Splenic Lesions in Surgery of Colorectal Cancer -Impact Onto the Early...
1
SSAT Abstracts * Chi-square test. † Univariate cox regression anaylsis. ‡ number of patients when incomplete data available. ϕ Median value (interquartile range) given. ω Non-parametric test. mGPS - modified Glasgow Prognostic Score. NLR - neutrophil:lymphocyte ratio Figure 1. The relationship between modified Glasgow Prognostic Score, mismatch repair status and cancer-specific survival in patients undergoing elective, curative colorectal can- cer resection Su1786 Laparoscopic Ventral Mesh Rectopexy Compared to Stapled Trans-Anal Rectal Resection (STARR) to Treat Internal Rectal Prolapse: A Matched Cohorts Study Pierpaolo Sileri, Luana Franceschilli, Federica Giorgi, Ilaria Capuano, Achille Gaspari Background: Laparoscopic Ventral Mesh Rectopexy (LVR) corrects both, internal and external rectal prolapse, improving obstructed defaecation symptoms (ODS) and faecal incontinence. Similarly, Stapled Trans-Anal Rectal Resection (STARR) allows resolution of ODS. However data from retrospective series or prospective trials comparing the two procedures for internal rectal prolapse (IRP, defined as recto-rectal or recto-anal intussusception) are absent. In this matched cohorts study we compared outcomes in terms of surgical complications and functional results of LVR and STARR in order to better understand the ideal surgical approach for IRP. Patients and Methods: All patients underwent preoperative evaluation with defaecating proctography or pelvic dynamic MRI. Only patients with recto-rectal or recto-anal intussusception, rectocoele with or without enterocoele or sigmoidocoele were considered from our prospectively kept database. Patients with concomitant middle and anterior pelvic compartment prolapses, were excluded. Two groups of patients were consid- ered according to the surgical technique (LVR or STARR) and matched for demographics, symptoms and characteristics of the prolapse. Only patients with a minimum of 1 year follow-up were considerd. End-points were surgical complications and functional results expressed as Wexner Constipation Score (WCS) and Faecal Incontinence Severity Index (FISI). Results: Twenty-seven patients who underwent LVR were compared to 27 patients who underwent STARR. After LVR, overall complications rate was 15% similar to STARR (11%), all minor. After LVR, WCS significantly improved to 5+/-3 from preoperative 15+/- 5 (p 0.03). Constipation improved in 89% and was cured in 81%. Similarly, after STARR, WCS score significantly improved to 6+/-5 from preoperative 16+/-11(p 0.03). Recurrence rate was 22%. Constipation improved in 85% and was cured in 78%. No significative differences were observed between the two groups. Considering incontinence, after LVR the FISI score significantly improved to 2+/-2 from preoperative 7+/-3 (p 0.03). Incontinence improved in 90% and was completely cured in 90%. After STARR, the FISI score improved to 4+/-2 from preoperative 8+/-5(p 0.06). Incontinence improved in 54% and was completely cured in 45%. These percentages were significantly lower compared to those observed after LVR. Conclusions: LVR and STARR seems to be equally valid to treat constipation associated to IRP, but LVR has greater chances to cure incontinence. Su1787 Lubiprostone (Amitiza) Activates Cellular Prostanoid Signaling to Enhance Intestinal Motility in Human Colon Jinping Gao, Zhongxian Hu, Yuxin Zhang, Yingxiu Cheng, Pengchao Zheng, Xiyu Wang, Guodu Wang Background and Aims: Lubiprostone as a prostaglandin E derivative can activate chloride channels in bowel epithelia to stimulate intestinal secretion. It is widely applied for the treatment of adult chronic idiopathic constipation and irritable bowel syndrome with consti- pation in adult women. Clinic therapies of lubiprostone showed it can induce some side effects, such as nausea, diarrhea, abdominal pain and bloating and dyspnea. The study aims to investigate mechanism of the side effects in human colonic motility. Methods: Immunoflorescence staining with EP receptor antibodies was performed in the cryostat- sections of human colon. Colonic motility and pharmacological examinations were analyzed S-1036 SSAT Abstracts with organ bath system and human colonic longitudinal and circular axe muscle strips (LAMSs and CAMSs that obtained from colonic and rectum surgical operations of the patients. Results: Immunostaining showed that 325 of 598 submucosal and 471 of 633 myenteric neurons and their nerve fibers are immunoreactive for Anti-Hu and EP4 receptor. EP4 receptor immunopostive neurons co-expressed choline acetyransferase (ChAT) and substance P in myenteric plexus. Bath application of lubiprostone increased the amplitude of spontaneous contractile activity and lift baseline tension in dose-dependent manner in 17of 24 LAMSs from 5 male and 7 female patients. This action was suppressed by pre- treatment with 10μM SC19220, an EP1 antagonist. Electrical field stimulation (EFS) evoked contracting amplitudes of LAMSs were enhanced by lubiprostone in dose-dependent manner in 21of 24 LAMSs. The EFS-evoked responses were suppressed by preincubation with 10μM L161980, an EP4 antagonist, but not by the SC19220. These EFS-evoked responses also were inhibited by pre-application of 2 μM cAMPS-Rp, a cAMP antagonist, and abolished by 1μM tetrodotoxin (TTX). Pretreatment with atropine (10μM), the neurokinin 1 antagonist, CP96345 (10μM), or the neurokinin 2 antagonist, GR159897 (20μM), suppressed enhance- ment effect of lubiprostone on EFS-evoked contractions. PGE2 (30nM-1μM) mimicked the actions of lubiprostone in the LAMSs. Application of lubiprostone did not alter the sponta- neous or EFS-evoked contractile activity of 28 colonic CAMSs from 8 male and 6 female patients. Conclusion: Lubiprostone can activate cellular prostanoid-cAMP signaling to enhance myogenic motility via EP1 receptor and neurogenic contracting responses via EP4 receptor in the human colon. The result suggested that side effects of lubiprostone may originate from its activating actions in EP receptors of enteric neurons and smooth muscles. Selective EP1 and EP4 antagonists may prevent the side effects of lubiprostone in clinic treat- ments. Su1788 Iatrogenic Splenic Lesions in Surgery of Colorectal Cancer - Impact Onto the Early Postoperative and Oncological Long-Term Result Ralf Steinert, Ingo Gastinger, Henry Ptok, Meyer Frank, Andreas Koch, Ronny Otto, Hans Lippert Consequences of splenectomy in surgery for colorectal cancer(Ca) have not sufficiently investigated yet since (under normal circumstances) it is not substantial part for extended radicalness. Therefore, it appears to be of great interest what the early postoperative & oncosurgical long-term outcome of iatrogenic lesions of the spleen followed by splenectomy or reconstruction (if possible) during surgery of colorectal Ca is. Methods: From 01/01/ 2000-12/31/2004, data obtained from 45,265 patients with colorectal Ca in a prospective multicenter observational study who had undergone tumor resection with curative or pal¬lia- tive intention were analyzed with regard to early postoperative (surgical) results & survival rates affected by iatrogenic splenic lesions. Results: In 638 patients (1.4%), iatrogenic splenic lesion occurred. In more than 80% of cases, spleen was injured in surgery of Ca of the left hemicolon & rectum. Logistic regression indicated that the crucial risk factor for this lesion was mobilization of the left colonic flexure. 126 patients (0.3%) underwent splenectomy whereas in 512 cases, spleen could be preserved. Morbidity was significantly lower without (36.0%) vs. with splenectomy (47.6%) or preservation of the spleen (48.6%), respectively. Rate of anastomotic insufficiency with need for surgical re-intervention was the highest in splenectomized patients (7.9%) whereas this rate was significantly lower in cases with splenic lesion but possible preservation of the organ (3.3%; p=0.003). Considering the overall hospital lethality of 3.1%, the specific lethality for splenectomy cases was significantly increased (11.9% / preservation of the spleen, 4.7%; p<0.0001 - no splenic lesion, 3.0%). 565 subjects agreed to register follow-up data; in 564 cases with iatrogenic splenic lesion, these data were investigated resulting in a follow-up rate of 99.8% (median follow-up period, 50.2 months). The median overall 5-year survival was 4.8 years (group I, splenic lesion with splenectomy) but it was significantly longer (8 years) in group II (preservation of the spleen), p=0.009, & there was no difference between group II & III (control with no splenic lesion). Multivariate Cox regression analysis elucidated that iatrogenic splenic lesion with splenectomy can be considered an independent risk factor for a worse oncosurgical outcome. Conclusions: Iatrogenic lesion of the spleen requiring splenectomy in colorectal Ca surgery is a significant risk fac¬tor for a worse early postoperative surgical result (higher morbidity, lethality, rate of anastomotic insufficiency) & long-term survival, in particular, comparing the group of splenectomized patients to those with organ preservation in splenic lesion. However, according to the results, spleen-preservation should be always attempted to avoid disadvantageous effect onto the outcome. Su1789 Effect of Delay in Surgical Treatment of Colon Cancer on Survival Farid Jalali, Argyrios Ziogas, Jason A. Zell, Michael J. Stamos, Hoda Anton-Culver, William E. Karnes Background: There has been minimal research on the impact of delay in definitive surgical treatment of colon cancer on patient outcomes. We investigated the time intervals between the diagnosis and the definitive surgical treatment of colon cancer, factors associated with delay, and the effect of delay on survival. Methods: We used the California Cancer Registry database to identify patients 40 years or older who were diagnosed with colon cancer from 1996 to 2005 and underwent colon cancer surgery. Stage IV colon cancers were excluded to focus the analysis on outcomes for surgical treatments with curative intent. Emergent and urgent cases, defined as having time between diagnosis to surgery interval ≤ 1 day and 2-7 days, respectively, were excluded to assess outcomes of elective cases. Cox proportional hazards model was used to investigate the impact of treatment delay time (TDT), defined as time interval between the diagnosis and the definitive surgical treatment, on five-year overall and disease-specific survival. Covariates adjusted for in multivariate analysis were cancer stage, right vs. left-sided cancer, age, gender, race, socioeconomic status (SES), insurance status, and marital status. Results: A total of 24,351 patients matched the inclusion criteria. Treatment delay time of 6 to 12 weeks (12.8% of cases) was associated with 26% increased risk of overall mortality (HR 1.26, p<0.0001, CI 1.18-1.36) and 14% increased risk of mortality due to colon cancer (HR 1.14, p=0.0259, CI 1.02-1.29) when compared to patients with TDT < 6 weeks. Survival was even worse with TDT ≥ 12 weeks (2.7% of
Transcript of Su1788 Iatrogenic Splenic Lesions in Surgery of Colorectal Cancer -Impact Onto the Early...

SS
AT
Ab
stra
cts
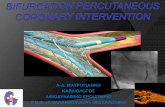
* Chi-square test. † Univariate cox regression anaylsis. ‡number of patients when incompletedata available. ϕ Median value (interquartile range) given. ω Non-parametric test. mGPS -modified Glasgow Prognostic Score. NLR - neutrophil:lymphocyte ratio
Figure 1. The relationship between modified Glasgow Prognostic Score, mismatch repairstatus and cancer-specific survival in patients undergoing elective, curative colorectal can-cer resection
Su1786
Laparoscopic Ventral Mesh Rectopexy Compared to Stapled Trans-Anal RectalResection (STARR) to Treat Internal Rectal Prolapse: A Matched CohortsStudyPierpaolo Sileri, Luana Franceschilli, Federica Giorgi, Ilaria Capuano, Achille Gaspari
Background: Laparoscopic Ventral Mesh Rectopexy (LVR) corrects both, internal and externalrectal prolapse, improving obstructed defaecation symptoms (ODS) and faecal incontinence.Similarly, Stapled Trans-Anal Rectal Resection (STARR) allows resolution of ODS. Howeverdata from retrospective series or prospective trials comparing the two procedures for internalrectal prolapse (IRP, defined as recto-rectal or recto-anal intussusception) are absent. In thismatched cohorts study we compared outcomes in terms of surgical complications andfunctional results of LVR and STARR in order to better understand the ideal surgicalapproach for IRP. Patients and Methods: All patients underwent preoperative evaluationwith defaecating proctography or pelvic dynamic MRI. Only patients with recto-rectal orrecto-anal intussusception, rectocoele with or without enterocoele or sigmoidocoele wereconsidered from our prospectively kept database. Patients with concomitant middle andanterior pelvic compartment prolapses, were excluded. Two groups of patients were consid-ered according to the surgical technique (LVR or STARR) and matched for demographics,symptoms and characteristics of the prolapse. Only patients with a minimum of 1 yearfollow-up were considerd. End-points were surgical complications and functional resultsexpressed as Wexner Constipation Score (WCS) and Faecal Incontinence Severity Index(FISI). Results: Twenty-seven patients who underwent LVR were compared to 27 patientswho underwent STARR. After LVR, overall complications rate was 15% similar to STARR(11%), all minor. After LVR, WCS significantly improved to 5+/-3 from preoperative 15+/-5 (p 0.03). Constipation improved in 89% and was cured in 81%. Similarly, after STARR,WCS score significantly improved to 6+/-5 from preoperative 16+/-11(p 0.03). Recurrencerate was 22%. Constipation improved in 85% and was cured in 78%. No significativedifferences were observed between the two groups. Considering incontinence, after LVR theFISI score significantly improved to 2+/-2 from preoperative 7+/-3 (p 0.03). Incontinenceimproved in 90% and was completely cured in 90%. After STARR, the FISI score improvedto 4+/-2 from preoperative 8+/-5(p 0.06). Incontinence improved in 54% and was completelycured in 45%. These percentages were significantly lower compared to those observed afterLVR. Conclusions: LVR and STARR seems to be equally valid to treat constipation associatedto IRP, but LVR has greater chances to cure incontinence.
Su1787
Lubiprostone (Amitiza) Activates Cellular Prostanoid Signaling to EnhanceIntestinal Motility in Human ColonJinping Gao, Zhongxian Hu, Yuxin Zhang, Yingxiu Cheng, Pengchao Zheng, Xiyu Wang,Guodu Wang
Background and Aims: Lubiprostone as a prostaglandin E derivative can activate chloridechannels in bowel epithelia to stimulate intestinal secretion. It is widely applied for thetreatment of adult chronic idiopathic constipation and irritable bowel syndrome with consti-pation in adult women. Clinic therapies of lubiprostone showed it can induce some sideeffects, such as nausea, diarrhea, abdominal pain and bloating and dyspnea. The studyaims to investigate mechanism of the side effects in human colonic motility. Methods:Immunoflorescence staining with EP receptor antibodies was performed in the cryostat-sections of human colon. Colonic motility and pharmacological examinations were analyzed
S-1036SSAT Abstracts
with organ bath system and human colonic longitudinal and circular axe muscle strips(LAMSs and CAMSs that obtained from colonic and rectum surgical operations of thepatients. Results: Immunostaining showed that 325 of 598 submucosal and 471 of 633myenteric neurons and their nerve fibers are immunoreactive for Anti-Hu and EP4 receptor.EP4 receptor immunopostive neurons co-expressed choline acetyransferase (ChAT) andsubstance P in myenteric plexus. Bath application of lubiprostone increased the amplitudeof spontaneous contractile activity and lift baseline tension in dose-dependent manner in17of 24 LAMSs from 5 male and 7 female patients. This action was suppressed by pre-treatment with 10μM SC19220, an EP1 antagonist. Electrical field stimulation (EFS) evokedcontracting amplitudes of LAMSs were enhanced by lubiprostone in dose-dependent mannerin 21of 24 LAMSs. The EFS-evoked responses were suppressed by preincubation with 10μML161980, an EP4 antagonist, but not by the SC19220. These EFS-evoked responses alsowere inhibited by pre-application of 2 μM cAMPS-Rp, a cAMP antagonist, and abolishedby 1μM tetrodotoxin (TTX). Pretreatment with atropine (10μM), the neurokinin 1 antagonist,CP96345 (10μM), or the neurokinin 2 antagonist, GR159897 (20μM), suppressed enhance-ment effect of lubiprostone on EFS-evoked contractions. PGE2 (30nM-1μM) mimicked theactions of lubiprostone in the LAMSs. Application of lubiprostone did not alter the sponta-neous or EFS-evoked contractile activity of 28 colonic CAMSs from 8 male and 6 femalepatients. Conclusion: Lubiprostone can activate cellular prostanoid-cAMP signaling toenhance myogenic motility via EP1 receptor and neurogenic contracting responses via EP4receptor in the human colon. The result suggested that side effects of lubiprostone mayoriginate from its activating actions in EP receptors of enteric neurons and smooth muscles.Selective EP1 and EP4 antagonists may prevent the side effects of lubiprostone in clinic treat-ments.
Su1788
Iatrogenic Splenic Lesions in Surgery of Colorectal Cancer - Impact Onto theEarly Postoperative and Oncological Long-Term ResultRalf Steinert, Ingo Gastinger, Henry Ptok, Meyer Frank, Andreas Koch, Ronny Otto, HansLippert
Consequences of splenectomy in surgery for colorectal cancer(Ca) have not sufficientlyinvestigated yet since (under normal circumstances) it is not substantial part for extendedradicalness. Therefore, it appears to be of great interest what the early postoperative &oncosurgical long-term outcome of iatrogenic lesions of the spleen followed by splenectomyor reconstruction (if possible) during surgery of colorectal Ca is. Methods: From 01/01/2000-12/31/2004, data obtained from 45,265 patients with colorectal Ca in a prospectivemulticenter observational study who had undergone tumor resection with curative or pal¬lia-tive intention were analyzed with regard to early postoperative (surgical) results & survivalrates affected by iatrogenic splenic lesions. Results: In 638 patients (1.4%), iatrogenic spleniclesion occurred. In more than 80% of cases, spleen was injured in surgery of Ca of the lefthemicolon & rectum. Logistic regression indicated that the crucial risk factor for this lesionwas mobilization of the left colonic flexure. 126 patients (0.3%) underwent splenectomywhereas in 512 cases, spleen could be preserved. Morbidity was significantly lower without(36.0%) vs. with splenectomy (47.6%) or preservation of the spleen (48.6%), respectively.Rate of anastomotic insufficiency with need for surgical re-intervention was the highest insplenectomized patients (7.9%) whereas this rate was significantly lower in cases with spleniclesion but possible preservation of the organ (3.3%; p=0.003). Considering the overallhospital lethality of 3.1%, the specific lethality for splenectomy cases was significantlyincreased (11.9% / preservation of the spleen, 4.7%; p<0.0001 - no splenic lesion, 3.0%).565 subjects agreed to register follow-up data; in 564 cases with iatrogenic splenic lesion,these data were investigated resulting in a follow-up rate of 99.8% (median follow-up period,50.2 months). The median overall 5-year survival was 4.8 years (group I, splenic lesionwith splenectomy) but it was significantly longer (8 years) in group II (preservation of thespleen), p=0.009, & there was no difference between group II & III (control with no spleniclesion). Multivariate Cox regression analysis elucidated that iatrogenic splenic lesion withsplenectomy can be considered an independent risk factor for a worse oncosurgical outcome.Conclusions: Iatrogenic lesion of the spleen requiring splenectomy in colorectal Ca surgeryis a significant risk fac¬tor for a worse early postoperative surgical result (higher morbidity,lethality, rate of anastomotic insufficiency) & long-term survival, in particular, comparingthe group of splenectomized patients to those with organ preservation in splenic lesion.However, according to the results, spleen-preservation should be always attempted to avoiddisadvantageous effect onto the outcome.
Su1789
Effect of Delay in Surgical Treatment of Colon Cancer on SurvivalFarid Jalali, Argyrios Ziogas, Jason A. Zell, Michael J. Stamos, Hoda Anton-Culver,William E. Karnes
Background: There has been minimal research on the impact of delay in definitive surgicaltreatment of colon cancer on patient outcomes. We investigated the time intervals betweenthe diagnosis and the definitive surgical treatment of colon cancer, factors associated withdelay, and the effect of delay on survival. Methods: We used the California Cancer Registrydatabase to identify patients 40 years or older who were diagnosed with colon cancer from1996 to 2005 and underwent colon cancer surgery. Stage IV colon cancers were excludedto focus the analysis on outcomes for surgical treatments with curative intent. Emergentand urgent cases, defined as having time between diagnosis to surgery interval ≤ 1 day and2-7 days, respectively, were excluded to assess outcomes of elective cases. Cox proportionalhazards model was used to investigate the impact of treatment delay time (TDT), definedas time interval between the diagnosis and the definitive surgical treatment, on five-yearoverall and disease-specific survival. Covariates adjusted for in multivariate analysis werecancer stage, right vs. left-sided cancer, age, gender, race, socioeconomic status (SES),insurance status, and marital status. Results: A total of 24,351 patients matched the inclusioncriteria. Treatment delay time of 6 to 12 weeks (12.8% of cases) was associated with 26%increased risk of overall mortality (HR 1.26, p<0.0001, CI 1.18-1.36) and 14% increasedrisk of mortality due to colon cancer (HR 1.14, p=0.0259, CI 1.02-1.29) when comparedto patients with TDT < 6 weeks. Survival was even worse with TDT ≥ 12 weeks (2.7% of