Psoriasis improvement after bariatric surgery
5
Surgery for Obesity and Related Diseases ] (2014) 00–00 Original article Psoriasis improvement after bariatric surgery Héctor Romero-Talamás, M.D. a , Ali Aminian, M.D. a , Ricard Corcelles, M.D. a , Anthony P. Fernandez, M.D., Ph.D. b , Philip R. Schauer, M.D. a , Stacy Brethauer, M.D. a, * Q1 a Bariatric and Metabolic Institute, Cleveland Clinic, Cleveland, Ohio Q4 b Departments of Dermatology and Anatomic Pathology, Cleveland Clinic, Cleveland, Ohio Received December 14, 2013; accepted March 31, 2014 Abstract Background: Psoriasis is a chronic inflammatory skin disease known to be associated with obesity and metabolic syndrome. Single case reports and small series suggest remission or improvement after bariatric surgery, hypothetically through a GLP-1 mediated mechanism. The objective of this study was to investigate on the effect of bariatric surgery on the clinical behavior of psoriasis in obese patients. Methods: A total of 33 morbidly obese individuals with psoriasis who were on active medical treatment were identified. Demographic characteristics and follow-up data were extracted from our database. Medication usage and percentage of affected body surface area (%ABSA) were recorded preoperatively and at least 6 months after bariatric surgery. Results: Nine (27.2%) patients were on systemic therapy at baseline. At a mean follow-up time of 26.2 20.3 months, a mean excess weight loss (EWL) of 48.7 2 6.6% was achieved. This was associated with improvement of psoriasis based on downgrade of medication and %ABSA in 30.3% and 26.1% of patients, respectively. In total, 13 of 33 patients (39.4%) had improvement based on either criteria. Eight (24.2%) patients were not on any psoriasis medication at the latest follow-up (P ¼ .001). Older age at the time of surgery (54.8 8.1 versus 48.1 10.4 years, P ¼ .047), Roux-en-Y gastric bypass versus nonbypass procedures (52.4% versus 16.7%, P ¼ .043), and greater EWL (64.2 26.0% versus 43.4 23.6%, P ¼ .036) predicted improvement. Only 1 (3%) patient experienced worsening after surgery. Conclusion: Almost 40% of our cohort showed improvement of psoriasis several months after bariatric surgery. Improvement is directly related to the degree of postoperative weight loss and is associated with the Roux-en-Y configuration. (Surg Obes Relat Dis 2014;]:00–00.) r 2014 American Society for Metabolic and Bariatric Surgery. All rights reserved. Keywords: Bariatric surgery; Psoriasis; GLP-1; Metabolic syndrome; Gastric bypass Psoriasis is a chronic inflammatory skin disease that affects 1–4% of the world’s population [1]. Patients with psoriasis are affected by chronic skin lesions that may involve any part of their body and usually require long-term treatment that negatively affects their quality of life [2]. It is well known that obesity is a risk factor for psoriasis and increased body mass index (BMI) is associated not only with greater extent of the disease, but also more refractory disease [3,4]. The association between psoriasis and obesity has been postulated as a complex interplay between the immune system, adiposity and metabolic dysregulation [5]. Although the exact mecha- nism of this relationship is unknown, investigators hypothe- size that an increase in proinflammatory cytokines such as (tumor necrosis factor α), interleukin (IL)-1, IL-6, IL-8, and leptin) synthesized by adipose tissue in obese individuals plays a central role. Obesity is linked with low-grade 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65 66 67 68 69 http://dx.doi.org/10.1016/j.soard.2014.03.025 1550-7289/ r 2014 American Society for Metabolic and Bariatric Surgery. All rights reserved. * Correspondence: Dr. Stacy Brethauer, Cleveland Clinic, Bariatric and Metabolic Institute, 9500 Euclid Avenue, M61, Cleveland, OH 44194. E-mail: [email protected]
Transcript of Psoriasis improvement after bariatric surgery

Q1
Q4
12345678910111213141516171819202122232425262728293031323334353637383940414243444546474849505152535455
http://dx.doi.org1550-7289/r 20
*CorrespondMetabolic Institu
E-mail: breth
Surgery for Obesity and Related Diseases ] (2014) 00–00
Original article
Psoriasis improvement after bariatric surgeryHéctor Romero-Talamás, M.D.a, Ali Aminian, M.D.a, Ricard Corcelles, M.D.a,
Anthony P. Fernandez, M.D., Ph.D.b, Philip R. Schauer, M.D.a, Stacy Brethauer, M.D.a,*aBariatric and Metabolic Institute, Cleveland Clinic, Cleveland, Ohio
bDepartments of Dermatology and Anatomic Pathology, Cleveland Clinic, Cleveland, Ohio
Received December 14, 2013; accepted March 31, 2014
Abstract Background: Psoriasis is a chronic inflammatory skin disease known to be associated with obesity
/10.1014 A
ence:te, 9as@c
and metabolic syndrome. Single case reports and small series suggest remission or improvementafter bariatric surgery, hypothetically through a GLP-1 mediated mechanism. The objective of thisstudy was to investigate on the effect of bariatric surgery on the clinical behavior of psoriasis inobese patients.Methods: A total of 33 morbidly obese individuals with psoriasis who were on active medicaltreatment were identified. Demographic characteristics and follow-up data were extracted from ourdatabase. Medication usage and percentage of affected body surface area (%ABSA) were recordedpreoperatively and at least 6 months after bariatric surgery.Results: Nine (27.2%) patients were on systemic therapy at baseline. At a mean follow-up time of26.2 � 20.3 months, a mean excess weight loss (EWL) of 48.7 �2 6.6% was achieved. This wasassociated with improvement of psoriasis based on downgrade of medication and %ABSA in 30.3%and 26.1% of patients, respectively. In total, 13 of 33 patients (39.4%) had improvement based oneither criteria. Eight (24.2%) patients were not on any psoriasis medication at the latest follow-up(P ¼ .001). Older age at the time of surgery (54.8 � 8.1 versus 48.1 � 10.4 years, P ¼ .047),Roux-en-Y gastric bypass versus nonbypass procedures (52.4% versus 16.7%, P ¼ .043), andgreater EWL (64.2 � 26.0% versus 43.4 �23.6%, P ¼ .036) predicted improvement. Only 1 (3%)patient experienced worsening after surgery.Conclusion: Almost 40% of our cohort showed improvement of psoriasis several months afterbariatric surgery. Improvement is directly related to the degree of postoperative weight loss and isassociated with the Roux-en-Y configuration. (Surg Obes Relat Dis 2014;]:00–00.) r 2014American Society for Metabolic and Bariatric Surgery. All rights reserved.
Keywords: Bariatric surgery; Psoriasis; GLP-1; Metabolic syndrome; Gastric bypass
56575859606162
Psoriasis is a chronic inflammatory skin disease that affects1–4% of the world’s population [1]. Patients with psoriasisare affected by chronic skin lesions that may involve any partof their body and usually require long-term treatment thatnegatively affects their quality of life [2]. It is well knownthat obesity is a risk factor for psoriasis and increased body
63646566
16/j.soard.2014.03.025merican Society for Metabolic and Bariatric Surgery. All r
Dr. Stacy Brethauer, Cleveland Clinic, Bariatric and500 Euclid Avenue, M61, Cleveland, OH 44194.cf.org
mass index (BMI) is associated not only with greater extentof the disease, but also more refractory disease [3,4]. Theassociation between psoriasis and obesity has been postulatedas a complex interplay between the immune system, adiposityand metabolic dysregulation [5]. Although the exact mecha-nism of this relationship is unknown, investigators hypothe-size that an increase in proinflammatory cytokines such as(tumor necrosis factor α), interleukin (IL)-1, IL-6, IL-8, andleptin) synthesized by adipose tissue in obese individualsplays a central role. Obesity is linked with low-grade
676869ights reserved.

707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116117118119120121122123124
125126127128129130131132133134135136137138139140
H. Romero-Talamás et al. / Surgery for Obesity and Related Diseases ] (2014) 00–002
systemic inflammation that in theory may precipitate and/orexacerbate psoriatic lesions in overweight and obese individ-uals [1].The obesity epidemic continues to grow worldwide
and surgery remains the only effective and durabletherapy for many individuals [6]. Bariatric surgery hasbeen shown to induce weight loss, improve quality oflife, and reduce co-morbidities [7]. Currently, the effectof bariatric surgery on psoriasis has not been wellstudied. Case reports suggest that Roux-en-Y gastricbypass (RYGB) in patients with psoriasis could result incomplete resolution of the disease [8]. Further smallseries support the benefits of weight loss surgery on thebehavior of psoriasis. The aim of this study is to furtherclarify these findings and identify predictive factors ofpsoriasis resolution after bariatric surgery.
T1
141142143144145146147148149150151152153154155156157158159160161162163164165166167168169170171172173174175176177178179
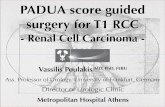
Table 1Metabolic profile of patients with psoriasis after bariatric surgery (n¼33)
Metabolic parameters* Baseline Follow-up P value
BMI (kg/m2) 50.2 � 10.1 38.5 � 9.8 o.001A1C (%) 7.9 � 1.3 6.4 � 1.2 .007FBG (mg/dL) 138.3 � 58.9 101.3 � 27 .005LDL cholesterol (mg/dL) 111.2 � 29.2 81.5 � 29.2 .001HDL cholesterol (mg/dL) 55.5 � 23.7 66 � 20.1 .002Triglycerides (mg/dL) 140.9 � 86.4 116.9 � 116 .236American Diabetes Association goalsA1C o 7% (%) 23.1 61.5 .038BP o 130/80 mmHg (%) 19.4 51.6 .005LDL o 100 mg/dL (%) 35.7 78.6 .014
BMI ¼ body mass index; BP ¼ blood pressure; FBG ¼ fasting bloodglucose; HbA1c ¼ glycated hemoglobin A1c; HDL ¼ high densitylipoprotein; LDL ¼ low density lipoprotein
*Values are mean � SD.
Methods
This was an Investigative Research Board approvedretrospective chart review of all morbidly obese individualswith psoriasis who underwent bariatric surgery at our centerbetween January 2004 and December 2012. We identifiedmorbidly obese patients with psoriasis who were on activemedical treatment at the time of surgery. Demographiccharacteristics (age, sex, and related co-morbidities) andfollow-up data were extracted and analyzed to assesspreoperative and postoperative parameters and outcomes.Psoriasis medication types and status and the percentage
of affected body surface area (%ABSA) were recordedbefore surgery and at least 6 months after the intervention.The %ABSA was calculated based on the dermatologist’sassessment, according to the National Psoriasis Founda-tion’s palm method (the surface area of the hand corre-sponds to 1%) [9]. Improvement of psoriasis was defined asa decrease in %ABSA and/or a downgrade in 1 or 2 of the 3treatment classes (no treatment, local and systemic therapy).The presence of a Koebner lesion (development of iso-morphic pathologic psoriatic lesions at the operative sitescar) was recorded, if present during follow-up [10].Remission of type 2 diabetes mellitus (T2DM) was
defined as glycated hemoglobin (HbA1 c) o 6.5% andfasting blood glucose (FBG) o 126 mg/dL without diabeticmedications. Clinical improvement of T2DM was definedas significant reduction in HbA1 c (by 4 1%), FBG(by 4 25 mg/dL), or diabetes medication requirement [11].Treatment goals of co-morbidities were defined based on
the American Diabetes Association criteria for control ofdiabetes (HbA1 c o 7%), blood pressure (o 130/80 mmHg), and cholesterol (LDL o 100 mg/dL).Data were analyzed using SPSS version for Windows
(SPSS, Inc., Chicago, IL, USA). Results were expressed inmean � SD, and frequency (%). Statistical significance ofmeans and proportions was tested with T test and Z-test,respectively. Categorical variables were analyzed with Χ2
or Fisher’s exact tests. Statistical significance was consid-ered at P o .05.
Results
A total of 33 patients with psoriasis were identified. Mostpatients were female (60.6%). Mean age of the studiedpopulation was 50.8 � 10.0 years and the mean duration ofpsoriasis before bariatric surgery was 24.0 � 9.0 months.Psoriatic arthropathy and family history of psoriasis werepresent in 24.2% and 9.1%, respectively. Presurgical treat-ment of psoriasis included local therapies in 24 (72.7%)patients and systemic medication in 9 patients (27.2%).Systemic agents included Methotrexate, oral corticosteroids,and biologics (tumor necrosis factor α blockers). Metabolicco-morbidities included T2DM (63.6%), hypertension(69.7%), and dyslipidemia (75.7%).Bariatric procedures included RYGB (n ¼ 21), sleeve
gastrectomy (SG) (n ¼ 8), and laparoscopic adjustablegastric banding (n ¼ 4). There were no conversions to opensurgery in our cohort, and no major postoperative compli-cations occurred. Mean BMI at the time of surgery was50.2 � 10.1 kg/m2, and BMI decreased to 38.5 � 9.8 at amean follow-up period of 26.2 � 20.3 months (range,6–77), which corresponded to mean percent excess weightloss (EWL) of 48.7 � 26.6%. Table 1 summarizes themetabolic profile of patients at baseline and follow-up.A total of 13 patients (39.4%) reported improvement in
psoriasis after the surgical intervention based on downgradein medication category (30.3%) and %ABSA (26.1%).Eight patients (24.2%) were not on any medication at thelatest follow-up point (P ¼ .001). Six (75%) of themunderwent RYGB, 1 (12.5%) had a SG, and 1 (12.5%) alaparoscopic adjustable gastric banding. Only 1 patient(3%), who underwent a SG, experienced worsening ofpsoriasis after bariatric surgery. Five (15.1%) patients wereon a systemic medication at follow-up. A significantreduction in %ABSA was observed after bariatric surgery

180181182183184185186187188189190191192193194195196197198199200201202203204205206207208209210211212213214215216217218219220221222223224225226227228229230231232233234
235236237238239240241242
Q3 Psoriasis after Bariatric Surgery / Surgery for Obesity and Related Diseases ] (2014) 00–00 3
(5.7 � 4.1% versus 1.7 � 2.1%, P ¼ .04). No patientdeveloped Koebner phenomenon within surgical scarsduring the follow-up period.Predictors of psoriasis improvement were older age at the
time of surgery (54.8 � 8.1 versus 48.1 � 10.4 years, P ¼.047), RYGB versus nonbypass procedures (52.4% versus16.7%, P ¼ .043) and greater %EWL (64.2 � 26.0 versus43.4 � 23.6, P ¼ .036).
243244245246247248249250251252253254255256257258259260261262263264265266267268269270271272273274275276277278279280281282283284285286287288289
Discussion
Psoriasis is an immune-mediated disease characterized byincreased epithelial turnover. Patients with psoriasis presentwith erythematous scaly patches and plaques that caninvolve any part of their anatomy. The negative effect ofpsoriasis on patient’s quality of life is significant, similar tothat of T2DM [12]. Psoriasis is also associated withmetabolic syndrome that may lead to hypertension,T2DM, and myocardial infarction [13]. The associationbetween psoriasis and obesity has been well established inseveral epidemiologic studies. A systematic review andmeta-analysis of 16 observational studies including4200,000 psoriasis patients has shown that individualswith psoriasis have a higher incidence and prevalence ofobesity compared to the general population (OR 1.66, CI95%CI 1.46–1.89) [14]. The same meta-analysis demonstratedthat patients with severe psoriasis have a higher risk ofbeing obese (OR 2.23, CI95% 1.63–3.05) than patients witha mild form of the disease (OR 1.46, CI95% 1.17–1.82).A recent cohort study by Love et al. [15] involving 75,395individuals with psoriasis reports an increased risk ofpsoriatic arthritis with increased BMI (relative risk of 1.48in patients with a BMI Z 35 kg/m2).Currently, the role of weight loss as a treatment modality
for psoriasis in obese patients is under investigation. Thereare a few randomized trials that investigate the clinicaleffects of weight loss on the severity of this skin disease[16,17]. Gisondi et al. [16] observed that weight lossinduced by a low-calorie diet improved the response tolow-dose cyclosporine therapy in patients with psoriasis.A prospective randomized controlled trial conducted byJensen et al. [17] also recently addressed the effect ofweight loss reduction in overweight psoriasis patients. Inthis study, the intervention group, which received a lowenergy diet (800–1000 kcal/d) for 8 weeks, experienced asignificant improvement in clinical response and quality oflife over the control group.Given this scenario, it seems reasonable to surmise that
weight loss surgery could be a treatment option in obesepatients with psoriasis. The literature regarding bariatricsurgery and psoriasis is limited to a few case reports andsmall case series describing improvement of the skin lesionsafter surgery [18–21]. Conversely, 1 case report showedpsoriasis worsening after surgery, although the type ofprocedure was not specified [22]. Herein, we report the
outcomes of 33 consecutive morbidly obese patients afterweight loss surgery. Forty percent of patients showedimprovement in psoriasis after surgical intervention basedon %ABSA affected and medication downgrade. Theclinical improvement observed in our study was inferiorto that published by other authors; however, there areseveral points that must be taken into consideration. Fariaset al. [19] reported a 70% psoriasis resolution rate at6 months follow-up and this is currently the highest rateever published. However, the study included only 10patients and there is no mention of how improvement wasmeasured. In addition, 4 of the 7 patients who had initiallyachieved remission relapsed at mid-term follow-up (0.5–2.5yr), bringing the resolution rate to a 30%. Hossler et al. [23]observed improvement of the skin lesions in 62% (n ¼ 34)of patients undergoing bariatric surgery (88% had RYGB).Data was collected retrospectively using a telephone surveyand no follow-up parameters were described. Differences intype of bariatric procedures, follow-up time, and the lack ofdocumentation of medication status after surgery make thecomparison between studies difficult. Our study presents thelongest reported follow-up to date on this topic(26.2 � 20.3 mo).The differences in methods used to determine psoriasis
improvement after surgery might also explain differentresults among the published series. In our study, wedemonstrated psoriasis improvement in 40% based on %ABSA and medication class reduction. We used the simpleand reproducible palm method to calculate the extent ofdisease based on the dermatologist description. The palmmethod scores 1% for each palm (100% of BSA corre-sponds to 100 palms) but fails to evaluate local severity. Inour cohort who were on active pharmacotherapy at the timeof surgery, 8 patients (24.2%) were not on any psoriasismedication at the latest follow-up visit (P ¼ .001), while 19patients were being treated by topical medications only,compared with the 24 individuals at baseline. It is alsoimportant to mention that only 1 patient worsened aftersurgery (3%). This was a 60-year-old man who developedmore widespread psoriasis 1-year after SG, despite EWL of50% and significant improvement of T2DM.Our analysis identified greater EWL (P ¼ .036), RYGB
(P ¼ .043), and advanced age at time of surgery (P ¼ .047)as predictors of psoriasis improvement. It has been reportedthat surgical and medical weight loss has a clear beneficialeffect over the activity of the disease. This hypothesis wassupported by our analysis, which showed a significantcorrelation between degree of EWL and psoriasis improve-ment after surgery. RYGB was also associated withsignificant improvement in our analysis. The 12 patientswho did not undergo RYGB (8 sleeve gastrectomy,4 gastric banding) had inferior outcomes in terms ofimprovement compared with the RYGB group, a findingthat is supported by results observed by other authors [19].Interestingly, the only patient that had worsening of the

Q5
290291292293294295296297298299300301302303304305306307308309310311312313314315316317318319320321322323324325326327328329330331332333334335336337338339340341342343344
345346347348349350351352353354355356357358359360361362363364365366367368369370371372373374375376377378379380381382383384385386387388389390391392393394
H. Romero-Talamás et al. / Surgery for Obesity and Related Diseases ] (2014) 00–004
disease had a laparoscopic sleeve gastrectomy as hisbariatric procedure. On this note, several studies haveshown that the gastrointestinal rearrangement after RYGB(duodenal exclusion with rapid food transit to the distalileum) is associated with T2DM and lipid profile improve-ment by endocrine-mediated mechanisms [24]. Because anincrease in GLP-1 seen after RYGB and sleeve has beenassociated with resolution of some metabolic conditions,some researchers have hypothesized that GLP-1 could playa role in psoriasis improvement after RYGB through ananti-inflammatory effect [25]. There are recently publishedreports of significant and rapid improvement of psoriasis inpatients treated with a GLP-1 receptor agonist (exenatide,liraglutide) [26,27], probably due to a direct anti-inflammatory effect on invariant natural killer T-cells [28].Furthermore, the presence of GLP-1 receptors has beenidentified in biopsies of psoriasis plaques demonstratingthe possibility of direct interaction between the lesion andthe peptide [29]. Further studies are required to explore therelationship between psoriasis resolution and GLP-1.In conjunction with obesity, metabolic syndrome con-
tributes to the development of a chronic systemic inflam-matory state and has been associated with psoriasis [22].Significant improvement in proinflammatory profiles (CRP,IL-6, leptin) and insulin sensitivity has recently beenreported after RYGB and this could certainly play animportant role in the improvement of psoriasis [30]. Theimproved metabolic profiles in our cohort support thisconcept. Surprisingly, advanced age at the time of surgerywas also identified as a predictor of psoriasis improvementafter surgery. We expected advanced age to negativelyaffect outcomes secondary to the chronicity of well-established disease; however, we found the exact opposite.The positive effect of advanced age on outcomes has beenreported by Hossler et al. [23], but a possible mechanismremains to be clarified.There are some limitations in our retrospective study.
First, the estimation of %ABSA by relying on clinicalrecords was not ideal and does not account for otherimportant clinical aspects of disease, including plaquethickness and amount of scale. Second, the sample size isrelatively small but sufficient to determine significantimprovement and predictors of it. Third, we were unableto assess whether other indirect factors may have alsocontributed to psoriasis improvement, including increasedphysical activity, dietary changes, or decreases/discontinua-tion in nonpsoriatic medications. Also, a psoriasis-relatedquality of life assessment could have enhanced this reportand should be included in future studies examining thisobesity-related co-morbidity.
395396397398399
Conclusion
Nearly 40% of our cohort showed improvement ofpsoriasis several months after bariatric surgery, confirming
the beneficial effect that these procedures have on psoriasis.Improvement appears to be directly related to the degree ofpostoperative weight loss of the individual as well as to thechoice of procedure. Psoriasis should be added to the list ofmedical conditions that improve after bariatric surgery.Further prospective research is warranted to evaluate themechanism by which these outcomes are achieved.
Disclosures
xx
References
[1] Schon MP, Boehncke WH. Psoriasis N Engl J Med 2005;352:1899–912.
[2] Johnson MA, Armstrong AW. Clinical and histologic diagnosticguidelines for psoriasis: a critical review. Clin Rev Allergy Immunol2013;44:166–72.
[3] Naldi L, Chatenoud L, Linder D, et al. Cigarette smoking, body massindex, and stressful life events as risk factors for psoriasis: resultsfrom an Italian case-control study. J Invest Dermatol 2005;125:61–7.
[4] Setty AR, Curhan G, Choi HK. Obesity, waist circumference, weightchange, and the risk of psoriasis in women: Nurses' Health Study II.Arch Intern Med 2007;167:1670–5.
[5] Hamminga EA, van der Lely AJ, Neumann HA, Thio HB. Chronicinflammation in psoriasis and obesity: implications for therapy. MedHypotheses 2006;67:768–73.
[6] Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of obesityand trends in body mass index among US children and adolescents,1999-2010. JAMA 2012;307:483–90.
[7] Buchwald H, Estok R, Fahrbach K, Banel D, Sledge I. Trends inmortality in bariatric surgery: a systematic review and meta-analysis.Surgery 2007;142:621–32.
[8] Halawi A, Abiad F, Abbas O. Bariatric surgery and its effects on theskin and skin diseases. Obes Surg 2013;23:408–13.
[9] Bremmer S, Van Voorhees AS, Hsu S, et al. Obesity and psoriasis:from the Medical Board of the National Psoriasis Foundation. J AmAcad Dermatol 2010;63:1058–69.
[10] Mendez-Fernandez MA. Koebner phenomenon: what you don't knowmay hurt you. Ann Plast Surg 2000;44:644–5.
[11] Brethauer SA, Aminian A, Romero-Talamas H, et al. Can diabetes besurgically cured? Long-term metabolic effects of bariatric surgery inobese patients with type 2 diabetes mellitus. Ann Surg 2013;258:628–36.
[12] Grozdev I, Kast D, Cao L, et al. Physical and mental impact ofpsoriasis severity as measured by the compact Short Form-12 HealthSurvey (SF-12) quality of life tool. J Invest Dermatol 2012;132:1111–6.
[13] Yeung H, Takeshita J, Mehta NN, et al. Psoriasis severity and theprevalence of major medical comorbidity: a population-based study.JAMA Dermatol 2013;149:1173–9.
[14] Armstrong AW, Harskamp CT, Armstrong EJ. The associationbetween psoriasis and obesity: a systematic review and meta-analysis of observational studies. Nutr Diabetes 2012;2:e54.
[15] Love TJ, Zhu Y, Zhang Y, et al. Obesity and the risk of psoriaticarthritis: a population-based study. Ann Rheum Dis 2012;71:1273–7.
[16] Gisondi P, Del Giglio M, Di Francesco V, Zamboni M, GirolomoniG. Weight loss improves the response of obese patients withmoderate-to-severe chronic plaque psoriasis to low-dose cyclosporinetherapy: a randomized, controlled, investigator-blinded clinical trial.Am J Clin Nutr 2008;88:1242–7.

400401402403404405406407408409410411412413414415416
417418419420421422423424425426427428429430431432433
Q3 Psoriasis after Bariatric Surgery / Surgery for Obesity and Related Diseases ] (2014) 00–00 5
[17] Jensen P, Zachariae C, Christensen R, et al. Effect of weight loss onthe severity of psoriasis: a randomized clinical study. JAMADermatol 2013;149:795–801.
[18] de Menezes Ettinger JE, Azaro E, de Souza CA, et al. Remission ofpsoriasis after open gastric bypass. Obes Surg 2006;16:94–7.
[19] Farias MM, Achurra P, Boza C, Vega A, de la Cruz C. Psoriasisfollowing bariatric surgery: clinical evolution and impact on qualityof life on 10 patients. Obes Surg 2012;22:877–80.
[20] Higa-Sansone G, Szomstein S, Soto F, et al. Psoriasis remission afterlaparoscopic Roux-en-Y gastric bypass for morbid obesity. Obes Surg2004;14:1132–4.
[21] Hossler EW, Maroon MS, Mowad CM. Gastric bypass surgeryimproves psoriasis. J Am Acad Dermatol 2011;65:198–200.
[22] Perez-Perez L, Allegue F, Caeiro JL, Zulaica JM. Severe psoriasis,morbid obesity and bariatric surgery. Clin Exp Dermatol 2009;34:e421–2.
[23] Hossler EW, Wood GC, Still CD, Mowad CM, Maroon MS. Theeffect of weight loss surgery on the severity of psoriasis. Br JDermatol 2013;168:660–1.
[24] Patel RT, Shukla AP, Ahn SM, Moreira M, Rubino F. Surgicalcontrol of obesity and diabetes: The role of intestinal vs. gastric
mechanisms in the regulation of body weight and glucose homeo-stasis. Obesity (Silver Spring) 2014;22:159–69.
[25] Faurschou A, Zachariae C, Skov L, Vilsboll T, Knop FK. Gastricbypass surgery: improving psoriasis through a GLP-1-dependentmechanism? Med Hypotheses 2011;77:1098–101.
[26] Buysschaert M, Tennstedt D, Preumont V. Improvement of psoriasisduring exenatide treatment in a patient with diabetes Diabetes Metab2012;38:86–8.
[27] Faurschou A, Knop FK, Thyssen JP, et al. Improvement in psoriasisafter treatment with the glucagon-like peptide-1 receptor agonistliraglutide. Acta Diabetol 2014;51:147–50.
[28] Hogan AE, Tobin AM, Ahern T, et al. Glucagon-like peptide-1(GLP-1) and the regulation of human invariant natural killer T cells:lessons from obesity, diabetes and psoriasis. Diabetologia 2011;54:2745–54.
[29] Faurschou A, Pedersen J, Gyldenlove M, et al. Increased expressionof glucagon-like peptide-1 receptors in psoriasis plaques. Exp Derm-atol 2013;22:150–2.
[30] Brethauer SA, Heneghan HM, Eldar S, et al. Early effects of gastricbypass on endothelial function, inflammation, and cardiovascular riskin obese patients. Surg Endosc 2011;25:2650–9.