Vacant sets and vacant nets: Component structures induced ...

PRRT in Management of NETs
Ioannis Karfis, MD PhD
Assistant Head of Clinic
Nuclear Medicine Dept
IJB, Brussels

Pavel M: Neuroendocrinology 2013;97:99-112
THERAPEUTIC TARGETS in NENs

locoregional treatments (surgery/RFA/TACE/TARE)
177Lu- / 90Y- PRRT
GRADE 2
SSAs
Chemo (STZ /
5FU / TMZ / CAP)
INF α-2b
sunitinib
(pNETs)
everolimus
GRADE 1
SSAs
INF α-2b
sunitinib
(pNETs)
everolimus
GRADE 3
Chemo
(cisplatin/etoposi
de,
temozolamide/ca
pecitabine,
topotecan, CAF)
THERAPEUTIC ARENA in NENs

KEY ROLE OF NM IN MGMT OF NETs
MOLECULAR IMAGING / DIAGNOSIS 68Gallium-DOTA-peptide (β+) [68Ga-DOTA-OCTREOTATE]
Receptor imaging
Staging/Sélection of patients (cold and hot SSAs)
Quantification
PEPTIDE RECEPTOR RADIONUCLIDE THERAPY 177Lutetium-DOTA-peptide (β-, γ) [177Lu-DOTA-OCTREOTATE]
Therapy
Dosimetry
CHELATOR PEPTIDE SS receptor
AGONIST

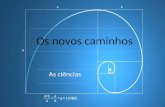
68Ga-DOTATATE PET MIP 177Lu-DOTATATE SPECT MIP
THERANOSTIC TWINS
WE SEE WHAT WE TREAT & WE TREAT WHAT WE SEE...

PRRT isotopes:
177Lu: third generation radionuclide
β-emission >>>>> therapy / reduced radiation dose to OaRs
γ-radiation >>>>> imaging / quantification / dosimetry
t1/2phys emissions energy
particule tissue
penetrationmax
111In 2,8d
γ
Auger e-
IC e-
0,5-25KeV
218-245KeV
0,02-10μm
200-550μm
90Y 2,7d β 2,2MeV 12mm
177Lu 6,7d γ β
497KeV
2mm
HISTORICAL BACKGROUND
Kwekkeboom DJ et al, Endocr-Rel Cancer 2010;17(1):R53-73

internalization
177Lu
Octr
90Y
Octr
Octr
111In
PRRT PRINCIPLE

Bodei L et al.: (joint IAEA/EANM/SNMMI guidelines). EJNMMI 2013

PRRT INDICATIONS
Bodei L et al.: (joint IAEA/EANM/SNMMI guidelines). EJNMMI 2013
The ideal candidates are those with well-differentiated NET
G1/G2 (metastatic or inoperable NET with positive
expression of sstr2)
patients with gastroenteropancreatic/bronchial NETs, but also
patients with phaeochromocytoma, paraganglioma,
neuroblastoma or medullary thyroid carcinoma.

Bodei L et al.: (joint IAEA/EANM/SNMMI guidelines. EJNMMI 2013)
ABSOLUTE: Pregnancy
Acute/Severe concomitant disease
Acute psychiatric disease
RELATIVE: Lactation
Compromised renal fonction
[<60% NV adjusted for age]
Compromised bone marrow fonction
[WBC: <3,000/μL with neutros<1,000/μL]
PLT: <75,000/μL
RBC: <3,000,000/μL]
PRRT CONTRAINDICATIONS

Tx MODALITIES (177Lu-PRRT)
One injection iv every 6-12 weeks
Administered activity: 5.5-7.4GBq (150-200mCi)/cycle
Number of cycles: 3-5
0 1 2 3 4 5 6h
AA AE
177Lu
END AA START AA
Bodei L et al.: (joint IAEA/EANM/SNMMI guidelines). EJNMMI 2013

HOSPITALISATION
Hospitalised in dedicated rooms / isolation
Duration according national regulations
Urine/faeces should be disposed to according national
regulations
Hydration/Urination as much as possible during the
process

POST-Tx RECOMMENDATIONS
Released if radiation rate <20µSv/h @1m
Oral/Written practical radioprotection instructions
Release Card to carry for up to 10x t1/2biol
Avoid close contacts (<1m) for up to 2 weeks
3 weeks if children <10y/pregnant women
Hydration as much as possible

0 5 10 15 20 25 30 35 40
Ezziddin et al, 2014 (Bonn)
Bodei et al, 2011 (Milan)
Garkavij et al, 2010 (Lund)
Sward et al, 2010 (Gothenberg)
Kweekeboom et al, 2008 (Rotterdam)
Pfeifer et al, 2011 (Copengahen)
Cwikla et al, 2010 (Warsaw)
Imhof et al, 2010 (Basel)
Valkema et al, 2006 -multicentric-
Bodei et al, 2004 (Milan)
Waldherr et al, 2002 (Basel)
Delpassand et al, 2012 (Houston)
Limouris et al, 2008 (Athens)
Anthony et al, 2002 (New Orleans)
Valkema et al, 2002 (Rotterdam)
111In-DTPAOC
90Y-DOTATOC
177Lu-DOTATATE
EFFICACY: OR(CR+PR)
%

EFFICACY: PFS/OS
Trial Therapeutic Agent pts PFS (m) OS (m)
Valkema et al, 2002 111In-DTPA-OC 32 - 12
Delpassand et al, 2012 111In-DTPA-OC 40 - 22
Valkema et al, 2006 90Y-DOTA-TOC 58 29 37
Bushnell et al, 2010 90Y-DOTA-TOC 90 16 27
Cwikla et al, 2010 90Y-DOTA-TOC 58 17 22
Pfeifer et al, 2011 90Y-DOTA-TOC 53 29 -
Kwekkeboom et al, 2008 177Lu-DOTATATE 310 33 46
Bodei et al, 2011 177Lu-DOTATATE 42 - 36
Ezziddin et al, 2014 177Lu-DOTATATE 74 26 55
Kouvaraki et al, 2004 STZ+5-FU+DOXORUBICIN 84 39 18/37
Kulke et al, 2009 TMZ 53 34 14/35
Chan et al, 2013 TMZ+BEVACIZUMAB 15 33 14/42
Chan et al, 2013 TMZ+EVEROLIMUS 43 40 15/-
Yao et al, 2011 EVEROLIMUS 207 5 11/-
Raymond et al, 2011 SUNITINIB 86 9 11/-

NETTER-1 multicentric (41 centers/8 countries), prospective,
randomized, phase III
sponsor: Advanced Accelerator Applications (Lutathera®)
unresectable progressive SSTR+ midgut NETs
Sandostatine LAR 60mg vs 177Lu-DOTATATE c.a.
229 patients were randomized on the 2 arms
study start date: 11/2012, estimated study completion
12/2019
Strosberg J et al.: NEJM 2017;376:125-35

RECIST 1.1 assessments every 12±1w from the first
treatment date until EOS
NETTER-1: DESIGN

NETTER-1: EFFICACY - PFS/OS (n: 229)
Octreotide LAR 60 mg
Median PFS: 8.4 m
177Lu-DOTATATE Median PFS: NR
trial has not yet reached the point at
which the mOS can be calculated
interim analysis results suggest a
longer mOS on the PRRT arm
mPFS has not been reached in the 177Lu-DOTATATE arm
Strosberg J et al.: NEJM 2017;376:125-35

PRRT (n=101) SSA (n=100)
Complete Response (n) 1 0
Partial Response (n) 18 3
Objective Response (n, %) 19% 3%
Progressive Disease (n, %) 5 (4%) 27 (24%)
Stable Disease (n, %) 77 (66%) 70 (62%)
NETTER-1: EFFICACY - OR (n: 229)
Strosberg J et al.: NEJM 2017;376:125-35

TOXICITY?
DOSE DEPENDENT
ACUTE
>nausea, vomiting
>fatigue (first 10d post-injection)
>abdominal pain/disconfort
>carcinoid crisis, <1% (6/479 pts)
SUBACUTE/CHRONIC
> G3/G4 hematological: <11% (BM: critical organ, nadir: 6-
8w PI)
> G1 alopecia: 65%
CHRONIC
> G4 renal: <3.5% (kidneys: critical organ)
de Keizer B et al.: EJNMMI 2008;35:749-55, Bodei L et al.: Sem NM 2016;46:225-238
Sabet A et al.: Nuclearmedizin 2014;53:54-59, Kwekkeboom DJ et al.: JCO 2008;26:2124-30

TOXICITY?
DOSE INDEPENDENT
MDS/AL
> rare: MDS (3%) / AL (1.1%)
> median interval btw last PRRT - MDS: 3.7y
> stochastic event: unidentified individual susceptibilities
> no correlation with administered activities
> consequence of mutational events induced by sequentional
cytotoxic therapies: prenious alkylating chemotherapy
>NETTER1: 1pt in the PRRT arm/229pts
>Kwekkeboom D et al: n: 504 MDS/ALL: 3
Sabet A et al: n: 203 MDS/ALL: 3
Bodei L et al: n: 807 MDS/ALL: 8
Strosberg J et al.: NEJM 2017;376:125-35, Bodei L et al.: EJNMMI 2015;42:5-19
Sabet A et al.: JNM 2013;54:1857-61, Kwekkeboom DJ et al.: JCO 2008;26:2124-30

PLACE OF PRRT (siNETs)?
Pavel M et al.: Neuroendocrinology 2016;103:172-185

PLACE OF PRRT (pNETs)?
Pavel M et al.: Neuroendocrinology 2016;103:172-185

PLACE OF PRRT? ideally, second line treatment, after failure of SSAs
outstanding results of NETTER1
effective treatments must be given earlier at the course of
the disease

IJB: one of the two PRRT centers in Belgium
63 pts: GEP-NETs: 46pts (1 insulinoma, 1 gastrinoma, 2
rectal)
mammary NET: 2pts
NET pulmonaire: 5 pt
paragangliome/pheochromocytome: 6pts
kidney NET: 1pt
CUPS: 3pts
186 injections iv so far
PRRT: THE IJB EXPERIENCE OF ~4y

LuMEn: ‘‘177Lu-octreotate treatment outcome prediction using
Multimodality imaging in refractory neuroEndocrine tumours’’
[NCT01842165]
ongoing φII, non-randomised trial
GEP-NETs
to be bicentric soon (+UZL)
objectives: evaluate the predictive value of the following imaging
biomarkers: 68Ga-DOTATATE and 18FDG uptake, tumor absorbed
dose > to identify non responding lesions / non responding patients.
endpoints: lb-TTP, pb-PFS, efficacy & safety
PRRT: THE IJB EXPERIENCE OF ~4y

LuMEn: main inclusion criteria:
Disease progression defined as follows:
- Radiological progression (RECIST 1.1) over the last 12m
- Progression on SSTR imaging, over the last 12m
- Clinical progression + significant increase in tumoral markers
Adequate renal function:
GFR≥50 mL/min/1.73m2
Adequate bone marrow function:
Hg≥9 g/dL;
WBC≥2·103/μL;
PLTs≥100·103/μL.
Adequate liver function
PRRT: THE IJB EXPERIENCE OF ~4y

UNMET NEEDS IN PRRT
REGISTRATION – APPROVAL UPON AUTHORITIES
ACCURATE DOSIMETRY TO GUIDE THERAPY
? cycles of PRRT
STANDARDISATION
optimal nephroprotection scheme
optimal interval between injections
optimal administered activity (cumulative, /cycle: standard vs tailored)
PREDICTIVE BIOMARKERS

PREDICTIVE BIOMARKERS?
OF RESPONSE:
High uptake on receptor imaging
[Rotterdam visual 5 scale: >liver uptake or ≥spleen uptake]
[68Ga-DOTA-peptide uptake correlates with sst2R expression]
OF NON RESPONSE:
Bulky hepatic metastases
Karnofsky performance score<70
Significant weight loss
Kwekkeboom DJ et al.: JCO 2008;26:2124-30
Boy C et al.: EJNMMI 2011;38:1224-36

STRATEGIES TO IMPROVE PRRT EFFICACY
combination with chemotherapy (5FU, Cap/Tem)
intra-arterial PRRT for liver only / dominant disease
α-emittors as novel therapeutic isotopes
re-Tx after progressive disease following PRRT
neo-adjuvant PRRT
Kashyap R et al.: EJNMMI 2014, Claringbold PG et al.: EJNMMI 2011, Limouris GS et al.: Clin Nucl Med
2016, Kratochwil C et al.: EJNMMI 2014, Sabet A et al.: EJNMMI 2014, van Vliet EI et al.: JNM 2015

TAKE HOME MESSAGES
PRRT IS EFFICIENT
high tumor response rates (80%: OR+SD)
PFS that may reach 40m according to NETTER1
SAFE PROFILE
excellent tolerance
mild acute AEs
<10% late AEs
ideally: second line Tx after failure of SSAs

MULTIDISCIPLINARITY IN NET MGMT
ENDOCRINO- LOGY
NUCLEAR MEDICINE
GASTRO- ENTEROLOGY
ONCOLOGY
RADIOLOGY
SURGERY
PATHOLOGY
PATIENT

10 novembre
THANK YOU
FOR YOUR
ATTENTION