Porcine hepatic response to sepsis and its amplification by ... · receptor antagonist ICI 118551...
12
467 Clinical Science (1998) 95, 467–478 (Printed in Great Britain) Porcine hepatic response to sepsis and its amplification by an adrenergic receptor α 1 agonist and a β 2 antagonist D. TIGHE, R. MOSS* and D. BENNETT Department of Physiological Medicine, St. George’s Hospital Medical School, Cranmer Terrace, London SW17 ORE, U.K., *Department of Electron Microscopy, St. George’s Hospital Medical School, Cranmer Terrace, London SW17 ORE, U.K., and Department of Intensive Care, St. George’s Hospital Medical School, Cranmer Terrace, London SW17 ORE, U.K. A B S T R A C T 1. We investigated the effect of adrenergic receptor stimulation or inhibition on the hepatic ultrastructural changes in a porcine faecal peritonitis model of multi-organ failure. We infused either the α 1 adrenergic receptor agonist methoxamine or the β 2 adrenergic receptor antagonist ICI 118551 during 8 h of the study. 2. Anaesthetized pigs (25–30 kg) were divided into four non-septic groups (control, non-septic, non-septic methoxamine and non-septic ICI 118551) and three septic groups (septic, septic methoxamine and septic ICI 118551). 3. Changes in hepatic ultrastructure were measured by morphometric analysis. The septic group was significantly worse than all the non-septic groups. Septic methoxamine and septic ICI 118551 were significantly worse than the septic group. 4. Septic methoxamine and septic ICI 118551 had a significantly increased perisinusoidal space ; septic methoxamine had significant hepatocyte vacuolation. 5. Hepatic ultrastructural changes were independent of hepatic blood flow. 6. Septic methoxamine had significant myocardial depression. 7. The α 1 adrenergic receptor agonist methoxamine or the β 2 antagonist ICI 118551 both amplified the hepatic injury normally found during sepsis in our porcine model. 8. These findings suggest that during sepsis a protective endogenous β 2 adrenergic receptor- mediated anti-inflammatory response is activated via cell membrane transduction to stimulate the trimeric G-protein complex Gs and activate the second cell messenger cAMP. 9. In addition, it is likely that α 1 adrenergic receptor agonists amplify the inflammatory response by stimulating the cell-surface receptor-linked trimeric G-protein complex to activate Gq and the second cell messenger phospholipase C. INTRODUCTION The high morbidity and mortality of patients with septicaemia and end-organ dysfunction has defied suc- cessful intervention and therapy. In critically ill patients, well-designed randomized prospective trials of agents Key words : adrenergic agonist, adrenergic antagonist, inflammation, methoxamine, sepsis. Abbreviations : IL, interleukin ; PAOP, pulmonary artery occlusion pressure. Correspondence : Dr Derek Tighe. designed to inhibit inflammatory mediators generated in septic patients [1–3] have shown little benefit. We developed a model of organ dysfunction in septic pigs [4,5] that mimics the changes seen in critically ill patients. Peritonitis is induced and, when well estab- lished, hepatic tissue is removed for histological study # 1998 The Biochemical Society and the Medical Research Society
Transcript of Porcine hepatic response to sepsis and its amplification by ... · receptor antagonist ICI 118551...

467Clinical Science (1998) 95, 467–478 (Printed in Great Britain)
Porcine hepatic response to sepsis and itsamplification by an adrenergic receptor
α1 agonist and a β2 antagonist
D. TIGHE, R. MOSS* and D. BENNETT†Department of Physiological Medicine, St. George’s Hospital Medical School, Cranmer Terrace, London SW17 ORE, U.K.,*Department of Electron Microscopy, St. George’s Hospital Medical School, Cranmer Terrace, London SW17 ORE, U.K., and†Department of Intensive Care, St. George’s Hospital Medical School, Cranmer Terrace, London SW17 ORE, U.K.
A B S T R A C T
1. We investigated the effect of adrenergic receptor stimulation or inhibition on the hepatic
ultrastructural changes in a porcine faecal peritonitis model of multi-organ failure. We infused
either the α1 adrenergic receptor agonist methoxamine or the β2 adrenergic receptor antagonist
ICI 118551 during 8 h of the study.
2. Anaesthetized pigs (25–30 kg) were divided into four non-septic groups (control, non-septic,
non-septic methoxamine and non-septic ICI 118551) and three septic groups (septic, septic
methoxamine and septic ICI 118551).
3. Changes in hepatic ultrastructure were measured by morphometric analysis. The septic group
was significantly worse than all the non-septic groups. Septic methoxamine and septic ICI 118551
were significantly worse than the septic group.
4. Septic methoxamine and septic ICI 118551 had a significantly increased perisinusoidal space;
septic methoxamine had significant hepatocyte vacuolation.
5. Hepatic ultrastructural changes were independent of hepatic blood flow.
6. Septic methoxamine had significant myocardial depression.
7. The α1 adrenergic receptor agonist methoxamine or the β2 antagonist ICI 118551 both amplified
the hepatic injury normally found during sepsis in our porcine model.
8. These findings suggest that during sepsis a protective endogenous β2 adrenergic receptor-
mediated anti-inflammatory response is activated via cell membrane transduction to stimulate
the trimeric G-protein complex Gs and activate the second cell messenger cAMP.
9. In addition, it is likely that α1 adrenergic receptor agonists amplify the inflammatory response
by stimulating the cell-surface receptor-linked trimeric G-protein complex to activate Gq and
the second cell messenger phospholipase C.
INTRODUCTION
The high morbidity and mortality of patients withsepticaemia and end-organ dysfunction has defied suc-cessful intervention and therapy. In critically ill patients,well-designed randomized prospective trials of agents
Key words : adrenergic agonist, adrenergic antagonist, inflammation, methoxamine, sepsis.Abbreviations : IL, interleukin; PAOP, pulmonary artery occlusion pressure.Correspondence: Dr Derek Tighe.
designed to inhibit inflammatory mediators generated inseptic patients [1–3] have shown little benefit.
We developed a model of organ dysfunction in septicpigs [4,5] that mimics the changes seen in critically illpatients. Peritonitis is induced and, when well estab-lished, hepatic tissue is removed for histological study
# 1998 The Biochemical Society and the Medical Research Society

468 D. Tighe, R. Moss and D. Bennett
and morphometric analysis of ultrastructural changes toquantify and compare these changes. We have recentlyreported [5] the important contrasting changes in liverultrastructure in this animal model when either dopex-amine or dobutamine is infused. We considered that thediffering pharmacology of these two agents was associ-ated with their dissimilar effect on hepatic ultrastructureduring sepsis. The pharmacology of dopexamine isreasonably well established [6,7] ; it is a β
#adrenergic
receptor agonist with dopamine 1 and 2 properties. Thepharmacology of dobutamine is not quite so clear cut ; theprime literature describes it as a racemic mixture [8–10].The (®)-enantiomer of dobutamine is predominantly anα1 adrenergic receptor agonist which has been shown todisplay greater inotropic selectivity than the ()-en-antiomer, which is predominantly a β
"and β
#adrenergic
receptor agonist. The drug’s inotropic effect appears tobe mediated primarily through α
"adrenergic receptor
stimulation which increases cardiac output by stimu-lation of cardiac α adrenergic receptors [11], but itspressor effect is offset by dilation of blood vessels inducedby β
#adrenergic receptor stimulation.
In this animal model of hepatic damage during sepsisthe changes are well documented [4,5] ; we have describedsinusoidal leucostasis and activation of sinusoidal leu-cocytes with endothelial and Kupffer cell swelling, whichresult in occlusion of the sinusoidal lumen. Althoughthere is deterioration of hepatocyte mitochondria anddilation of endoplasmic reticulum there are rarely anyother major changes to hepatocytes or dilation of theSpace of Disse.
In an earlier study we reported [5] how further majordeterioration was observed in the liver when dobutaminewas infused during sepsis. The endothelium becamedetached from the hepatocyte apical membrane, manyapical membranes were disrupted spilling out their cellcontents, and hepatocytes became detached from eachother allowing blood cells to circulate among them. Inaddition, a considerable number of membrane-linedvacuoles were observed in the hepatocytes. This de-terioration was observed when hepatic blood flow wasmaintained above basal levels, discounting the possibilitythat further hepatic injury might have been due toischaemia or inappropriate distribution of blood flow.
When dopexamine was infused in this septic animalmodel there was a reduction in hepatic ultrastructuraldeterioration reflected by a significant reduction insinusoidal leucostasis, endothelial and Kupffer cellswelling and sinusoidal occlusion. There was no dilationof the Space of Disse and no vacuolation of hepatocytes.
The difference between these two agents lies indobutamine being an α
"adrenergic receptor agonist.
There are no previous reports of α adrenergic receptoragonists inducing additional injury in septic animalswhen normal blood flow is maintained. Minneman [12]described how inflammatory mediators such as throm-
bin, histamine, leukotrienes and bradykinin, and the α"
adrenergic receptor agonists, although stimulating theirown cell surface receptor, all elicit a cellular response byactivating the same trimeric G-protein complex toactivate the transmitter Gq. Gq activation initiates theinflammatory process by the production of both inflam-matory lipids and peptides.
Competitive binding studies [13] using β"
and β#
adrenergic receptor antagonists showed both adrenergicreceptors to be present on the endothelium; 89% were β
#
receptors and 11% β"
receptors. The anti-inflammatoryeffect of isoproterenol is via the β
#receptor alone. It is
well established that β#
adrenergic receptor agonistsreduce the inflammatory response in sepsis, endotoxinand reperfusion injury in animal models. We haverecently reviewed [14] much of the work describing theanti-inflammatory effect of β
#adrenergic receptor
agonists. We described the reduction in both capillarypermeability and the production of inflammatory me-diators in monolayer preparations of endothelium, iso-lated organs and whole animals to inflammatory stimu-lation. We suggested that in endothelial cells, when thesecond messenger cytosolic cAMP is raised, an endogen-ous anti-inflammatory response is initiated, but inhi-bition of this endogenous response could cause anamplification of the inflammatory response.
We hypothesized that stimulation of α"
adrenergicreceptors or inhibition of β
#adrenergic receptors in this
animal model is very likely to amplify the inflammatoryresponse to sepsis and result in additional hepatic injury.Such a finding would be novel and could change ourunderstanding of the mechanism of the inflammatoryresponse and the action of adrenergic receptor agonists,especially when given during a major inflammatoryresponse.
Methoxamine is a specific α"
adrenergic receptoragonist with no record of tissue injury when normalblood flow is maintained. The specific β
#adrenergic
receptor antagonist ICI 118551 has been used extensivelyin animal studies [15,16] and β adrenergic receptorantagonists (e.g. propranolol) are used extensively inclinical practice ; neither have a record of tissue injury.
To provide data for our hypothesis we infused thesetwo agents in our established septic porcine model ofhepatic injury for 8 h, measuring cardiac output andportal blood flow. Portal blood flow was measured as anindex of hepatic blood flow. We have previously meas-ured both portal blood flow and hepatic artery bloodflow to calculate total blood flow. Our experience hasshown that hepatic artery measurement is unnecessary, asincreasing total blood flow does not provide hepaticprotection during sepsis in this animal model. In pigs,hepatic artery blood flow accounts for about 15% oftotal flow; if hepatic artery blood flow reduces there isusually a compensatory increase from the portal vein tomaintain total hepatic blood flow. Our previous study [5]
# 1998 The Biochemical Society and the Medical Research Society

469Adrenoceptor agonist and antagonist in sepsis
shows that total hepatic blood flow is primarily de-pendent on cardiac output.
In the non-septic methoxamine group cardiac outputand portal blood flow were also measured to prevent afall in these parameters. Surgical interventions such as alaparotomy have known associations with major changesin leucocyte function. Experience of this surgical pro-cedure combined with gut manipulation when insertingflow probes stimulate a considerable increase in per-itoneal fluid leak requiring fluid infusion to maintainbaseline parameters. We avoid this intervention whenstudying control animals. An infusion of ICI 118551 isnot associated with major vasoactive effects so it wasunnecessary to perform a laparotomy in the non-septicgroup treated with ICI 118551. We also studied two non-infected groups: a control group with minimal inter-vention for normal histology and a non-septic groupwith similar criteria to the non-septic ICI 118551 group.
Morphometric analysis was performed on hepatictissue removed from these animals after 8 h of sepsis. Theevidence provided by this study supports the hypothesisthat α
"adrenergic receptor agonists are pro-inflam-
matory only during the septic response. Inhibition of β#
adrenergic receptors potentiates the inflammatory re-sponse to sepsis and amplifies hepatic ultrastructuraldamage.
METHOD
The study was authorized by the U.K. Secretary of Stateunder the provisions of the 1986 Animals (ScientificProcedures) Act. The number of pigs in each group waskept to a minimum because of the high cost involved inlarge animal studies and the unnecessary use of animals inmedical research, in line with current thoughts on animalwelfare. Anaesthesia was induced with azaperone(2.0 mg}kg intramuscularly) and metomidate (10 mg}kgintraperitoneally) in 31 Middle White adolescent pigsweighing 25–30 kg. Sterile conditions were maintainedthroughout the study in all groups. The pigs were placedon the operating table and a face mask used to administeroxygen, nitrous oxide and isoflurane. A tracheotomy wasperformed to maintain anaesthesia during the surgicalprocedure and multi-bore catheters were inserted intothe internal jugular vein for fluid and drug infusion. Asingle-lumen catheter was inserted into the ear vein forlater anaesthetic administration. The study protocol isshown in Table 1.
Eleven of these animals had no more surgical inter-ventions performed and were divided into three groupsfor control hepatic histology. Five of these animals(control group) had hepatic tissue removed and werethen culled to demonstrate normal hepatic tissue. Threeanimals were infused with saline (15 ml[h−"[kg−") andlater culled and hepatic tissue removed (non-septic
Table 1 Interventions performed during the studyX ¯ intervention.
Treatment groups n Non-septic Laparotomy Septic
Control 5 XNon-septic 3 XNon-septicICI 118551 3 XNon-septicmethoxamine 5 X XSeptic 5 X XSepticICI 118551 5 X XSepticmethoxamine 5 X X
group) to show the effect of 8 h of anaesthesia. Threewere infused with saline and a bolus of the β
#adrenergic
receptor antagonist ICI 118551 (200 mg}kg, followed bya similar hourly infusion) and observed for 8 h when theywere culled and hepatic tissue removed (non-septicICI118551 group) to demonstrate the effect of ICI 118551 innon-septic, non-traumatized anaesthetized animals.Although ICI 118551 has been used in many studies itwas necessary to have a non-infected control group tocheck for toxicity. These three groups of animals did nothave a laparotomy performed for the reasons mentionedearlier and it was unnecessary to measure the haemo-dynamics.
Twenty animals had additional catheters inserted; intothe descending aorta via the femoral artery for bloodsampling and arterial blood pressure monitoring. Aballoon-tipped thermodilution catheter was inserted intothe femoral vein and advanced into the pulmonary arteryunder pressure control to measure pulmonary arteryocclusion pressure (PAOP), right atrial pressure andcardiac output. A midline laparotomy was performedand an ultrasound flow probe was placed around thehepatic portal vein. In 15 animals an incision was made inthe caecum, 35 ml of the contents was aspirated and theincision closed. During the course of surgery, saline wasinfused (approximately 12–15 ml[min−"[kg−") to main-tain normal physiological parameters.
When surgery was completed in all animals anaesthesiawas changed to ketamine (5 mg}kg) and xylazine(1 mg}kg), and mechanical ventilation initiated with theFiO
#maintained at approximately 0.4. Tidal volume was
adjusted to maintain pCO#
at approximately 40 mmHgand a 30-min stabilization period was observed.
These twenty animals were divided into four groups.One group was kept non-septic and methoxamineinfused (non-septic methoxamine group) to establishhistological changes associated with the infusion of thisspecific α
"agonist. Unlike the other control animals this
group was instrumented to maintain blood flow, es-pecially portal blood flow, at or above basal levels becauseof the real danger of splanchnic and hepatic hypoxiawhen using this vasoactive drug. In the other threegroups sepsis was induced by spreading the caecal
# 1998 The Biochemical Society and the Medical Research Society

470 D. Tighe, R. Moss and D. Bennett
aspirant into the peritoneum. The other three groupswere divided into the septic group where only saline wasinfused, the septic methoxamine group and the septic ICI118551 group. All methoxamine-treated animals received80 mg}h and all ICI 118551-treated animals received abolus of 200 mg}kg followed by a similar hourly in-fusion.
Colloid in the form of hydroxyethyl starch was infusedto maintain the PAOP at 10–12 mmHg in the septic andsepticICI 118551 groups. In the methoxamine-treatedanimals colloid infusion was adjusted to maintain portalblood flow above the basal value of 650 ml}min. Theconcentration of drug infused was also reduced period-ically to maintain haemodynamic parameters when fluidadjustment alone would not suffice. Methoxamine in-fusion caused initial vasoconstriction but after an hour inthe septic group this effect was considerably reduced anddid not represent a problem. Haemodynamic parameterswere measured hourly. After 8 h of study tissue coresamples 2 mm in diameter were taken from at least 10different areas of the liver using a BARD Biopsy-Cutfitted with a 14G biopsy needle (Bard Limited, Crawley,Sussex, UK.) and fixed in 3% glutaraldehyde in caco-dylate buffer. The animals were then culled. Haemo-dynamic parameters at 8 h only are presented for the sakeof clarity. All the hourly data for each parameter duringthe study are available.
Systemic, right atrial and pulmonary artery occlusionpressures were recorded on an Ormed polygraph(Lectromed, Jersey, U.K.) using disposable transducers(Baxter Healthcare). These transducers were electricallycalibrated at the beginning of the study and then hourlyfor its duration. A thermodilution computer (Edward’sLaboratories, California, U.S.A.) was used to measurecardiac output by calculating the mean of three injectionsof 10 ml of iced physiological saline injected randomlyduring the respiration cycle. Portal vein blood flow wasmeasured using an ultrasound flow probe (TransonicSystems, Ithaca, NY, U.S.A.). The flow probe wascalibrated by passing blood at known flow rates throughan excised blood vessel. Zero values were established byclamping the vessels for a short period at the beginning ofthe study and checked at the end. Blood gas analysis wasperformed on arterial blood using a 1306 IL machine(Instruments Laboratory, Milan, Italy). The 1306 ILblood gas analyser was calibrated with each set ofmeasurements. Standard formulae were used to calculatesystemic vascular resistance.
Hepatic tissue was post-fixed in buffered 1% osmiumtetroxide, dehydrated through ascending concentrationsof ethanol and embedded in Spurr’s resin. Semi-thin resinsections (2 µm) of hepatic tissue were prepared for lightmicroscopy, mounted on glass slides, coded and ran-domized so that the observer was unaware of the studygroups. They were viewed using a light microscope andvideo monitor at a magnification of 800; 10 consecutive
areas on each slide were captured and digitized by pixelcounting, using the N.I.H. image analysis programme(public domain freeware). The areas digitized were :endothelial area (area occupied by endothelium), peri-sinusoidal area (the area between the endothelium andhepatocytes), vacuolation area (area of open membrane-bound cytosolic vacuoles within hepatocyte cells). Aleucocyte count per sinusoid was taken.
Statistical analysisHaemodynamic data were analysed by single-factoranalysis of variance after 8 h of infection to comparedifferences among the groups at the time hepatic tissuewas taken. Morphometric data were not normally dis-tributed and a logarithmic transformation was per-formed. The data were analysed by single-factor analysisof variance. All tests were two-tailed with a P ! 0.05considered significant. Summary data are expressed asmeans and S.D.
RESULTS
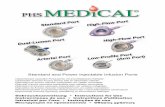
Hepatic histologyThe severity of the hepatic histological changes in thisstudy can be seen in the micrographs of Figure 1. Hepatictissue taken from the control group showed patentsinusoids lined by a thin endothelium overlaying adistinct narrow perisinusoidal Space of Disse and theapical microvillus hepatocyte surface. Within the sinusoidlumen were free-flowing erythrocytes, lymphocytes andneutrophils. The hepatocytes were normal, containingwithin their cytoplasm distinct mitochondria and bothrough and smooth endoplasmic reticulum.
Tissue taken from the septic group showed derangedmorphology. In the sinusoid lumen there were occlusiveplugs of lymphocytes, polymorphonuclear leucocytes,platelets, cellular debris, membranous ghosts and oc-clusive spherical erythrocytes. Both the swollen en-dothelium and activated Kupffer cells bulged into thesinusoid and often occluded the sinusoid lumenappearing to trap platelets and leucocytes. Single-membrane-bound vacuoles containing granuloreticularmaterial were visible in both endothelial and Kupffercells. The perisinusoidal Space of Disse was eitherindistinct or absent as the swollen endothelium ortrapped luminal leucocytes flattened the hepatocyteapical microvilli. The hepatocytes showed swollen,granular indistinct mitochondria and both normal anddilated irregular forms of endoplasmic reticulum. Therewas the occasional presence of single-membrane-boundvacuoles in the cytoplasm. The platelets were activatedand had many pseudopods.
In tissue taken from the septic ICI 118551 group thesinusoid lumen contained lymphocytes, polymorpho-nuclear leucocytes, platelets and spherical erythrocytes.
# 1998 The Biochemical Society and the Medical Research Society

471Adrenoceptor agonist and antagonist in sepsis
Figure 1 Histological changes in hepatic biopsies from control and septic groups(A) Control group. Narrow patent sinusoids (S) are lined by a thin fenestrated endothelium (end), overlaying a perisinusoidal Space of Disse (D) and containing withinthe lumen free-flowing erythrocytes [red blood cells (rbc)]. The surrounding hepatocytes (H) show both normal mitochondria (m) and rough endoplasmic reticulum (er).Magnification ¬3200. (B) Septic group. The sinusoid (S) is lined by swollen endothelium (end), reducing and making indistinct the Space of Disse. Within the lumenare swollen erythrocytes (rbc) and an occlusive neutrophil (pmn). The surrounding hepatocytes (H) show swollen mitochondria (m) and dilated rough endoplasmicreticulum (er). Magnification ¬3200. (C) Septic ICI 118551 group. The sinusoid (S) is lined by irregular endothelium (end) and a Kupffer cell (Kc). The perisinusoidalSpace of Disse (D) is greatly enlarged and has an extravasated swollen erythrocyte (rbc). Within the lumen is an occlusive activated platelet (pl) with pseudopodia. Thesurrounding hepatocytes (H) show swollen mitochondria (m) and dilated rough endoplasmic reticulum (er). Magnification ¬3200. (D) Septic methoxamine group. Thesinusoid (S) is lined by irregular endothelium (end) with an enlarged perisinusoidal Space of Disse (D). Within the lumen are swollen erythrocytes (rbc), cell debris andgranular protein precipitates. The surrounding hepatocytes (H) show extensive vacuolation (v) having within similar granular protein precipitates, swollen lucentmitochondria (m) and dilated rough endoplasmic reticulum (er). Magnification ¬2700.
# 1998 The Biochemical Society and the Medical Research Society

472 D. Tighe, R. Moss and D. Bennett
Table 2 Morphometric analysis of the ultrastructure of hepatic tissueThe letter in column 4 is used to identify the treatment group. When a letter appears in column 5 it denotes those treatmentgroups that are statistically significant (P ! 0.05) compared with the treatment group in column 4, e.g. leucocyte numberin the non-septic methoxamine group (a) is significantly different from the septic group (c) and the septicICI 118551 group(e). Meth ¯ methoxamine ; ICI ¯ ICI 118851.
Variable Treatment Value Statistic
Leucocyte no./sinusoid Non-septic meth 2.08 (0.36) a ceSeptic meth 2.8 (0.49) b cdefgSeptic 4.70 (1.4) c abdfgControl 1.48 (0.4) d bceSeptic ICI 4.72 (23.1) e abdfgNon-septic 1.57 (0.81) f bceNon-septic ICI 1.53 (0.92) g bce
Endothelium (µm2) Non-septic meth 286 (43) a cdSeptic meth 367 (96) b dSeptic 418.0 (107.1) c adfControl 197.0 (31.0) d abcegSeptic ICI 393.6 (151.2) e dfNon-septic 250 (69) f ceNon-septic ICI 325 (34) g d
Perisinusoidal area (µm2) Non-septic meth 55 (101) a beSeptic meth 377 (268) b adcfgSeptic 134.0 (203.3) c bdefControl 0.8 (1.9) d bceSeptic ICI 347.4 (340.2) e acdfgNon-septic 0 (0) f bceNon-septic ICI 12 (20) g be
Vacuolation (µm2) Non-septic meth 47 (67) a bdfSeptic meth 242 (120) b acdefgSeptic 48.5 (68.3) c bdfControl 0 (0) d abcSeptic ICI 2.2 (4.9) e bNon-septic 0 0 f abcNon-septic ICI 2 (3) g b
The sinusoids were lined by an irregular endotheliumwith enlarged Space of Disse. The enlarged perisinusoidalarea contained extravasated erythrocytes and cell debris.The apical membrane of the hepatocytes was frequentlydisrupted with their contents spilling into the peri-sinusoidal space. The surrounding hepatocytes containedswollen mitochondria and dilated rough endoplasmicreticulum. They were often separated from their neigh-bouring hepatocytes downwards from the apical surface.
In hepatic tissue taken from the septic methoxaminegroup the sinusoidal endothelium showed some areas ofswelling but maintained its integrity. The lumen con-tained many erythrocytes, leucocytes and platelets ap-pearing to flow normally. The perisinusoidal Space ofDisse was enlarged, separating it from the frequentlydamaged apical hepatocyte surface where the plasmamembrane was often ruptured allowing cell contents tospill into the perisinusoidal area. Hepatocytes were oftenseparated from each other and contained in the cytoplasm
along with swollen mitochondria, many single-membrane-bound vacuoles containing granular material.
Morphometric analysis of the ultrastructureof hepatic tissueThe numerical and statistical changes are presented inTable 2. Leucocyte numbers in all the non-septic groupswere similar to the control group. The septic andsepticICI 118551 groups had significantly highernumbers than all the other groups including septicmethoxamine. Methoxamine infusion was associatedwith an attenuation of hepatic leucostasis during sepsis.Leucocyte numbers in the septic methoxamine groupwere significantly higher than in control, non-septic ornon-septic ICI groups but not the non-septic methox-amine group.
Endothelial area in the control group was significantlylower than both uninfected groups (non-septic methox-amine or non-septic ICI 118551) and the three infected
# 1998 The Biochemical Society and the Medical Research Society

473Adrenoceptor agonist and antagonist in sepsis
Table 3 Haemodynamic measurements at the time hepatic tissue was removedStatistical significance (P ! 0.05) is demonstrated when the assigned letter in column 4 is compared with the letter(s) incolumn 5 (see legend of Figure 2 for details). Meth ¯ methoxamine ; ICI ¯ ICI 118551.
Variable Treatment Value Statistic
Mean arterial Septic 74 (26) a cpressure (mmHg) Septic ICI 73 (6) b c
Non-septic meth 105 (11) c abSeptic meth 84 (20) d
PAOP (mmHg) Septic 10.2 (3.2) a cdSeptic ICI 11.4 (1.5) b cdNon-septic meth 15.6 (1.5) c abdSeptic meth 21.4 (3.6) d abc
Cardiac output (l/min) Septic 3.28 (0.5) a bSeptic ICI 5.3 (1.9) b aNon-septic meth 3.9 (1.0) cSeptic meth 3.6 (0.3) d
Stroke volume resistance Septic 1518 (443) a(dyne[s−1[cm−5) Septic ICI 1004 (482) b c
Non-septic meth 2054 (856) c bSeptic meth 1468 (517) d
Stroke volume Septic 33.9 (5.1) a b(ml/min) Septic ICI 47.9 (14.4) b acd
Non-septic meth 34.2 (7.3) c bSeptic meth 30.5 (3.0) d b
Portal blood flow Septic 668 (148) a b(ml/min) Septic ICI 992 (244) b a
Non-septic meth 795 (403) cSeptic meth 804 (101) d
Heart rate (beats/min) Septic 98 (21) aSeptic ICI 111 (21) bNon-septic meth 114 (29) cSeptic meth 120 (11) d
Fluid (ml/8 h) Septic 4248 (2684) aSeptic ICI 6342 (3022) bNon-septic meth 4610 (2893) cSeptic meth 4332 (1624) d
groups (septic, septic methoxamine or septic ICI 118551).Endothelial area in the septic group was significantlyhigher than in all the non-septic groups except non-septicICI 118551. Neither methoxamine nor ICI 118551 hadany effect on endothelial area during sepsis.
Perisinusoidal area in all the non-septic groups wassimilar and significantly lower than either septic methox-amine or septic ICI 118551. The septic group values weresignificantly higher than those in the control or non-septic groups but significantly lower than in the septicmethoxamine or septic ICI 118551 groups. Values in theseptic methoxamine and septic ICI 118551 groups weresimilar and significantly higher than in all the othergroups. Both of these agents caused a separation ofendothelium from the hepatocytes and the hepatocytesfrom each other.
Hepatocyte vacuolation was similar and at a very low
level in the control, non-septic, non-septic ICI 118551and septic ICI 118551 groups, but levels in the non-septicmethoxamine group and the septic group were signifi-cantly higher than in either the control group or the non-septic group. The septic group and non-septic methox-amine groups had significantly less hepatocyte vacuo-lation than the septic methoxamine group. The septic ICI118551 group had significantly less vacuolation thaneither of the two methoxamine-treated groups. Hepat-ocyte vacuolation in the septic methoxamine group wassignificantly higher than in all the other groups.
HaemodynamicsHaemodynamic data were recorded after 8 h of sepsis atthe time hepatic tissue was removed for ultrastructuralanalysis and are presented in Table 3. The mean arterialpressure in the non-septic methoxamine group was
# 1998 The Biochemical Society and the Medical Research Society

474 D. Tighe, R. Moss and D. Bennett
significantly higher than either the septic or septic ICIgroups. In the septic methoxamine group mean arterialpressure was not different to any of the other groups. Itis important to stress that although the mean arterialpressure in the non-septic methoxamine group wassignificantly higher than in the septic group, mean arterialpressure in the septic methoxamine group was notdifferent to that in the septic group. The septic animalswere becoming refractory to the vasoactive effect of thedrug. The PAOP in the non-septic methoxamine andseptic methoxamine groups was significantly higher thanin the septic or septic ICI 118551 groups. The PAOP inthe septic methoxamine group was also significantlyhigher than in the non-septic methoxamine group. Thecardiac output in the septic ICI 118551 group wassignificantly higher than in the septic group; otherwise itwas similar in all the other groups where it was recorded.In the septic methoxamine group the combination of asignificantly higher PAOP without an increase in cardiacoutput is suggestive of heart failure induced by methox-amine. The stroke volume in the septic ICI 118551 groupwas significantly higher than in the septic, non-septicmethoxamine or septic methoxamine groups. The sys-temic vascular resistance in the non-septic methoxaminegroup was significantly higher than in the septic ICI118551 group; otherwise there was little difference in thisparameter among the other groups. Sepsis has a profoundeffect on reducing stroke volume resistance that was notantagonized by the vasoactive effect characteristic ofmethoxamine. Portal blood flow in the septic ICI 118551group was significantly higher than in the septic group.There were no significant differences in heart rate or fluidadministration in any of the groups.
DISCUSSION
The data in this study address the question of whether anα"
adrenergic receptor agonist or a β#
adrenergic receptorantagonist are pro-inflammatory when administeredduring sepsis. The question was examined by morpho-metric analysis of the hepatic changes seen in a septicporcine model of organ damage. In sepsis both agentswere found to increase hepatic injury to tissue elementsnot normally observed in sepsis alone. The α
"adrenergic
receptor agonist also has detrimental effects on myo-cardial performance during sepsis, causing considerableheart failure.
The question was identified as important when it wasfound [5] that during sepsis, although hepatic blood flowwas maintained 30% above the basal level, dobutamineinfusion was associated with increased hepatic injury, butwhen dopexamine was infused hepatic injury was lessthan that observed in sepsis alone. We described in theintroduction one of the differences between dopexamineand dobutamine, which is the α
"adrenergic receptor
agonist of dobutamine; both dopexamine and dobut-amine are adrenergic β agonists. It is well established thatβ#
adrenergic receptor agonists induce an anti-inflam-matory response when an organism is challenged withpro-inflammatory agents [14]. When an endothelialmonolayer, isolated organ or a whole animal arechallenged with inflammatory mediators such as his-tamine, thrombin, leukotrienes or bradykinin, adrenergicβ#
agonists such as salbutamol or isoprenaline attenuatethe inflammatory response. It was likely that β
#adren-
ergic receptor stimulation was the characteristic ofdopexamine that rendered it anti-inflammatory in ourstudy. It is assumed that adrenergic β
#agonists stimulate
a pre-existing endogenous anti-inflammatory cellularresponse initiated by cell-surface receptor activation andmembrane transduction to inhibit or control the cytosolicpathway of inflammatory mediator production. Thereseemed little point in duplicating the earlier workdemonstrating the anti-inflammatory characteristics ofthese agents. Blockade of the supposed endogenous β
#
adrenergic receptor-stimulated anti-inflammatory cellu-lar response had not been reported previously.
Methoxamine is a specific α1 adrenergic receptoragonist whereas ICI 118551 is a specific β
#adrenergic
receptor antagonist. A detailed morphometric analysis ofhepatic components and their changes in sepsis withmethoxamine or ICI 118551 was made, and the resultscompared with septic and non-septic hepatic tissuesamples taken from our pig model both with and withoutthese adrenergic receptor agents.
In this animal study there was considerable deterio-ration in hepatic ultrastructure in septic animals. How-ever, in those septic animals infused with either ICI118551 or methoxamine there was further significantdeterioration. There were significant differences in thehepatic ultrastructure in the four groups of animals butthe portal blood flow measured in the septic groups orthe non-septic methoxamine group was either similar tobaseline values or higher. There was no correlationbetween the reported portal blood flow and changes inthe hepatic ultrastructure ; portal blood flow measured inthis study did not seem to be an important parameter indetermining changes in the hepatic ultrastructuralelements.
Deterioration in perivascular elements was similarwhen the two agents being investigated were infused.Administration of the β
#adrenergic receptor antagonist
or the α"
adrenergic receptor agonist during sepsis wasassociated with considerable deterioration inhepatocyte}hepatocyte and hepatocyte}endothelial ad-hesion. Some hepatocytes had damage to their apicalmembrane but damage to the plasma membrane separ-ating the hepatocytes was not seen. This finding suggeststhat the hepatocytes had lost their ability to adhere toeach other either because their binding site was blockedor, more likely, the cytosolic production of adhesion
# 1998 The Biochemical Society and the Medical Research Society

475Adrenoceptor agonist and antagonist in sepsis
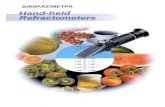
Scheme 1 Inflammatory cell transduction pathway initiated by α1 adrenoceptor agonistPLC, phospholipase C ; IP3, inositol trisphosphate ; DAG, diacylglycerol ; PLA2c, cytosolic phospholipase A2 ; LTB, leukotriene ; TBX, thromboxane ; PAF, platelet-activatingfactor ; MAP kinase, mitogen-activated protein kinase ; NF-κB, nuclear factor κB ; Iκ-B, NF-κB inhibitor.
molecules especially the cadherins [17] was inhibited. Inthe septic methoxamine-treated animals it is possible thatthe production of all types of adhesion molecules hadbeen inhibited as demonstrated by the significant lack ofsinusoidal leucostasis.
In the septic methoxamine group but not in the septicICI 118551 group, significant hepatocyte vacuolationwas observed. The hepatocytes showed a substantialnumber of membrane-lined vacuoles, giving the micro-scopic sections of the liver an appearance of ‘Swiss
cheese ’. These changes represent a substantial deterio-ration of the hepatic ultrastructure compared with thesepsis group.
Methoxamine is an α"
adrenergic receptor agonist withno record of cellular damage when blood flow ismaintained. α
"adrenergic receptor agonists are not
normally associated with inflammatory changes inphysiological preparations but do have characteristics incommon with inflammatory mediators such as thrombin,bradykinin and leukotrienes. Although they all activate
# 1998 The Biochemical Society and the Medical Research Society

476 D. Tighe, R. Moss and D. Bennett
their own cell-surface receptors, their cell response isachieved by the stimulation of the common trimericG-protein complex [12,18] and formation of the cellmembrane transmitter Gq described in Scheme 1. Gqactivates phospholipase C which increases diacylglyceroland inositol triphosphate ; intracellular calcium concen-tration is raised by the formation of inositol triphosphate[14] and inflammatory lipids are produced by the actionof diacylglycerol and the activation of calcium-dependentcytosolic phospholipase A2. Diacylglycerol also activatesprotein kinase C that phosphorylates nuclear factor-κBinhibitor, releasing nuclear factor-κB. Inflammatorypeptides such as cytokines are produced by the activationof the gene transcription factors mitogen-activated pro-tein kinase and nuclear factor-κB. Activation of Gq isintimately involved in the activation of the inflammatoryprocess, increasing cytosolic calcium, and the productionof both inflammatory lipids and peptides.
α"
Adrenergic receptor agonists such as methoxamineare known to cause constriction of smooth muscle andprecipitate vasoconstriction by raising intracellular cal-cium. A similar system is also present in endothelial cellswhen the actin}myosin cytoskeleton is activated to causecell contraction and increase capillary permeability.When inositol triphosphate is released into the cytosol itincreases the permeability of endoplasmic reticulum andthe plasma membrane to calcium allowing its rapid influxinto the cell. This increase in cytosolic calcium, althoughphysiological, is associated with major changes in cellularactivity depending on the cell type. High levels of calciumin the cytosol are toxic to the cell and quickly cause itsdeath. The uptake of calcium by the mitochondria, usedas a ‘sink’ to reduce calcium levels, is associated withuncoupling of respiration and irreversible destruction[19]. Raised cytosolic calcium is important in many of thesteps of the signal transduction cascade activated by thepro-inflammatory mediators mentioned earlier to pro-duce inflammatory lipids and peptides. The hepatocytevacuoles that we have described may contain calcium andrepresent an attempt by the cell to reduce cytosoliccalcium concentration.
This is the first report showing that the characteristicsof a drug are radically changed when there is a majorinflammatory response to tissue injury. We have pre-viously reported that dobutamine infusion during sepsisis associated with major hepatic injury similar to thechanges seen in the methoxamine-treated animals. It ishighly likely that the α
"adrenergic receptor agonist
properties of dobutamine cause the hepatic injury wheninfused during sepsis. A recent publication by Le Tulzoet al. has shown the importance of α adrenergic receptorblockade in reducing the inflammatory response to tissueinjury [20]. Phentolamine administration in haemor-rhagic mice prevented the rise in mRNA level ofinterleukin (IL)-1, tumour necrosis factor and the ac-tivation of the gene transcription factor nuclear factor-κB
normally seen with this haemorrhagic animal model.Propranolol pretreatment caused an increase in thesefactors, greater than haemorrhage alone, that might beassociated with greater deterioration of organ function inthis animal model.
We have previously shown [5] that hepatic ultra-structural protection is produced by dopexamine associ-ated with its β
#adrenergic receptor agonist properties. It
seems likely that there is an endogenous anti-inflam-matory response to sepsis mediated by β
#adrenoceptor
agonists on the cell surface that can be inhibited by ICI118551. Amplification of hepatic injury in these septicanimals treated with ICI 118551 confirms the presence ofa β
#adrenergic receptor-mediated endogenous anti-
inflammatory response to tissue injury.There is considerable research documentation re-
porting that β#
adrenergic receptor agonists reduce thetissue response to inflammatory mediators by bothreducing capillary permeability and inhibiting the pro-duction of further inflammatory mediators. Severalreports describe how a second messenger of membranetransduction cAMP or protein kinase A, activated whenGs is formed from β
#adrenergic receptor activation,
inhibits the activation of phospholipase C and the genetranscription factor mitogen-activated protein kinase (seeScheme 2). Inhibition of membrane-bound phospho-lipase C reduces the production of inflammatory lipidsand the transcription of inflammatory peptides [21].
Szabo et al. [22] described how pretreatment of ratswith isoproterenol blunted the lipopolysaccharide-induced increase in tumour necrosis factor and nitricoxide production but increased the IL-10 response (ananti-inflammatory cytokine). In a model of inflammation[23] bradykinin infusion was used to stimulate theintracellular production of phospholipase C, inositoltrisphosphate, diacylglycerol and arachidonic acid.Arginine vasopressin, forskolin and isobutylmethyl-xanthine were infused to increase cAMP levels andstimulate protein kinase A production. An increasedcellular concentration of protein kinase A was associatedwith an inhibition of the inflammatory response tobradykinin with a reduction of the transmembranemediators of inflammation, especially phospholipase C,inositol trisphosphate and diacylglycerol.
We have recently reviewed [14] the importance of β#
adrenergic receptor agonists during the inflammatoryresponse to sepsis and the mechanism of cell protection.The cytokine IL-10 is produced during the inflammatoryprocesses, usually by the same cells that release inflam-matory cytokines. It is a potent anti-inflammatorymolecule which inhibits the synthesis of pro-inflam-matory cytokines (tumour necrosis factor, IL-1, IL-6 andIL-8) by monocytes, macrophages [24], neutrophils [25]and eosinophils [26]. Interleukin-10 suppresses freeoxygen radical release and nitric oxide-dependent micro-bicidal activity of macrophages as well as their production
# 1998 The Biochemical Society and the Medical Research Society

477Adrenoceptor agonist and antagonist in sepsis
Scheme 2 Endogenous anti-inflammatory cell transduction pathway initiated by β2 adrenoceptor agonistsCRE, cyclic AMP response element ; IL-10, interleukin 10.
of prostaglandins [27–30]. It inhibits the production ofthese inflammatory cytokines by a negative-feedbackmechanism. Endogenous production of IL-10 can beincreased by several pharmacological compounds whichelevate intracellular cAMP [31]. There appears to be apromoter sequence on the IL-10 gene [32] to the cAMPresponse element (CRE) that binds to the gene tran-scription factor CRE binding factor (CREB). β
#Agonists
have recently been shown to increase production of IL-10 from monocytes challenged with endotoxin [33].
The clinical significance of these findings is that, inseptic patients, α
"adrenergic receptor agonists such as
noradrenaline or dobutamine, used to stimulate car-diovascular function and tissue perfusion as well asmaintain arterial blood pressure in hypotensive patients,may cause hepatic dysfunction and increase mortality inan already high-risk group of patients. These findingsmay explain the high mortality that is seen in septic
patients with end-organ failure who exhibit significanthepatic dysfunction.
β#
Adrenergic receptor agonists activate the endothelialcell transduction process to initiate an endogenous anti-inflammatory response in sepsis [14] that can be sig-nificantly attenuated by the β
#adrenergic receptor
antagonist ICI 118551. ICI 118551 is associated with anamplification of the inflammatory response when infusedduring sepsis. This paper also presents evidence thatendogenous β
#adrenergic receptor agonists produce an
anti-inflammatory response and may give some pro-tection against the tissue injury associated with severeinflammation caused by sepsis. The α
"agonists can
amplify the inflammatory response to sepsis even whenblood flow is maintained. These data provide evidencethat adrenergic receptor agonists are important in modi-fying the cellular response to inflammation, sepsis or thesystemic inflammatory response syndrome.
# 1998 The Biochemical Society and the Medical Research Society

478 D. Tighe, R. Moss and D. Bennett
REFERENCES
1 Ziegler, E. J., Fisher, C. J., Sprung, C. L. et al. (1991)Treatment of Gram-negative bacteremia and septic shockwith HA-1A human monoclonal antibody againstendotoxin. A randomized, double-blind, placebo-controlled trial. The HA-1A Sepsis Study Group [seecomments]. N. Engl. J. Med. 324, 429–436
2 Abraham, E., Wunderink, R., Silverman, H. et al. (1995)Efficacy and safety of monoclonal antibody to humantumor necrosis factor-alpha in patients with sepsissyndrome. J. Am. Med. Assoc. 273, 931–934
3 Fisher, C. J., Dhainaut, J.-F. A., Opal, S. M. et al. (1994)Recombinant human interleukin-1 receptor antagonist inthe patients with sepsis syndrome: results from arandomized, double blind, placebo-controlled trial. J. Am.Med. Assoc. 272, 1170
4 Tighe, D., Moss, R., Hynd, J., et al. (1990) Pretreatmentwith pentoxifylline improves the hemodynamic andhistologic changes and decreases neutrophil adhesiveness ina pig fecal peritonitis model [see comments]. Crit. CareMed. 18, 184–189
5 Tighe, D., Moss, R., Heywood, G. et al. (1995) Goaldirected therapy with dopexamine, dobutamine andvolume: effects of systemic oxygen transport on hepaticultrastructure in porcine sepsis. Crit. Care Med. 23,1997–2007
6 Brown, R. A., Farmer, J. B., Hall, J. C. et al. (1985) Theeffects of dopexamine on the cardiovascular system of thedog. Br. J. Pharmacol. 85, 609–619
7 Brown, R. A., Dixon, J., Farmer, J. B. et al. (1985)Dopexamine: a novel agonist at peripheral dopaminereceptors and β2-adrenoceptors. Br. J. Pharmacol. 85,599–608
8 Kenakin, T. P. (1980) An in vitro qualitative analysis of thealpha adrenoceptor partial agonist activity of dobutamineand its relavance to inotropic selectivity. J. Pharmacol.Exp. Ther. 216, 210–219
9 Ruffolo, R. J., Spradlin, T. A., Pollock, G. D. et al. (1981)Alpha and beta adrenergic effects of the stereoisomers ofdobutamine. J. Pharmacol. Exp. Ther. 219, 447–452
10 Ruffolo, R. J. and Messick, K. (1985) Inotropic selectivityof dobutamine enantiomers in the pithed rat. J. Pharmacol.Exp. Ther. 235, 344–348
11 Kenakin, T. P. and Johnson, S. F. (1985) The importanceof the alpha-adrenoceptor agonist activity of dobutamineto inotropic selectivity in the anaesthetized cat. Eur. J.Pharmacol. 111, 347–354
12 Minneman, K. P. (1988) Alpha 1-adrenergic receptorsubtypes, inositol phosphates, and sources of cell Ca#+[Review]. Pharmacol. Rev. 40, 87–119
13 Minnear, F. L., DeMichele, M. A., Leonhardt, S. et al.(1993) Isoproterenol antagonizes endothelial permeabilityinduced by thrombin and thrombin receptor peptide. J.Appl. Physiol. 75, 1171–1179
14 Tighe, D., Moss, R. and Bennett, D. (1996) Cell surfaceadrenergic receptor stimulation modifies the endothelialresponse to SIRS. New Horizons 4, 426–442
15 Winter, R. J., Dickinson, K. E., Rudd, R. M. et al. (1986)Tissue specific modulation of β-adrenoceptor number inrats with chronic hypoxia with an attenuated response todown-regulation by salbutamol. Clin. Sci. 70, 159–165
16 Levy, F. O., Zhu, X., Kaumann, A. J. et al. (1993) Efficacyof beta 1-adrenergic receptors is lower than that of β2-adrenergic receptors. Proc. Natl. Acad. Sci. U.S.A. 90,10798–10802
Received 28 January 1998/29 April 1998; accepted 15 May 1998
17 Lum, H. and Malik, A. B. (1994) Regulation of vascularendothelial barrier function [Review]. Am. J. Physiol. 267,L223–L241
18 Hung, D. T., Wong, Y. H., Vu, T. K. et al. (1992) Thecloned platelet thrombin receptor couples to at least twodistinct effectors to stimulate phosphoinositide hydrolysisand inhibit adenylyl cyclase. J. Biol. Chem. 267,20831–20834
19 Trump, B. F., Berezesky, I. K., Laiho, K. U. et al. (1980)The role of calcium in cell injury. A review. Scan. Elec.Micro. 492, 437–462
20 Le Tulzo, Y., Shenkar, R., Kaneko, D. et al. (1997)Hemorrhage increases cytokine expression in lungmononuclear cells in mice : involvement of catecholaminesin nuclear factor-kappaB regulation and cytokineexpression. J. Clin. Invest. 99, 1516–1524
21 Rhee, S. G., Lee, C. W. and Jhon, D. Y. (1993)Phospholipase C isozymes and modulation by cAMP-dependent protein kinase. Adv. Second MessengerPhosphoprotein Res. 28, 57–64
22 Szabo, C., Hasko, G., Zingarelli, B. et al. (1997)Isoproterenol regulates tumour necrosis factor,interleukin-10, interleukin-6 and nitric oxide productionand protects against the development of vascularhyporeactivity in endotoxaemia. Immunology 90, 95–100
23 Kennedy, C. R., Proulx, P. R. and Hebert, R. L. (1995)Regulation of bradykinin-stimulated phospholipase C andarachidonic acid release by protein kinase A in MDCK-D1cells. Biochim. Biophys. Acta. 1258, 206–214
24 Moore, K. W., O’Garra, A., de Waal, C. et al. (1993)Interleukin-10 [Review]. Ann. Rev. Immunol. 11, 165–190
25 Cassatella, M. A., Meda, L., Bonora, S. et al. (1993)Interleukin 10 (IL-10) inhibits the release ofproinflammatory cytokines from humanpolymorphonuclear leukocytes. Evidence for an autocrinerole of tumor necrosis factor and IL-1 beta in mediatingthe production of IL-8 triggered by lipopolysaccharide.J. Exp. Med. 178, 2207–2211
26 Takanaski, S., Nonaka, R., Xing, Z. et al. (1994)Interleukin 10 inhibits lipopolysaccharide-induced survivaland cytokine production by human peripheral bloodeosinophils. J. Exp. Med. 180, 711–715
27 Gazzinelli, R. T., Oswald, I. P., James, S. L. et al. (1992)IL-10 inhibits parasite killing and nitrogen oxideproduction by IFN-gamma-activated macrophages.J. Immunol. 148, 1792–1796
28 Cunha, F. Q., Moncada, S. and Liew, F. Y. (1992)Interleukin-10 (IL-10) inhibits the induction of nitric oxidesynthase by interferon-gamma in murine macrophages.Biochem. Biophys. Res. Commun. 182, 1155–1159
29 Mertz, P. M., DeWitt, D. L., Stetler, S. W. et al. (1994)Interleukin 10 suppression of monocyte prostaglandin Hsynthase-2. Mechanism of inhibition of prostaglandin-dependent matrix metalloproteinase production. J. Biol.Chem. 269, 21322–21329
30 Niiro, H., Otsuka, T., Kuga, S. et al. (1994) IL-10 inhibitsprostaglandin E2 production by lipopolysaccharide-stimulated monocytes. Int. Immunol. 6, 661–664
31 Platzer, C., Meisel, C., Vogt, K. et al. (1995) Up-regulationof monocytic IL-10 by tumor necrosis factor-alpha andcAMP elevating drugs. Int. Immunol. 7, 517–523
32 Strassmann, G., Patil, R., Koota, V., Finkelman, F. et al.(1994) Evidence for the involvement of interleukin 10 inthe differential deactivation of murine peritonealmacrophages by prostaglandin E2. J. Exp. Med. 180,2365–2370
33 van der Poll, T., Coyle, S. M., Barbosa, K. et al. (1996)Epinephrine inhibits tumor necrosis factor and potentiatesIL-10 production during human endotoxemia. J. Clin.Invest. 97, 713–719
# 1998 The Biochemical Society and the Medical Research Society