National Kidney Foundation Primer on Kidney Diseases || Minimal Change Disease
6
164 TERMINOLOGY AND HISTOPATHOLOGY Minimal change disease (MCD) is a common cause of the nephrotic syndrome (NS). Also known as lipoid nephrosis, nil disease, and minimal change nephropathy, the kidney his- tology on light microscopy in MCD is relatively normal and lacks the significant glomerular cell proliferation, infiltration by circulating immunoeffector cells, immune deposits, tubu- lointerstitial changes, or alterations in the glomerular base- ment membrane (GBM) that characterize other glomerular diseases. The defining feature of MCD is diffuse effacement and fusion of podocyte foot processes without electron-dense deposits on electron microscopy. Immunofluorescence is typ- ically negative or may show low-level staining for C3 and IgM. Although MCD is histologically defined by the previously mentioned criteria, it can also be diagnosed clinically by exhibiting responsiveness to corticosteroid treatment. In children, because MCD is the cause of 90% of cases of idio- pathic NS, a kidney biopsy is only warranted if the clinical and laboratory evidence, including disease onset before 6 months of age or following adolescence, unexpected sys- temic manifestations, or a low serum C3 level, suggests an alternative diagnosis. Children who do not exhibit these characteristics will typically have MCD and will consequently respond to steroids. The nomenclature “steroid-sensitive nephrotic syndrome (SSNS)” is also used to describe such children. Steroid responsiveness is a marker of a favorable long-term prognosis. In contrast, children with steroid- resistant nephrotic syndrome (SRNS) are more likely on subsequent kidney biopsies to show focal segmental glomer- ulosclerosis (FSGS), a disease that is associated with a worse prognosis. The causes of the NS in adults are more varied and include a higher percentage of cases with membranous nephropathy (MN) and membranoproliferative glomerulo- nephritis (MPGN). Because MCD only accounts for approx- imately 10% to 15% of cases, a kidney biopsy is usually warranted to establish the etiology of nephrotic syndrome. PATHOPHYSIOLOGY The pathogenesis of MCD is not well understood. The effacement of podocyte foot processes that is a hallmark of MCD may be mediated by various intracellular signaling pathways. For example, it has been demonstrated that mark- ers of focal adhesion complex–mediated Crk-dependent signaling are enhanced in MCD but not FSGS. Moreover, increased production of proteins such as CD80 and angio- poietin-like protein 4 by podocytes in MCD models supports the central role of podocyte damage in the pathogenesis of MCD. It has been thought that proteinuria occurs solely because of a defect in glomerular permselectivity, although alterations in tubular reabsorption may contribute. MCD is unique in that it predominantly reflects a decrease in the negative charge present in endothelial cells, the GBM, and podocytes, thereby causing selective protein- uria. The reduction in negative charge appears to be a dif- fuse abnormality that is manifest in capillaries throughout the body with leakage of albumin in the peripheral circula- tion and accumulation of interstitial fluid. The cause of the diminished negative charge density probably results from immune-mediated defects that inhibit sulfate incorporation into the GBM rather than a genetic mutation in a podocyte protein. In addition, immunoeffector cells may elaborate soluble molecules, such as vascular endothelial growth fac- tor, that directly increase GBM permeability to protein. It is likely that the molecular identity of circulating permeabil- ity factors that cause proteinuria will differ in patients with MCD and FSGS. This is supported by the recent report indi- cating that circulating levels of soluble urokinase receptor (suPAR) are elevated in nearly 70% of patients with FSGS, but they are undetectable in patients with MCD or MN. A link between abnormal T-cell function and MCD was initially proposed more than 30 years ago by Shalhoub, and many studies since then have documented altered subtype distribution and activity of lymphocytes in children with MCD. A recent study in which albuminuria and podocyte foot process effacement was induced by injection of CD34+ stem cells isolated from patients with MCD or FSGS into immunodeficient NOD/SCID mice underscores the pivotal role of the immune system in the pathogenesis of MCD. This role is supported by the finding of a higher Th17/Treg cell ratio in children with MCD. Minimal change disease represents a fascinating instance of organ dysfunction caused by a variable interaction between intrinsic structural defects and immunologic disturbances. Although MCD can occur in a familial pattern with both ver- tical and horizontal transmission, it has not been linked to mutations in any of the well-recognized proteins associated with FSGS, such as Wilms tumor-1, TRPC6, or α-actinin-4. Interestingly, there have been observations linking fre- quently relapsing childhood MCD to allelic heterogeneity in the gene for nephrin, a key component of the slit diaphragm and a major genetic locus for congenital NS. In addition, in a study of 214 Chinese patients with MCD, variants in the podo- cin gene were more common than in healthy controls, and they correlated with the level of urinary protein excretion. Alterations in histone H3 lysine 4 trimethylation in children Minimal Change Disease Howard Trachtman | Jonathan Hogan | Jai Radhakrishnan 17
Transcript of National Kidney Foundation Primer on Kidney Diseases || Minimal Change Disease
Minimal Change DiseaseHoward Trachtman | Jonathan Hogan | Jai Radhakrishnan
17
164
TERMINOLOGY AND HISTOPATHOLOGY
Minimal change disease (MCD) is a common cause of the nephrotic syndrome (NS). Also known as lipoid nephrosis, nil disease, and minimal change nephropathy, the kidney his-tology on light microscopy in MCD is relatively normal and lacks the significant glomerular cell proliferation, infiltration by circulating immunoeffector cells, immune deposits, tubu-lointerstitial changes, or alterations in the glomerular base-ment membrane (GBM) that characterize other glomerular diseases. The defining feature of MCD is diffuse effacement and fusion of podocyte foot processes without electron-dense deposits on electron microscopy. Immunofluorescence is typ-ically negative or may show low-level staining for C3 and IgM.
Although MCD is histologically defined by the previously mentioned criteria, it can also be diagnosed clinically by exhibiting responsiveness to corticosteroid treatment. In children, because MCD is the cause of 90% of cases of idio-pathic NS, a kidney biopsy is only warranted if the clinical and laboratory evidence, including disease onset before 6 months of age or following adolescence, unexpected sys-temic manifestations, or a low serum C3 level, suggests an alternative diagnosis. Children who do not exhibit these characteristics will typically have MCD and will consequently respond to steroids. The nomenclature “steroid-sensitive nephrotic syndrome (SSNS)” is also used to describe such children. Steroid responsiveness is a marker of a favorable long-term prognosis. In contrast, children with steroid-resistant nephrotic syndrome (SRNS) are more likely on subsequent kidney biopsies to show focal segmental glomer-ulosclerosis (FSGS), a disease that is associated with a worse prognosis. The causes of the NS in adults are more varied and include a higher percentage of cases with membranous nephropathy (MN) and membranoproliferative glomerulo-nephritis (MPGN). Because MCD only accounts for approx-imately 10% to 15% of cases, a kidney biopsy is usually warranted to establish the etiology of nephrotic syndrome.
PATHOPHYSIOLOGY
The pathogenesis of MCD is not well understood. The effacement of podocyte foot processes that is a hallmark of MCD may be mediated by various intracellular signaling pathways. For example, it has been demonstrated that mark-ers of focal adhesion complex–mediated Crk-dependent signaling are enhanced in MCD but not FSGS. Moreover, increased production of proteins such as CD80 and angio-poietin-like protein 4 by podocytes in MCD models supports
the central role of podocyte damage in the pathogenesis of MCD. It has been thought that proteinuria occurs solely because of a defect in glomerular permselectivity, although alterations in tubular reabsorption may contribute.
MCD is unique in that it predominantly reflects a decrease in the negative charge present in endothelial cells, the GBM, and podocytes, thereby causing selective protein-uria. The reduction in negative charge appears to be a dif-fuse abnormality that is manifest in capillaries throughout the body with leakage of albumin in the peripheral circula-tion and accumulation of interstitial fluid. The cause of the diminished negative charge density probably results from immune-mediated defects that inhibit sulfate incorporation into the GBM rather than a genetic mutation in a podocyte protein. In addition, immunoeffector cells may elaborate soluble molecules, such as vascular endothelial growth fac-tor, that directly increase GBM permeability to protein. It is likely that the molecular identity of circulating permeabil-ity factors that cause proteinuria will differ in patients with MCD and FSGS. This is supported by the recent report indi-cating that circulating levels of soluble urokinase receptor (suPAR) are elevated in nearly 70% of patients with FSGS, but they are undetectable in patients with MCD or MN.
A link between abnormal T-cell function and MCD was initially proposed more than 30 years ago by Shalhoub, and many studies since then have documented altered subtype distribution and activity of lymphocytes in children with MCD. A recent study in which albuminuria and podocyte foot process effacement was induced by injection of CD34+ stem cells isolated from patients with MCD or FSGS into immunodeficient NOD/SCID mice underscores the pivotal role of the immune system in the pathogenesis of MCD. This role is supported by the finding of a higher Th17/Treg cell ratio in children with MCD.
Minimal change disease represents a fascinating instance of organ dysfunction caused by a variable interaction between intrinsic structural defects and immunologic disturbances. Although MCD can occur in a familial pattern with both ver-tical and horizontal transmission, it has not been linked to mutations in any of the well-recognized proteins associated with FSGS, such as Wilms tumor-1, TRPC6, or α-actinin-4. Interestingly, there have been observations linking fre-quently relapsing childhood MCD to allelic heterogeneity in the gene for nephrin, a key component of the slit diaphragm and a major genetic locus for congenital NS. In addition, in a study of 214 Chinese patients with MCD, variants in the podo-cin gene were more common than in healthy controls, and they correlated with the level of urinary protein excretion. Alterations in histone H3 lysine 4 trimethylation in children

with MCD raise the possibility that epigenetic changes may contribute to the occurrence of MCD.
MCD also is associated with various “secondary” causes (Box 17.1), including medications, infections, toxins, and malignancies. The pathophysiologic link between these sec-ondary causes and the resulting MCD is not understood.
Minimal change disease can be the cause of significant short-term morbidity and can manifest with a chronic relaps-ing course with long-term adverse consequences well into adulthood. Both first-line treatment and secondary thera-peutic options for more difficult cases can lead to serious toxicity. Therefore, although the long-term prognosis is excellent, optimal management of MCD requires clinical acumen to balance the risks of untreated disease activity against the hazards of available pharmacologic choices. This chapter will review the definition, incidence, presentation, and treatment options for MCD, highlighting key differences between pediatric and adult patients with the goal of provid-ing a rational basis for the management of this disorder.
INCIDENCE
The overall incidence of primary or idiopathic NS comprised of MCD and its variants, FSGS, MN, and MPGN, is approxi-mately three to five cases/100,000 population/yr in children and adults. This rate is fairly constant throughout the world and in most racial and ethnic groups. The contribution of MCD to this general category varies tremendously with the age of the patient. Thus, in prepubertal patients more than 6 months of age, MCD accounts for nearly 90% of all cases of idiopathic NS, whereas in adults the percentage of cases attrib-utable to MCD falls to 10% to 15%. Adolescence represents the transition period between the two ends of the spectrum. In a study of 1523 consecutive Chinese patients who under-went biopsy performed during the evaluation of NS, in those
165 CHAPTER 17 — MINIMAL CHANGE DISEASE
aged 14 to 24 years, MCD was documented in 33% of the sub-group. Similarly, in a report by Mubarak of biopsy findings in 538 pediatric patients in Pakistan, among whom 365 were younger children (mean age 7.3 years) and 173 were adoles-cents (mean age 15.1 years), approximately one third of the older group had FSGS and only one fourth had MCD. The incidence of MN and MPGN was significantly higher in the older group than in the younger group. These findings sug-gest that adolescents correspond more closely to adults than they do to younger children and school-age pediatric patients.
CLINICAL PRESENTATION
Minimal change disease causes the NS with nephrotic range proteinuria, hypoalbuminemia, edema, and hypercholester-olemia. The most common presenting symptom of MCD is edema, and the onset may be acute. There may be an ante-cedent infection, typically respiratory, that is associated with the onset of MCD. Infections may also trigger subsequent relapses of MCD. The rapidity of the appearance of edema is characteristic of MCD compared to other etiologies of NS. In children, edema can occur anywhere in the body, including the periorbital region, scrotum, or abdomen. Less frequent presenting complaints include infections such as cellulitis secondary to localized accumulation of fluid and skin breakdown, or bacterial peritonitis in patients with ascites. The incidence of thromboembolic events, includ-ing renal vein thrombosis and pulmonary emboli, is tenfold higher in adults than in children, and typically these events occur in patients with severe hypoalbuminemia.
Urinalysis reveals microscopic hematuria in 10% to 30% of adults and children with MCD, but gross hematuria is rare. Microscopic examination of the urine may also show waxy casts and oval fat bodies. In one series, acute kidney injury (AKI) occurred in 17.8% of adult patients who presented
Malignancy
Hematologic Tumors
Hodgkin lymphomaNon-Hodgkin lymphomaLeukemia
Solid Tumors
ThymomaRenal cell carcinomaLung carcinomaMesothelioma
Infection
SyphilisMycoplasmaEhrlichiosisStrongyloidiasisEchinococcusTuberculosis
HIVHepatitis C virus
Drugs
NSAIDs, including COX-2 inhibitorsAntimicrobials (ampicillin, rifampicin, cephalosporins)LithiumD-penicillamineBisphosphonates (Pamidronate)Sulfasalazines (mesalazine and salazopyrine)TrimethadioneImmunizationsInterferon-γ
Other Renal and Systemic Diseases
SLEFabry diseasePolycystic kidney diseaseIPEX syndrome
HIV, Human immunodeficiency virus; IPEX, immune dysregulation polyendocrinopathy, enteropathy, X-linked; NSAIDs, nonsteroidal antiinflammatory drugs; SLE, systemic lupus erythematosus.
Box 17.1 Secondary Causes of Minimal Change Disease

166 SECTION 3 — GLOMERULAR DISEASES
with nephrotic syndrome and were subsequently diagnosed with MCD. These patients tended to be older, male, hyperten-sive, and had more severe proteinuria and hypoalbuminemia than patients who did not develop AKI. Kidney biopsies of these patients showed a variety of histologic patterns of injury including tubular atropy, interstitial inflammation and fibro-sis, and atherosclerotic disease. Serum levels of C3 and C4 are typically normal, and antinuclear antibodies and cryoglobu-lins are usually absent.
INITIAL TREATMENT
Corticosteroids represent the time-honored initial therapy for presumed and biopsy-confirmed MCD. As mentioned, the sen-sitivity of MCD to steroid treatment prompts many physicians to empirically treat nephrotic patients with glucocorticoids without a kidney biopsy, particularly children. Prednisone is the usual agent prescribed, and the standard dose in pediatric patients is 60 mg/m2 or 2 mg/kg daily for 4 to 6 weeks fol-lowed by 40 mg/m2 or 1.5 mg/kg every other day for 4 to 6 weeks. In children, 70% will achieve remission after 10 to 14 days of treatment, and the vast majority will no longer have proteinuria after 4 weeks of therapy. There are conflicting data in the literature as to whether lengthening the course of the initial treatment from 8 to 12 weeks delays the time to first relapse and reduces overall exposure to steroids. Efficacy may vary depending on the patient population, and the precise treatment should be guided by the experience at each center.
Adults are treated with oral prednisone 1 mg/kg/day or alternate-day prednisone at 2 mg/kg/day. However, unlike children, responses in adults may take up to 24 weeks before the patient is designated “steroid responsive” or “steroid resistant.” In adults, up to 20% of patients with an initial diagnosis of MCD may be refractory to steroids at the end of 24 weeks.
Relapse therapy involves similar doses, but usually for a shorter period of time. Various modifications in corticoste-roid dosing such as extended tapering schedules, avoidance of every other day administration, and prolonged low-dose hydrocortisone to prevent adrenal insufficiency have been
tried to prevent relapses and to minimize side effects. Dif-ferent formulations of steroids such a deflazacort have also been tried with mixed results. Adults do not tolerate relaps-ing disease as well as children as a consequence of the intrin-sic morbidity of MCD and the toxicity related to repeated exposures to corticosteroids. Therefore, these patients are often candidates for prompt implementation of immuno-suppressive therapy.
SHORT-TERM COURSE
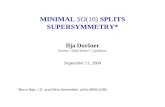
Minimal change disease is usually a chronic relapsing disease (Fig. 17.1). Less than 10% of cases will remain completely free of relapses after the initial episode. The remaining patients can be divided into three categories. One third will have infrequent relapses that are easily managed by intermit-tent administration of courses of corticosteroids. Another third will have frequent relapses defined by ≥2 relapses in a 6-month period; however, they, too, are successfully man-aged with intermittent administration of courses of cortico-steroids, and they do not manifest significant steroid-induced side effects. The final third are frequently relapsing patients or those with steroid dependence defined as relapse occur-ring on alternate-day steroid treatment or within 2 weeks of discontinuing corticosteroids. It has proved difficult to pre-dict the short-term, i.e., ≤2 years after disease onset, prog-nosis in individual patients. In children, those who go into remission during the first week of corticosteroid treatment and who have no hematuria are more likely to be infrequent relapsers, defined as <2 episodes in 6 months or <3 in 1 year. The presence of small involuted glomeruli, which can be dis-tinguished from other causes of global glomerulosclerosis by the presence of vital podocytes and parietal epithelial cells, may be a marker of frequently relapsing MCD in children.
The last category of patients usually experience steroid toxicity, and they are candidates for the second-line treat-ments, which will be outlined later. Key steroid-induced side effects in children are impaired linear growth, obesity, behavioral changes, and cosmetic changes. In addition to these clinical effects, children with MCD also experience
Figure 17.1 Minimal change disease: short-term natural history.
Infrequent relapses30%
AdultsSECOND-LINE THERAPY
CyclophosphamideMycophenolate mofetil
Cyclosporine/tacrolimus
Children and adultsSECOND-LINE THERAPY
CyclophosphamideMycophenolate mofetil
Cyclosporine/tacrolimus
Frequent relapsesSteroid dependency
Steroid toxicity30%
Frequent relapsesNo steroid toxicity
30%
MCDPATIENTS
No further relapses10%

altered quality of life and psychosocial adjustment that is related both to illness-related variables and to alterations in the family climate. In adults, additional evidence of steroid toxicity includes cataracts and altered bone density. Hyper-tension and hyperlipidemia occur across the age spectrum. It is the last category of patients that most require careful nephrologist attention for ongoing management and care.
LONG-TERM TREATMENT
IMMUNOSUPPRESSIVE THERAPY
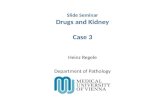
Second-line therapy is used in patients who relapse fre-quently, are steroid dependent, or manifest steroid side effects as a consequence of repeated exposure to the drug (Table 17.1). The first class of drugs that were used under these circumstances was alkylating agents such as cyclophos-phamide and chlorambucil. A prolonged remission of at least 1 year was achieved in 70% of patients. With cyclophospha-mide, most patients require at least 12 weeks of therapy, and they should be monitored carefully for side effects including leukopenia, infection, hemorrhagic cystitis, gonadal toxic-ity, and malignancy. However, more than 25% of patients with MCD who were treated with cyclophosphamide were not in sustained remission after puberty, and they required prolonged immunosuppressive treatment. Thus, because of the serious toxicity associated with the alkylating agents, the reluctance to prescribe a second course, and the guarded long-term effect, there has been greater reliance on alterna-tive medications to cyclophosphamide for frequently relaps-ing or steroid-dependent patients with MCD.
Antimetabolites such as azathioprine and mycophenolate mofetil can reduce the relapse rate by approximately 50%, although they are not as effective as alkylating agents in inducing a permanent remission. They are useful, because
167 CHAPTER 17 — MINIMAL CHANGE DISEASE
they have a more favorable side-effect profile, can be admin-istered for an extended period, and require less intensive monitoring.
A third option is calcineurin inhibitors such as cyclo-sporine and tacrolimus. These agents induce a prolonged remission in nearly 80% to 90% of patients while the patient is taking the drug; however, relapses frequently occur shortly after stopping the drug. In addition, calcineurin inhibitors can cause undesirable cosmetic changes (hair growth and gingival hyperplasia), hepatoxicity, hypertension, and neph-rotoxicity. Therefore, patients taking calcineurin inhibi-tors for more than 1 year may require periodic blood tests and serial kidney biopsies to insure that irreversible kidney injury does not occur.
Finally, the newest agent used to treat children with fre-quently relapsing or steroid-dependent MCD and clinical evidence of steroid-induced side effects is rituximab. Admin-istration of this anti-CD20 monoclonal antibody on B cells is likely to achieve remission in up to 80% of steroid sensitive cases when used in combination with calcineurin inhibitors. This was confirmed in a study of 54 children (mean age 11 years) in which rituximab plus low-dose steroids and tacro-limus was as effective as treatment with standard doses of the latter two drugs; however, this therapy is costly, and the long-term risks are unknown. Therefore, it is advisable that randomized clinical trials are performed and ongoing sur-veillance be maintained to gain perspective on the proper place of this biologic agent in the therapeutic management of children with difficult to treat MCD.
The decision to recommend one of these second-line agents in an effort to alleviate the adverse consequences of steroids must be weighed on an individual basis and must take into account the patient’s age, sex, and likely compli-ance with treatment. Consideration should be given to the severity of the side effect, the likelihood of reversal of the complication, and the odds that the MCD will spontaneously
Table 17.1 Second-Line Treatments of Minimal Change Disease
Drug Dose Efficacy Side Effects
Cyclophosphamide Children and adults:2-2.5 mg/kg/day × 8-12 wk*
Prolonged remission(>1 yr) in 70%
Leukopenia, hemorrhagic cystitis, alopecia, seizures, gonadal toxicity, malignancy
Chlorambucil Children and adults:0.15 mg/kg/day × 8-12 wk*
Mycophenolate mofetil
Children:24-36 mg/kg/day or600 mg/m2/dose BIDAdults: 1-1.5 g BID
50% reduction in overall relapse rate
Gastrointestinal complaints, leukopenia, elevated liver enzymes
Cyclosporine Children and adults:4-5 mg/kg/day in divided doses†
70% to 80% of patients achieve complete remission on treatment
Gingival hyperplasia, tremor, elevated liver enzymes, nephrotoxicity
Tacrolimus Children and adults:0.05-0.3 mg/kg/day in divided
doses†
70%-80% Tremor, nephrotoxicity
Rituximab Children and adults:375-1000 mg/m2/dose2 doses, 2 wk apart
80% in steroid responsive MCD InfectionMalignancy
BID,Twice daily; SSNS, steroid-sensitive nephrotic syndrome.*It is recommended that the duration of therapy be extended to 12 weeks in patients with steroid-dependent disease.†Target trough levels for cyclosporine and tacrolimus are 100-200 ng/mL and 4-8 ng/mL, respectively. Children may require more frequent
do sing to maintain a therapeutic drug level. After achieving remission, reduce doses to the lowest dose compatible with staying in remission.

168 SECTION 3 — GLOMERULAR DISEASES
resolve. Although a number of other immunomodulatory agents have been tried in the past in patients with MCD, the data have been collected in relatively small studies that hin-der broad generalizations about efficacy. In addition, drugs such as levamisole are generally not available in the United States for use in patients with MCD. This underscores the need to develop newer agents that can be used to control proteinuria in patients with MCD, especially in children with steroid toxicity and adults with relapsing disease.
SUPPORTIVE CARE
After the initial diagnosis, patients with MCD are usually monitored with daily dipstick testing for proteinuria. In most patients, relapses are detected by the onset of pro-teinuria 3 to 4 days before edema ensues. In those patients who develop edema before a relapse is recognized or who respond slowly to prednisone, edema can be controlled by prescribing a low-salt (2 g sodium) diet and oral diuret-ics. Options include loop diuretics, such as furosemide 1 to 2 mg/kg administered once or twice daily or a thiazide diuretic. The duration of action of diuretic agents may be diminished secondary to hypoalbuminemia and enhanced renal clearance, but this is rarely clinically significant because the medications are only needed for 1 to 2 weeks until treat-ment response occurs and proteinuria resolves. Children who have frequent relapses and persistent edema are at risk for bacterial peritonitis and can be given prophylactic penicillin. Immunization with the pneumococcal vaccine is also helpful under these circumstances. If feasible, the tim-ing of vaccine administration should be delayed for at least 2 weeks after administration of prednisone to ensure maxi-mal immunologic response.
PROGNOSIS
The prognosis for patients with MCD is excellent, and, accord-ing to the literature, the disease eventually resolves without further relapses in >95% of patients. However, this presumed benign course is based on scarce data of patients followed into adulthood. A recent study of 42 adult patients, median age 28 years, who were monitored for a median of 22 years after the diagnosis of MCD, demonstrated that 33% were still relapsing in adulthood. Children who had a relapsing course and/or required immunosuppressive medications were more likely to have persistent disease in adulthood. Moreover, although final height was normal, nearly half of adult patients with relapsing MCD have excess weight gain, hypertension, cata-racts, osteoporosis, and sperm abnormalities. Whether MCD has any long-term effect on the incidence or age at onset of cardiovascular disease in adults remains unclear. Clinical outcomes in patients enrolled in large health maintenance organizations indicate that persistent NS is associated with an increased incidence of atherosclerotic disease, and the rela-tive risk in patients with MCD versus more refractory forms of idiopathic NS requires further study. Based on the persis-tence beyond childhood of relapsing disease and the devel-opment of serious side effects, transition from a pediatric to an adult nephrologist is warranted in patients with relapsing MCD or a history of prolonged steroid or immunosuppres-sive drug use for MCD as they reach adulthood.
The overwhelming majority of children with MCD have no evidence of progressive chronic kidney disease. Recognizing that the diagnosis of FSGS can be difficult to establish if a kidney biopsy specimen does not include the few abnormal glomeruli at the corticomedullary junction, it is conceivable that the rare cases of presumed MCD with a poor outcome and progressive GFR loss may represent unidentified FSGS.
CONCLUSION
Although MCD is not a common illness, it causes short-term morbidity related to edema and infection. Initial treatment with corticosteroids results in remission of proteinuria in nearly all patients; however, 90% of patients will manifest a frequently relapsing or steroid-dependent course with ste-roid toxicity. These patients are candidates for treatment with second-line agents such as cyclophosphamide, myco-phenolate mofetil, or tacrolimus. The choice of drug will vary from center to center and reflect local experience and preferences of the individual physician. The disease can per-sist into adulthood and can lead to chronic sequelae such as bone demineralization, atherosclerosis, and obesity. There-fore, long-term follow-up is warranted in those patients who continue to relapse and require immunosuppressive medication. Further research is needed to define better the cause of MCD, that is, the immunologic basis and/or role of podocyte protein abnormalities, so as to develop more effective treatments that can promote long-term remission without the side effects associated with current therapeutic options.
KEY BIBLIOGRAPHYClement LC, Avila-Casado C, Macé C, et al: Podocyte-secreted angiopoi-
etin-like-4 mediates proteinuria in glucocorticoid-sensitive nephrotic syndrome, Nat Med 17:117-122, 2011.
Dijkman HBPM, Wetzels JFM, Gemnick JH, et al: Glomerular involu-tion in children with frequently relapsing minimal change nephrotic syndrome: an unrecognized form of glomerulosclerosis? Kidney Int 71:44-52, 2007.
Fakhouri F, Bocqueret N, Taupin P, et al: Children with steroid-sensi-tive nephrotic syndrome come of age: long-term outcome, J Pediatr 147:202-207, 2005.
Garin EH, Diaz LN, Mu W, et al: Urinary CD80 excretion increases in idiopathic minimal-change disease, J Am Soc Nephrol 20:260-266, 2009.
George B, Verma R, Soofi AA, et al: Crk1/2-dependent signaling is nec-essary for podocyte foot process spreading in mouse models of glo-merular disease, J Clin Invest 122:674-692, 2012.
Gulati A, Sinha A, Jordan SC, et al: Efficacy and safety of treatment with rituximab for difficult steroid-resistant and -dependent nephrotic syndrome: multicentric report, Clin J Am Soc Nephrol 5:2207-2212, 2010.
Kisner T, Burst V, Teschner S, et al: Rituximab treatment for adults with refractory nephrotic syndrome: a single-center experience and review of the literature, Nephron Clin Pract 120:c79-c85, 2012.
Kitamura A, Tsukaguchi H, Hiramoto R, et al: A familial childhood-onset relapsing nephrotic syndrome, Kidney Int 71:946-951, 2007.
Kyriels HA, Levtchenko EN, Wetzels JF: Long-term outcome after cyclo-phosphamide treatment in children with steroid-dependent and fre-quently relapsing minimal change nephrotic syndrome, Am J Kidney Dis 49:592-597, 2007.
McCarthy ET, Sharma M, Savin VJ: Factors in idiopathic nephrotic syn-drome and focal segmental glomerulosclerosis, Clin J Am Soc Nephrol 5:2115-2121, 2010.
Mubarak M, Kazi JI, Lanewala A, et al: Pathology of idiopathic nephrotic syndrome in children: are the adolescents different from young chil-dren? Nephrol Dial Transplant 27:722-726, 2012.

Nachman PH, Jennette JC, Falk RJ: Primary glomerular diseases. In Brenner BM, editor: The kidney, ed 8, Philadelphia, 2008, W.B. Saun-ders Company, pp 987-1279.
Palmer SC, Nand K, Strippoli GF: Interventions for minimal change disease in adults with nephrotic syndrome, Cochrane Database Syst Rev(1), 2008 Jan 23. CD001537.
Sellier-Leclerc AL, Macher MA, Loirat C, et al: Rituximab efficiency in children with steroid-dependent nephrotic syndrome, Pediatr Nephrol 25:1109-1115, 2010.
van Husen M, Kemper MJ: New therapies in steroid-sensitive and steroid-resistant idiopathic nephrotic syndrome, Pediatr Nephrol 26:881-892, 2011.
Waldman M, Crew RJ, Valeri A, et al: Adult minimal-change disease: clinical characteristics, treatment, and outcomes, Clin J Am Soc Nephrol 2:445-453, 2007.
169 CHAPTER 17 — MINIMAL CHANGE DISEASE
Wei C, El Hindi S, Li J, et al: Circulating urokinase receptor as a cause of focal segmental glomerulosclerosis, Nat Med 17:952-960, 2011.
Zhang L, Dai Y, Peng W, et al: Genome-wide analysis of histone H3 lysine 4 trimethylation in peripheral blood mononuclear cells of minimal change nephrotic syndrome patients, Am J Nephrol 30:505-513, 2009.
Zhou FD, Chen M: The renal histopathological spectrum of patients with nephrotic syndrome: an analysis of 1523 patients in a single C hinese center, Nephrol Dial Transplant 26:3993-3997, 2011.
Zhu L, Yu L, Wang CD, et al: Genetic effect of the NPHS2 gene vari-ants on proteinuria in minimal change disease and immunoglobulin A nephropathy, Nephrology 14:728-734, 2009.
Full bibliography can be found on www.expertconsult.com.