MINI-STERNOTOMY FOR AVR · HISTORY I •A right parasternal incision is made, extending from the...
21
MINI-STERNOTOMY FOR AVR Γ. ΔΡΟΣΟΣ Θ.ΚΑΡΑΙΣΚΟΣ ΧΕΙΡΟΥΡΓΙΚΗ ΚΛΙΝΙΚΗ ΘΩΡΑΚΟΣ ΚΑΡΔΙΑΣ ΝΟΣ. ΠΑΠΑΝΙΚΟΛΑΟΥ
Transcript of MINI-STERNOTOMY FOR AVR · HISTORY I •A right parasternal incision is made, extending from the...

MINI-STERNOTOMY FOR AVR
Γ ΔΡΟΣΟΣ ΘΚΑΡΑΙΣΚΟΣ
ΧΕΙΡΟΥΡΓΙΚΗ ΚΛΙΝΙΚΗ ΘΩΡΑΚΟΣ ΚΑΡΔΙΑΣ
ΝΟΣ ΠΑΠΑΝΙΚΟΛΑΟΥ
HISTORY I
Minimally Invasive Approach for Aortic Valve Operations
Delos M Cosgrove III MD and Joseph F Sabik MD
Department of Thoracic and Cardiovascular Surgery
The Cleveland Clinic Foundation Cleveland Ohio
A minimally invasive procedure for performing repair or replacement of the aortic valve has been developed that simplifies the technique and reduces surgical trauma
Ann Thorac Surg 199662596-7
HISTORY I
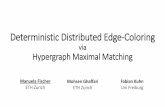
bull A right parasternal incision is made extending from the lower edge of the second costal cartilage to the superior edge of the fifth costal cartilage The pectoralis major muscle is divided exposing the second third and fourth intercostal spaces and the third and fourth costal cartilages The third and fourth costal cartilages are totally excised The right internal thoracic artery is ligated just below the second costal cartilage and just above the fifth costal cartilage Intercostal muscles and pleura are incised lateral to the edge of the sternum entering the right pleural cavity The pericardium is incised exposing the ascending aorta and right atrium and a tangential incision is made in the aorta exiting into the noncoronary sinus
bull A common femoral artery and vein are exposed and after heparinization are cannulated Adequate venous drainage is obtained by placing a long venous cannula so that the tip of the cannula passes through the right atrium and lies in the superior vena cava A centrifugal pump is attached to the venous line to actively drain the right side of the heart Alternatively a cannula may be placed in the right atrial appendage After cardiopulmonary bypass is established the aorta is encircled with umbilical tape and the aorta cross-clamped with a right-angled clamp A suture is then placed just above each commissure and clamped to the surrounding drape under tension This elevates the aortic root into the operative field When isolated aortic stenosis is present cardioplegia is administered into the ascending aorta in the presence of aortic insufficiency cardioplegia is given directly into the coronary ostia after the aortotomy is performed The aortic valve is either repaired or replaced A suction catheter is placed into the left ventricle through the aortic annulus as needed At the completion of the repair or replacement the aortotomy is closed and air is removed from the heart through the aortic incision with the assistance of the transesophagealechocardiography probe Atrial and ventricular pacing wires are placed and the cross-clamp is removed
HISTORY I
From January to April 1996 this approach was em- ployed in 25 patients with isolated aortic valve disease Repairs of the aortic valve were carried out in 6 patients Nineteen patients had valve replacement 10 Carpentier- Edwards pericardial valves 8 aortic homografts and 1 St Jude valve There were no deaths reoperations for bleeding strokes or wound infections
History II
bull Minimally invasive cardiac valve surgery improves patient satisfaction while reducing costs of cardiac valve replacement and repair
bull L H Cohn D H Adams G S Couper D P Bichell D M Rosborough S P Sears and S F Aranki
bull From the Division of Cardiac Surgery Brigham and Womens Hospital Department of Surgery Harvard Medical School Boston Massachusetts
bull Ann Surg 1997 Oct 226(4) 421ndash428
History II
History II
bull Of the 84 patients there were 2 operative mortalities both in class IV aortic patients from multisystem organ failure There was no operative mortality in the patients undergoing mitral valve replacement or repair The operations were carried out with the same accuracy and attention to detail as with the conventional operation There was minimal postoperative bleeding cerebral vascular accidents or other major morbidity Groin cannulation complications primarily were related to atherosclerotic femoral arteries
Minimally Invasive and Conventional Aortic Valve ReplacementA Propensity Score Analysis
Department of Adult Cardiac Surgery Daniyar Gilmanov G Pasquinucci Heart Hospital Massa Italy
Methods
bull This is a retrospective observational cohort study of prospectively collected data on 709 patients undergoing isolated primary aortic valve replacement between 2004 and 2011 Of these 338
were performed through either right anterior minithoracotomy or upper ministernotomy With propensity score matching 182 patients (minimally invasive group) were compared with 182
patients in conventional sternotomy (control group)
Conclusions
bull Our experience shows that mini-access isolated aortic valve surgery is a reproducible safe and effective procedure and reduces assisted ventilation duration the need for blood product
transfusion and incidence of post-surgery atrial fibrillation
(Ann Thorac Surg 201396837ndash43)
Introduction
bull The approaches taken under the umbrella of minimally-invasive surgical aortic valve replacement (MICS SAVR) essentially consist of a variety of access options to the aortic valve using smaller incisions
bull Importantly there is no convention or consensus as to what size incision qualifies as a minimally-invasive procedure
bull Furthermore lsquominimally-invasiversquo cardiac surgery (MICS) arguably is somewhat of a misnomer certainly in comparison interventions such as TAVR because the most invasive portions of the surgery including cross-clamping of the aorta ischemic cardiac arrest the use of cardiopulmonary bypass and opening of the aorta with introduction of air into the heart chambers all remain the same
Mahesh K Ramchandani MDAnnals of Thoracic Surgery ( in press)
ΜΙΝΙ
ν=28
ΥΠΟΛΟΙΠΟΙ
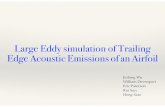
ν=131Ηλικία 722plusmn84 704plusmn98Γυναίκες(n) 10 (357) 58(442)Euro score 227plusmn2 18plusmn19ΜΕΘ μέρες 196plusmn06 198plusmn11Μέρες νοσηλείας 6plusmn218 57plusmn18Νοσηλεία lt5
μέρες
14(50) 37(517)
Μετάγγιση
RBC UNITS
12plusmn09 15plusmn13
CPB min 1124plusmn37 933plusmn33Μηχανικός
αερισμός (ώρες)
86plusmn45 104plusmn13
ΜΙΝΙ Στερνοτομές 2018Μεμονωμένη αντικατάσταση αορτικής βαλβίδας 2018
Σύνολο 159- ΜΙΝΙ 28 (176)
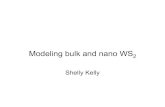
Χαρακτηριστικά ασθενών Επιπλοκές
ΜΙΝΙ
ν=28
ΥΠΟΛΟΙΠΟΙ
ν=131
P value
LCOS(n) 1 (36) 3(23) 069
Επαναδιάνοιξη(n) 0 4(31) 035
Λοιμώξεις
στερνοτομής(n)
1 (36) 3(23) 069
Stroke 0 2(15) 051
NIV 1 (36) 6(46) 081
Επαναδιασωλήνωση 0 3(23) 042
AKI(n) 3(107) 12(92) 079
Κολπική μαρμαρυγή 7(25) 40(305) 056
Θάνατος 0 3(23) 042
Minimally Invasive Approaches to Surgical Aortic Valve Replacement
A Meta-Analysis
Carolyn Chang BS Sajjad Raza MD Salah E Altarabsheh MD Sarah Delozier PhD Umesh M Sharma MD MBA Aisha Zia MD Muhammad Shahzeb Khan MD Mandy Neudecker MS Alan H Markowitz MD Joseph F Sabik III MD and Salil V Deo MD
Cleveland Ohio
(Ann Thorac Surg 20181061881ndash9)
Minimally Invasive Approaches to Surgical Aortic Valve ReplacementA Meta-Analysis
The outcomes of the 2 minimally invasive aortic valve replacement (AVR) strategiesmdashmini-sternotomy (AVR-st) and right anterior thoracotomy (AVR-th) with each other and with conventional AVR (cAVR)
Searched Medline PubMed Embase and Web of Science in December 2017 for studies comparing AVR-st AVR-th and cAVR Endpoints studied included hospital mortality stroke atrial fibrillation cardiopulmonary bypass (CPB) time and length of stay
A total of 19 studies (gt10000 pooled patients) met the inclusion criteria
bull Mortality (p [ 006) and stroke (p [ 015) were comparable between minimally invasive and conventional AVR
bull CPB times were longer with AVR-th versus cAVR (124 minutes [range 5 to 19] p lt 001) In the AVR-th cohort CPB duration was weakly inversely related to study size (p [ 006)
bull Atrial fibrillation was much less after AVR-th (odds ratio 047 [035 to 063] p lt 0001)
bull Hospital stay was significantly lower after minimally invasive surgery (08 [04 to 13] days p lt 001
Minimally invasive approaches to AVR yield excellent outcomes in high-volume centers They reduce hospital stay and incidence of postoperative atrial fibrillation and therefore should be considered in patients undergoing AVR The operative approach should be selected according to surgeonrsquos technical expertise and what is best for specific patient profile
(Ann Thorac Surg 20181061881ndash9)
Full Sternotomy Hemisternotomy and Minithoracotomyfor Aortic Valve Surgery Is There a Difference
Elisa Mikus MD Simone Calvi MD Gianluca Campo MD Rita Pavasini MD Marco Paris MD Eliana Raviola MD Marco Panzavolta MD Alberto Tripodi MD Roberto Ferrari MD PhD and Mauro Del Giglio MD PhD
Cardiothoracic and Vascular Department Maria Cecilia Hospital GVM Care amp Research Cotignola (RA) Cardiovascular Institute Azienda Ospedaliero-Universitaria di Ferrara Cona (FE) and Cardiovascular Department Istituto Clinico San Rocco Ome (BS) Italy
(Ann Thorac Surg 20181061782ndash8)
Full Sternotomy Hemisternotomy and Minithoracotomyfor Aortic Valve Surgery Is There a Difference
bull The study included all 1907 consecutive patients hospitalized at the Maria Cecilia Hospital (Cotignola RA Italy) between January 2010 and March 2017 undergoing isolated AVR through PUH RAT or MS The choice of the approach was left to surgeonrsquos preference To adjust for differences in baseline characteristics between the study groups a propensity score matching was performed Linear and logistic regression analyses were performed
bull Results Partial upper hemisternotomy was performed in 820 patients (43) right anterior minithoracotomy in 488 (26) and median sternotomy in 599 (31) After propensity score matching three groups of 377 patients were obtained Cardiopulmonary bypass and crossclamptimes were shorter in the right anterior minithoracotomy group than in the median sternotomy and partial upper hemisternotomy groups (p lt 0001) No significant differences in in-hospital mortality were observed (p [ 09) Renal failure (odds ratio 54 95 confidence interval 23 to 114 p lt 00001) extracardiac arteriopathy (odds ratio 29 95 confidence interval 11 to 67 p [ 0017) and left ventricular ejection fraction (odds ratio 096 95 confidence interval 093 to 099 p [ 0009) emerged as independent predictors of in hospital mortality
bull Conclusions Minimal-access isolated aortic valve surgery is a reproducible safe and effective procedure with similar outcomes and operating times compared with conventional sternotomy
Ann Thorac Surg 20181061782ndash8
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full median sternotomy for aortic valve replacement
Sukumaran K Nair FRCS(CTh) et al
bull From the a Department of Cardiothoracic Surgery PapworthHospital Cambridge United Kingdom Freeman Hospital Newcastle upon Tyne United Kingdom Leeds Institute of Clinical Trials Research University of Leeds Leeds United Kingdom Health Economics Research Group Brunel University London London United Kingdom and London School of Hygiene and Tropical Medicine Keppel Street London United Kingdom
J Thorac Cardiovasc Surg 20181562124-32
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacement
bull Methods This RCT compared MS with FS for first-time isolated AVR in 2 United Kingdom National Health Service hospitals Primary endpoints were duration of postoperative hospital stay and the time to fitness for discharge from hospital after AVR analyzed in the intent-to-treat population
bull Results In this RCT 222 patients were recruited and randomized (n frac14 118 in the MS group n frac14 104 in the FS group) Compared with the FS group the MS group had a longer hospital length of stay (mean 95 days vs 86 days) and took longer to achieve fitness for discharge home (mean 85 days vs 75 days) Adjusting for valve type sex and surgeon hazard ratios (HRs) from Cox models did not show a statistically significant effect of MS (relative to FS) on either hospital stay (HR 0874 95 confidence interval [CI] 0668-1143 P frac14 3246) or time to fitness for discharge (HR 0907 95 CI 0688-1197 P value frac14 4914) During a mean follow-up of 760 days (745 days for the MS group and 777 days for the FS group) 12 patients (10) in the MS group and 7 patients (7) in the FS group died (HR 1871 95 CI 0723-4844 P frac14 1966) Average extra cost for MS was pound1714 during the first 12 months
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacementCentral Message
In the United Kingdomrsquos National Health Service compared with a conventional median sternotomy approach for surgical aortic valve replacement mini-sternotomy did not hasten recovery or hospital discharge and was not cost-effective
Measuring What Matters
Having lived through the growth of percutaneous coronary intervention and now seeing the expansion of transcatheter aortic valve replacement I find myself asking the somewhat existential question ldquoAre we measuring what matters to patientsrdquo
Thoralf M Sundt MD Division of Cardiac Surgery
Massachusetts General Hospital Boston Massachusetts
Ann Thorac Surg 20181061602
Measuring What Matters
In a study performed at Dartmouth-Hitchcock
elderly patients prioritized ability to pursue activities maintaining independence and reducing symptoms
over
mortality benefit
Coleywright M et al Patients defined goals for the treatment of sever AVS a qualitative analysis
Health Expect 2016 191036-43
Measuring What Matters
These sorts of ldquosoftrdquo outcome variables are challenging to us We think of ourselvesmdashat least I domdashas medical scientists interested in ldquohardrdquo endpoints
But our patients are challenging us to consider what they value most not what we can measure easily Irsquod say it is time for us to broaden our horizons and revisit how we can better measure what matters
Ann Thorac Surg 20181061602

HISTORY I
Minimally Invasive Approach for Aortic Valve Operations
Delos M Cosgrove III MD and Joseph F Sabik MD
Department of Thoracic and Cardiovascular Surgery
The Cleveland Clinic Foundation Cleveland Ohio
A minimally invasive procedure for performing repair or replacement of the aortic valve has been developed that simplifies the technique and reduces surgical trauma
Ann Thorac Surg 199662596-7
HISTORY I
bull A right parasternal incision is made extending from the lower edge of the second costal cartilage to the superior edge of the fifth costal cartilage The pectoralis major muscle is divided exposing the second third and fourth intercostal spaces and the third and fourth costal cartilages The third and fourth costal cartilages are totally excised The right internal thoracic artery is ligated just below the second costal cartilage and just above the fifth costal cartilage Intercostal muscles and pleura are incised lateral to the edge of the sternum entering the right pleural cavity The pericardium is incised exposing the ascending aorta and right atrium and a tangential incision is made in the aorta exiting into the noncoronary sinus
bull A common femoral artery and vein are exposed and after heparinization are cannulated Adequate venous drainage is obtained by placing a long venous cannula so that the tip of the cannula passes through the right atrium and lies in the superior vena cava A centrifugal pump is attached to the venous line to actively drain the right side of the heart Alternatively a cannula may be placed in the right atrial appendage After cardiopulmonary bypass is established the aorta is encircled with umbilical tape and the aorta cross-clamped with a right-angled clamp A suture is then placed just above each commissure and clamped to the surrounding drape under tension This elevates the aortic root into the operative field When isolated aortic stenosis is present cardioplegia is administered into the ascending aorta in the presence of aortic insufficiency cardioplegia is given directly into the coronary ostia after the aortotomy is performed The aortic valve is either repaired or replaced A suction catheter is placed into the left ventricle through the aortic annulus as needed At the completion of the repair or replacement the aortotomy is closed and air is removed from the heart through the aortic incision with the assistance of the transesophagealechocardiography probe Atrial and ventricular pacing wires are placed and the cross-clamp is removed
HISTORY I
From January to April 1996 this approach was em- ployed in 25 patients with isolated aortic valve disease Repairs of the aortic valve were carried out in 6 patients Nineteen patients had valve replacement 10 Carpentier- Edwards pericardial valves 8 aortic homografts and 1 St Jude valve There were no deaths reoperations for bleeding strokes or wound infections
History II
bull Minimally invasive cardiac valve surgery improves patient satisfaction while reducing costs of cardiac valve replacement and repair
bull L H Cohn D H Adams G S Couper D P Bichell D M Rosborough S P Sears and S F Aranki
bull From the Division of Cardiac Surgery Brigham and Womens Hospital Department of Surgery Harvard Medical School Boston Massachusetts
bull Ann Surg 1997 Oct 226(4) 421ndash428
History II
History II
bull Of the 84 patients there were 2 operative mortalities both in class IV aortic patients from multisystem organ failure There was no operative mortality in the patients undergoing mitral valve replacement or repair The operations were carried out with the same accuracy and attention to detail as with the conventional operation There was minimal postoperative bleeding cerebral vascular accidents or other major morbidity Groin cannulation complications primarily were related to atherosclerotic femoral arteries
Minimally Invasive and Conventional Aortic Valve ReplacementA Propensity Score Analysis
Department of Adult Cardiac Surgery Daniyar Gilmanov G Pasquinucci Heart Hospital Massa Italy
Methods
bull This is a retrospective observational cohort study of prospectively collected data on 709 patients undergoing isolated primary aortic valve replacement between 2004 and 2011 Of these 338
were performed through either right anterior minithoracotomy or upper ministernotomy With propensity score matching 182 patients (minimally invasive group) were compared with 182
patients in conventional sternotomy (control group)
Conclusions
bull Our experience shows that mini-access isolated aortic valve surgery is a reproducible safe and effective procedure and reduces assisted ventilation duration the need for blood product
transfusion and incidence of post-surgery atrial fibrillation
(Ann Thorac Surg 201396837ndash43)
Introduction
bull The approaches taken under the umbrella of minimally-invasive surgical aortic valve replacement (MICS SAVR) essentially consist of a variety of access options to the aortic valve using smaller incisions
bull Importantly there is no convention or consensus as to what size incision qualifies as a minimally-invasive procedure
bull Furthermore lsquominimally-invasiversquo cardiac surgery (MICS) arguably is somewhat of a misnomer certainly in comparison interventions such as TAVR because the most invasive portions of the surgery including cross-clamping of the aorta ischemic cardiac arrest the use of cardiopulmonary bypass and opening of the aorta with introduction of air into the heart chambers all remain the same
Mahesh K Ramchandani MDAnnals of Thoracic Surgery ( in press)
ΜΙΝΙ
ν=28
ΥΠΟΛΟΙΠΟΙ
ν=131Ηλικία 722plusmn84 704plusmn98Γυναίκες(n) 10 (357) 58(442)Euro score 227plusmn2 18plusmn19ΜΕΘ μέρες 196plusmn06 198plusmn11Μέρες νοσηλείας 6plusmn218 57plusmn18Νοσηλεία lt5
μέρες
14(50) 37(517)
Μετάγγιση
RBC UNITS
12plusmn09 15plusmn13
CPB min 1124plusmn37 933plusmn33Μηχανικός
αερισμός (ώρες)
86plusmn45 104plusmn13
ΜΙΝΙ Στερνοτομές 2018Μεμονωμένη αντικατάσταση αορτικής βαλβίδας 2018
Σύνολο 159- ΜΙΝΙ 28 (176)
Χαρακτηριστικά ασθενών Επιπλοκές
ΜΙΝΙ
ν=28
ΥΠΟΛΟΙΠΟΙ
ν=131
P value
LCOS(n) 1 (36) 3(23) 069
Επαναδιάνοιξη(n) 0 4(31) 035
Λοιμώξεις
στερνοτομής(n)
1 (36) 3(23) 069
Stroke 0 2(15) 051
NIV 1 (36) 6(46) 081
Επαναδιασωλήνωση 0 3(23) 042
AKI(n) 3(107) 12(92) 079
Κολπική μαρμαρυγή 7(25) 40(305) 056
Θάνατος 0 3(23) 042
Minimally Invasive Approaches to Surgical Aortic Valve Replacement
A Meta-Analysis
Carolyn Chang BS Sajjad Raza MD Salah E Altarabsheh MD Sarah Delozier PhD Umesh M Sharma MD MBA Aisha Zia MD Muhammad Shahzeb Khan MD Mandy Neudecker MS Alan H Markowitz MD Joseph F Sabik III MD and Salil V Deo MD
Cleveland Ohio
(Ann Thorac Surg 20181061881ndash9)
Minimally Invasive Approaches to Surgical Aortic Valve ReplacementA Meta-Analysis
The outcomes of the 2 minimally invasive aortic valve replacement (AVR) strategiesmdashmini-sternotomy (AVR-st) and right anterior thoracotomy (AVR-th) with each other and with conventional AVR (cAVR)
Searched Medline PubMed Embase and Web of Science in December 2017 for studies comparing AVR-st AVR-th and cAVR Endpoints studied included hospital mortality stroke atrial fibrillation cardiopulmonary bypass (CPB) time and length of stay
A total of 19 studies (gt10000 pooled patients) met the inclusion criteria
bull Mortality (p [ 006) and stroke (p [ 015) were comparable between minimally invasive and conventional AVR
bull CPB times were longer with AVR-th versus cAVR (124 minutes [range 5 to 19] p lt 001) In the AVR-th cohort CPB duration was weakly inversely related to study size (p [ 006)
bull Atrial fibrillation was much less after AVR-th (odds ratio 047 [035 to 063] p lt 0001)
bull Hospital stay was significantly lower after minimally invasive surgery (08 [04 to 13] days p lt 001
Minimally invasive approaches to AVR yield excellent outcomes in high-volume centers They reduce hospital stay and incidence of postoperative atrial fibrillation and therefore should be considered in patients undergoing AVR The operative approach should be selected according to surgeonrsquos technical expertise and what is best for specific patient profile
(Ann Thorac Surg 20181061881ndash9)
Full Sternotomy Hemisternotomy and Minithoracotomyfor Aortic Valve Surgery Is There a Difference
Elisa Mikus MD Simone Calvi MD Gianluca Campo MD Rita Pavasini MD Marco Paris MD Eliana Raviola MD Marco Panzavolta MD Alberto Tripodi MD Roberto Ferrari MD PhD and Mauro Del Giglio MD PhD
Cardiothoracic and Vascular Department Maria Cecilia Hospital GVM Care amp Research Cotignola (RA) Cardiovascular Institute Azienda Ospedaliero-Universitaria di Ferrara Cona (FE) and Cardiovascular Department Istituto Clinico San Rocco Ome (BS) Italy
(Ann Thorac Surg 20181061782ndash8)
Full Sternotomy Hemisternotomy and Minithoracotomyfor Aortic Valve Surgery Is There a Difference
bull The study included all 1907 consecutive patients hospitalized at the Maria Cecilia Hospital (Cotignola RA Italy) between January 2010 and March 2017 undergoing isolated AVR through PUH RAT or MS The choice of the approach was left to surgeonrsquos preference To adjust for differences in baseline characteristics between the study groups a propensity score matching was performed Linear and logistic regression analyses were performed
bull Results Partial upper hemisternotomy was performed in 820 patients (43) right anterior minithoracotomy in 488 (26) and median sternotomy in 599 (31) After propensity score matching three groups of 377 patients were obtained Cardiopulmonary bypass and crossclamptimes were shorter in the right anterior minithoracotomy group than in the median sternotomy and partial upper hemisternotomy groups (p lt 0001) No significant differences in in-hospital mortality were observed (p [ 09) Renal failure (odds ratio 54 95 confidence interval 23 to 114 p lt 00001) extracardiac arteriopathy (odds ratio 29 95 confidence interval 11 to 67 p [ 0017) and left ventricular ejection fraction (odds ratio 096 95 confidence interval 093 to 099 p [ 0009) emerged as independent predictors of in hospital mortality
bull Conclusions Minimal-access isolated aortic valve surgery is a reproducible safe and effective procedure with similar outcomes and operating times compared with conventional sternotomy
Ann Thorac Surg 20181061782ndash8
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full median sternotomy for aortic valve replacement
Sukumaran K Nair FRCS(CTh) et al
bull From the a Department of Cardiothoracic Surgery PapworthHospital Cambridge United Kingdom Freeman Hospital Newcastle upon Tyne United Kingdom Leeds Institute of Clinical Trials Research University of Leeds Leeds United Kingdom Health Economics Research Group Brunel University London London United Kingdom and London School of Hygiene and Tropical Medicine Keppel Street London United Kingdom
J Thorac Cardiovasc Surg 20181562124-32
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacement
bull Methods This RCT compared MS with FS for first-time isolated AVR in 2 United Kingdom National Health Service hospitals Primary endpoints were duration of postoperative hospital stay and the time to fitness for discharge from hospital after AVR analyzed in the intent-to-treat population
bull Results In this RCT 222 patients were recruited and randomized (n frac14 118 in the MS group n frac14 104 in the FS group) Compared with the FS group the MS group had a longer hospital length of stay (mean 95 days vs 86 days) and took longer to achieve fitness for discharge home (mean 85 days vs 75 days) Adjusting for valve type sex and surgeon hazard ratios (HRs) from Cox models did not show a statistically significant effect of MS (relative to FS) on either hospital stay (HR 0874 95 confidence interval [CI] 0668-1143 P frac14 3246) or time to fitness for discharge (HR 0907 95 CI 0688-1197 P value frac14 4914) During a mean follow-up of 760 days (745 days for the MS group and 777 days for the FS group) 12 patients (10) in the MS group and 7 patients (7) in the FS group died (HR 1871 95 CI 0723-4844 P frac14 1966) Average extra cost for MS was pound1714 during the first 12 months
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacementCentral Message
In the United Kingdomrsquos National Health Service compared with a conventional median sternotomy approach for surgical aortic valve replacement mini-sternotomy did not hasten recovery or hospital discharge and was not cost-effective
Measuring What Matters
Having lived through the growth of percutaneous coronary intervention and now seeing the expansion of transcatheter aortic valve replacement I find myself asking the somewhat existential question ldquoAre we measuring what matters to patientsrdquo
Thoralf M Sundt MD Division of Cardiac Surgery
Massachusetts General Hospital Boston Massachusetts
Ann Thorac Surg 20181061602
Measuring What Matters
In a study performed at Dartmouth-Hitchcock
elderly patients prioritized ability to pursue activities maintaining independence and reducing symptoms
over
mortality benefit
Coleywright M et al Patients defined goals for the treatment of sever AVS a qualitative analysis
Health Expect 2016 191036-43
Measuring What Matters
These sorts of ldquosoftrdquo outcome variables are challenging to us We think of ourselvesmdashat least I domdashas medical scientists interested in ldquohardrdquo endpoints
But our patients are challenging us to consider what they value most not what we can measure easily Irsquod say it is time for us to broaden our horizons and revisit how we can better measure what matters
Ann Thorac Surg 20181061602

HISTORY I
bull A right parasternal incision is made extending from the lower edge of the second costal cartilage to the superior edge of the fifth costal cartilage The pectoralis major muscle is divided exposing the second third and fourth intercostal spaces and the third and fourth costal cartilages The third and fourth costal cartilages are totally excised The right internal thoracic artery is ligated just below the second costal cartilage and just above the fifth costal cartilage Intercostal muscles and pleura are incised lateral to the edge of the sternum entering the right pleural cavity The pericardium is incised exposing the ascending aorta and right atrium and a tangential incision is made in the aorta exiting into the noncoronary sinus
bull A common femoral artery and vein are exposed and after heparinization are cannulated Adequate venous drainage is obtained by placing a long venous cannula so that the tip of the cannula passes through the right atrium and lies in the superior vena cava A centrifugal pump is attached to the venous line to actively drain the right side of the heart Alternatively a cannula may be placed in the right atrial appendage After cardiopulmonary bypass is established the aorta is encircled with umbilical tape and the aorta cross-clamped with a right-angled clamp A suture is then placed just above each commissure and clamped to the surrounding drape under tension This elevates the aortic root into the operative field When isolated aortic stenosis is present cardioplegia is administered into the ascending aorta in the presence of aortic insufficiency cardioplegia is given directly into the coronary ostia after the aortotomy is performed The aortic valve is either repaired or replaced A suction catheter is placed into the left ventricle through the aortic annulus as needed At the completion of the repair or replacement the aortotomy is closed and air is removed from the heart through the aortic incision with the assistance of the transesophagealechocardiography probe Atrial and ventricular pacing wires are placed and the cross-clamp is removed
HISTORY I
From January to April 1996 this approach was em- ployed in 25 patients with isolated aortic valve disease Repairs of the aortic valve were carried out in 6 patients Nineteen patients had valve replacement 10 Carpentier- Edwards pericardial valves 8 aortic homografts and 1 St Jude valve There were no deaths reoperations for bleeding strokes or wound infections
History II
bull Minimally invasive cardiac valve surgery improves patient satisfaction while reducing costs of cardiac valve replacement and repair
bull L H Cohn D H Adams G S Couper D P Bichell D M Rosborough S P Sears and S F Aranki
bull From the Division of Cardiac Surgery Brigham and Womens Hospital Department of Surgery Harvard Medical School Boston Massachusetts
bull Ann Surg 1997 Oct 226(4) 421ndash428
History II
History II
bull Of the 84 patients there were 2 operative mortalities both in class IV aortic patients from multisystem organ failure There was no operative mortality in the patients undergoing mitral valve replacement or repair The operations were carried out with the same accuracy and attention to detail as with the conventional operation There was minimal postoperative bleeding cerebral vascular accidents or other major morbidity Groin cannulation complications primarily were related to atherosclerotic femoral arteries
Minimally Invasive and Conventional Aortic Valve ReplacementA Propensity Score Analysis
Department of Adult Cardiac Surgery Daniyar Gilmanov G Pasquinucci Heart Hospital Massa Italy
Methods
bull This is a retrospective observational cohort study of prospectively collected data on 709 patients undergoing isolated primary aortic valve replacement between 2004 and 2011 Of these 338
were performed through either right anterior minithoracotomy or upper ministernotomy With propensity score matching 182 patients (minimally invasive group) were compared with 182
patients in conventional sternotomy (control group)
Conclusions
bull Our experience shows that mini-access isolated aortic valve surgery is a reproducible safe and effective procedure and reduces assisted ventilation duration the need for blood product
transfusion and incidence of post-surgery atrial fibrillation
(Ann Thorac Surg 201396837ndash43)
Introduction
bull The approaches taken under the umbrella of minimally-invasive surgical aortic valve replacement (MICS SAVR) essentially consist of a variety of access options to the aortic valve using smaller incisions
bull Importantly there is no convention or consensus as to what size incision qualifies as a minimally-invasive procedure
bull Furthermore lsquominimally-invasiversquo cardiac surgery (MICS) arguably is somewhat of a misnomer certainly in comparison interventions such as TAVR because the most invasive portions of the surgery including cross-clamping of the aorta ischemic cardiac arrest the use of cardiopulmonary bypass and opening of the aorta with introduction of air into the heart chambers all remain the same
Mahesh K Ramchandani MDAnnals of Thoracic Surgery ( in press)
ΜΙΝΙ
ν=28
ΥΠΟΛΟΙΠΟΙ
ν=131Ηλικία 722plusmn84 704plusmn98Γυναίκες(n) 10 (357) 58(442)Euro score 227plusmn2 18plusmn19ΜΕΘ μέρες 196plusmn06 198plusmn11Μέρες νοσηλείας 6plusmn218 57plusmn18Νοσηλεία lt5
μέρες
14(50) 37(517)
Μετάγγιση
RBC UNITS
12plusmn09 15plusmn13
CPB min 1124plusmn37 933plusmn33Μηχανικός
αερισμός (ώρες)
86plusmn45 104plusmn13
ΜΙΝΙ Στερνοτομές 2018Μεμονωμένη αντικατάσταση αορτικής βαλβίδας 2018
Σύνολο 159- ΜΙΝΙ 28 (176)
Χαρακτηριστικά ασθενών Επιπλοκές
ΜΙΝΙ
ν=28
ΥΠΟΛΟΙΠΟΙ
ν=131
P value
LCOS(n) 1 (36) 3(23) 069
Επαναδιάνοιξη(n) 0 4(31) 035
Λοιμώξεις
στερνοτομής(n)
1 (36) 3(23) 069
Stroke 0 2(15) 051
NIV 1 (36) 6(46) 081
Επαναδιασωλήνωση 0 3(23) 042
AKI(n) 3(107) 12(92) 079
Κολπική μαρμαρυγή 7(25) 40(305) 056
Θάνατος 0 3(23) 042
Minimally Invasive Approaches to Surgical Aortic Valve Replacement
A Meta-Analysis
Carolyn Chang BS Sajjad Raza MD Salah E Altarabsheh MD Sarah Delozier PhD Umesh M Sharma MD MBA Aisha Zia MD Muhammad Shahzeb Khan MD Mandy Neudecker MS Alan H Markowitz MD Joseph F Sabik III MD and Salil V Deo MD
Cleveland Ohio
(Ann Thorac Surg 20181061881ndash9)
Minimally Invasive Approaches to Surgical Aortic Valve ReplacementA Meta-Analysis
The outcomes of the 2 minimally invasive aortic valve replacement (AVR) strategiesmdashmini-sternotomy (AVR-st) and right anterior thoracotomy (AVR-th) with each other and with conventional AVR (cAVR)
Searched Medline PubMed Embase and Web of Science in December 2017 for studies comparing AVR-st AVR-th and cAVR Endpoints studied included hospital mortality stroke atrial fibrillation cardiopulmonary bypass (CPB) time and length of stay
A total of 19 studies (gt10000 pooled patients) met the inclusion criteria
bull Mortality (p [ 006) and stroke (p [ 015) were comparable between minimally invasive and conventional AVR
bull CPB times were longer with AVR-th versus cAVR (124 minutes [range 5 to 19] p lt 001) In the AVR-th cohort CPB duration was weakly inversely related to study size (p [ 006)
bull Atrial fibrillation was much less after AVR-th (odds ratio 047 [035 to 063] p lt 0001)
bull Hospital stay was significantly lower after minimally invasive surgery (08 [04 to 13] days p lt 001
Minimally invasive approaches to AVR yield excellent outcomes in high-volume centers They reduce hospital stay and incidence of postoperative atrial fibrillation and therefore should be considered in patients undergoing AVR The operative approach should be selected according to surgeonrsquos technical expertise and what is best for specific patient profile
(Ann Thorac Surg 20181061881ndash9)
Full Sternotomy Hemisternotomy and Minithoracotomyfor Aortic Valve Surgery Is There a Difference
Elisa Mikus MD Simone Calvi MD Gianluca Campo MD Rita Pavasini MD Marco Paris MD Eliana Raviola MD Marco Panzavolta MD Alberto Tripodi MD Roberto Ferrari MD PhD and Mauro Del Giglio MD PhD
Cardiothoracic and Vascular Department Maria Cecilia Hospital GVM Care amp Research Cotignola (RA) Cardiovascular Institute Azienda Ospedaliero-Universitaria di Ferrara Cona (FE) and Cardiovascular Department Istituto Clinico San Rocco Ome (BS) Italy
(Ann Thorac Surg 20181061782ndash8)
Full Sternotomy Hemisternotomy and Minithoracotomyfor Aortic Valve Surgery Is There a Difference
bull The study included all 1907 consecutive patients hospitalized at the Maria Cecilia Hospital (Cotignola RA Italy) between January 2010 and March 2017 undergoing isolated AVR through PUH RAT or MS The choice of the approach was left to surgeonrsquos preference To adjust for differences in baseline characteristics between the study groups a propensity score matching was performed Linear and logistic regression analyses were performed
bull Results Partial upper hemisternotomy was performed in 820 patients (43) right anterior minithoracotomy in 488 (26) and median sternotomy in 599 (31) After propensity score matching three groups of 377 patients were obtained Cardiopulmonary bypass and crossclamptimes were shorter in the right anterior minithoracotomy group than in the median sternotomy and partial upper hemisternotomy groups (p lt 0001) No significant differences in in-hospital mortality were observed (p [ 09) Renal failure (odds ratio 54 95 confidence interval 23 to 114 p lt 00001) extracardiac arteriopathy (odds ratio 29 95 confidence interval 11 to 67 p [ 0017) and left ventricular ejection fraction (odds ratio 096 95 confidence interval 093 to 099 p [ 0009) emerged as independent predictors of in hospital mortality
bull Conclusions Minimal-access isolated aortic valve surgery is a reproducible safe and effective procedure with similar outcomes and operating times compared with conventional sternotomy
Ann Thorac Surg 20181061782ndash8
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full median sternotomy for aortic valve replacement
Sukumaran K Nair FRCS(CTh) et al
bull From the a Department of Cardiothoracic Surgery PapworthHospital Cambridge United Kingdom Freeman Hospital Newcastle upon Tyne United Kingdom Leeds Institute of Clinical Trials Research University of Leeds Leeds United Kingdom Health Economics Research Group Brunel University London London United Kingdom and London School of Hygiene and Tropical Medicine Keppel Street London United Kingdom
J Thorac Cardiovasc Surg 20181562124-32
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacement
bull Methods This RCT compared MS with FS for first-time isolated AVR in 2 United Kingdom National Health Service hospitals Primary endpoints were duration of postoperative hospital stay and the time to fitness for discharge from hospital after AVR analyzed in the intent-to-treat population
bull Results In this RCT 222 patients were recruited and randomized (n frac14 118 in the MS group n frac14 104 in the FS group) Compared with the FS group the MS group had a longer hospital length of stay (mean 95 days vs 86 days) and took longer to achieve fitness for discharge home (mean 85 days vs 75 days) Adjusting for valve type sex and surgeon hazard ratios (HRs) from Cox models did not show a statistically significant effect of MS (relative to FS) on either hospital stay (HR 0874 95 confidence interval [CI] 0668-1143 P frac14 3246) or time to fitness for discharge (HR 0907 95 CI 0688-1197 P value frac14 4914) During a mean follow-up of 760 days (745 days for the MS group and 777 days for the FS group) 12 patients (10) in the MS group and 7 patients (7) in the FS group died (HR 1871 95 CI 0723-4844 P frac14 1966) Average extra cost for MS was pound1714 during the first 12 months
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacementCentral Message
In the United Kingdomrsquos National Health Service compared with a conventional median sternotomy approach for surgical aortic valve replacement mini-sternotomy did not hasten recovery or hospital discharge and was not cost-effective
Measuring What Matters
Having lived through the growth of percutaneous coronary intervention and now seeing the expansion of transcatheter aortic valve replacement I find myself asking the somewhat existential question ldquoAre we measuring what matters to patientsrdquo
Thoralf M Sundt MD Division of Cardiac Surgery
Massachusetts General Hospital Boston Massachusetts
Ann Thorac Surg 20181061602
Measuring What Matters
In a study performed at Dartmouth-Hitchcock
elderly patients prioritized ability to pursue activities maintaining independence and reducing symptoms
over
mortality benefit
Coleywright M et al Patients defined goals for the treatment of sever AVS a qualitative analysis
Health Expect 2016 191036-43
Measuring What Matters
These sorts of ldquosoftrdquo outcome variables are challenging to us We think of ourselvesmdashat least I domdashas medical scientists interested in ldquohardrdquo endpoints
But our patients are challenging us to consider what they value most not what we can measure easily Irsquod say it is time for us to broaden our horizons and revisit how we can better measure what matters
Ann Thorac Surg 20181061602

HISTORY I
From January to April 1996 this approach was em- ployed in 25 patients with isolated aortic valve disease Repairs of the aortic valve were carried out in 6 patients Nineteen patients had valve replacement 10 Carpentier- Edwards pericardial valves 8 aortic homografts and 1 St Jude valve There were no deaths reoperations for bleeding strokes or wound infections
History II
bull Minimally invasive cardiac valve surgery improves patient satisfaction while reducing costs of cardiac valve replacement and repair
bull L H Cohn D H Adams G S Couper D P Bichell D M Rosborough S P Sears and S F Aranki
bull From the Division of Cardiac Surgery Brigham and Womens Hospital Department of Surgery Harvard Medical School Boston Massachusetts
bull Ann Surg 1997 Oct 226(4) 421ndash428
History II
History II
bull Of the 84 patients there were 2 operative mortalities both in class IV aortic patients from multisystem organ failure There was no operative mortality in the patients undergoing mitral valve replacement or repair The operations were carried out with the same accuracy and attention to detail as with the conventional operation There was minimal postoperative bleeding cerebral vascular accidents or other major morbidity Groin cannulation complications primarily were related to atherosclerotic femoral arteries
Minimally Invasive and Conventional Aortic Valve ReplacementA Propensity Score Analysis
Department of Adult Cardiac Surgery Daniyar Gilmanov G Pasquinucci Heart Hospital Massa Italy
Methods
bull This is a retrospective observational cohort study of prospectively collected data on 709 patients undergoing isolated primary aortic valve replacement between 2004 and 2011 Of these 338
were performed through either right anterior minithoracotomy or upper ministernotomy With propensity score matching 182 patients (minimally invasive group) were compared with 182
patients in conventional sternotomy (control group)
Conclusions
bull Our experience shows that mini-access isolated aortic valve surgery is a reproducible safe and effective procedure and reduces assisted ventilation duration the need for blood product
transfusion and incidence of post-surgery atrial fibrillation
(Ann Thorac Surg 201396837ndash43)
Introduction
bull The approaches taken under the umbrella of minimally-invasive surgical aortic valve replacement (MICS SAVR) essentially consist of a variety of access options to the aortic valve using smaller incisions
bull Importantly there is no convention or consensus as to what size incision qualifies as a minimally-invasive procedure
bull Furthermore lsquominimally-invasiversquo cardiac surgery (MICS) arguably is somewhat of a misnomer certainly in comparison interventions such as TAVR because the most invasive portions of the surgery including cross-clamping of the aorta ischemic cardiac arrest the use of cardiopulmonary bypass and opening of the aorta with introduction of air into the heart chambers all remain the same
Mahesh K Ramchandani MDAnnals of Thoracic Surgery ( in press)
ΜΙΝΙ
ν=28
ΥΠΟΛΟΙΠΟΙ
ν=131Ηλικία 722plusmn84 704plusmn98Γυναίκες(n) 10 (357) 58(442)Euro score 227plusmn2 18plusmn19ΜΕΘ μέρες 196plusmn06 198plusmn11Μέρες νοσηλείας 6plusmn218 57plusmn18Νοσηλεία lt5
μέρες
14(50) 37(517)
Μετάγγιση
RBC UNITS
12plusmn09 15plusmn13
CPB min 1124plusmn37 933plusmn33Μηχανικός
αερισμός (ώρες)
86plusmn45 104plusmn13
ΜΙΝΙ Στερνοτομές 2018Μεμονωμένη αντικατάσταση αορτικής βαλβίδας 2018
Σύνολο 159- ΜΙΝΙ 28 (176)
Χαρακτηριστικά ασθενών Επιπλοκές
ΜΙΝΙ
ν=28
ΥΠΟΛΟΙΠΟΙ
ν=131
P value
LCOS(n) 1 (36) 3(23) 069
Επαναδιάνοιξη(n) 0 4(31) 035
Λοιμώξεις
στερνοτομής(n)
1 (36) 3(23) 069
Stroke 0 2(15) 051
NIV 1 (36) 6(46) 081
Επαναδιασωλήνωση 0 3(23) 042
AKI(n) 3(107) 12(92) 079
Κολπική μαρμαρυγή 7(25) 40(305) 056
Θάνατος 0 3(23) 042
Minimally Invasive Approaches to Surgical Aortic Valve Replacement
A Meta-Analysis
Carolyn Chang BS Sajjad Raza MD Salah E Altarabsheh MD Sarah Delozier PhD Umesh M Sharma MD MBA Aisha Zia MD Muhammad Shahzeb Khan MD Mandy Neudecker MS Alan H Markowitz MD Joseph F Sabik III MD and Salil V Deo MD
Cleveland Ohio
(Ann Thorac Surg 20181061881ndash9)
Minimally Invasive Approaches to Surgical Aortic Valve ReplacementA Meta-Analysis
The outcomes of the 2 minimally invasive aortic valve replacement (AVR) strategiesmdashmini-sternotomy (AVR-st) and right anterior thoracotomy (AVR-th) with each other and with conventional AVR (cAVR)
Searched Medline PubMed Embase and Web of Science in December 2017 for studies comparing AVR-st AVR-th and cAVR Endpoints studied included hospital mortality stroke atrial fibrillation cardiopulmonary bypass (CPB) time and length of stay
A total of 19 studies (gt10000 pooled patients) met the inclusion criteria
bull Mortality (p [ 006) and stroke (p [ 015) were comparable between minimally invasive and conventional AVR
bull CPB times were longer with AVR-th versus cAVR (124 minutes [range 5 to 19] p lt 001) In the AVR-th cohort CPB duration was weakly inversely related to study size (p [ 006)
bull Atrial fibrillation was much less after AVR-th (odds ratio 047 [035 to 063] p lt 0001)
bull Hospital stay was significantly lower after minimally invasive surgery (08 [04 to 13] days p lt 001
Minimally invasive approaches to AVR yield excellent outcomes in high-volume centers They reduce hospital stay and incidence of postoperative atrial fibrillation and therefore should be considered in patients undergoing AVR The operative approach should be selected according to surgeonrsquos technical expertise and what is best for specific patient profile
(Ann Thorac Surg 20181061881ndash9)
Full Sternotomy Hemisternotomy and Minithoracotomyfor Aortic Valve Surgery Is There a Difference
Elisa Mikus MD Simone Calvi MD Gianluca Campo MD Rita Pavasini MD Marco Paris MD Eliana Raviola MD Marco Panzavolta MD Alberto Tripodi MD Roberto Ferrari MD PhD and Mauro Del Giglio MD PhD
Cardiothoracic and Vascular Department Maria Cecilia Hospital GVM Care amp Research Cotignola (RA) Cardiovascular Institute Azienda Ospedaliero-Universitaria di Ferrara Cona (FE) and Cardiovascular Department Istituto Clinico San Rocco Ome (BS) Italy
(Ann Thorac Surg 20181061782ndash8)
Full Sternotomy Hemisternotomy and Minithoracotomyfor Aortic Valve Surgery Is There a Difference
bull The study included all 1907 consecutive patients hospitalized at the Maria Cecilia Hospital (Cotignola RA Italy) between January 2010 and March 2017 undergoing isolated AVR through PUH RAT or MS The choice of the approach was left to surgeonrsquos preference To adjust for differences in baseline characteristics between the study groups a propensity score matching was performed Linear and logistic regression analyses were performed
bull Results Partial upper hemisternotomy was performed in 820 patients (43) right anterior minithoracotomy in 488 (26) and median sternotomy in 599 (31) After propensity score matching three groups of 377 patients were obtained Cardiopulmonary bypass and crossclamptimes were shorter in the right anterior minithoracotomy group than in the median sternotomy and partial upper hemisternotomy groups (p lt 0001) No significant differences in in-hospital mortality were observed (p [ 09) Renal failure (odds ratio 54 95 confidence interval 23 to 114 p lt 00001) extracardiac arteriopathy (odds ratio 29 95 confidence interval 11 to 67 p [ 0017) and left ventricular ejection fraction (odds ratio 096 95 confidence interval 093 to 099 p [ 0009) emerged as independent predictors of in hospital mortality
bull Conclusions Minimal-access isolated aortic valve surgery is a reproducible safe and effective procedure with similar outcomes and operating times compared with conventional sternotomy
Ann Thorac Surg 20181061782ndash8
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full median sternotomy for aortic valve replacement
Sukumaran K Nair FRCS(CTh) et al
bull From the a Department of Cardiothoracic Surgery PapworthHospital Cambridge United Kingdom Freeman Hospital Newcastle upon Tyne United Kingdom Leeds Institute of Clinical Trials Research University of Leeds Leeds United Kingdom Health Economics Research Group Brunel University London London United Kingdom and London School of Hygiene and Tropical Medicine Keppel Street London United Kingdom
J Thorac Cardiovasc Surg 20181562124-32
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacement
bull Methods This RCT compared MS with FS for first-time isolated AVR in 2 United Kingdom National Health Service hospitals Primary endpoints were duration of postoperative hospital stay and the time to fitness for discharge from hospital after AVR analyzed in the intent-to-treat population
bull Results In this RCT 222 patients were recruited and randomized (n frac14 118 in the MS group n frac14 104 in the FS group) Compared with the FS group the MS group had a longer hospital length of stay (mean 95 days vs 86 days) and took longer to achieve fitness for discharge home (mean 85 days vs 75 days) Adjusting for valve type sex and surgeon hazard ratios (HRs) from Cox models did not show a statistically significant effect of MS (relative to FS) on either hospital stay (HR 0874 95 confidence interval [CI] 0668-1143 P frac14 3246) or time to fitness for discharge (HR 0907 95 CI 0688-1197 P value frac14 4914) During a mean follow-up of 760 days (745 days for the MS group and 777 days for the FS group) 12 patients (10) in the MS group and 7 patients (7) in the FS group died (HR 1871 95 CI 0723-4844 P frac14 1966) Average extra cost for MS was pound1714 during the first 12 months
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacementCentral Message
In the United Kingdomrsquos National Health Service compared with a conventional median sternotomy approach for surgical aortic valve replacement mini-sternotomy did not hasten recovery or hospital discharge and was not cost-effective
Measuring What Matters
Having lived through the growth of percutaneous coronary intervention and now seeing the expansion of transcatheter aortic valve replacement I find myself asking the somewhat existential question ldquoAre we measuring what matters to patientsrdquo
Thoralf M Sundt MD Division of Cardiac Surgery
Massachusetts General Hospital Boston Massachusetts
Ann Thorac Surg 20181061602
Measuring What Matters
In a study performed at Dartmouth-Hitchcock
elderly patients prioritized ability to pursue activities maintaining independence and reducing symptoms
over
mortality benefit
Coleywright M et al Patients defined goals for the treatment of sever AVS a qualitative analysis
Health Expect 2016 191036-43
Measuring What Matters
These sorts of ldquosoftrdquo outcome variables are challenging to us We think of ourselvesmdashat least I domdashas medical scientists interested in ldquohardrdquo endpoints
But our patients are challenging us to consider what they value most not what we can measure easily Irsquod say it is time for us to broaden our horizons and revisit how we can better measure what matters
Ann Thorac Surg 20181061602

History II
bull Minimally invasive cardiac valve surgery improves patient satisfaction while reducing costs of cardiac valve replacement and repair
bull L H Cohn D H Adams G S Couper D P Bichell D M Rosborough S P Sears and S F Aranki
bull From the Division of Cardiac Surgery Brigham and Womens Hospital Department of Surgery Harvard Medical School Boston Massachusetts
bull Ann Surg 1997 Oct 226(4) 421ndash428
History II
History II
bull Of the 84 patients there were 2 operative mortalities both in class IV aortic patients from multisystem organ failure There was no operative mortality in the patients undergoing mitral valve replacement or repair The operations were carried out with the same accuracy and attention to detail as with the conventional operation There was minimal postoperative bleeding cerebral vascular accidents or other major morbidity Groin cannulation complications primarily were related to atherosclerotic femoral arteries
Minimally Invasive and Conventional Aortic Valve ReplacementA Propensity Score Analysis
Department of Adult Cardiac Surgery Daniyar Gilmanov G Pasquinucci Heart Hospital Massa Italy
Methods
bull This is a retrospective observational cohort study of prospectively collected data on 709 patients undergoing isolated primary aortic valve replacement between 2004 and 2011 Of these 338
were performed through either right anterior minithoracotomy or upper ministernotomy With propensity score matching 182 patients (minimally invasive group) were compared with 182
patients in conventional sternotomy (control group)
Conclusions
bull Our experience shows that mini-access isolated aortic valve surgery is a reproducible safe and effective procedure and reduces assisted ventilation duration the need for blood product
transfusion and incidence of post-surgery atrial fibrillation
(Ann Thorac Surg 201396837ndash43)
Introduction
bull The approaches taken under the umbrella of minimally-invasive surgical aortic valve replacement (MICS SAVR) essentially consist of a variety of access options to the aortic valve using smaller incisions
bull Importantly there is no convention or consensus as to what size incision qualifies as a minimally-invasive procedure
bull Furthermore lsquominimally-invasiversquo cardiac surgery (MICS) arguably is somewhat of a misnomer certainly in comparison interventions such as TAVR because the most invasive portions of the surgery including cross-clamping of the aorta ischemic cardiac arrest the use of cardiopulmonary bypass and opening of the aorta with introduction of air into the heart chambers all remain the same
Mahesh K Ramchandani MDAnnals of Thoracic Surgery ( in press)
ΜΙΝΙ
ν=28
ΥΠΟΛΟΙΠΟΙ
ν=131Ηλικία 722plusmn84 704plusmn98Γυναίκες(n) 10 (357) 58(442)Euro score 227plusmn2 18plusmn19ΜΕΘ μέρες 196plusmn06 198plusmn11Μέρες νοσηλείας 6plusmn218 57plusmn18Νοσηλεία lt5
μέρες
14(50) 37(517)
Μετάγγιση
RBC UNITS
12plusmn09 15plusmn13
CPB min 1124plusmn37 933plusmn33Μηχανικός
αερισμός (ώρες)
86plusmn45 104plusmn13
ΜΙΝΙ Στερνοτομές 2018Μεμονωμένη αντικατάσταση αορτικής βαλβίδας 2018
Σύνολο 159- ΜΙΝΙ 28 (176)
Χαρακτηριστικά ασθενών Επιπλοκές
ΜΙΝΙ
ν=28
ΥΠΟΛΟΙΠΟΙ
ν=131
P value
LCOS(n) 1 (36) 3(23) 069
Επαναδιάνοιξη(n) 0 4(31) 035
Λοιμώξεις
στερνοτομής(n)
1 (36) 3(23) 069
Stroke 0 2(15) 051
NIV 1 (36) 6(46) 081
Επαναδιασωλήνωση 0 3(23) 042
AKI(n) 3(107) 12(92) 079
Κολπική μαρμαρυγή 7(25) 40(305) 056
Θάνατος 0 3(23) 042
Minimally Invasive Approaches to Surgical Aortic Valve Replacement
A Meta-Analysis
Carolyn Chang BS Sajjad Raza MD Salah E Altarabsheh MD Sarah Delozier PhD Umesh M Sharma MD MBA Aisha Zia MD Muhammad Shahzeb Khan MD Mandy Neudecker MS Alan H Markowitz MD Joseph F Sabik III MD and Salil V Deo MD
Cleveland Ohio
(Ann Thorac Surg 20181061881ndash9)
Minimally Invasive Approaches to Surgical Aortic Valve ReplacementA Meta-Analysis
The outcomes of the 2 minimally invasive aortic valve replacement (AVR) strategiesmdashmini-sternotomy (AVR-st) and right anterior thoracotomy (AVR-th) with each other and with conventional AVR (cAVR)
Searched Medline PubMed Embase and Web of Science in December 2017 for studies comparing AVR-st AVR-th and cAVR Endpoints studied included hospital mortality stroke atrial fibrillation cardiopulmonary bypass (CPB) time and length of stay
A total of 19 studies (gt10000 pooled patients) met the inclusion criteria
bull Mortality (p [ 006) and stroke (p [ 015) were comparable between minimally invasive and conventional AVR
bull CPB times were longer with AVR-th versus cAVR (124 minutes [range 5 to 19] p lt 001) In the AVR-th cohort CPB duration was weakly inversely related to study size (p [ 006)
bull Atrial fibrillation was much less after AVR-th (odds ratio 047 [035 to 063] p lt 0001)
bull Hospital stay was significantly lower after minimally invasive surgery (08 [04 to 13] days p lt 001
Minimally invasive approaches to AVR yield excellent outcomes in high-volume centers They reduce hospital stay and incidence of postoperative atrial fibrillation and therefore should be considered in patients undergoing AVR The operative approach should be selected according to surgeonrsquos technical expertise and what is best for specific patient profile
(Ann Thorac Surg 20181061881ndash9)
Full Sternotomy Hemisternotomy and Minithoracotomyfor Aortic Valve Surgery Is There a Difference
Elisa Mikus MD Simone Calvi MD Gianluca Campo MD Rita Pavasini MD Marco Paris MD Eliana Raviola MD Marco Panzavolta MD Alberto Tripodi MD Roberto Ferrari MD PhD and Mauro Del Giglio MD PhD
Cardiothoracic and Vascular Department Maria Cecilia Hospital GVM Care amp Research Cotignola (RA) Cardiovascular Institute Azienda Ospedaliero-Universitaria di Ferrara Cona (FE) and Cardiovascular Department Istituto Clinico San Rocco Ome (BS) Italy
(Ann Thorac Surg 20181061782ndash8)
Full Sternotomy Hemisternotomy and Minithoracotomyfor Aortic Valve Surgery Is There a Difference
bull The study included all 1907 consecutive patients hospitalized at the Maria Cecilia Hospital (Cotignola RA Italy) between January 2010 and March 2017 undergoing isolated AVR through PUH RAT or MS The choice of the approach was left to surgeonrsquos preference To adjust for differences in baseline characteristics between the study groups a propensity score matching was performed Linear and logistic regression analyses were performed
bull Results Partial upper hemisternotomy was performed in 820 patients (43) right anterior minithoracotomy in 488 (26) and median sternotomy in 599 (31) After propensity score matching three groups of 377 patients were obtained Cardiopulmonary bypass and crossclamptimes were shorter in the right anterior minithoracotomy group than in the median sternotomy and partial upper hemisternotomy groups (p lt 0001) No significant differences in in-hospital mortality were observed (p [ 09) Renal failure (odds ratio 54 95 confidence interval 23 to 114 p lt 00001) extracardiac arteriopathy (odds ratio 29 95 confidence interval 11 to 67 p [ 0017) and left ventricular ejection fraction (odds ratio 096 95 confidence interval 093 to 099 p [ 0009) emerged as independent predictors of in hospital mortality
bull Conclusions Minimal-access isolated aortic valve surgery is a reproducible safe and effective procedure with similar outcomes and operating times compared with conventional sternotomy
Ann Thorac Surg 20181061782ndash8
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full median sternotomy for aortic valve replacement
Sukumaran K Nair FRCS(CTh) et al
bull From the a Department of Cardiothoracic Surgery PapworthHospital Cambridge United Kingdom Freeman Hospital Newcastle upon Tyne United Kingdom Leeds Institute of Clinical Trials Research University of Leeds Leeds United Kingdom Health Economics Research Group Brunel University London London United Kingdom and London School of Hygiene and Tropical Medicine Keppel Street London United Kingdom
J Thorac Cardiovasc Surg 20181562124-32
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacement
bull Methods This RCT compared MS with FS for first-time isolated AVR in 2 United Kingdom National Health Service hospitals Primary endpoints were duration of postoperative hospital stay and the time to fitness for discharge from hospital after AVR analyzed in the intent-to-treat population
bull Results In this RCT 222 patients were recruited and randomized (n frac14 118 in the MS group n frac14 104 in the FS group) Compared with the FS group the MS group had a longer hospital length of stay (mean 95 days vs 86 days) and took longer to achieve fitness for discharge home (mean 85 days vs 75 days) Adjusting for valve type sex and surgeon hazard ratios (HRs) from Cox models did not show a statistically significant effect of MS (relative to FS) on either hospital stay (HR 0874 95 confidence interval [CI] 0668-1143 P frac14 3246) or time to fitness for discharge (HR 0907 95 CI 0688-1197 P value frac14 4914) During a mean follow-up of 760 days (745 days for the MS group and 777 days for the FS group) 12 patients (10) in the MS group and 7 patients (7) in the FS group died (HR 1871 95 CI 0723-4844 P frac14 1966) Average extra cost for MS was pound1714 during the first 12 months
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacementCentral Message
In the United Kingdomrsquos National Health Service compared with a conventional median sternotomy approach for surgical aortic valve replacement mini-sternotomy did not hasten recovery or hospital discharge and was not cost-effective
Measuring What Matters
Having lived through the growth of percutaneous coronary intervention and now seeing the expansion of transcatheter aortic valve replacement I find myself asking the somewhat existential question ldquoAre we measuring what matters to patientsrdquo
Thoralf M Sundt MD Division of Cardiac Surgery
Massachusetts General Hospital Boston Massachusetts
Ann Thorac Surg 20181061602
Measuring What Matters
In a study performed at Dartmouth-Hitchcock
elderly patients prioritized ability to pursue activities maintaining independence and reducing symptoms
over
mortality benefit
Coleywright M et al Patients defined goals for the treatment of sever AVS a qualitative analysis
Health Expect 2016 191036-43
Measuring What Matters
These sorts of ldquosoftrdquo outcome variables are challenging to us We think of ourselvesmdashat least I domdashas medical scientists interested in ldquohardrdquo endpoints
But our patients are challenging us to consider what they value most not what we can measure easily Irsquod say it is time for us to broaden our horizons and revisit how we can better measure what matters
Ann Thorac Surg 20181061602

History II
History II
bull Of the 84 patients there were 2 operative mortalities both in class IV aortic patients from multisystem organ failure There was no operative mortality in the patients undergoing mitral valve replacement or repair The operations were carried out with the same accuracy and attention to detail as with the conventional operation There was minimal postoperative bleeding cerebral vascular accidents or other major morbidity Groin cannulation complications primarily were related to atherosclerotic femoral arteries
Minimally Invasive and Conventional Aortic Valve ReplacementA Propensity Score Analysis
Department of Adult Cardiac Surgery Daniyar Gilmanov G Pasquinucci Heart Hospital Massa Italy
Methods
bull This is a retrospective observational cohort study of prospectively collected data on 709 patients undergoing isolated primary aortic valve replacement between 2004 and 2011 Of these 338
were performed through either right anterior minithoracotomy or upper ministernotomy With propensity score matching 182 patients (minimally invasive group) were compared with 182
patients in conventional sternotomy (control group)
Conclusions
bull Our experience shows that mini-access isolated aortic valve surgery is a reproducible safe and effective procedure and reduces assisted ventilation duration the need for blood product
transfusion and incidence of post-surgery atrial fibrillation
(Ann Thorac Surg 201396837ndash43)
Introduction
bull The approaches taken under the umbrella of minimally-invasive surgical aortic valve replacement (MICS SAVR) essentially consist of a variety of access options to the aortic valve using smaller incisions
bull Importantly there is no convention or consensus as to what size incision qualifies as a minimally-invasive procedure
bull Furthermore lsquominimally-invasiversquo cardiac surgery (MICS) arguably is somewhat of a misnomer certainly in comparison interventions such as TAVR because the most invasive portions of the surgery including cross-clamping of the aorta ischemic cardiac arrest the use of cardiopulmonary bypass and opening of the aorta with introduction of air into the heart chambers all remain the same
Mahesh K Ramchandani MDAnnals of Thoracic Surgery ( in press)
ΜΙΝΙ
ν=28
ΥΠΟΛΟΙΠΟΙ
ν=131Ηλικία 722plusmn84 704plusmn98Γυναίκες(n) 10 (357) 58(442)Euro score 227plusmn2 18plusmn19ΜΕΘ μέρες 196plusmn06 198plusmn11Μέρες νοσηλείας 6plusmn218 57plusmn18Νοσηλεία lt5
μέρες
14(50) 37(517)
Μετάγγιση
RBC UNITS
12plusmn09 15plusmn13
CPB min 1124plusmn37 933plusmn33Μηχανικός
αερισμός (ώρες)
86plusmn45 104plusmn13
ΜΙΝΙ Στερνοτομές 2018Μεμονωμένη αντικατάσταση αορτικής βαλβίδας 2018
Σύνολο 159- ΜΙΝΙ 28 (176)
Χαρακτηριστικά ασθενών Επιπλοκές
ΜΙΝΙ
ν=28
ΥΠΟΛΟΙΠΟΙ
ν=131
P value
LCOS(n) 1 (36) 3(23) 069
Επαναδιάνοιξη(n) 0 4(31) 035
Λοιμώξεις
στερνοτομής(n)
1 (36) 3(23) 069
Stroke 0 2(15) 051
NIV 1 (36) 6(46) 081
Επαναδιασωλήνωση 0 3(23) 042
AKI(n) 3(107) 12(92) 079
Κολπική μαρμαρυγή 7(25) 40(305) 056
Θάνατος 0 3(23) 042
Minimally Invasive Approaches to Surgical Aortic Valve Replacement
A Meta-Analysis
Carolyn Chang BS Sajjad Raza MD Salah E Altarabsheh MD Sarah Delozier PhD Umesh M Sharma MD MBA Aisha Zia MD Muhammad Shahzeb Khan MD Mandy Neudecker MS Alan H Markowitz MD Joseph F Sabik III MD and Salil V Deo MD
Cleveland Ohio
(Ann Thorac Surg 20181061881ndash9)
Minimally Invasive Approaches to Surgical Aortic Valve ReplacementA Meta-Analysis
The outcomes of the 2 minimally invasive aortic valve replacement (AVR) strategiesmdashmini-sternotomy (AVR-st) and right anterior thoracotomy (AVR-th) with each other and with conventional AVR (cAVR)
Searched Medline PubMed Embase and Web of Science in December 2017 for studies comparing AVR-st AVR-th and cAVR Endpoints studied included hospital mortality stroke atrial fibrillation cardiopulmonary bypass (CPB) time and length of stay
A total of 19 studies (gt10000 pooled patients) met the inclusion criteria
bull Mortality (p [ 006) and stroke (p [ 015) were comparable between minimally invasive and conventional AVR
bull CPB times were longer with AVR-th versus cAVR (124 minutes [range 5 to 19] p lt 001) In the AVR-th cohort CPB duration was weakly inversely related to study size (p [ 006)
bull Atrial fibrillation was much less after AVR-th (odds ratio 047 [035 to 063] p lt 0001)
bull Hospital stay was significantly lower after minimally invasive surgery (08 [04 to 13] days p lt 001
Minimally invasive approaches to AVR yield excellent outcomes in high-volume centers They reduce hospital stay and incidence of postoperative atrial fibrillation and therefore should be considered in patients undergoing AVR The operative approach should be selected according to surgeonrsquos technical expertise and what is best for specific patient profile
(Ann Thorac Surg 20181061881ndash9)
Full Sternotomy Hemisternotomy and Minithoracotomyfor Aortic Valve Surgery Is There a Difference
Elisa Mikus MD Simone Calvi MD Gianluca Campo MD Rita Pavasini MD Marco Paris MD Eliana Raviola MD Marco Panzavolta MD Alberto Tripodi MD Roberto Ferrari MD PhD and Mauro Del Giglio MD PhD
Cardiothoracic and Vascular Department Maria Cecilia Hospital GVM Care amp Research Cotignola (RA) Cardiovascular Institute Azienda Ospedaliero-Universitaria di Ferrara Cona (FE) and Cardiovascular Department Istituto Clinico San Rocco Ome (BS) Italy
(Ann Thorac Surg 20181061782ndash8)
Full Sternotomy Hemisternotomy and Minithoracotomyfor Aortic Valve Surgery Is There a Difference
bull The study included all 1907 consecutive patients hospitalized at the Maria Cecilia Hospital (Cotignola RA Italy) between January 2010 and March 2017 undergoing isolated AVR through PUH RAT or MS The choice of the approach was left to surgeonrsquos preference To adjust for differences in baseline characteristics between the study groups a propensity score matching was performed Linear and logistic regression analyses were performed
bull Results Partial upper hemisternotomy was performed in 820 patients (43) right anterior minithoracotomy in 488 (26) and median sternotomy in 599 (31) After propensity score matching three groups of 377 patients were obtained Cardiopulmonary bypass and crossclamptimes were shorter in the right anterior minithoracotomy group than in the median sternotomy and partial upper hemisternotomy groups (p lt 0001) No significant differences in in-hospital mortality were observed (p [ 09) Renal failure (odds ratio 54 95 confidence interval 23 to 114 p lt 00001) extracardiac arteriopathy (odds ratio 29 95 confidence interval 11 to 67 p [ 0017) and left ventricular ejection fraction (odds ratio 096 95 confidence interval 093 to 099 p [ 0009) emerged as independent predictors of in hospital mortality
bull Conclusions Minimal-access isolated aortic valve surgery is a reproducible safe and effective procedure with similar outcomes and operating times compared with conventional sternotomy
Ann Thorac Surg 20181061782ndash8
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full median sternotomy for aortic valve replacement
Sukumaran K Nair FRCS(CTh) et al
bull From the a Department of Cardiothoracic Surgery PapworthHospital Cambridge United Kingdom Freeman Hospital Newcastle upon Tyne United Kingdom Leeds Institute of Clinical Trials Research University of Leeds Leeds United Kingdom Health Economics Research Group Brunel University London London United Kingdom and London School of Hygiene and Tropical Medicine Keppel Street London United Kingdom
J Thorac Cardiovasc Surg 20181562124-32
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacement
bull Methods This RCT compared MS with FS for first-time isolated AVR in 2 United Kingdom National Health Service hospitals Primary endpoints were duration of postoperative hospital stay and the time to fitness for discharge from hospital after AVR analyzed in the intent-to-treat population
bull Results In this RCT 222 patients were recruited and randomized (n frac14 118 in the MS group n frac14 104 in the FS group) Compared with the FS group the MS group had a longer hospital length of stay (mean 95 days vs 86 days) and took longer to achieve fitness for discharge home (mean 85 days vs 75 days) Adjusting for valve type sex and surgeon hazard ratios (HRs) from Cox models did not show a statistically significant effect of MS (relative to FS) on either hospital stay (HR 0874 95 confidence interval [CI] 0668-1143 P frac14 3246) or time to fitness for discharge (HR 0907 95 CI 0688-1197 P value frac14 4914) During a mean follow-up of 760 days (745 days for the MS group and 777 days for the FS group) 12 patients (10) in the MS group and 7 patients (7) in the FS group died (HR 1871 95 CI 0723-4844 P frac14 1966) Average extra cost for MS was pound1714 during the first 12 months
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacementCentral Message
In the United Kingdomrsquos National Health Service compared with a conventional median sternotomy approach for surgical aortic valve replacement mini-sternotomy did not hasten recovery or hospital discharge and was not cost-effective
Measuring What Matters
Having lived through the growth of percutaneous coronary intervention and now seeing the expansion of transcatheter aortic valve replacement I find myself asking the somewhat existential question ldquoAre we measuring what matters to patientsrdquo
Thoralf M Sundt MD Division of Cardiac Surgery
Massachusetts General Hospital Boston Massachusetts
Ann Thorac Surg 20181061602
Measuring What Matters
In a study performed at Dartmouth-Hitchcock
elderly patients prioritized ability to pursue activities maintaining independence and reducing symptoms
over
mortality benefit
Coleywright M et al Patients defined goals for the treatment of sever AVS a qualitative analysis
Health Expect 2016 191036-43
Measuring What Matters
These sorts of ldquosoftrdquo outcome variables are challenging to us We think of ourselvesmdashat least I domdashas medical scientists interested in ldquohardrdquo endpoints
But our patients are challenging us to consider what they value most not what we can measure easily Irsquod say it is time for us to broaden our horizons and revisit how we can better measure what matters
Ann Thorac Surg 20181061602

History II
bull Of the 84 patients there were 2 operative mortalities both in class IV aortic patients from multisystem organ failure There was no operative mortality in the patients undergoing mitral valve replacement or repair The operations were carried out with the same accuracy and attention to detail as with the conventional operation There was minimal postoperative bleeding cerebral vascular accidents or other major morbidity Groin cannulation complications primarily were related to atherosclerotic femoral arteries
Minimally Invasive and Conventional Aortic Valve ReplacementA Propensity Score Analysis
Department of Adult Cardiac Surgery Daniyar Gilmanov G Pasquinucci Heart Hospital Massa Italy
Methods
bull This is a retrospective observational cohort study of prospectively collected data on 709 patients undergoing isolated primary aortic valve replacement between 2004 and 2011 Of these 338
were performed through either right anterior minithoracotomy or upper ministernotomy With propensity score matching 182 patients (minimally invasive group) were compared with 182
patients in conventional sternotomy (control group)
Conclusions
bull Our experience shows that mini-access isolated aortic valve surgery is a reproducible safe and effective procedure and reduces assisted ventilation duration the need for blood product
transfusion and incidence of post-surgery atrial fibrillation
(Ann Thorac Surg 201396837ndash43)
Introduction
bull The approaches taken under the umbrella of minimally-invasive surgical aortic valve replacement (MICS SAVR) essentially consist of a variety of access options to the aortic valve using smaller incisions
bull Importantly there is no convention or consensus as to what size incision qualifies as a minimally-invasive procedure
bull Furthermore lsquominimally-invasiversquo cardiac surgery (MICS) arguably is somewhat of a misnomer certainly in comparison interventions such as TAVR because the most invasive portions of the surgery including cross-clamping of the aorta ischemic cardiac arrest the use of cardiopulmonary bypass and opening of the aorta with introduction of air into the heart chambers all remain the same
Mahesh K Ramchandani MDAnnals of Thoracic Surgery ( in press)
ΜΙΝΙ
ν=28
ΥΠΟΛΟΙΠΟΙ
ν=131Ηλικία 722plusmn84 704plusmn98Γυναίκες(n) 10 (357) 58(442)Euro score 227plusmn2 18plusmn19ΜΕΘ μέρες 196plusmn06 198plusmn11Μέρες νοσηλείας 6plusmn218 57plusmn18Νοσηλεία lt5
μέρες
14(50) 37(517)
Μετάγγιση
RBC UNITS
12plusmn09 15plusmn13
CPB min 1124plusmn37 933plusmn33Μηχανικός
αερισμός (ώρες)
86plusmn45 104plusmn13
ΜΙΝΙ Στερνοτομές 2018Μεμονωμένη αντικατάσταση αορτικής βαλβίδας 2018
Σύνολο 159- ΜΙΝΙ 28 (176)
Χαρακτηριστικά ασθενών Επιπλοκές
ΜΙΝΙ
ν=28
ΥΠΟΛΟΙΠΟΙ
ν=131
P value
LCOS(n) 1 (36) 3(23) 069
Επαναδιάνοιξη(n) 0 4(31) 035
Λοιμώξεις
στερνοτομής(n)
1 (36) 3(23) 069
Stroke 0 2(15) 051
NIV 1 (36) 6(46) 081
Επαναδιασωλήνωση 0 3(23) 042
AKI(n) 3(107) 12(92) 079
Κολπική μαρμαρυγή 7(25) 40(305) 056
Θάνατος 0 3(23) 042
Minimally Invasive Approaches to Surgical Aortic Valve Replacement
A Meta-Analysis
Carolyn Chang BS Sajjad Raza MD Salah E Altarabsheh MD Sarah Delozier PhD Umesh M Sharma MD MBA Aisha Zia MD Muhammad Shahzeb Khan MD Mandy Neudecker MS Alan H Markowitz MD Joseph F Sabik III MD and Salil V Deo MD
Cleveland Ohio
(Ann Thorac Surg 20181061881ndash9)
Minimally Invasive Approaches to Surgical Aortic Valve ReplacementA Meta-Analysis
The outcomes of the 2 minimally invasive aortic valve replacement (AVR) strategiesmdashmini-sternotomy (AVR-st) and right anterior thoracotomy (AVR-th) with each other and with conventional AVR (cAVR)
Searched Medline PubMed Embase and Web of Science in December 2017 for studies comparing AVR-st AVR-th and cAVR Endpoints studied included hospital mortality stroke atrial fibrillation cardiopulmonary bypass (CPB) time and length of stay
A total of 19 studies (gt10000 pooled patients) met the inclusion criteria
bull Mortality (p [ 006) and stroke (p [ 015) were comparable between minimally invasive and conventional AVR
bull CPB times were longer with AVR-th versus cAVR (124 minutes [range 5 to 19] p lt 001) In the AVR-th cohort CPB duration was weakly inversely related to study size (p [ 006)
bull Atrial fibrillation was much less after AVR-th (odds ratio 047 [035 to 063] p lt 0001)
bull Hospital stay was significantly lower after minimally invasive surgery (08 [04 to 13] days p lt 001
Minimally invasive approaches to AVR yield excellent outcomes in high-volume centers They reduce hospital stay and incidence of postoperative atrial fibrillation and therefore should be considered in patients undergoing AVR The operative approach should be selected according to surgeonrsquos technical expertise and what is best for specific patient profile
(Ann Thorac Surg 20181061881ndash9)
Full Sternotomy Hemisternotomy and Minithoracotomyfor Aortic Valve Surgery Is There a Difference
Elisa Mikus MD Simone Calvi MD Gianluca Campo MD Rita Pavasini MD Marco Paris MD Eliana Raviola MD Marco Panzavolta MD Alberto Tripodi MD Roberto Ferrari MD PhD and Mauro Del Giglio MD PhD
Cardiothoracic and Vascular Department Maria Cecilia Hospital GVM Care amp Research Cotignola (RA) Cardiovascular Institute Azienda Ospedaliero-Universitaria di Ferrara Cona (FE) and Cardiovascular Department Istituto Clinico San Rocco Ome (BS) Italy
(Ann Thorac Surg 20181061782ndash8)
Full Sternotomy Hemisternotomy and Minithoracotomyfor Aortic Valve Surgery Is There a Difference
bull The study included all 1907 consecutive patients hospitalized at the Maria Cecilia Hospital (Cotignola RA Italy) between January 2010 and March 2017 undergoing isolated AVR through PUH RAT or MS The choice of the approach was left to surgeonrsquos preference To adjust for differences in baseline characteristics between the study groups a propensity score matching was performed Linear and logistic regression analyses were performed
bull Results Partial upper hemisternotomy was performed in 820 patients (43) right anterior minithoracotomy in 488 (26) and median sternotomy in 599 (31) After propensity score matching three groups of 377 patients were obtained Cardiopulmonary bypass and crossclamptimes were shorter in the right anterior minithoracotomy group than in the median sternotomy and partial upper hemisternotomy groups (p lt 0001) No significant differences in in-hospital mortality were observed (p [ 09) Renal failure (odds ratio 54 95 confidence interval 23 to 114 p lt 00001) extracardiac arteriopathy (odds ratio 29 95 confidence interval 11 to 67 p [ 0017) and left ventricular ejection fraction (odds ratio 096 95 confidence interval 093 to 099 p [ 0009) emerged as independent predictors of in hospital mortality
bull Conclusions Minimal-access isolated aortic valve surgery is a reproducible safe and effective procedure with similar outcomes and operating times compared with conventional sternotomy
Ann Thorac Surg 20181061782ndash8
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full median sternotomy for aortic valve replacement
Sukumaran K Nair FRCS(CTh) et al
bull From the a Department of Cardiothoracic Surgery PapworthHospital Cambridge United Kingdom Freeman Hospital Newcastle upon Tyne United Kingdom Leeds Institute of Clinical Trials Research University of Leeds Leeds United Kingdom Health Economics Research Group Brunel University London London United Kingdom and London School of Hygiene and Tropical Medicine Keppel Street London United Kingdom
J Thorac Cardiovasc Surg 20181562124-32
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacement
bull Methods This RCT compared MS with FS for first-time isolated AVR in 2 United Kingdom National Health Service hospitals Primary endpoints were duration of postoperative hospital stay and the time to fitness for discharge from hospital after AVR analyzed in the intent-to-treat population
bull Results In this RCT 222 patients were recruited and randomized (n frac14 118 in the MS group n frac14 104 in the FS group) Compared with the FS group the MS group had a longer hospital length of stay (mean 95 days vs 86 days) and took longer to achieve fitness for discharge home (mean 85 days vs 75 days) Adjusting for valve type sex and surgeon hazard ratios (HRs) from Cox models did not show a statistically significant effect of MS (relative to FS) on either hospital stay (HR 0874 95 confidence interval [CI] 0668-1143 P frac14 3246) or time to fitness for discharge (HR 0907 95 CI 0688-1197 P value frac14 4914) During a mean follow-up of 760 days (745 days for the MS group and 777 days for the FS group) 12 patients (10) in the MS group and 7 patients (7) in the FS group died (HR 1871 95 CI 0723-4844 P frac14 1966) Average extra cost for MS was pound1714 during the first 12 months
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacementCentral Message
In the United Kingdomrsquos National Health Service compared with a conventional median sternotomy approach for surgical aortic valve replacement mini-sternotomy did not hasten recovery or hospital discharge and was not cost-effective
Measuring What Matters
Having lived through the growth of percutaneous coronary intervention and now seeing the expansion of transcatheter aortic valve replacement I find myself asking the somewhat existential question ldquoAre we measuring what matters to patientsrdquo
Thoralf M Sundt MD Division of Cardiac Surgery
Massachusetts General Hospital Boston Massachusetts
Ann Thorac Surg 20181061602
Measuring What Matters
In a study performed at Dartmouth-Hitchcock
elderly patients prioritized ability to pursue activities maintaining independence and reducing symptoms
over
mortality benefit
Coleywright M et al Patients defined goals for the treatment of sever AVS a qualitative analysis
Health Expect 2016 191036-43
Measuring What Matters
These sorts of ldquosoftrdquo outcome variables are challenging to us We think of ourselvesmdashat least I domdashas medical scientists interested in ldquohardrdquo endpoints
But our patients are challenging us to consider what they value most not what we can measure easily Irsquod say it is time for us to broaden our horizons and revisit how we can better measure what matters
Ann Thorac Surg 20181061602

Minimally Invasive and Conventional Aortic Valve ReplacementA Propensity Score Analysis
Department of Adult Cardiac Surgery Daniyar Gilmanov G Pasquinucci Heart Hospital Massa Italy
Methods
bull This is a retrospective observational cohort study of prospectively collected data on 709 patients undergoing isolated primary aortic valve replacement between 2004 and 2011 Of these 338
were performed through either right anterior minithoracotomy or upper ministernotomy With propensity score matching 182 patients (minimally invasive group) were compared with 182
patients in conventional sternotomy (control group)
Conclusions
bull Our experience shows that mini-access isolated aortic valve surgery is a reproducible safe and effective procedure and reduces assisted ventilation duration the need for blood product
transfusion and incidence of post-surgery atrial fibrillation
(Ann Thorac Surg 201396837ndash43)
Introduction
bull The approaches taken under the umbrella of minimally-invasive surgical aortic valve replacement (MICS SAVR) essentially consist of a variety of access options to the aortic valve using smaller incisions
bull Importantly there is no convention or consensus as to what size incision qualifies as a minimally-invasive procedure
bull Furthermore lsquominimally-invasiversquo cardiac surgery (MICS) arguably is somewhat of a misnomer certainly in comparison interventions such as TAVR because the most invasive portions of the surgery including cross-clamping of the aorta ischemic cardiac arrest the use of cardiopulmonary bypass and opening of the aorta with introduction of air into the heart chambers all remain the same
Mahesh K Ramchandani MDAnnals of Thoracic Surgery ( in press)
ΜΙΝΙ
ν=28
ΥΠΟΛΟΙΠΟΙ
ν=131Ηλικία 722plusmn84 704plusmn98Γυναίκες(n) 10 (357) 58(442)Euro score 227plusmn2 18plusmn19ΜΕΘ μέρες 196plusmn06 198plusmn11Μέρες νοσηλείας 6plusmn218 57plusmn18Νοσηλεία lt5
μέρες
14(50) 37(517)
Μετάγγιση
RBC UNITS
12plusmn09 15plusmn13
CPB min 1124plusmn37 933plusmn33Μηχανικός
αερισμός (ώρες)
86plusmn45 104plusmn13
ΜΙΝΙ Στερνοτομές 2018Μεμονωμένη αντικατάσταση αορτικής βαλβίδας 2018
Σύνολο 159- ΜΙΝΙ 28 (176)
Χαρακτηριστικά ασθενών Επιπλοκές
ΜΙΝΙ
ν=28
ΥΠΟΛΟΙΠΟΙ
ν=131
P value
LCOS(n) 1 (36) 3(23) 069
Επαναδιάνοιξη(n) 0 4(31) 035
Λοιμώξεις
στερνοτομής(n)
1 (36) 3(23) 069
Stroke 0 2(15) 051
NIV 1 (36) 6(46) 081
Επαναδιασωλήνωση 0 3(23) 042
AKI(n) 3(107) 12(92) 079
Κολπική μαρμαρυγή 7(25) 40(305) 056
Θάνατος 0 3(23) 042
Minimally Invasive Approaches to Surgical Aortic Valve Replacement
A Meta-Analysis
Carolyn Chang BS Sajjad Raza MD Salah E Altarabsheh MD Sarah Delozier PhD Umesh M Sharma MD MBA Aisha Zia MD Muhammad Shahzeb Khan MD Mandy Neudecker MS Alan H Markowitz MD Joseph F Sabik III MD and Salil V Deo MD
Cleveland Ohio
(Ann Thorac Surg 20181061881ndash9)
Minimally Invasive Approaches to Surgical Aortic Valve ReplacementA Meta-Analysis
The outcomes of the 2 minimally invasive aortic valve replacement (AVR) strategiesmdashmini-sternotomy (AVR-st) and right anterior thoracotomy (AVR-th) with each other and with conventional AVR (cAVR)
Searched Medline PubMed Embase and Web of Science in December 2017 for studies comparing AVR-st AVR-th and cAVR Endpoints studied included hospital mortality stroke atrial fibrillation cardiopulmonary bypass (CPB) time and length of stay
A total of 19 studies (gt10000 pooled patients) met the inclusion criteria
bull Mortality (p [ 006) and stroke (p [ 015) were comparable between minimally invasive and conventional AVR
bull CPB times were longer with AVR-th versus cAVR (124 minutes [range 5 to 19] p lt 001) In the AVR-th cohort CPB duration was weakly inversely related to study size (p [ 006)
bull Atrial fibrillation was much less after AVR-th (odds ratio 047 [035 to 063] p lt 0001)
bull Hospital stay was significantly lower after minimally invasive surgery (08 [04 to 13] days p lt 001
Minimally invasive approaches to AVR yield excellent outcomes in high-volume centers They reduce hospital stay and incidence of postoperative atrial fibrillation and therefore should be considered in patients undergoing AVR The operative approach should be selected according to surgeonrsquos technical expertise and what is best for specific patient profile
(Ann Thorac Surg 20181061881ndash9)
Full Sternotomy Hemisternotomy and Minithoracotomyfor Aortic Valve Surgery Is There a Difference
Elisa Mikus MD Simone Calvi MD Gianluca Campo MD Rita Pavasini MD Marco Paris MD Eliana Raviola MD Marco Panzavolta MD Alberto Tripodi MD Roberto Ferrari MD PhD and Mauro Del Giglio MD PhD
Cardiothoracic and Vascular Department Maria Cecilia Hospital GVM Care amp Research Cotignola (RA) Cardiovascular Institute Azienda Ospedaliero-Universitaria di Ferrara Cona (FE) and Cardiovascular Department Istituto Clinico San Rocco Ome (BS) Italy
(Ann Thorac Surg 20181061782ndash8)
Full Sternotomy Hemisternotomy and Minithoracotomyfor Aortic Valve Surgery Is There a Difference
bull The study included all 1907 consecutive patients hospitalized at the Maria Cecilia Hospital (Cotignola RA Italy) between January 2010 and March 2017 undergoing isolated AVR through PUH RAT or MS The choice of the approach was left to surgeonrsquos preference To adjust for differences in baseline characteristics between the study groups a propensity score matching was performed Linear and logistic regression analyses were performed
bull Results Partial upper hemisternotomy was performed in 820 patients (43) right anterior minithoracotomy in 488 (26) and median sternotomy in 599 (31) After propensity score matching three groups of 377 patients were obtained Cardiopulmonary bypass and crossclamptimes were shorter in the right anterior minithoracotomy group than in the median sternotomy and partial upper hemisternotomy groups (p lt 0001) No significant differences in in-hospital mortality were observed (p [ 09) Renal failure (odds ratio 54 95 confidence interval 23 to 114 p lt 00001) extracardiac arteriopathy (odds ratio 29 95 confidence interval 11 to 67 p [ 0017) and left ventricular ejection fraction (odds ratio 096 95 confidence interval 093 to 099 p [ 0009) emerged as independent predictors of in hospital mortality
bull Conclusions Minimal-access isolated aortic valve surgery is a reproducible safe and effective procedure with similar outcomes and operating times compared with conventional sternotomy
Ann Thorac Surg 20181061782ndash8
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full median sternotomy for aortic valve replacement
Sukumaran K Nair FRCS(CTh) et al
bull From the a Department of Cardiothoracic Surgery PapworthHospital Cambridge United Kingdom Freeman Hospital Newcastle upon Tyne United Kingdom Leeds Institute of Clinical Trials Research University of Leeds Leeds United Kingdom Health Economics Research Group Brunel University London London United Kingdom and London School of Hygiene and Tropical Medicine Keppel Street London United Kingdom
J Thorac Cardiovasc Surg 20181562124-32
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacement
bull Methods This RCT compared MS with FS for first-time isolated AVR in 2 United Kingdom National Health Service hospitals Primary endpoints were duration of postoperative hospital stay and the time to fitness for discharge from hospital after AVR analyzed in the intent-to-treat population
bull Results In this RCT 222 patients were recruited and randomized (n frac14 118 in the MS group n frac14 104 in the FS group) Compared with the FS group the MS group had a longer hospital length of stay (mean 95 days vs 86 days) and took longer to achieve fitness for discharge home (mean 85 days vs 75 days) Adjusting for valve type sex and surgeon hazard ratios (HRs) from Cox models did not show a statistically significant effect of MS (relative to FS) on either hospital stay (HR 0874 95 confidence interval [CI] 0668-1143 P frac14 3246) or time to fitness for discharge (HR 0907 95 CI 0688-1197 P value frac14 4914) During a mean follow-up of 760 days (745 days for the MS group and 777 days for the FS group) 12 patients (10) in the MS group and 7 patients (7) in the FS group died (HR 1871 95 CI 0723-4844 P frac14 1966) Average extra cost for MS was pound1714 during the first 12 months
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacementCentral Message
In the United Kingdomrsquos National Health Service compared with a conventional median sternotomy approach for surgical aortic valve replacement mini-sternotomy did not hasten recovery or hospital discharge and was not cost-effective
Measuring What Matters
Having lived through the growth of percutaneous coronary intervention and now seeing the expansion of transcatheter aortic valve replacement I find myself asking the somewhat existential question ldquoAre we measuring what matters to patientsrdquo
Thoralf M Sundt MD Division of Cardiac Surgery
Massachusetts General Hospital Boston Massachusetts
Ann Thorac Surg 20181061602
Measuring What Matters
In a study performed at Dartmouth-Hitchcock
elderly patients prioritized ability to pursue activities maintaining independence and reducing symptoms
over
mortality benefit
Coleywright M et al Patients defined goals for the treatment of sever AVS a qualitative analysis
Health Expect 2016 191036-43
Measuring What Matters
These sorts of ldquosoftrdquo outcome variables are challenging to us We think of ourselvesmdashat least I domdashas medical scientists interested in ldquohardrdquo endpoints
But our patients are challenging us to consider what they value most not what we can measure easily Irsquod say it is time for us to broaden our horizons and revisit how we can better measure what matters
Ann Thorac Surg 20181061602

Introduction
bull The approaches taken under the umbrella of minimally-invasive surgical aortic valve replacement (MICS SAVR) essentially consist of a variety of access options to the aortic valve using smaller incisions
bull Importantly there is no convention or consensus as to what size incision qualifies as a minimally-invasive procedure
bull Furthermore lsquominimally-invasiversquo cardiac surgery (MICS) arguably is somewhat of a misnomer certainly in comparison interventions such as TAVR because the most invasive portions of the surgery including cross-clamping of the aorta ischemic cardiac arrest the use of cardiopulmonary bypass and opening of the aorta with introduction of air into the heart chambers all remain the same
Mahesh K Ramchandani MDAnnals of Thoracic Surgery ( in press)
ΜΙΝΙ
ν=28
ΥΠΟΛΟΙΠΟΙ
ν=131Ηλικία 722plusmn84 704plusmn98Γυναίκες(n) 10 (357) 58(442)Euro score 227plusmn2 18plusmn19ΜΕΘ μέρες 196plusmn06 198plusmn11Μέρες νοσηλείας 6plusmn218 57plusmn18Νοσηλεία lt5
μέρες
14(50) 37(517)
Μετάγγιση
RBC UNITS
12plusmn09 15plusmn13
CPB min 1124plusmn37 933plusmn33Μηχανικός
αερισμός (ώρες)
86plusmn45 104plusmn13
ΜΙΝΙ Στερνοτομές 2018Μεμονωμένη αντικατάσταση αορτικής βαλβίδας 2018
Σύνολο 159- ΜΙΝΙ 28 (176)
Χαρακτηριστικά ασθενών Επιπλοκές
ΜΙΝΙ
ν=28
ΥΠΟΛΟΙΠΟΙ
ν=131
P value
LCOS(n) 1 (36) 3(23) 069
Επαναδιάνοιξη(n) 0 4(31) 035
Λοιμώξεις
στερνοτομής(n)
1 (36) 3(23) 069
Stroke 0 2(15) 051
NIV 1 (36) 6(46) 081
Επαναδιασωλήνωση 0 3(23) 042
AKI(n) 3(107) 12(92) 079
Κολπική μαρμαρυγή 7(25) 40(305) 056
Θάνατος 0 3(23) 042
Minimally Invasive Approaches to Surgical Aortic Valve Replacement
A Meta-Analysis
Carolyn Chang BS Sajjad Raza MD Salah E Altarabsheh MD Sarah Delozier PhD Umesh M Sharma MD MBA Aisha Zia MD Muhammad Shahzeb Khan MD Mandy Neudecker MS Alan H Markowitz MD Joseph F Sabik III MD and Salil V Deo MD
Cleveland Ohio
(Ann Thorac Surg 20181061881ndash9)
Minimally Invasive Approaches to Surgical Aortic Valve ReplacementA Meta-Analysis
The outcomes of the 2 minimally invasive aortic valve replacement (AVR) strategiesmdashmini-sternotomy (AVR-st) and right anterior thoracotomy (AVR-th) with each other and with conventional AVR (cAVR)
Searched Medline PubMed Embase and Web of Science in December 2017 for studies comparing AVR-st AVR-th and cAVR Endpoints studied included hospital mortality stroke atrial fibrillation cardiopulmonary bypass (CPB) time and length of stay
A total of 19 studies (gt10000 pooled patients) met the inclusion criteria
bull Mortality (p [ 006) and stroke (p [ 015) were comparable between minimally invasive and conventional AVR
bull CPB times were longer with AVR-th versus cAVR (124 minutes [range 5 to 19] p lt 001) In the AVR-th cohort CPB duration was weakly inversely related to study size (p [ 006)
bull Atrial fibrillation was much less after AVR-th (odds ratio 047 [035 to 063] p lt 0001)
bull Hospital stay was significantly lower after minimally invasive surgery (08 [04 to 13] days p lt 001
Minimally invasive approaches to AVR yield excellent outcomes in high-volume centers They reduce hospital stay and incidence of postoperative atrial fibrillation and therefore should be considered in patients undergoing AVR The operative approach should be selected according to surgeonrsquos technical expertise and what is best for specific patient profile
(Ann Thorac Surg 20181061881ndash9)
Full Sternotomy Hemisternotomy and Minithoracotomyfor Aortic Valve Surgery Is There a Difference
Elisa Mikus MD Simone Calvi MD Gianluca Campo MD Rita Pavasini MD Marco Paris MD Eliana Raviola MD Marco Panzavolta MD Alberto Tripodi MD Roberto Ferrari MD PhD and Mauro Del Giglio MD PhD
Cardiothoracic and Vascular Department Maria Cecilia Hospital GVM Care amp Research Cotignola (RA) Cardiovascular Institute Azienda Ospedaliero-Universitaria di Ferrara Cona (FE) and Cardiovascular Department Istituto Clinico San Rocco Ome (BS) Italy
(Ann Thorac Surg 20181061782ndash8)
Full Sternotomy Hemisternotomy and Minithoracotomyfor Aortic Valve Surgery Is There a Difference
bull The study included all 1907 consecutive patients hospitalized at the Maria Cecilia Hospital (Cotignola RA Italy) between January 2010 and March 2017 undergoing isolated AVR through PUH RAT or MS The choice of the approach was left to surgeonrsquos preference To adjust for differences in baseline characteristics between the study groups a propensity score matching was performed Linear and logistic regression analyses were performed
bull Results Partial upper hemisternotomy was performed in 820 patients (43) right anterior minithoracotomy in 488 (26) and median sternotomy in 599 (31) After propensity score matching three groups of 377 patients were obtained Cardiopulmonary bypass and crossclamptimes were shorter in the right anterior minithoracotomy group than in the median sternotomy and partial upper hemisternotomy groups (p lt 0001) No significant differences in in-hospital mortality were observed (p [ 09) Renal failure (odds ratio 54 95 confidence interval 23 to 114 p lt 00001) extracardiac arteriopathy (odds ratio 29 95 confidence interval 11 to 67 p [ 0017) and left ventricular ejection fraction (odds ratio 096 95 confidence interval 093 to 099 p [ 0009) emerged as independent predictors of in hospital mortality
bull Conclusions Minimal-access isolated aortic valve surgery is a reproducible safe and effective procedure with similar outcomes and operating times compared with conventional sternotomy
Ann Thorac Surg 20181061782ndash8
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full median sternotomy for aortic valve replacement
Sukumaran K Nair FRCS(CTh) et al
bull From the a Department of Cardiothoracic Surgery PapworthHospital Cambridge United Kingdom Freeman Hospital Newcastle upon Tyne United Kingdom Leeds Institute of Clinical Trials Research University of Leeds Leeds United Kingdom Health Economics Research Group Brunel University London London United Kingdom and London School of Hygiene and Tropical Medicine Keppel Street London United Kingdom
J Thorac Cardiovasc Surg 20181562124-32
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacement
bull Methods This RCT compared MS with FS for first-time isolated AVR in 2 United Kingdom National Health Service hospitals Primary endpoints were duration of postoperative hospital stay and the time to fitness for discharge from hospital after AVR analyzed in the intent-to-treat population
bull Results In this RCT 222 patients were recruited and randomized (n frac14 118 in the MS group n frac14 104 in the FS group) Compared with the FS group the MS group had a longer hospital length of stay (mean 95 days vs 86 days) and took longer to achieve fitness for discharge home (mean 85 days vs 75 days) Adjusting for valve type sex and surgeon hazard ratios (HRs) from Cox models did not show a statistically significant effect of MS (relative to FS) on either hospital stay (HR 0874 95 confidence interval [CI] 0668-1143 P frac14 3246) or time to fitness for discharge (HR 0907 95 CI 0688-1197 P value frac14 4914) During a mean follow-up of 760 days (745 days for the MS group and 777 days for the FS group) 12 patients (10) in the MS group and 7 patients (7) in the FS group died (HR 1871 95 CI 0723-4844 P frac14 1966) Average extra cost for MS was pound1714 during the first 12 months
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacementCentral Message
In the United Kingdomrsquos National Health Service compared with a conventional median sternotomy approach for surgical aortic valve replacement mini-sternotomy did not hasten recovery or hospital discharge and was not cost-effective
Measuring What Matters
Having lived through the growth of percutaneous coronary intervention and now seeing the expansion of transcatheter aortic valve replacement I find myself asking the somewhat existential question ldquoAre we measuring what matters to patientsrdquo
Thoralf M Sundt MD Division of Cardiac Surgery
Massachusetts General Hospital Boston Massachusetts
Ann Thorac Surg 20181061602
Measuring What Matters
In a study performed at Dartmouth-Hitchcock
elderly patients prioritized ability to pursue activities maintaining independence and reducing symptoms
over
mortality benefit
Coleywright M et al Patients defined goals for the treatment of sever AVS a qualitative analysis
Health Expect 2016 191036-43
Measuring What Matters
These sorts of ldquosoftrdquo outcome variables are challenging to us We think of ourselvesmdashat least I domdashas medical scientists interested in ldquohardrdquo endpoints
But our patients are challenging us to consider what they value most not what we can measure easily Irsquod say it is time for us to broaden our horizons and revisit how we can better measure what matters
Ann Thorac Surg 20181061602

ΜΙΝΙ
ν=28
ΥΠΟΛΟΙΠΟΙ
ν=131Ηλικία 722plusmn84 704plusmn98Γυναίκες(n) 10 (357) 58(442)Euro score 227plusmn2 18plusmn19ΜΕΘ μέρες 196plusmn06 198plusmn11Μέρες νοσηλείας 6plusmn218 57plusmn18Νοσηλεία lt5
μέρες
14(50) 37(517)
Μετάγγιση
RBC UNITS
12plusmn09 15plusmn13
CPB min 1124plusmn37 933plusmn33Μηχανικός
αερισμός (ώρες)
86plusmn45 104plusmn13
ΜΙΝΙ Στερνοτομές 2018Μεμονωμένη αντικατάσταση αορτικής βαλβίδας 2018
Σύνολο 159- ΜΙΝΙ 28 (176)
Χαρακτηριστικά ασθενών Επιπλοκές
ΜΙΝΙ
ν=28
ΥΠΟΛΟΙΠΟΙ
ν=131
P value
LCOS(n) 1 (36) 3(23) 069
Επαναδιάνοιξη(n) 0 4(31) 035
Λοιμώξεις
στερνοτομής(n)
1 (36) 3(23) 069
Stroke 0 2(15) 051
NIV 1 (36) 6(46) 081
Επαναδιασωλήνωση 0 3(23) 042
AKI(n) 3(107) 12(92) 079
Κολπική μαρμαρυγή 7(25) 40(305) 056
Θάνατος 0 3(23) 042
Minimally Invasive Approaches to Surgical Aortic Valve Replacement
A Meta-Analysis
Carolyn Chang BS Sajjad Raza MD Salah E Altarabsheh MD Sarah Delozier PhD Umesh M Sharma MD MBA Aisha Zia MD Muhammad Shahzeb Khan MD Mandy Neudecker MS Alan H Markowitz MD Joseph F Sabik III MD and Salil V Deo MD
Cleveland Ohio
(Ann Thorac Surg 20181061881ndash9)
Minimally Invasive Approaches to Surgical Aortic Valve ReplacementA Meta-Analysis
The outcomes of the 2 minimally invasive aortic valve replacement (AVR) strategiesmdashmini-sternotomy (AVR-st) and right anterior thoracotomy (AVR-th) with each other and with conventional AVR (cAVR)
Searched Medline PubMed Embase and Web of Science in December 2017 for studies comparing AVR-st AVR-th and cAVR Endpoints studied included hospital mortality stroke atrial fibrillation cardiopulmonary bypass (CPB) time and length of stay
A total of 19 studies (gt10000 pooled patients) met the inclusion criteria
bull Mortality (p [ 006) and stroke (p [ 015) were comparable between minimally invasive and conventional AVR
bull CPB times were longer with AVR-th versus cAVR (124 minutes [range 5 to 19] p lt 001) In the AVR-th cohort CPB duration was weakly inversely related to study size (p [ 006)
bull Atrial fibrillation was much less after AVR-th (odds ratio 047 [035 to 063] p lt 0001)
bull Hospital stay was significantly lower after minimally invasive surgery (08 [04 to 13] days p lt 001
Minimally invasive approaches to AVR yield excellent outcomes in high-volume centers They reduce hospital stay and incidence of postoperative atrial fibrillation and therefore should be considered in patients undergoing AVR The operative approach should be selected according to surgeonrsquos technical expertise and what is best for specific patient profile
(Ann Thorac Surg 20181061881ndash9)
Full Sternotomy Hemisternotomy and Minithoracotomyfor Aortic Valve Surgery Is There a Difference
Elisa Mikus MD Simone Calvi MD Gianluca Campo MD Rita Pavasini MD Marco Paris MD Eliana Raviola MD Marco Panzavolta MD Alberto Tripodi MD Roberto Ferrari MD PhD and Mauro Del Giglio MD PhD
Cardiothoracic and Vascular Department Maria Cecilia Hospital GVM Care amp Research Cotignola (RA) Cardiovascular Institute Azienda Ospedaliero-Universitaria di Ferrara Cona (FE) and Cardiovascular Department Istituto Clinico San Rocco Ome (BS) Italy
(Ann Thorac Surg 20181061782ndash8)
Full Sternotomy Hemisternotomy and Minithoracotomyfor Aortic Valve Surgery Is There a Difference
bull The study included all 1907 consecutive patients hospitalized at the Maria Cecilia Hospital (Cotignola RA Italy) between January 2010 and March 2017 undergoing isolated AVR through PUH RAT or MS The choice of the approach was left to surgeonrsquos preference To adjust for differences in baseline characteristics between the study groups a propensity score matching was performed Linear and logistic regression analyses were performed
bull Results Partial upper hemisternotomy was performed in 820 patients (43) right anterior minithoracotomy in 488 (26) and median sternotomy in 599 (31) After propensity score matching three groups of 377 patients were obtained Cardiopulmonary bypass and crossclamptimes were shorter in the right anterior minithoracotomy group than in the median sternotomy and partial upper hemisternotomy groups (p lt 0001) No significant differences in in-hospital mortality were observed (p [ 09) Renal failure (odds ratio 54 95 confidence interval 23 to 114 p lt 00001) extracardiac arteriopathy (odds ratio 29 95 confidence interval 11 to 67 p [ 0017) and left ventricular ejection fraction (odds ratio 096 95 confidence interval 093 to 099 p [ 0009) emerged as independent predictors of in hospital mortality
bull Conclusions Minimal-access isolated aortic valve surgery is a reproducible safe and effective procedure with similar outcomes and operating times compared with conventional sternotomy
Ann Thorac Surg 20181061782ndash8
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full median sternotomy for aortic valve replacement
Sukumaran K Nair FRCS(CTh) et al
bull From the a Department of Cardiothoracic Surgery PapworthHospital Cambridge United Kingdom Freeman Hospital Newcastle upon Tyne United Kingdom Leeds Institute of Clinical Trials Research University of Leeds Leeds United Kingdom Health Economics Research Group Brunel University London London United Kingdom and London School of Hygiene and Tropical Medicine Keppel Street London United Kingdom
J Thorac Cardiovasc Surg 20181562124-32
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacement
bull Methods This RCT compared MS with FS for first-time isolated AVR in 2 United Kingdom National Health Service hospitals Primary endpoints were duration of postoperative hospital stay and the time to fitness for discharge from hospital after AVR analyzed in the intent-to-treat population
bull Results In this RCT 222 patients were recruited and randomized (n frac14 118 in the MS group n frac14 104 in the FS group) Compared with the FS group the MS group had a longer hospital length of stay (mean 95 days vs 86 days) and took longer to achieve fitness for discharge home (mean 85 days vs 75 days) Adjusting for valve type sex and surgeon hazard ratios (HRs) from Cox models did not show a statistically significant effect of MS (relative to FS) on either hospital stay (HR 0874 95 confidence interval [CI] 0668-1143 P frac14 3246) or time to fitness for discharge (HR 0907 95 CI 0688-1197 P value frac14 4914) During a mean follow-up of 760 days (745 days for the MS group and 777 days for the FS group) 12 patients (10) in the MS group and 7 patients (7) in the FS group died (HR 1871 95 CI 0723-4844 P frac14 1966) Average extra cost for MS was pound1714 during the first 12 months
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacementCentral Message
In the United Kingdomrsquos National Health Service compared with a conventional median sternotomy approach for surgical aortic valve replacement mini-sternotomy did not hasten recovery or hospital discharge and was not cost-effective
Measuring What Matters
Having lived through the growth of percutaneous coronary intervention and now seeing the expansion of transcatheter aortic valve replacement I find myself asking the somewhat existential question ldquoAre we measuring what matters to patientsrdquo
Thoralf M Sundt MD Division of Cardiac Surgery
Massachusetts General Hospital Boston Massachusetts
Ann Thorac Surg 20181061602
Measuring What Matters
In a study performed at Dartmouth-Hitchcock
elderly patients prioritized ability to pursue activities maintaining independence and reducing symptoms
over
mortality benefit
Coleywright M et al Patients defined goals for the treatment of sever AVS a qualitative analysis
Health Expect 2016 191036-43
Measuring What Matters
These sorts of ldquosoftrdquo outcome variables are challenging to us We think of ourselvesmdashat least I domdashas medical scientists interested in ldquohardrdquo endpoints
But our patients are challenging us to consider what they value most not what we can measure easily Irsquod say it is time for us to broaden our horizons and revisit how we can better measure what matters
Ann Thorac Surg 20181061602

Minimally Invasive Approaches to Surgical Aortic Valve Replacement
A Meta-Analysis
Carolyn Chang BS Sajjad Raza MD Salah E Altarabsheh MD Sarah Delozier PhD Umesh M Sharma MD MBA Aisha Zia MD Muhammad Shahzeb Khan MD Mandy Neudecker MS Alan H Markowitz MD Joseph F Sabik III MD and Salil V Deo MD
Cleveland Ohio
(Ann Thorac Surg 20181061881ndash9)
Minimally Invasive Approaches to Surgical Aortic Valve ReplacementA Meta-Analysis
The outcomes of the 2 minimally invasive aortic valve replacement (AVR) strategiesmdashmini-sternotomy (AVR-st) and right anterior thoracotomy (AVR-th) with each other and with conventional AVR (cAVR)
Searched Medline PubMed Embase and Web of Science in December 2017 for studies comparing AVR-st AVR-th and cAVR Endpoints studied included hospital mortality stroke atrial fibrillation cardiopulmonary bypass (CPB) time and length of stay
A total of 19 studies (gt10000 pooled patients) met the inclusion criteria
bull Mortality (p [ 006) and stroke (p [ 015) were comparable between minimally invasive and conventional AVR
bull CPB times were longer with AVR-th versus cAVR (124 minutes [range 5 to 19] p lt 001) In the AVR-th cohort CPB duration was weakly inversely related to study size (p [ 006)
bull Atrial fibrillation was much less after AVR-th (odds ratio 047 [035 to 063] p lt 0001)
bull Hospital stay was significantly lower after minimally invasive surgery (08 [04 to 13] days p lt 001
Minimally invasive approaches to AVR yield excellent outcomes in high-volume centers They reduce hospital stay and incidence of postoperative atrial fibrillation and therefore should be considered in patients undergoing AVR The operative approach should be selected according to surgeonrsquos technical expertise and what is best for specific patient profile
(Ann Thorac Surg 20181061881ndash9)
Full Sternotomy Hemisternotomy and Minithoracotomyfor Aortic Valve Surgery Is There a Difference
Elisa Mikus MD Simone Calvi MD Gianluca Campo MD Rita Pavasini MD Marco Paris MD Eliana Raviola MD Marco Panzavolta MD Alberto Tripodi MD Roberto Ferrari MD PhD and Mauro Del Giglio MD PhD
Cardiothoracic and Vascular Department Maria Cecilia Hospital GVM Care amp Research Cotignola (RA) Cardiovascular Institute Azienda Ospedaliero-Universitaria di Ferrara Cona (FE) and Cardiovascular Department Istituto Clinico San Rocco Ome (BS) Italy
(Ann Thorac Surg 20181061782ndash8)
Full Sternotomy Hemisternotomy and Minithoracotomyfor Aortic Valve Surgery Is There a Difference
bull The study included all 1907 consecutive patients hospitalized at the Maria Cecilia Hospital (Cotignola RA Italy) between January 2010 and March 2017 undergoing isolated AVR through PUH RAT or MS The choice of the approach was left to surgeonrsquos preference To adjust for differences in baseline characteristics between the study groups a propensity score matching was performed Linear and logistic regression analyses were performed
bull Results Partial upper hemisternotomy was performed in 820 patients (43) right anterior minithoracotomy in 488 (26) and median sternotomy in 599 (31) After propensity score matching three groups of 377 patients were obtained Cardiopulmonary bypass and crossclamptimes were shorter in the right anterior minithoracotomy group than in the median sternotomy and partial upper hemisternotomy groups (p lt 0001) No significant differences in in-hospital mortality were observed (p [ 09) Renal failure (odds ratio 54 95 confidence interval 23 to 114 p lt 00001) extracardiac arteriopathy (odds ratio 29 95 confidence interval 11 to 67 p [ 0017) and left ventricular ejection fraction (odds ratio 096 95 confidence interval 093 to 099 p [ 0009) emerged as independent predictors of in hospital mortality
bull Conclusions Minimal-access isolated aortic valve surgery is a reproducible safe and effective procedure with similar outcomes and operating times compared with conventional sternotomy
Ann Thorac Surg 20181061782ndash8
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full median sternotomy for aortic valve replacement
Sukumaran K Nair FRCS(CTh) et al
bull From the a Department of Cardiothoracic Surgery PapworthHospital Cambridge United Kingdom Freeman Hospital Newcastle upon Tyne United Kingdom Leeds Institute of Clinical Trials Research University of Leeds Leeds United Kingdom Health Economics Research Group Brunel University London London United Kingdom and London School of Hygiene and Tropical Medicine Keppel Street London United Kingdom
J Thorac Cardiovasc Surg 20181562124-32
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacement
bull Methods This RCT compared MS with FS for first-time isolated AVR in 2 United Kingdom National Health Service hospitals Primary endpoints were duration of postoperative hospital stay and the time to fitness for discharge from hospital after AVR analyzed in the intent-to-treat population
bull Results In this RCT 222 patients were recruited and randomized (n frac14 118 in the MS group n frac14 104 in the FS group) Compared with the FS group the MS group had a longer hospital length of stay (mean 95 days vs 86 days) and took longer to achieve fitness for discharge home (mean 85 days vs 75 days) Adjusting for valve type sex and surgeon hazard ratios (HRs) from Cox models did not show a statistically significant effect of MS (relative to FS) on either hospital stay (HR 0874 95 confidence interval [CI] 0668-1143 P frac14 3246) or time to fitness for discharge (HR 0907 95 CI 0688-1197 P value frac14 4914) During a mean follow-up of 760 days (745 days for the MS group and 777 days for the FS group) 12 patients (10) in the MS group and 7 patients (7) in the FS group died (HR 1871 95 CI 0723-4844 P frac14 1966) Average extra cost for MS was pound1714 during the first 12 months
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacementCentral Message
In the United Kingdomrsquos National Health Service compared with a conventional median sternotomy approach for surgical aortic valve replacement mini-sternotomy did not hasten recovery or hospital discharge and was not cost-effective
Measuring What Matters
Having lived through the growth of percutaneous coronary intervention and now seeing the expansion of transcatheter aortic valve replacement I find myself asking the somewhat existential question ldquoAre we measuring what matters to patientsrdquo
Thoralf M Sundt MD Division of Cardiac Surgery
Massachusetts General Hospital Boston Massachusetts
Ann Thorac Surg 20181061602
Measuring What Matters
In a study performed at Dartmouth-Hitchcock
elderly patients prioritized ability to pursue activities maintaining independence and reducing symptoms
over
mortality benefit
Coleywright M et al Patients defined goals for the treatment of sever AVS a qualitative analysis
Health Expect 2016 191036-43
Measuring What Matters
These sorts of ldquosoftrdquo outcome variables are challenging to us We think of ourselvesmdashat least I domdashas medical scientists interested in ldquohardrdquo endpoints
But our patients are challenging us to consider what they value most not what we can measure easily Irsquod say it is time for us to broaden our horizons and revisit how we can better measure what matters
Ann Thorac Surg 20181061602

Minimally Invasive Approaches to Surgical Aortic Valve ReplacementA Meta-Analysis
The outcomes of the 2 minimally invasive aortic valve replacement (AVR) strategiesmdashmini-sternotomy (AVR-st) and right anterior thoracotomy (AVR-th) with each other and with conventional AVR (cAVR)
Searched Medline PubMed Embase and Web of Science in December 2017 for studies comparing AVR-st AVR-th and cAVR Endpoints studied included hospital mortality stroke atrial fibrillation cardiopulmonary bypass (CPB) time and length of stay
A total of 19 studies (gt10000 pooled patients) met the inclusion criteria
bull Mortality (p [ 006) and stroke (p [ 015) were comparable between minimally invasive and conventional AVR
bull CPB times were longer with AVR-th versus cAVR (124 minutes [range 5 to 19] p lt 001) In the AVR-th cohort CPB duration was weakly inversely related to study size (p [ 006)
bull Atrial fibrillation was much less after AVR-th (odds ratio 047 [035 to 063] p lt 0001)
bull Hospital stay was significantly lower after minimally invasive surgery (08 [04 to 13] days p lt 001
Minimally invasive approaches to AVR yield excellent outcomes in high-volume centers They reduce hospital stay and incidence of postoperative atrial fibrillation and therefore should be considered in patients undergoing AVR The operative approach should be selected according to surgeonrsquos technical expertise and what is best for specific patient profile
(Ann Thorac Surg 20181061881ndash9)
Full Sternotomy Hemisternotomy and Minithoracotomyfor Aortic Valve Surgery Is There a Difference
Elisa Mikus MD Simone Calvi MD Gianluca Campo MD Rita Pavasini MD Marco Paris MD Eliana Raviola MD Marco Panzavolta MD Alberto Tripodi MD Roberto Ferrari MD PhD and Mauro Del Giglio MD PhD
Cardiothoracic and Vascular Department Maria Cecilia Hospital GVM Care amp Research Cotignola (RA) Cardiovascular Institute Azienda Ospedaliero-Universitaria di Ferrara Cona (FE) and Cardiovascular Department Istituto Clinico San Rocco Ome (BS) Italy
(Ann Thorac Surg 20181061782ndash8)
Full Sternotomy Hemisternotomy and Minithoracotomyfor Aortic Valve Surgery Is There a Difference
bull The study included all 1907 consecutive patients hospitalized at the Maria Cecilia Hospital (Cotignola RA Italy) between January 2010 and March 2017 undergoing isolated AVR through PUH RAT or MS The choice of the approach was left to surgeonrsquos preference To adjust for differences in baseline characteristics between the study groups a propensity score matching was performed Linear and logistic regression analyses were performed
bull Results Partial upper hemisternotomy was performed in 820 patients (43) right anterior minithoracotomy in 488 (26) and median sternotomy in 599 (31) After propensity score matching three groups of 377 patients were obtained Cardiopulmonary bypass and crossclamptimes were shorter in the right anterior minithoracotomy group than in the median sternotomy and partial upper hemisternotomy groups (p lt 0001) No significant differences in in-hospital mortality were observed (p [ 09) Renal failure (odds ratio 54 95 confidence interval 23 to 114 p lt 00001) extracardiac arteriopathy (odds ratio 29 95 confidence interval 11 to 67 p [ 0017) and left ventricular ejection fraction (odds ratio 096 95 confidence interval 093 to 099 p [ 0009) emerged as independent predictors of in hospital mortality
bull Conclusions Minimal-access isolated aortic valve surgery is a reproducible safe and effective procedure with similar outcomes and operating times compared with conventional sternotomy
Ann Thorac Surg 20181061782ndash8
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full median sternotomy for aortic valve replacement
Sukumaran K Nair FRCS(CTh) et al
bull From the a Department of Cardiothoracic Surgery PapworthHospital Cambridge United Kingdom Freeman Hospital Newcastle upon Tyne United Kingdom Leeds Institute of Clinical Trials Research University of Leeds Leeds United Kingdom Health Economics Research Group Brunel University London London United Kingdom and London School of Hygiene and Tropical Medicine Keppel Street London United Kingdom
J Thorac Cardiovasc Surg 20181562124-32
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacement
bull Methods This RCT compared MS with FS for first-time isolated AVR in 2 United Kingdom National Health Service hospitals Primary endpoints were duration of postoperative hospital stay and the time to fitness for discharge from hospital after AVR analyzed in the intent-to-treat population
bull Results In this RCT 222 patients were recruited and randomized (n frac14 118 in the MS group n frac14 104 in the FS group) Compared with the FS group the MS group had a longer hospital length of stay (mean 95 days vs 86 days) and took longer to achieve fitness for discharge home (mean 85 days vs 75 days) Adjusting for valve type sex and surgeon hazard ratios (HRs) from Cox models did not show a statistically significant effect of MS (relative to FS) on either hospital stay (HR 0874 95 confidence interval [CI] 0668-1143 P frac14 3246) or time to fitness for discharge (HR 0907 95 CI 0688-1197 P value frac14 4914) During a mean follow-up of 760 days (745 days for the MS group and 777 days for the FS group) 12 patients (10) in the MS group and 7 patients (7) in the FS group died (HR 1871 95 CI 0723-4844 P frac14 1966) Average extra cost for MS was pound1714 during the first 12 months
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacementCentral Message
In the United Kingdomrsquos National Health Service compared with a conventional median sternotomy approach for surgical aortic valve replacement mini-sternotomy did not hasten recovery or hospital discharge and was not cost-effective
Measuring What Matters
Having lived through the growth of percutaneous coronary intervention and now seeing the expansion of transcatheter aortic valve replacement I find myself asking the somewhat existential question ldquoAre we measuring what matters to patientsrdquo
Thoralf M Sundt MD Division of Cardiac Surgery
Massachusetts General Hospital Boston Massachusetts
Ann Thorac Surg 20181061602
Measuring What Matters
In a study performed at Dartmouth-Hitchcock
elderly patients prioritized ability to pursue activities maintaining independence and reducing symptoms
over
mortality benefit
Coleywright M et al Patients defined goals for the treatment of sever AVS a qualitative analysis
Health Expect 2016 191036-43
Measuring What Matters
These sorts of ldquosoftrdquo outcome variables are challenging to us We think of ourselvesmdashat least I domdashas medical scientists interested in ldquohardrdquo endpoints
But our patients are challenging us to consider what they value most not what we can measure easily Irsquod say it is time for us to broaden our horizons and revisit how we can better measure what matters
Ann Thorac Surg 20181061602

Full Sternotomy Hemisternotomy and Minithoracotomyfor Aortic Valve Surgery Is There a Difference
Elisa Mikus MD Simone Calvi MD Gianluca Campo MD Rita Pavasini MD Marco Paris MD Eliana Raviola MD Marco Panzavolta MD Alberto Tripodi MD Roberto Ferrari MD PhD and Mauro Del Giglio MD PhD
Cardiothoracic and Vascular Department Maria Cecilia Hospital GVM Care amp Research Cotignola (RA) Cardiovascular Institute Azienda Ospedaliero-Universitaria di Ferrara Cona (FE) and Cardiovascular Department Istituto Clinico San Rocco Ome (BS) Italy
(Ann Thorac Surg 20181061782ndash8)
Full Sternotomy Hemisternotomy and Minithoracotomyfor Aortic Valve Surgery Is There a Difference
bull The study included all 1907 consecutive patients hospitalized at the Maria Cecilia Hospital (Cotignola RA Italy) between January 2010 and March 2017 undergoing isolated AVR through PUH RAT or MS The choice of the approach was left to surgeonrsquos preference To adjust for differences in baseline characteristics between the study groups a propensity score matching was performed Linear and logistic regression analyses were performed
bull Results Partial upper hemisternotomy was performed in 820 patients (43) right anterior minithoracotomy in 488 (26) and median sternotomy in 599 (31) After propensity score matching three groups of 377 patients were obtained Cardiopulmonary bypass and crossclamptimes were shorter in the right anterior minithoracotomy group than in the median sternotomy and partial upper hemisternotomy groups (p lt 0001) No significant differences in in-hospital mortality were observed (p [ 09) Renal failure (odds ratio 54 95 confidence interval 23 to 114 p lt 00001) extracardiac arteriopathy (odds ratio 29 95 confidence interval 11 to 67 p [ 0017) and left ventricular ejection fraction (odds ratio 096 95 confidence interval 093 to 099 p [ 0009) emerged as independent predictors of in hospital mortality
bull Conclusions Minimal-access isolated aortic valve surgery is a reproducible safe and effective procedure with similar outcomes and operating times compared with conventional sternotomy
Ann Thorac Surg 20181061782ndash8
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full median sternotomy for aortic valve replacement
Sukumaran K Nair FRCS(CTh) et al
bull From the a Department of Cardiothoracic Surgery PapworthHospital Cambridge United Kingdom Freeman Hospital Newcastle upon Tyne United Kingdom Leeds Institute of Clinical Trials Research University of Leeds Leeds United Kingdom Health Economics Research Group Brunel University London London United Kingdom and London School of Hygiene and Tropical Medicine Keppel Street London United Kingdom
J Thorac Cardiovasc Surg 20181562124-32
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacement
bull Methods This RCT compared MS with FS for first-time isolated AVR in 2 United Kingdom National Health Service hospitals Primary endpoints were duration of postoperative hospital stay and the time to fitness for discharge from hospital after AVR analyzed in the intent-to-treat population
bull Results In this RCT 222 patients were recruited and randomized (n frac14 118 in the MS group n frac14 104 in the FS group) Compared with the FS group the MS group had a longer hospital length of stay (mean 95 days vs 86 days) and took longer to achieve fitness for discharge home (mean 85 days vs 75 days) Adjusting for valve type sex and surgeon hazard ratios (HRs) from Cox models did not show a statistically significant effect of MS (relative to FS) on either hospital stay (HR 0874 95 confidence interval [CI] 0668-1143 P frac14 3246) or time to fitness for discharge (HR 0907 95 CI 0688-1197 P value frac14 4914) During a mean follow-up of 760 days (745 days for the MS group and 777 days for the FS group) 12 patients (10) in the MS group and 7 patients (7) in the FS group died (HR 1871 95 CI 0723-4844 P frac14 1966) Average extra cost for MS was pound1714 during the first 12 months
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacementCentral Message
In the United Kingdomrsquos National Health Service compared with a conventional median sternotomy approach for surgical aortic valve replacement mini-sternotomy did not hasten recovery or hospital discharge and was not cost-effective
Measuring What Matters
Having lived through the growth of percutaneous coronary intervention and now seeing the expansion of transcatheter aortic valve replacement I find myself asking the somewhat existential question ldquoAre we measuring what matters to patientsrdquo
Thoralf M Sundt MD Division of Cardiac Surgery
Massachusetts General Hospital Boston Massachusetts
Ann Thorac Surg 20181061602
Measuring What Matters
In a study performed at Dartmouth-Hitchcock
elderly patients prioritized ability to pursue activities maintaining independence and reducing symptoms
over
mortality benefit
Coleywright M et al Patients defined goals for the treatment of sever AVS a qualitative analysis
Health Expect 2016 191036-43
Measuring What Matters
These sorts of ldquosoftrdquo outcome variables are challenging to us We think of ourselvesmdashat least I domdashas medical scientists interested in ldquohardrdquo endpoints
But our patients are challenging us to consider what they value most not what we can measure easily Irsquod say it is time for us to broaden our horizons and revisit how we can better measure what matters
Ann Thorac Surg 20181061602

Full Sternotomy Hemisternotomy and Minithoracotomyfor Aortic Valve Surgery Is There a Difference
bull The study included all 1907 consecutive patients hospitalized at the Maria Cecilia Hospital (Cotignola RA Italy) between January 2010 and March 2017 undergoing isolated AVR through PUH RAT or MS The choice of the approach was left to surgeonrsquos preference To adjust for differences in baseline characteristics between the study groups a propensity score matching was performed Linear and logistic regression analyses were performed
bull Results Partial upper hemisternotomy was performed in 820 patients (43) right anterior minithoracotomy in 488 (26) and median sternotomy in 599 (31) After propensity score matching three groups of 377 patients were obtained Cardiopulmonary bypass and crossclamptimes were shorter in the right anterior minithoracotomy group than in the median sternotomy and partial upper hemisternotomy groups (p lt 0001) No significant differences in in-hospital mortality were observed (p [ 09) Renal failure (odds ratio 54 95 confidence interval 23 to 114 p lt 00001) extracardiac arteriopathy (odds ratio 29 95 confidence interval 11 to 67 p [ 0017) and left ventricular ejection fraction (odds ratio 096 95 confidence interval 093 to 099 p [ 0009) emerged as independent predictors of in hospital mortality
bull Conclusions Minimal-access isolated aortic valve surgery is a reproducible safe and effective procedure with similar outcomes and operating times compared with conventional sternotomy
Ann Thorac Surg 20181061782ndash8
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full median sternotomy for aortic valve replacement
Sukumaran K Nair FRCS(CTh) et al
bull From the a Department of Cardiothoracic Surgery PapworthHospital Cambridge United Kingdom Freeman Hospital Newcastle upon Tyne United Kingdom Leeds Institute of Clinical Trials Research University of Leeds Leeds United Kingdom Health Economics Research Group Brunel University London London United Kingdom and London School of Hygiene and Tropical Medicine Keppel Street London United Kingdom
J Thorac Cardiovasc Surg 20181562124-32
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacement
bull Methods This RCT compared MS with FS for first-time isolated AVR in 2 United Kingdom National Health Service hospitals Primary endpoints were duration of postoperative hospital stay and the time to fitness for discharge from hospital after AVR analyzed in the intent-to-treat population
bull Results In this RCT 222 patients were recruited and randomized (n frac14 118 in the MS group n frac14 104 in the FS group) Compared with the FS group the MS group had a longer hospital length of stay (mean 95 days vs 86 days) and took longer to achieve fitness for discharge home (mean 85 days vs 75 days) Adjusting for valve type sex and surgeon hazard ratios (HRs) from Cox models did not show a statistically significant effect of MS (relative to FS) on either hospital stay (HR 0874 95 confidence interval [CI] 0668-1143 P frac14 3246) or time to fitness for discharge (HR 0907 95 CI 0688-1197 P value frac14 4914) During a mean follow-up of 760 days (745 days for the MS group and 777 days for the FS group) 12 patients (10) in the MS group and 7 patients (7) in the FS group died (HR 1871 95 CI 0723-4844 P frac14 1966) Average extra cost for MS was pound1714 during the first 12 months
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacementCentral Message
In the United Kingdomrsquos National Health Service compared with a conventional median sternotomy approach for surgical aortic valve replacement mini-sternotomy did not hasten recovery or hospital discharge and was not cost-effective
Measuring What Matters
Having lived through the growth of percutaneous coronary intervention and now seeing the expansion of transcatheter aortic valve replacement I find myself asking the somewhat existential question ldquoAre we measuring what matters to patientsrdquo
Thoralf M Sundt MD Division of Cardiac Surgery
Massachusetts General Hospital Boston Massachusetts
Ann Thorac Surg 20181061602
Measuring What Matters
In a study performed at Dartmouth-Hitchcock
elderly patients prioritized ability to pursue activities maintaining independence and reducing symptoms
over
mortality benefit
Coleywright M et al Patients defined goals for the treatment of sever AVS a qualitative analysis
Health Expect 2016 191036-43
Measuring What Matters
These sorts of ldquosoftrdquo outcome variables are challenging to us We think of ourselvesmdashat least I domdashas medical scientists interested in ldquohardrdquo endpoints
But our patients are challenging us to consider what they value most not what we can measure easily Irsquod say it is time for us to broaden our horizons and revisit how we can better measure what matters
Ann Thorac Surg 20181061602

Mini-Stern TrialA randomized trial comparing mini-sternotomy to full median sternotomy for aortic valve replacement
Sukumaran K Nair FRCS(CTh) et al
bull From the a Department of Cardiothoracic Surgery PapworthHospital Cambridge United Kingdom Freeman Hospital Newcastle upon Tyne United Kingdom Leeds Institute of Clinical Trials Research University of Leeds Leeds United Kingdom Health Economics Research Group Brunel University London London United Kingdom and London School of Hygiene and Tropical Medicine Keppel Street London United Kingdom
J Thorac Cardiovasc Surg 20181562124-32
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacement
bull Methods This RCT compared MS with FS for first-time isolated AVR in 2 United Kingdom National Health Service hospitals Primary endpoints were duration of postoperative hospital stay and the time to fitness for discharge from hospital after AVR analyzed in the intent-to-treat population
bull Results In this RCT 222 patients were recruited and randomized (n frac14 118 in the MS group n frac14 104 in the FS group) Compared with the FS group the MS group had a longer hospital length of stay (mean 95 days vs 86 days) and took longer to achieve fitness for discharge home (mean 85 days vs 75 days) Adjusting for valve type sex and surgeon hazard ratios (HRs) from Cox models did not show a statistically significant effect of MS (relative to FS) on either hospital stay (HR 0874 95 confidence interval [CI] 0668-1143 P frac14 3246) or time to fitness for discharge (HR 0907 95 CI 0688-1197 P value frac14 4914) During a mean follow-up of 760 days (745 days for the MS group and 777 days for the FS group) 12 patients (10) in the MS group and 7 patients (7) in the FS group died (HR 1871 95 CI 0723-4844 P frac14 1966) Average extra cost for MS was pound1714 during the first 12 months
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacementCentral Message
In the United Kingdomrsquos National Health Service compared with a conventional median sternotomy approach for surgical aortic valve replacement mini-sternotomy did not hasten recovery or hospital discharge and was not cost-effective
Measuring What Matters
Having lived through the growth of percutaneous coronary intervention and now seeing the expansion of transcatheter aortic valve replacement I find myself asking the somewhat existential question ldquoAre we measuring what matters to patientsrdquo
Thoralf M Sundt MD Division of Cardiac Surgery
Massachusetts General Hospital Boston Massachusetts
Ann Thorac Surg 20181061602
Measuring What Matters
In a study performed at Dartmouth-Hitchcock
elderly patients prioritized ability to pursue activities maintaining independence and reducing symptoms
over
mortality benefit
Coleywright M et al Patients defined goals for the treatment of sever AVS a qualitative analysis
Health Expect 2016 191036-43
Measuring What Matters
These sorts of ldquosoftrdquo outcome variables are challenging to us We think of ourselvesmdashat least I domdashas medical scientists interested in ldquohardrdquo endpoints
But our patients are challenging us to consider what they value most not what we can measure easily Irsquod say it is time for us to broaden our horizons and revisit how we can better measure what matters
Ann Thorac Surg 20181061602

Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacement
bull Methods This RCT compared MS with FS for first-time isolated AVR in 2 United Kingdom National Health Service hospitals Primary endpoints were duration of postoperative hospital stay and the time to fitness for discharge from hospital after AVR analyzed in the intent-to-treat population
bull Results In this RCT 222 patients were recruited and randomized (n frac14 118 in the MS group n frac14 104 in the FS group) Compared with the FS group the MS group had a longer hospital length of stay (mean 95 days vs 86 days) and took longer to achieve fitness for discharge home (mean 85 days vs 75 days) Adjusting for valve type sex and surgeon hazard ratios (HRs) from Cox models did not show a statistically significant effect of MS (relative to FS) on either hospital stay (HR 0874 95 confidence interval [CI] 0668-1143 P frac14 3246) or time to fitness for discharge (HR 0907 95 CI 0688-1197 P value frac14 4914) During a mean follow-up of 760 days (745 days for the MS group and 777 days for the FS group) 12 patients (10) in the MS group and 7 patients (7) in the FS group died (HR 1871 95 CI 0723-4844 P frac14 1966) Average extra cost for MS was pound1714 during the first 12 months
Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacementCentral Message
In the United Kingdomrsquos National Health Service compared with a conventional median sternotomy approach for surgical aortic valve replacement mini-sternotomy did not hasten recovery or hospital discharge and was not cost-effective
Measuring What Matters
Having lived through the growth of percutaneous coronary intervention and now seeing the expansion of transcatheter aortic valve replacement I find myself asking the somewhat existential question ldquoAre we measuring what matters to patientsrdquo
Thoralf M Sundt MD Division of Cardiac Surgery
Massachusetts General Hospital Boston Massachusetts
Ann Thorac Surg 20181061602
Measuring What Matters
In a study performed at Dartmouth-Hitchcock
elderly patients prioritized ability to pursue activities maintaining independence and reducing symptoms
over
mortality benefit
Coleywright M et al Patients defined goals for the treatment of sever AVS a qualitative analysis
Health Expect 2016 191036-43
Measuring What Matters
These sorts of ldquosoftrdquo outcome variables are challenging to us We think of ourselvesmdashat least I domdashas medical scientists interested in ldquohardrdquo endpoints
But our patients are challenging us to consider what they value most not what we can measure easily Irsquod say it is time for us to broaden our horizons and revisit how we can better measure what matters
Ann Thorac Surg 20181061602

Mini-Stern TrialA randomized trial comparing mini-sternotomy to full
median sternotomy for aortic valve replacementCentral Message
In the United Kingdomrsquos National Health Service compared with a conventional median sternotomy approach for surgical aortic valve replacement mini-sternotomy did not hasten recovery or hospital discharge and was not cost-effective
Measuring What Matters
Having lived through the growth of percutaneous coronary intervention and now seeing the expansion of transcatheter aortic valve replacement I find myself asking the somewhat existential question ldquoAre we measuring what matters to patientsrdquo
Thoralf M Sundt MD Division of Cardiac Surgery
Massachusetts General Hospital Boston Massachusetts
Ann Thorac Surg 20181061602
Measuring What Matters
In a study performed at Dartmouth-Hitchcock
elderly patients prioritized ability to pursue activities maintaining independence and reducing symptoms
over
mortality benefit
Coleywright M et al Patients defined goals for the treatment of sever AVS a qualitative analysis
Health Expect 2016 191036-43
Measuring What Matters
These sorts of ldquosoftrdquo outcome variables are challenging to us We think of ourselvesmdashat least I domdashas medical scientists interested in ldquohardrdquo endpoints
But our patients are challenging us to consider what they value most not what we can measure easily Irsquod say it is time for us to broaden our horizons and revisit how we can better measure what matters
Ann Thorac Surg 20181061602

Measuring What Matters
Having lived through the growth of percutaneous coronary intervention and now seeing the expansion of transcatheter aortic valve replacement I find myself asking the somewhat existential question ldquoAre we measuring what matters to patientsrdquo
Thoralf M Sundt MD Division of Cardiac Surgery
Massachusetts General Hospital Boston Massachusetts
Ann Thorac Surg 20181061602
Measuring What Matters
In a study performed at Dartmouth-Hitchcock
elderly patients prioritized ability to pursue activities maintaining independence and reducing symptoms
over
mortality benefit
Coleywright M et al Patients defined goals for the treatment of sever AVS a qualitative analysis
Health Expect 2016 191036-43
Measuring What Matters
These sorts of ldquosoftrdquo outcome variables are challenging to us We think of ourselvesmdashat least I domdashas medical scientists interested in ldquohardrdquo endpoints
But our patients are challenging us to consider what they value most not what we can measure easily Irsquod say it is time for us to broaden our horizons and revisit how we can better measure what matters
Ann Thorac Surg 20181061602

Measuring What Matters
In a study performed at Dartmouth-Hitchcock
elderly patients prioritized ability to pursue activities maintaining independence and reducing symptoms
over
mortality benefit
Coleywright M et al Patients defined goals for the treatment of sever AVS a qualitative analysis
Health Expect 2016 191036-43
Measuring What Matters
These sorts of ldquosoftrdquo outcome variables are challenging to us We think of ourselvesmdashat least I domdashas medical scientists interested in ldquohardrdquo endpoints
But our patients are challenging us to consider what they value most not what we can measure easily Irsquod say it is time for us to broaden our horizons and revisit how we can better measure what matters
Ann Thorac Surg 20181061602

Measuring What Matters
These sorts of ldquosoftrdquo outcome variables are challenging to us We think of ourselvesmdashat least I domdashas medical scientists interested in ldquohardrdquo endpoints
But our patients are challenging us to consider what they value most not what we can measure easily Irsquod say it is time for us to broaden our horizons and revisit how we can better measure what matters
Ann Thorac Surg 20181061602