HbSC disease –is it different and how should we manage it?
29
HbSC disease – is it different and how should we manage it? David Rees Department of Paediatric Haematology, King’s College Hospital, London
Transcript of HbSC disease –is it different and how should we manage it?
HbSC disease – is it different and
how should we manage it?
David Rees
Department of Paediatric Haematology,
King’s College Hospital, London
Different types of sickle cell disesease
• Severe sickle cell disease– HbSS
– HbS/β0thalassaemia
– Severe HbS/β+thalassaemia
– HbSOArab
• Moderate sickle cell disease– HbSC
– Moderate HbS/β+thalassaemia
– HbSDPunjab
• Mild sickle cell disease– Mild HbS/β++thalassaemia
– HbSE
– HbS/HPFH
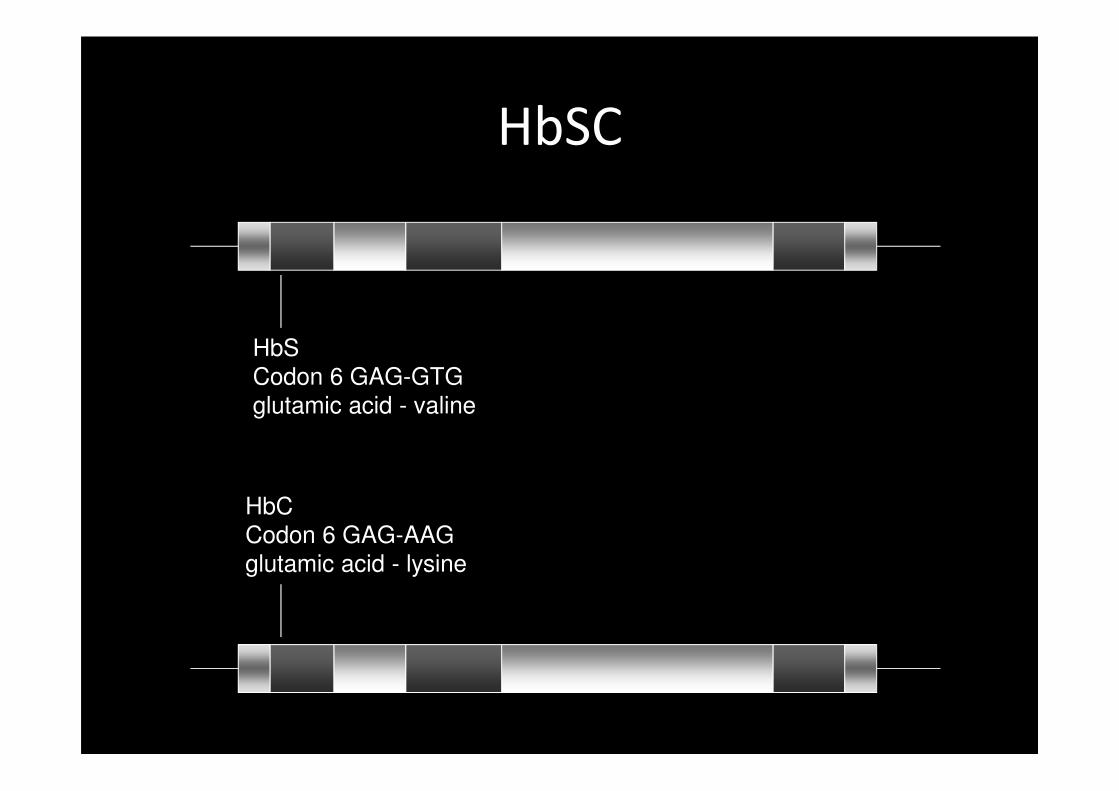
HbSC
HbC
Codon 6 GAG-AAG
glutamic acid - lysine
HbS
Codon 6 GAG-GTG
glutamic acid - valine
HbSC
• Population genetics
– HbC polymorphic in West Africa
– Reduced risk of P falciparum malaria with HbAC
and HbCC
– 25% population in some areas of West Africa have
HbSC
– 25-30% cases of SCD in UK, USA
• 3000 – 5000 people with HbSC in UK
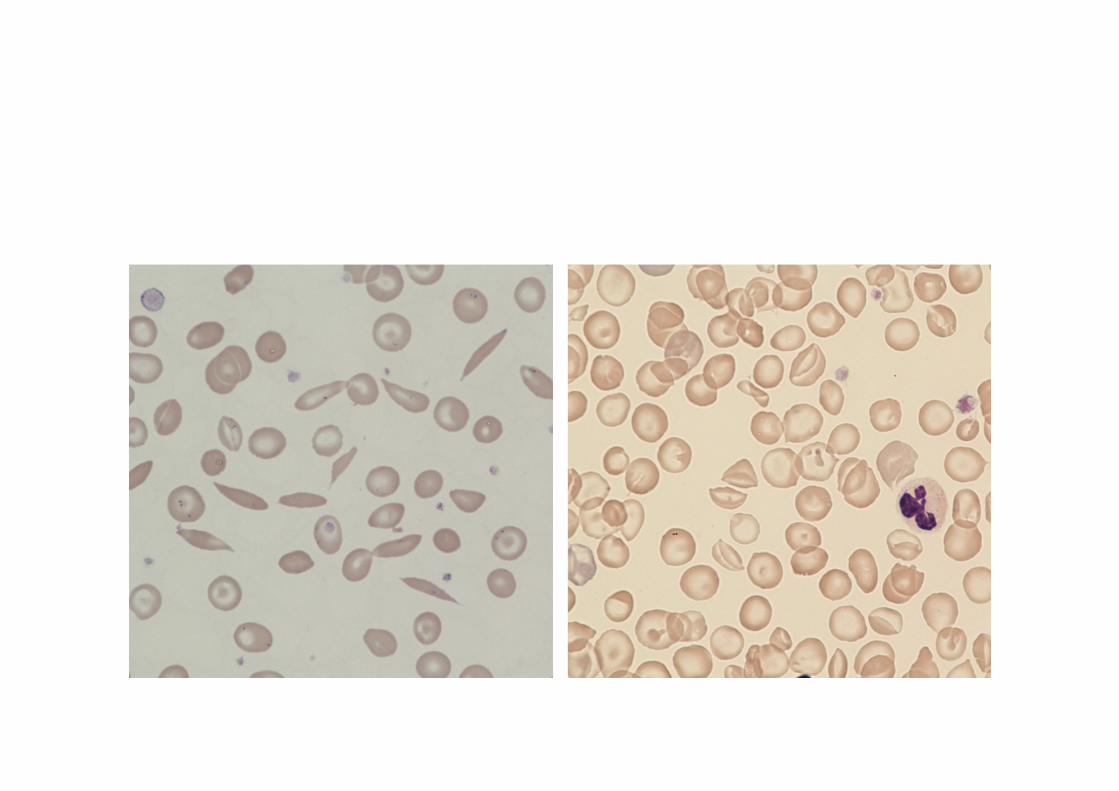
Diagnosis of HbSC disease
• Straightforward
• Suggested by blood film
• Haemoglobin analysis
• DNA analysis not usually necessary
– Unless unexpectedly severe phenotype
• Detected by neonatal screening
• Prenatal diagnosis offered in UK
Is HbSC different different to HbSS?
• Yes
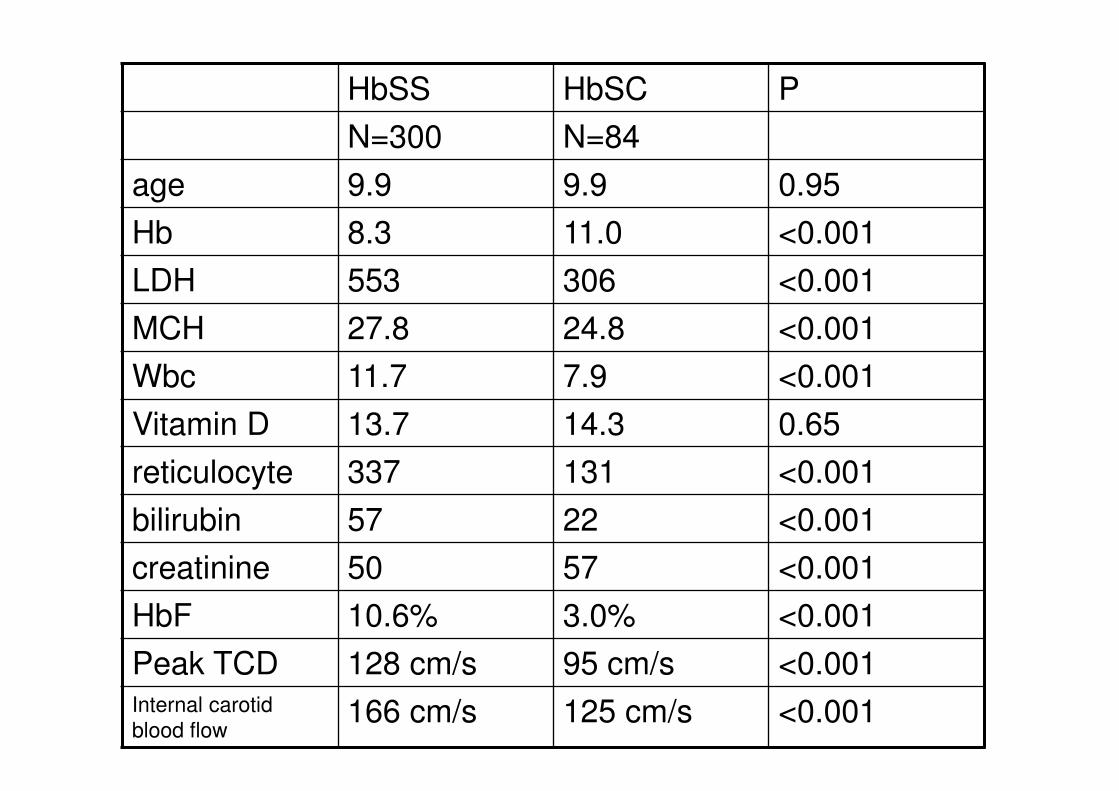
HbSS HbSC P
N=300 N=84
age 9.9 9.9 0.95
Hb 8.3 11.0 <0.001
LDH 553 306 <0.001
MCH 27.8 24.8 <0.001
Wbc 11.7 7.9 <0.001
Vitamin D 13.7 14.3 0.65
reticulocyte 337 131 <0.001
bilirubin 57 22 <0.001
creatinine 50 57 <0.001
HbF 10.6% 3.0% <0.001
Peak TCD 128 cm/s 95 cm/s <0.001Internal carotid
blood flow166 cm/s 125 cm/s <0.001
Pathophysiology
• Typical red cell contains– 47% HbC, 47%HbS, 4%HbF, 2%HbA2
• Red cell dehydration occurs– HbC binds to red cell membrane
– Abnormal cation transport• Red cell dehydration
– Increased intracellular HbS concentration
– Deoxygenation worsens dehydration and causes HbS polymerization
• HbC crystals form in oxygenated state
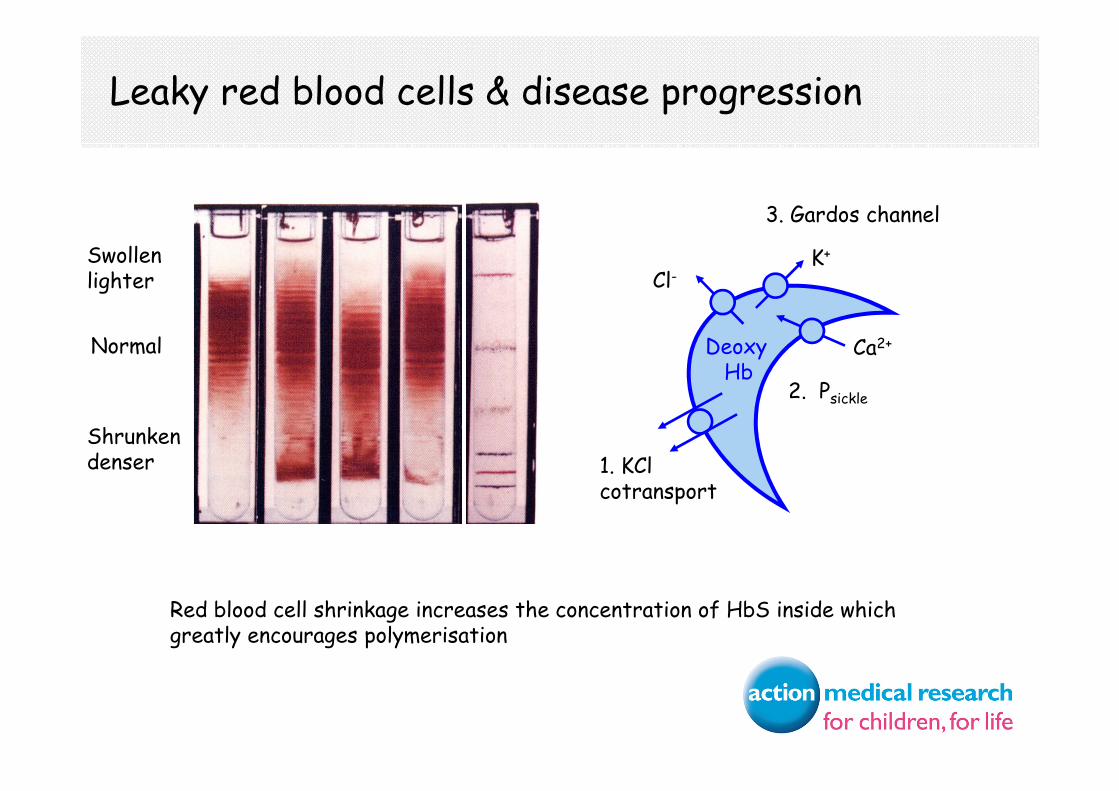
K+
2. Psickle
3. Gardos channel
Cl-
DeoxyHb
Ca2+
1. KCl cotransport
Leaky red blood cells & disease progression
Normal
Swollenlighter
Shrunkendenser
Red blood cell shrinkage increases the concentration of HbS inside which greatly encourages polymerisation
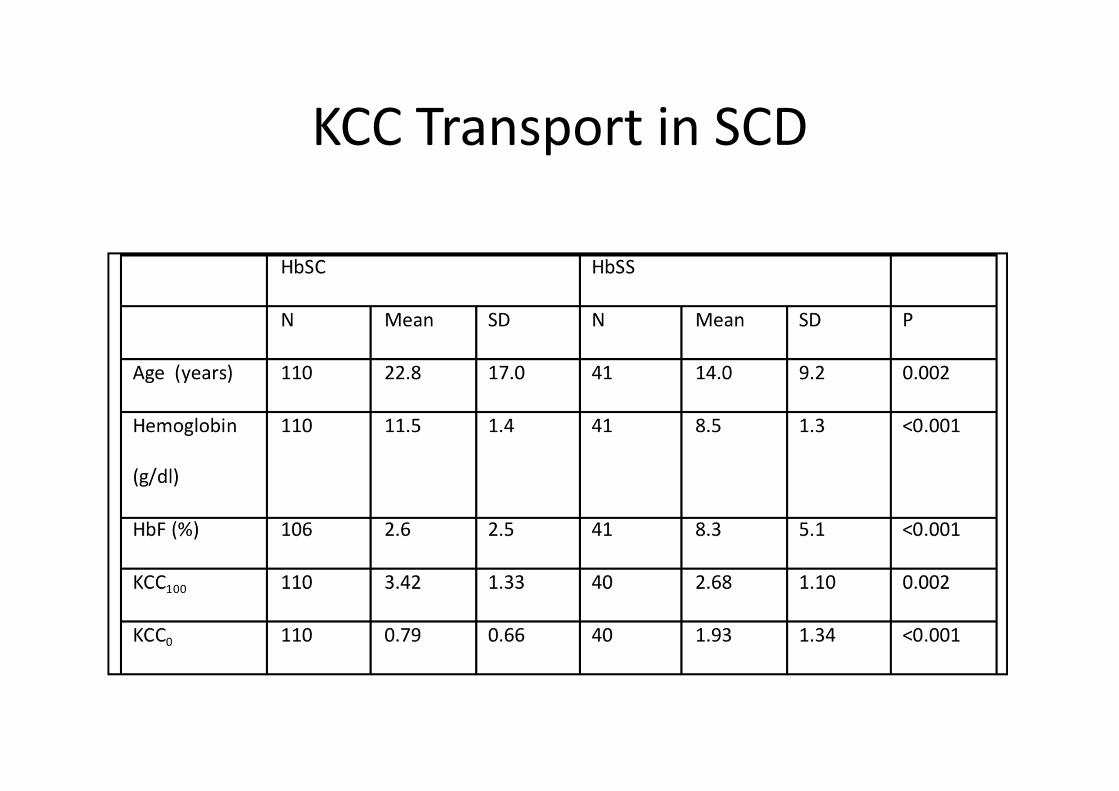
KCC Transport in SCD
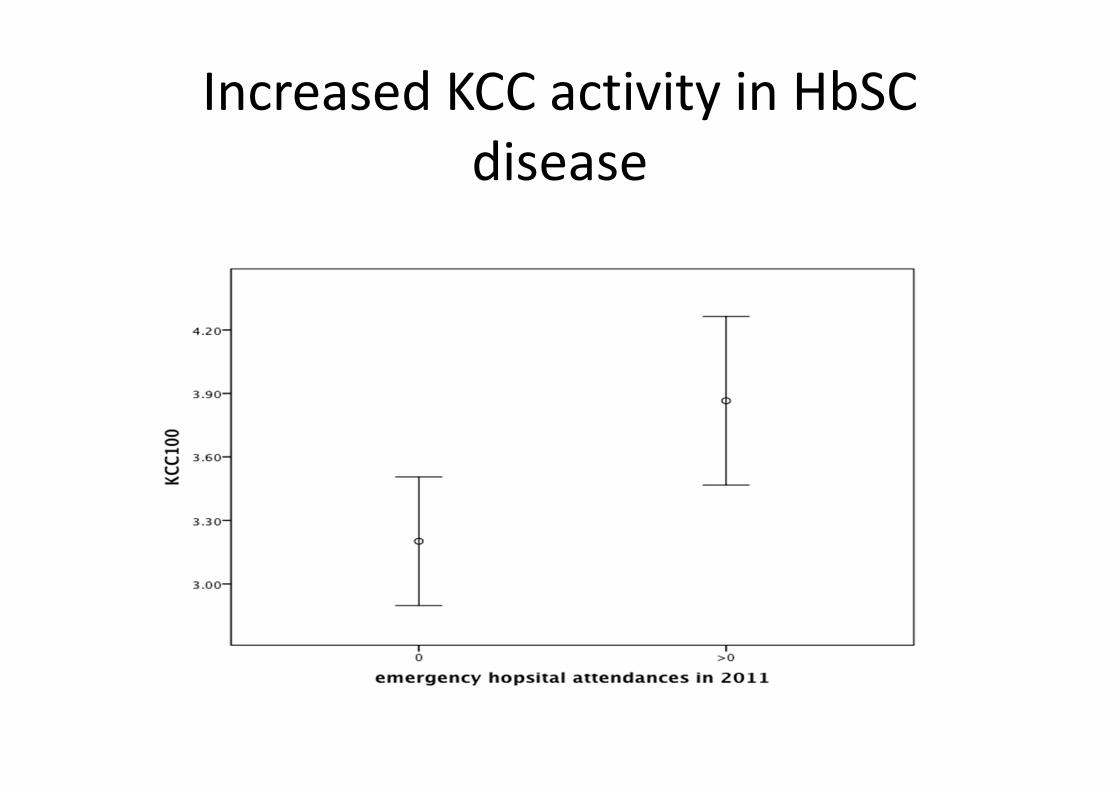
Increased KCC activity in HbSC
disease
Clinical Features of HbSC Disease
• Mortality
– Life expectancy 10-20 years greater than for HbSS
– Increased mortality evident only after the age of 20 years
– Median survival in USA
• 60 years for men
• 68 years for women
• Growth
– Normal height, weight
– Puberty at normal time
Stevens et al 1986
Clinical Features of HbSC Disease
• Acute pain
– Pain rate approximately half that of HbSS patients
– 0.4 episodes of acute pain per year
– 40% adults never experienced acute pain
• Acute chest syndrome
– Incidence similar to that in HbSS
– 30% patients affected
– Later onset than in HbSS and less likely to progress to
chronic lung disease
– Potentially more difficult to treat with higher haemoglobin
giving less scope for simple transfusion
Vichinsky at al 1997
Proliferative Retinopathy in HbSC Disease
• More common than in HbSS– Possible effect of increased blood viscosity
– Possible reduced damage to peripheral vessels results in more abnormal vessels
• 30% adults with HbSC have proliferative retinopathy (3% HbSS)– Clinically significant retinopathy in 8%
• Retinopathy rare before 14 years age
• 6% eyes of HbSC adults have significant visual impairment
Clarkson 1992, Condon et al 1972
Clinical Features of HbSC Disease
• Splenic function
– In children
• Splenic function preserved for longer
– normal at 4 years
• 6% children had splenic complications
– painful infarction, acute sequestration, haemorrhage
– In adults, on ultrasonography
• 50% have splenomegaly
• 40% asplenic
• 10% normal spleens
• 10% adults may benefit from splenectomy
Zimmerman et al 2000, Aquino et al 1997, Subbannan et al 2009
Clinical Features of HbSC Disease
• Renal complications
– Similar prevalence of papillary necrosis to HbSS
– 2.2% have chronic renal failure (half rate of HbSS)
– Median onset of chronic renal failure 25 years
later than in HbSS
Lesorbe et al, 1978
Clinical Features of HbSC Disease
• Cerebrovascular disease
– Stroke risk 50-100 fold greater than in general
population
– 2-3% patients have stroke
– Transcranial Doppler readings lower in HbSC than
HbSS
• Role of TCD not defined
Deane et al 2008
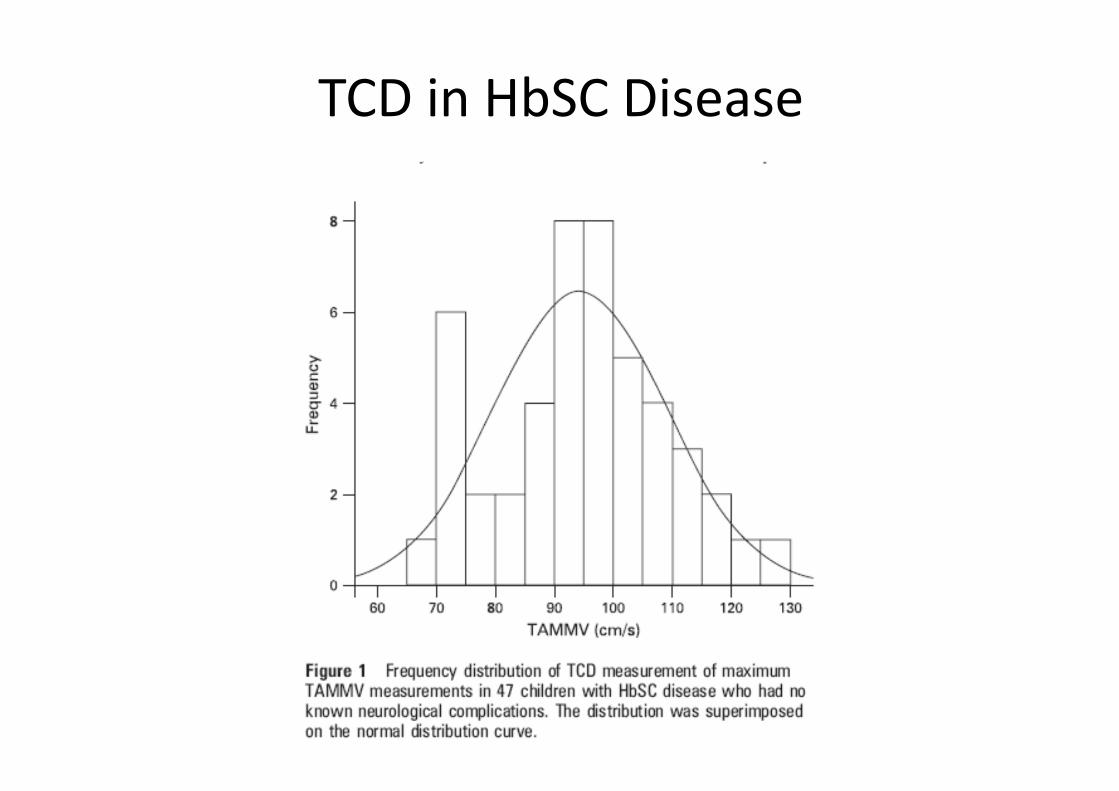
TCD in HbSC Disease
Clinical Features of HbSC Disease
• Pregnancy
– Pregnancy complications higher than controls
– HbSC sometimes first presents in pregnancy
– Pain, transfusion and UTI less common than in
HbSS
– ACS, hypertension, VTE similar incidence to HbSS
• Pulmonary hypertension
– Less common that HbSS but does occur
How should HbSC disease be
managed?
• No evidence interventions
• Management largely based on studies on
patients with HbSS
– Sometimes management inferred from studies of
HbSS
– Sometimes smaller numbers of HbSC incuded in
larger study
Pain in HbSC disease
• Precipitants not identified– Preliminary evidence suggests that environmental
factors may be different
• Intravenous fluids– Value unknown
• Oxygen– Unknown but theoretically harmful
• Increased cation red cell loss
• Formation of HbC crystals
• Transfusion rarely appropriate– Possible role for venesection
Infection in HbSC Disease
• Infection– Increased risk of infection but less than for HbSS
– Gram-negative bacteremia more prominent than pyogenic infections in HbSS
– Risk of septicaemia possibly greater in older children and teenagers
• Penicillin V
– PROPS study did not include children with HbSC disease
– usually prescribed for HbSC in UK as for HbSS
– In UK recommended life-long
– Increasing tendency to stop aged 5 years
– possible arguments for starting in later childhood
Lane et al 1994, Milner et al 1991
Management of HbSC Disease
• Primary Stroke Prevention
– Value of transcranial Doppler scanning undefined
– Possible role for children to have TCD at some point – eg at
5 and 10 years
– Different criteria needed for interpretation
– Abnormal > 130cm/s
• Silent cerebral infarctions
– Frequency and significance unknown
– MRI/MRA as clinically indicated
Miller et al 2001
Management of HbSC Disease
• Blood transfusion
– More likely to require exchange transfusion because of higher haemoglobin
– Transfusion targets based on keeping %HbS+%HbC below a certain level
• Perioperative management
– Not included in TAPS study
– 18% overall complication rate post-operatively
– In intra-abdominal surgery
• 35% incidence of ACS or acute pain in untransfused
• 0% incidence in transfused patients
Hydroxyurea and HbSC disease
• No randomised controlled studies
• Study of 15 patients from North America
– Yates et al, Paediatr Blood Cancer 2013;60:323-325
– HU dose: median maximum 24mg/kg
– No change in total Hb: 10.5 vs 1.8g/dl
– Increased MCV 72.5 vs 91.7fl
– Increased HbF: 2.2% vs 7.3%
– Reduced episodes of pain: 1.18 vs 0.44/year
– Reduced ACS: 0.24 vs 0 /year
– Recurrent thrombocytopenia main side-effect
Magnesium and hydroxyurea
• Randomised controlled trial in HbSC disese
– 5 – 53 years old
– Endpoint: reduction in hyperdense cells
• HU + placebo
• Mg + placebo
• Hu + Mg
• Placebo + placebo
– Stopped early because of slow recruitment
– Mg had no effects, but no effective inhibition of HbSC achieved
Conclusions
• HbSC is significantly different to HbSS– less severe– Much less evidence on management
• Need specific patient/parent information for children with HbSC– Currently not available
• Need to say different things to parents of neonates with HbSC– No evidence that splenic palpation is useful– 40% chance of being asymptomatic– Risk of life and organ threatening complications low
• Need research specifically on HbSC disease