Febrile Rash and Convalescent Rash of Dengue Fever · INDIAN PEDIATRICS 717 VOLUME 50__JULY 15,...
2
INDIAN PEDIATRICS 717 VOLUME 50 __ JULY 15, 2013 I M A G E S I M A G E S I M A G E S I M A G E S I M A G E S Febrile Rash and Convalescent Rash of Dengue Fever A 1-year-old boy infant presented with fever for 3 days. On examination he was febrile and his face, trunk and extremities were erythematous which blanched upon pressure (Fig. 1). His platelet count dropped to 83,000 per μL on day 5 of illness. His dengue serology IgM was positive suggestive of primary dengue infection. A 9-year-old girl presented with fever for 4 days. On day 8 of illness, when her fever subsided, she developed hypotension. Her platelet count dropped to 15000/ml and hematocrit increased to 42.8%. She was resuscitated with fluid boluses. She developed typical dengue rash of convalescence 3 days after defervescence (Fig. 2). Her dengue serology IgM and IgG were positive, suggestive of secondary dengue infection. During the first 24-48 hours of fever, children with dengue fever may develop a transient generalized macular erythematous rash which blanches upon pressure. The convalescent rash of dengue fever appears about 2-3 days after defervescence. It is characterized by generalized confluent petechial rash which does not blanch upon pressure, with multiple small round islets of normal skin. It is otherwise called “white islands in a sea of red”. Some children with this rash may experience generalized pruritus. This rash gradually fades over one week. AM VIJAYALAKSHMI AND A JAYAVARDHANA Department of Pediatrics, PSG Institute of Medical Sciences and Research, Peelamedu, Coimbatore 641 004. Tamil Nadu, India. [email protected] FIG. 1 Febrile rash of dengue which blanches upon pressure. FIG. 2 Convalescent rash of dengue – “White isles in the sea of red”. Darier-White Disease A 6-years-old boy presented with multiple dark, raised lesions all over the body since 1 year (Fig. 1a). The disease began with discrete hyperpigmented hyperkeratotic papules over the knee and elbows which later progressed to involve the preauricular region, ear lobe, neck, both flexor and extensor aspect of upper limbs and lower limbs and buttocks (Fig. 1b). There was history of photo- exacerbation of the lesions. The child complained of pruritus and difficulty in sitting due to pain because of multiple hyperkeratotic lesions over the buttocks. There was presence of palmar pits. Oral mucosa and nails were normal. His 4-year-old sibling also presented with similar lesions over the knees and elbows. A clinical diagnosis of Darier-White disease was made. Histopathological examination from punch biopsy of a lesion showed acantholysis along with classical dyskeratosis and hyperkeratosis in the epidermis.
Transcript of Febrile Rash and Convalescent Rash of Dengue Fever · INDIAN PEDIATRICS 717 VOLUME 50__JULY 15,...

INDIAN PEDIATRICS 717 VOLUME 50__JULY 15, 2013
I M A G E SI M A G E SI M A G E SI M A G E SI M A G E S
Febrile Rash and ConvalescentRash of Dengue Fever
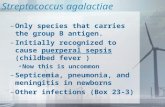
A 1-year-old boy infant presented with fever for 3 days. Onexamination he was febrile and his face, trunk andextremities were erythematous which blanched uponpressure (Fig. 1). His platelet count dropped to 83,000 perμL on day 5 of illness. His dengue serology IgM waspositive suggestive of primary dengue infection.
A 9-year-old girl presented with fever for 4 days. Onday 8 of illness, when her fever subsided, she developedhypotension. Her platelet count dropped to 15000/ml andhematocrit increased to 42.8%. She was resuscitated withfluid boluses. She developed typical dengue rash ofconvalescence 3 days after defervescence (Fig. 2). Herdengue serology IgM and IgG were positive, suggestive ofsecondary dengue infection.
During the first 24-48 hours of fever, children withdengue fever may develop a transient generalized macularerythematous rash which blanches upon pressure. Theconvalescent rash of dengue fever appears about 2-3 daysafter defervescence. It is characterized by generalizedconfluent petechial rash which does not blanch uponpressure, with multiple small round islets of normal skin. Itis otherwise called “white islands in a sea of red”. Somechildren with this rash may experience generalized pruritus.This rash gradually fades over one week.
AM VIJAYALAKSHMI AND A JAYAVARDHANA
Department of Pediatrics,PSG Institute of Medical Sciences and Research,
Peelamedu, Coimbatore 641 004. Tamil Nadu, [email protected]
FIG. 1 Febrile rash of dengue which blanches upon pressure.
FIG. 2 Convalescent rash of dengue – “White isles in the seaof red”.
Darier-White Disease
A 6-years-old boy presented with multiple dark, raisedlesions all over the body since 1 year (Fig. 1a). The diseasebegan with discrete hyperpigmented hyperkeratoticpapules over the knee and elbows which later progressed toinvolve the preauricular region, ear lobe, neck, both flexorand extensor aspect of upper limbs and lower limbs andbuttocks (Fig. 1b). There was history of photo-
exacerbation of the lesions. The child complained ofpruritus and difficulty in sitting due to pain because ofmultiple hyperkeratotic lesions over the buttocks. Therewas presence of palmar pits. Oral mucosa and nails werenormal. His 4-year-old sibling also presented with similarlesions over the knees and elbows. A clinical diagnosis ofDarier-White disease was made. Histopathologicalexamination from punch biopsy of a lesion showedacantholysis along with classical dyskeratosis andhyperkeratosis in the epidermis.

INDIAN PEDIATRICS 718 VOLUME 50__JULY 15, 2013
IMAGES
FIG. 1 Multiple hyperkeratotic lesions including (a) knees andelbows, and (b) buttocks.
(a) (b)
Darier-White disease or keratosis follicularis is said tooccur as a result of mutation in the ATP2A2 gene located onchromosome 12q23-24.1, responsible for coding sarco/endoplasmic reticulum calcium ATPase type 2 (SERCA2).It is characterized clinically by hyperkeratotic papulesdistributed mostly on the seborrheic areas of the body. Nailinvolvement is characterized by V-shaped nicking at thedistal aspect of the nail bed, longitudinal red and whitealternating bands, and subungual hyperkeratosis. Mucosalmembrane involvement may occur as white papules on thebuccal mucosae, palate, and gingiva with a cobblestoneappearance. Palmoplantar involvement usually presents asdiscrete, punctate keratoses that appear as small,hyperkeratotic papules or small, centrally depressed pits. Inflexures like axilla and groin, the lesions may become largeexuberant growth. They may get infected due to constantmaceration resulting in malodorous purulent discharge.Heat, sweat, humidity, sunlight, oral corticosteroids andmechanical trauma have been reported to exacerbate thiscondition.
Conventional therapy for severe disease still reliesgreatly on oral retinoids. Acitretin is effective at 0.6 mg/kg/day, the hyperkeratosis is reduced and papules areflattened. Basic measures include use of sunscreens, coolcotton clothing, and avoidance of hot environment.Moisturizers with urea or lactic acid can reduce scaling andhyperkeratosis. Surgical treatment includes dermabrasion,carbon dioxide laser, and the erbium YAG laser. Thecondition runs a chronic relapsing course, withexacerbations throughout life.
NIRUPAMA PARWANDA, *NEETI KUMARI AND#PRAVEEN BHARDWAJ
From the Department of Dermatology,Patna Medical College and Hospital, Patna;
*SGRRIMHS, Dehradun; and #Dermatology,Bangalore Medical College, Bangalore, India.
BBBBB OOOOO OOOOO K K K K K R R R R R EEEEE VVVVV IIIII EEEEE WWWWW
Clinical Assessment andManagement of ChildhoodPsychiatric DisordersSAVITA MALHOTRA
CBS Publishers & Distributors; NewDelhi.Pages: 226; Price: Rs. 350/-
This edition contains 12 chapters anda glossary of terms, Child Guidance Clinic Proforma andimportant assessment scales (many by the author) adaptedfor India. The development perspective of the child hasbeen provided with an emphasis on the roles of family andschool. The approach to psychological, psychiatric andneurodevelopment assessment is elucidated in detail. The
International classifications of childhood psychiatricdisorders is also given. The important issues related toadolescence are discussed separately. The book providessteps to diagnose and treat common childhood psychiatricemergencies. The simple presentation style of the bookmakes it useful for undergraduate and postgraduatestudents, pediatricians and mental health professionals.Inclusion of case reports, photographs, and childhoodproblems related to schools in future edition will enrich thetext and make it also useful for teachers and parents.
MS BHATIA
Professor & Head, Department of Psychiatry,UCMS & GTB Hospital, Dilshad Garden,
Delhi 110 095, [email protected]









![The host immune response in respiratory virus infection ... · (IFN-α/β receptor), activating the JAK/STAT pathway [3]. ... croup, tonsilitis Seasonal influenza Sialic acids Fever,](https://static.fdocument.org/doc/165x107/5c7b1b0809d3f277748b45cf/the-host-immune-response-in-respiratory-virus-infection-ifn-receptor.jpg)