Pediatrics as discipline Department of pediatrics.
90
Pediatrics as discipline Department of pediatrics
-
Upload
brianne-harrison -
Category
Documents
-
view
303 -
download
5
Transcript of Pediatrics as discipline Department of pediatrics.

Pediatrics as discipline
Department of pediatrics

Pediatrics
•Pediatrics is a Greek term , which proceeds from two words:
•παῖς (pais = child) • ἰατρός (iatros = doctor )

History of pediatrics• • Hippocrates described cephalohematoma,
hydrocephalus, diarrhea, strophulus, asthma and varicella• • Soranus of Ephesus (c. AD 100) described the test for
maternal milk quality appreciation (if the milk drop sticks to the nail, it has sufficient fats, if does not stick – has not fats)
• • Galen (c. AD 200) described otitis, pneumonia, prolapse of intestin, rickets.
• • Avicenna, (c. AD 990) – tetanos, convulsions, meningitis, omphalitis.
• • Avenzoor (c. 1150) performed tracheotomy. • • Hieronymus in 1583 has writen the book De Morbus
Pusiorum

History of pediatrics
• In IX century - Rhazes (Muhammad ibn Zakarīya Rāzi - Persia) has described the child’s diseases (is considering the father of pediatrics).
• 1530 Thomas Phaer, Book of the child. • 1852 first hospital in London The Hospital
for Sick Children, Great Ormond • Abraham Jacobi, - the founder of pediatrics
in USA .

History of pediatrics
•Hôpital des Enfants Malades (French = Hospital for Sick Children), in Paris , june, 1802
•Charité (hospital founded in1710) in Berlin has opened a separately pavilion for children in 1830
•Saint Petersburg - 1834 • Vienna and Breslau (Wrocław) - 1837.

History of pediatrics
•Thomas Sydenham (1624–1689), Hippocrate of England, described scarlet fever, rubella, epilepsy, rickets, fever, scorbutus, chorea which is known as St. Vitus Dance.

History of pediatrics
•Edward Jenner (1749–1823) has vaccinated first time a 8 years boy against smallpox.


History of pediatrics•Prof. Mihail Manicatide, born at Giurgiu
in 1867, is considered the founder of rumanian scientific school of pediatrics.
•He is the author of two treatises of infant medicine for students, appeared in many editions.
•Dr. Alfred D. Rusescu, born in 1895 at Bucharest, organized pediatrics and superior medicine studies on modern basis, being the mentor of great professors which developed the pediatrics until our times.

History of pediatrics
•Faculty of Medicine from Yassy opened its courses at 1 december 1879, but the chair of infantile Clinic appears la 1897.
•The chair had as basis the Gregorian Institute founded in 1852, and the clinical base functioned in the infantile section of Epitropia “Holy Spiridon" from Yassy.

Pediatrics
• Pediatrics has as study object the growing, development and pathology of the child from the birth until 18 years age.

Pediatrics - subspecialities:• preventive pediatrics; • social pediatrics;• neonatology (new-born - 0-28 days); • infantile psychiatry; • cardiology; • pediatric pneumology; • nutritional and metabolism diseases; • oncology; • surgery, orthopedy and pediatric
traumatology.

Preventive pediatrics• includes all measures destined to maintain the health
and to prevent the appearance of disease in children. • It is dividing in :
Primary prophylaxis – avoidance of healthy individual taking ill (vaccination, water chlorining)Secondary prophylaxis– recognition and elimination of disease precursors and the addressing to population with increased risk for certain affection. Includes also the diseases complications prevention.Tertiary prophylaxis– has the goal the improving or stopping of still established disease complications, avoiding the evolution to invalidity or decease.

Primary prophylaxis
• includes 2 types of measures:A) measure applied to collectivity
B) measure applied individually

Measure applied to collectivity• A) it is realizing through a series of public
health programs which differ from country to country in function of its development degree.Some programs of public health with central value are not still universally adopted.Applied measures: - accidents prevention– is difficult and can’t be performed through public education.Prevention of intoxications (detergents, alcohol, mushrooms etc.)prevention of suicides and murdersprophylaxis of pregnancy in adolescentsprevention of drugs using.

Pediatrics – in Republic of Moldova
creation of abilities for physical and neuropsychical health state assessment in children and adolescents
• care and alimentation of healthy and sick child
• organization and carrying out of prophylactic, sanitaro-antiepidemical and medical measures at home and in preschool and school institutions

Pediatrics – in Republic of Moldova• Correct diagnosis of acute and chronic
diseases on the base of anamnesis, clinical and paraclinical examination, conformable to WHO diseases classification
• appreciation of investigations and treatment volume after national standards of RM
• According to emergency care to children at stages home - FDC - hospital
• assimilating of correct dispensary control of healthy and sick children.

Goal of discipline:
Study of child’s physiologic and pathologic changes, knowledge of child’s diseases evolution, diagnosis, treatment and prophylaxis, development of clinical reasoning and medical synthesis – defining elements in the training of each physician.

Objectives of forming:• To appreciate the state of physical and
neuropsychical development, to determine the groups of health and risk in children;
• To perform the collection of anamnesis and objective clinical examination of children, interpretation of collected data;
• To argue the prescribing and interpretation of laboratory investigations and paraclinical examination in dependence of basic pathology and national standards;
• To possess the general medical manoeuvres in diverse pathologies of the child;

Objectives of forming:
• Enteral and parenteral alimentation;• gastric washing, performing of evacuator and
medicamentous enemas, urinary bladder catheterization;
• Determining of pulse, arterial pressure, respiration rate;
• Interpretation of radiologic, ultrasonographic, ECG data, general laboratory, microbiologic, biochemical, immunologic investigations;
• To determine the tactics of medical conduct in the cases of emergencies: shock, coma, acute respiratory and cardiac failure, crisis of bronchial asthma, accidental poisonings, traumas, insect bites, sinking.

Childhood periods
•There are evidencing the following periods:
• · new-born period (4 weeks); • · suckling period (until 1 year); • · period of milk teeth (from 1 until 6-7 yrs); • · period of big childhood (from 8 until 11
yrs); • · period of sexual maturation (12-17 yrs).

Period of new-born
• It constitutes the period to extrauterine life adaptation, in which a series of characteristic phenomena have place, for example: physiologic icterus, physiologic weight loss, genital crise etc.
• Duration of new-born period is considered until the age of 30 days (so- the first month of life).

Period of suckling
• This period, which lasts from 1 month until 1 year, is characterized by very active growing.
• The period of suckling has the most rapid period of growing, not spread in another periods. In this period, also, the psychomotory development of suckling is in permanent progress, especially due to continuous development of nervous system.


Period of infant (little child)• After 1 year age, the child is not still
considered suckling baby, he walks alone, speaks, becomes active. The growing in height and weight is less accentuated.
• This period includes the age between 1 and 3 yrs. In this period the surrounding conditions organization is very important.
• Correct infant follow-up, good conduced education work contributes to assimilation of first hygienic skills and of elementary education rules.

Preschool period
• It occurs between 3 and 7 yrs, the age in which the child’s mind intensively develops due to more complex development of central nervous system.
• Assimilation of knowledge about surrounding world increases continuously, in report with development of attention, spirit of observation, memory.
• The child becomes more independent, due to continuous development of these functions.

School period• The growing rhythm is more lent at this
period beginning (in comparison to preschool age), for to its end to accelerate, at the same time with puberty appearance.
• Gradually, the exterior aspect of pupil gets near to that of adult. Due to central nervous system maturation, the pupil has more complex psychic activity, which allows to assimilate various and ample knowledge.

•SEMEIOLOGY semeion – sign logos – science, speech Semeiology is the fundamental basis of diagnosis which
can be established on the basis of anamnestic data which orientates, of clinical data which substantiate and of laboratory data which confirm it.
•Semeiology – interpretation of different diseases signs having the goal to establish more correctly and more rapidly the diagnosis.
•Semeiology uses symptoms, signs, syndromes and also paraclinical investigations which must be aimed for diagnosis confirmation.

•Symptoms – have subjective character, being related by patient, are variable in different cases, after perception mode and not always are objective (fever, headache, insomnia, astenia, hiccups, dyspnea etc.)
•Signs – objective manifestations produced by disease, observed by patient and completed by physician through proper feelings(e.g. murmur, rale, dullness etc.)
•Syndrome–group of symptoms and signs which expresses a pathologic state, which have a common physiopathologic mechanism; allow by their sum the orientation to certain diagnosis; for elucidating or confirmation the complementary investigations as possible aimed are performing. Conclusion resulted from signs and symptoms analysis and confirmation by analyses guide us to the diagnosis which could be also a syndrome.

• The health – is defined by WHO as „ a state of complete physical, mental and social good and not consists only from disease or inflammation absence”
• The disease is defined in different mode but after Rumanian medical dictionary represents: „ deviation from health state due to some internal medium modifications or external medium agents action” or „ is a deviation or turning off from normal with undesirable consequences on personal comfort and social activity”.
• Acute disease – a short duration episode at the end of which the patient takes again his normal activity.
• Chronic disease– a long duration disease which generates permanent, partial or total incapacity, there is an organic or functional alteration which obligates the patient to modify his normal life mode and which persists more long time.

Teguments• At birth, the epidermis is very thin and the
smallest irritation produces lesions which very easily are infecting.
• New-born has the skin covered by protector fat layer (named vernix caseosa), after removal of which the fine epidermis, by pink color, appears.
• The skin has the protection role of organs which it covers, of body constant temperature maintaining; has, also, the respiration function, which in children is very important.

Teguments
•Subcutaneous layer of fat is not completely formed at birth, and is developing gradually:
•It appears first of all on face, after that on superior and inferior members, thorax and after all on abdomen (in the age around 45 days).

Skin fold
•It has in suckling babies the thickness by 1,5-2 cm. This fat layer (cellular, subcutaneous tissue) has the role of protection, role in the thermoregulation mechanism, role of nutritive reserve and of diverse organs supporting.
• In healthy child, the teguments palpation gives a special sensation of resistance to pressing.

Teguments of suckling baby• In healthy breast fed suckling they are
white-pink, velvet-like, in artificially fed they are more pale.
• The thickening of epidermis horny layer and basal cells pigment appearance begin, the chromatoforming cells develop, the resistance to infections and physico-chemical agents increases.
• Dermis is maturating, the dermal papillae are multiplying, the capillaries become longer.

Teguments of suckling baby
•are elastic, skin fold returns immediately to initial form;
• in dehydration states the fold returns slowly or is persistent.

Sebaceous glands
• good developed at birth, have sometimes an excess of secretion which determines the appearance of seborrheic dermatitis at the head skin level.

Sweat glands
•Begin to develop in 2-3 months age and in 2 yrs when the corresponding nervous centers are maturating achieve their integral functional activity.

Hair
•During growing they change the color. •During the puberty installation as part of
secondary sexual characters the facial, axillar, anterior thoracic, pubian, on external part of members hair growing appear.

Suckling skin surface• It is big in report to his corporal weight and decreases
with the age.• Skin surface is calculating after Lassabliere formula:• Skin s. =T 2x0,92• Specific skin surface represents the report between
skin surface and corporal weight:• Skin s. (in cm 2)/W(kg) • in n.b. specific skin surface = 660 cm 2/kg body; • in 1 year specific skin surface = 420 cm 2/kg body; • in adult specific skin surface = 220 cm 2/kg body.

Cellular subcutaneous tissue
• Good represented in new-born on the face, continues to develop on superior, inferior members, thorax and still at 6 weeks on abdomen.
• In malnutrition states its disappearance occurs in the inverse order of its appearance:
• abdomen, thorax, inferior members, superior members, and at the end - on face (Bichat pads disappearanse).

Clinical assessment of suckling nutrition state• Measurement of thoracic (normal 1-1,5 cm)
and abdominal (1,5-2 cm) skin fold thickness, • Presence of adductors folds on thigh internal
part• presence of turgor (resistance which we feel
at pressure taking between fingers the tissues on the external part of thigh;
• in malnutrition – the disappearance of cellular subcutaneous tissue
• turgor is diminished; sometimes is pasty in suckling babies excessively fed with floury products).

Clinical assessment of suckling baby nutrition state•More precise assessment of nutrition
state is realizing calculating: •ponderal index(PI),• perimeter of medium arm (MAP), •Nutritional index (NI) and • body Mass Index - BMI.

EXAMENATION OF TEGUMENTS, MUCOSAE AND DERIVATES
• COLOR OF TEGUMENTS Pallor : there is more open color of teguments and mucosae and appears in
the case of superficial circulation reducing, in vasoconstriction or appears more frequently in anemias.
• - iron deficient anemia – waxy or chalk pallor • In hemolytic and megaloblastic anemia –yellowish, like to wheat straw.• In chronic leukemia and CRF – a grey-sallow color appears• In bacterial infectious endocarditis – pallor is by milk coffee type
Redness :appears through accentuated vasodilatation or circulatory oxihemoglobin quantity increasing (polyglobulia)
After exposure to increased temperature or in febrile states, after physical effort, in neuro-vegetative dystonia, in carbon oxide intoxication, in primary or secondary polyglobulias.

Cyanosis (kianos) :there is a bluish – violet color of skin and mucosae and appears due to reduced hemoglobin increasing at the level of small vessels in certain areas.
True cyanosis: in conditions of reduced hemoglobin absolute quantity increasing. In capillaries (over 5 g /100 ml of blood). It appears more at extremities and depends from some factors:
- volume of skin and mucous capillaries, thickness and transparence of cutaneo-mucous layer (best observed on ears lobes, cheek bones, lips and nail bed).
-skin pigmentation (in black race or other skin hyperpigmentations) it is better seen on palms or conjunctival mucosa
-association with other pigments in the same time, for ex. with jaundice
-concentration of Hemoglobin in blood, appearing more rapidly in polyglobulia than in anemia
False cyanosis appears in:
-intoxication with carbon oxide (carboxyhemoglobinemia), which has a bluish color with carmine tint
-polycytemia vera, when the cyanosis has red-violet aspect

-methemoglobinemia and sulphhemoglobinemia (intoxication with nitrites, nitrotoluene, benzene etc)
-argiria – deposition of silver salts in teguments, giving a bluish-grey colouring
In the cyanosis appearance the absolute level of redused Hemoglobin has importance. La anemics, especially at values ↓5 g. /100 ml blood the cyanosis can’t be distinguished.
CENTRAL CYANOSIS: is due to insufficient saturation of arterial blood with oxygen, which leads to reduced Hemoglobin absolute level increasing in arterial blood over limit value of 5 g/100 ml. This cyanosis is generalized and involves both teguments and mucosae, the temperature being not decreased; there is so-called warm cyanosis
Causes of central type cyanosis:
1. Respiratory causes:
-affections which reduce the circulation bed: massive pneumonias, bronchopneumonias, miliar TBC, extended pulmonary fibroses, massive pleuresies, pneumothorax, fibrothorax, kypho-scoliotic thorax, etc.
- Affections which produce the respiratory pathways obstruction: laryngo-tracheal diseases, tumors which compress respiratory pathways, bronchial asthma, chronic broncho - pulmonal obstructive diseases, etc.

2. Cardiac causes:
- left cardiac failure, mitro-aortic valvulopathies, cardiomyopathies, disorders of rhythm and conductibility.
- congenital complexe cardiopathies which can be installing at birth, persisting all life
– blue disease. - Potent ductus arteriosus
- arterio-venous fistulas of great and middle vessels, with veno-arterial shunt after aneurismas or on small vessels, in hereditary telangiectasia.
3. Mixt causes: cardiac and respiratory. The chronic cor pulmonale in which the right heart failure consecutively some broncho - pulmonal affection appearing, is typically.
PERIPHERAL CYANOSIS:is determined by vasoconstriction followed by blood circulation speed slowing in a peripheral area, which leads to increased oxygen extraction by tissues from arterial blood.
- Generalized cyanosis: appears after exposure to cold or in congestive cardiac failure, when the cutaneous compensatory vasoconstriction is associated. It is more pronounced on the limbs which are cold and in the right and congestive cardiac failure the edemas can appear.

-Localized cyanosis– appears in venous or arterial trunks obstructions and is strictly localized at corresponding area. If the obstacle is in superior vena cava the cyanosis of cephalic extremity, of superior members, of neck and of thorax superior part appears(cyanosis in pelerine with or without edema).
Disorders of pigmentation:-Hypomelanoses are characterized by melanic pigment decreasing or absence. The
albinism characterized by absence of pigment in skin, hair and eyes and vitiligo characterized by light color with hyperpigmented contour spots appearance take part from this group.
-Hypermelanoses appear through numeric increasing of melanic cells and their overloading with pigment and are due to hormonal causes: chronic insufficiency of suprarenal glands (Addison disease), hyperthyroidism (Basedow disease). Ephelides- small brown – redish spots on cheeks, shoulders, back, dorsal part of hands appear through pigmentation of skin under the form of freckles and have familial and constitutional character.
-Icterus is the yellow colouring of the skin, mucosae and scleres determined by their impregnation with bilirubin when it has increased values in blood (over normal value by1mg at 100 ml of blood).

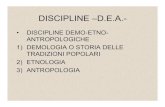
Teguments in childrenHyperpigmentation Hyperpigmentation

CUTANEOUS LESIONS: Macula: smooth spot, by pink or redish color, with small dimensions (under 1cm
diameter) which not exceeds tegumentar plane and appears in erruptive infectious diseases such as measles, rubella, typhoid fever.
Papule :a small, round prominence on skin, with the diameter under 0,5 cm, palpable; appears in scarlet fever, urticaria
Nodule is a dermic or hypodermic formation by varied dimensions, palpable, which appears in xantomatosis, lipomatosis, erythema nodosa.
Vesicle is a raised above the surrounding skin plane, under 1cm diameter, fluid-filled lesion which appears in varicella, herpes Zoster.
Bulla is a vesicle with purulent content which appears in acnea, variola, impetigo. Cyst is a soft, raised, encapsulated lesion filled with semisolid or liquid contents. Crusts have deposits of solidified exudates on tegument surface which appear in the
evolution of herpes, zone Zoster or as consequence of erosions, ulcerations or at the level of cutaneous eczema.
Cicatrix appears after skin plagues healing where the fibrous tissue is developing. Fissures are deep linear defects of the skin below its basal membrane level. Erosion is a superficial defect of the skin.

Ulcer is a deep defect of the skin below its basal membrane level. Gangrena is a necrosis of tissue and underlying stratum which can suprainfect
becoming fetide. Scar is a change in the skin secondary to some injury or inflammation. Sites may be
erythematous, hypopigmented or hypertrophic depending on their age or character. Sites on hair-bearing areas may be characterized by destruction of hair follicles.
Atrophy is an acquired loss of substance. In the skin, this may appear as a depression with intact epidermis (i.e., loss of dermal or subcutaneous tissue) or as
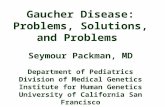
sites of shiny, delicate, wrinkled lesions (i.e., epidermal atrophy). Vascular lesions at the skin level: Petechiae: are hemorrhagic spots by small dimensions (< 1cm) by round or oval
form which appear on skin or mucosae. Ecchymoses :are hemorrhagic dermo-hypodermic spots more than 1cm. Telangiectasies:are small vessels dilatations on the skin or mucosae which appear in
hypovitaminoses B, cirrhosis.

Teguments in childrenecchymoses ecchymoses

Teguments in children

Teguments in childrenImpetigo varicella

Teguments in childrenAtopic dermatitis Atopic dermatitis

Reticular livedoPeriarteritis nodosa Periarteritis nodosa

Teguments in childrenFungic affection Contact dermatitis

Teguments in childrenCoxachie disease Urticaria

Teguments in childrenScarlet fever Roseola

Examination of hair: Hypotrichosis represents hair rarefying (hypothyroidism, Addison disease). Calvition is the hair loosing on determined area. Allopecia is the head hair loosing. Hypertrychosis is hair density increasing in cutaneous hairy areas. Hirsutism represents the hypertrychosis on more extended areas Qualitative modifications of hair include the fiber thickness, shining and hair pigmentation.
Examination of nails:
The form, thickness, friablity and their color are examining.
• Bulging – pathologic accentuation of nail convexity appears in the case of hyppocratic fingers and is characterized by last phalange soft tissues hypertrophy and aspect of the nail like to glass watch. This aspect appears in different broncho-pulmonary diseases (neoplasma, bronchiectasis, pulmonary abscess, empiema, interstitial fibrosis), cardiac diseases (congenital angio-cardiopathies, infectious endocarditis, cardiac failure), digestive diseases (hepatic cirrhosis, intestinal polyposis, ulcero-hemorrhagic rectocolitis), polyglobulias.
• Koilonychia is flattening and concavity of the nail plate with loss of normal contour, producing a spoon-shaped nail. It is observed in iron deficient anemias, mixedema, acromegaly.

Adipose and muscular system:•Adipose tissue is assessed by general inspection and by
measurement of skin fold on abdomen or on arm, appreciating in this way the patient’s nutrition state.
•Muscular system is examining by inspection and palpation, establishing therefore the development and musculature tonus: hypertrophy, hypotrophy, muscular hypertonia, hypotonia or normal aspect.

Facies can offer important data about the presence of some respiratory diseases such as:
vultuos facies– with red cheekbones , shining eyes, on febrile background, which appears in lobar pneumonia (Jaccoud sign - hyperemia on the same part with pneumonia).
pale facies, so-called „venice facies” typical in the past for TBC or in advanced phases - pale-yellowish , hectic, hollow facies with sunken eyes, with dark rings but red cheekbones(„cemetery roses”).
Cyanotic facies – especially of lips, cheekbones and nose top – denotes a severe pulmonary affection (bronchopneumonia, massive pneumonia, pulmonary neoplasma,etc.) or chronic cor pulmonale.
cyanotic-black, „blue-bloatter” facies appears in mediastinal syndrome „pink-puffer” facies typical for emphysematous patients
Examen of teguments and mucosae – reveal described facies modifications in which the labial herpes characteristic in viral pneumonias or in lobar pneumonia is adding.
Don’t forget to examine the inferior members teguments.

Ostheo-articular system:
• Objective examination of bones:
• Fractures are characterized by abnormal mobility of one bone segment and bone crepitation.
• Bone deformations appear as a result of abnormal growing and development of bones, tumoral proliferation or endocrine (acromegaly) or metabolic (rickets, osteomalacia, Paget disease) disorders.
• Obiective examination of articulations:
-Congestion – redish coloring of teguments around articulations appears in the case of arthrites (articular inflammation).
-Tumefaction of periarticular tissues leads to articular deformation, spontaneous pain at movement and limitation of articular mobility.
-Articular pain – sensibility is found at articulations palpation and at active or passive movements effectuated by patient.
-Articular deformations are observing at attent inspection, having significance in arthrites or în arthroses (degenerative articular processes with chronic character).
-Articular mobility is evidencing at active or passive movements of articulations, articular diseases determining the reducing or disappearance of one articulation mobility both from pains cause, and from articular ankylosis or semiankylosis cause

Locomotor system
•Locomotor system has three major components :
• - bones•- articulations•- muscles and their nerves.

Skeleton and its functions
• gives the form and support to the body• represents the storage of easy mobilizing
calcium (97%)•Some elements of skeleton protect the
body from external and internal forces.•The bones offer the attaching surfaces for
muscles and represents the movement levers.
•The dynamic agent of locomotion is represented by skeletal muscle.

The major symptoms of locomotor system affection•· pain•· functional incapability

Pain
•biting• smarting•burning• spearing• excruciating •pulsative•It can be continuous or intermittent,
progressive or alternant in evolution, localized or diffuse, expressed or dull, superficial or profound.

Spatial characteristics • ! Number of affected articulations: • • monoarthritis (infectious arthritis); • • oligoarthritis (reactive arthritis = ReA); • • polyarthritis (rheumatoid polyarthritis = RPA); • ! symmetry (RPA)/asymmetry (ReA); • ! articular/periarticular feeling; • ! distal irradiation: syndromes of nervous compression• (syndrome of tunnel/compartment); • ! referred pain: for example, the affection of hip
can • generate the pain in knees (especially in
children).

Temporal characteristics
• Duration of arthralgies: • if occurs long time: continuous, recurrent, • periods of activity and periods of complete remission• if occurs many years # to exclude an acute infectious or • malignant process. • chronic infection (fungic, tuberculosis) can• persist a lot of years• persists in one articulation or passes from one• articulation to another: migratory polyarthritis (one
articulation affection # improvement # other articulation
• affection): leukemia, gonococcic arthritis, • sarcoidosis, juvenile rheumatoid arthritis; • time: day moment when the pain begins to intensify;

Inflammatory pain• Often is accentuated in morning• it is ameliorating after periods of articulation
repose if the articulation is used (RPA, SA);• it can intensify if the articulation is
overworked or even only at moderated movements (also as in arthrosis);
• When the pain is severe, the patient can wake up
• PAR (and tendency) can produce early awake, especially when the patient stands on affected
• member; • Sudden pain onset in one articulation

Antecedents
• recent history of pharyngitis/angina (throat pain),
•Followed after 10-14 days by articular pains # suspicion of AAR;
• • tbc, syphilis, hemophilia (hemarthrosis), renal colics (uric lithiasis associated to gout), cutaneous streptococcal, staphylococcal infections

Other signs/symptoms
Other signs/symptoms: local: objective articular (signs of inflammation: swelling, local warmth, redness at palpation, spontaneous pain and functional impotence) or periarticular modifications;
•general/systemic # system disease: •general: fever, astenia, loss of appetite; •Multiorganic affection: cardiac, pulmonary,
digestive, renal.

Articular examination• Enlargement in volume of articulation, liquid
accumulation, pain, flat contour of articulation, bulging of sinovial sack bottom, with/without signs of inflammation(redness, warmth).
• At palpation fluctuation, pain. The knees: rotulian shock, wave sign.
• Differential diagnostic: inflammation of periarticular tissue, deformation of articulation through repeated
• traumatisms can be differentiated using echography

Member deformation
vicious positions due to bones, articular, periarticular changes: knees (varus, valgus), hip (varus, valgus), foot (plate, hollow, equine), halux valgus, vertebral column (scoliosis, kyphosis, lordosis)
Articular deformations: nodules Heberden, Bouchard, neuropathic articulation (Charcot)

Mobility increasing
•Can be congenital (conjunctive tissue anomalies:
•Ehlers-Danlos syndrome) or acquired (ruptures of
• ligaments, muscular hypotonia in neuropathies.

Mobility decreasing
•Mobility examination must be performed with attention in the case of traumatism, hemophilia.
•Identifying of affected articulations is carried out in function of difficult performing movements: combing, putting on shoes, buttoning.

Partial mobility decreasing
• Reversible• • acute = (impossibility of• Active or passive articulation mobilization): traumatisms,
inflammations, • Inclusively by infectious case• • chronic = stiffness: movement limitation often due to• Inflammatory, reversible, intra- and periarticular
processes. • Can vary in function of day moment. • Improvement as the articulation is used; accentuation after • A period of articulation rest, especially in morning. • Irreversible = semiankylosis:• Movements limitation often after irreversible, intra- and
periarticular fibrosing processes, deformant cicatrix of articular capsula: modifications are not by inflammatory type, but destructive and cicatrizing, irreversible;

Mobility loosing
• Reversible = articular block: temporary fixing of articulation in certain position and which can’t bereducing actively or passively; can be antalgic, due to muscular contracture, mechanical irritation due to some intraarticular free body (fragment of cartilage, for example broken meniscus), functional due to sinovial inflammation (rarely until block, de regulă remains at the level of stiffness);
• Irreversible = ankylosis: anatomic or therapeuticirreversible process; after tbc arthritis, SA

Articular cracking
•friction of articular rugged cartilages surfaces.
•Not confound with physiologic cracks (sliding of ligaments/tendons over bone surfaces).
•Other causes: shoulder luxation, shifting of biceps tendon from bicipital groove, lesions of meniscus (knee), dysfunction of temporomandibular articulation.

Laboratory examinations
• General • inflammatory: inflammatory syndrome (ESR,
fibrinogen, α2-globulins, C-reactive protein) • noninfectious/systemic: • systemic lupus erythematosus : complement, lupic
cells, • circulant immune complexes, specific antibodies; • Rheumatoid polyarthritis: rheumatoid factor; • acute polyarticular rheumatism: ASLO; • infectious/local: leucocytosis, leucocytary formula • (neutrophilia) > SLE (leucopenia) • degenerative: not modified

Special: articular liquid examination
• Articular puncture. • Normal aspect. • Viscosity increases with hialuronic acid
concentration• Or with leucocytes count.
• Macroscopic aspect: • • transparent, viscous, not coagulable, cells < 10/µL • degenerative artropathies ; • • turbid # inflammatory process (many cells or
many fibrin);

Special: articular liquid examination•Cellularity: • • <200/µL normal • • 200-2.000/µL not inflammatory • • 2.000-20.000(75.000)/µL inflammatory • • >20.000/µL septic (infectious arthrites) • ~30 000/µL specific infectious arthritis(tbc):
turbid or even purulent liquid, lymphocytes predominate
• >100.000/µL nonspecific infectious arthritis: yellow-
•Greenish liquid, turbid (purulent), neutrophils predominate; in culture the germ is identifying.

General principles of examination• asymmetry: nodules, atrophy, tumoral masses,
deformations. • signs of inflammation: swelling, local warmth (using
the • back part of palm for to compare one part with• another), redness, sensibility to palpation. • palpation: zones of sensibility or bone discontinuity. • Articular cracking – the articular cartilages surface is rugged. • amplitude of articular movements (inflammed
articulations can be painful and must be moved with kindness). • Isolated (individual muscles) and integrated
(muscular groups) muscular function and gait refer to neurologic examination.
• Assessment of neck, superior and inferior members musculature force.

Functional impotence•Causes are multiple: • interruption of osseous continuity or of
musculo-tendinous formations which execute the movement,
•blockage, •stiffness or articular ankyloses, •antalgic reaction as a consequence of
traumatism or some painful affection, •Lesions of rahidian nerves or• lesions of central nervous system etc.

Muscular pain (myalgia)• In inferior member at gait- peripheral ischemia
(pain of ischemic musculature). • Associated with weakness- suspicion of
primary muscular affection. • Spontaneous muscular pain - systemic
inflammatory states: generalized myalgias; • infections: • • viral (acute febrile diseases) • • bacterial: streptococcus, staphylococcus, gonococcus, • secondary or tertiar lues; • muscular phlegmon: swelling, pain, sometimes
supuration; • overloading (after intense efforts for which the• respective individual has not training)

Muscular hypotony
• syndrome of neuro-muscular pathology; •pyramidal syndrome in acute stage; •lesions of posterior roots and posterior cords
(tabes); •cerebellum affection syndrome; •periodic familial paralysis.

Muscular hypertony
• antalgic contracture (of spinal muscles in acute lumbago • or in lumboischiasis, of abdominal musculature in • peritonitis, neck stiffness in meningeal syndrome); • neurologic lesions. • • spasticity or pyramidal contracture in • pyramidal syndrome: • In the trial of flexion/extension of member, there is a
big resistance, then, this resistance being surpassed, the movement is easy realizing (like to pocket knife closing).
• • rigidity or extrapyramidal contracture (contracture is surpassed gradually with sensation of toothed wheal or led tube)

Muscular atrophy• Amyotrophy - flattening of normal muscular relief,
often substituted by depressions, the bone relief having contrast prominence.
• Causes: • • inactivity (immobilization in gyps or after
some• Osteoarticular lesion: ankylosis). • • myogene (protopathic) by primarily muscular cause • primitive myopathies: progressive muscular
dystrophies (PMD). • Initially more genetically different subtypes
were described. • predominant localization of amyotrophies: • pelvifemoral (Duchenne, Becker), pelviscapular, • pelviscapulofacial (congenital PMD, myotonic PMD),
facioscapulohumeral, oculopharingeal, distal.

Bone pain
• Profound, piercing, dull or intense. • In rest with nocturnal accentuation # the patient • can’t sleep: acute infections: acute ostheomyelitis (AOM); • permanent with progressive accentuation or in very intense during
short time accesses (malignant bone tumors); connected with movement:
• fractures – sharp pain, preceded by traumatism; • sometimes in chronic infections: chronic ostheomyelitis (COM),
TBC. • Infectious causes: • Non-specific (AOM, COM); • • AOM – intense sensibility to touching; is intensifying as the
infection• persists), inflammatory edema (hard), redness, increased local
temperature, functional impotence: does not move respective member due to pain
• the movement amplifies the pain). Nocturnal aggravation, due to congestion.
• • chronic ostheomyelitis (COM).

Bone deformations• Ostheoporosis, ostheomalacia, rickets, Paget disease,
syphilis • tertiary syphilis: ostheoperiostitis and gome
ostheomyelitis • = ostheoperiostitis affecting long and flat bones,
with evolution to necrosis and ulceration # the formations contain necrosis material by gum consistence (gome), which are opening on the skin surface # ulcerations.
• congenital tardive syphilis: In children from mothers with syphilis (especially recent, active, in the first year of infection) - intrauterine, transplacentar infection. Manifestations equivalent to tertiary
• syphilis: plastic ostheoperiostitis (tibia in yataghan) • and gomous ostheomyelitis (nose in the form of
saddle or opera glasses).

Formations in bones• Traumatic causes: callus after fracture, vicious callus: • discrepancy, angling, torsion of both bone fragments, nervous,
vascular compressions. • Infectious causes: • AOM: signs of inflammation: • Very painful swelling, erythema, local warmth; sometimes local
regional adenopathy• COM; • Tumoral causes: • benign bone tumors, bone cysts: well delimited, painless, adhere
to bone, not adhere to superficial planes, no ulcer, when are very voluminous.
• malignant bone tumors: infiltrative formation, adherence to profound plane, but in soft parts; variable consistence, sometimes ulcerations; parchment-like crepitation (like to egg shell breaking); local circulation is increased (tissular turn-over more accelerated as in normal bone), with increased local temperature and evident venous network; sarcomas give metastasis especially on sanguine pathway # usually there is not adenopathy;
• multiple bone tumors: multiple myeloma (at the level of calotte) adherent to profound plane,
• mobile relatively to teguments, hard or pseudofluctuant (can be confound with sebaceous cysts).