
Extended-spectrum β-lactamase-producing Klebsiella pneumoniae in the neonatal intensive care unit:...
6
Major article Extended-spectrum b-lactamase-producing Klebsiella pneumoniae in the neonatal intensive care unit: Does vancomycin play a role? Ali M. Somily MBChB a , Sarah S. Alsubaie MBBS b , Abdulaziz A. BinSaeed PhD c, *, Armen A. Torchyan MPH c , Fahad A. Alzamil MBBS b , AbdulKarim I. Al-Aska MBBS d , Fatimah S. Al-Khattaf MBBS e , Lyla A. Khalifa MBBS e , Sahar I. Al-Thawadi MD f , Alwaleed A. Alaidan PhD f , Mohammed N. Al-Ahdal PhD f , Ahmed A. Al-Qahtani PhD f , Thomas S. Murray PhD g a Department of Pathology, College of Medicine, King Saud University, Riyadh, Saudi Arabia b Department of Pediatrics, College of Medicine, King Saud University, Riyadh, Saudi Arabia c Department of Family and Community Medicine, College of Medicine, King Saud University, Riyadh, Saudi Arabia d Department of Medicine, College of Medicine, King Saud University, Riyadh, Saudi Arabia e Department of Infection Control, College of Medicine, King Saud University, Riyadh, Saudi Arabia f Department of Infection and Immunity, Research Center, King Faisal Specialist Hospital and Research Center, Riyadh, Saudi Arabia g Department of Laboratory Medicine, Yale University School of Medicine, New Haven, CT Key Words: Antibiotics Colonization Infection Outbreak Saudi Arabia Background: Extended-spectrum b-lactamase (ESBL)-producing Klebsiella species cause worldwide problems in neonatal intensive care units (NICUs). This study aimed to determine possible risk factors for infection or colonization with ESBL-producing Klebsiella pneumoniae (ESBLKp) during an outbreak in the NICU. Methods: A retrospective cohort study was conducted among neonates admitted to the NICU of a teaching hospital in Riyadh, Saudi Arabia, during an outbreak of ESBLKp from April to July 2008. The incidence density ratio was calculated to determine possible predictors of ESBLKp colonization or infection. Results: During 2,265 person-days of follow-up of 118 neonates, 4 became infected, and 8 were colonized with ESBLKp. Univariate analyzes revealed that, among 14 neonates who were treated with vancomycin, 9 (64.3%) developed infection or colonization with ESBLKp, whereas, among 104 neonates who were not treated with vancomycin, 3 (2.9%) were affected, with an incidence density ratio of 4.22 (95% confidence interval: 1.47-5.15). Parenteral feeding and mechanical ventilation were found to be marginally signifi- cant risk factors. Conclusion: Treatment with vancomycin appears to be a risk factor for infection or colonization with ESBLKp in the NICU setting. Copyright Ó 2014 by the Association for Professionals in Infection Control and Epidemiology, Inc. Published by Elsevier Inc. All rights reserved. Hospital-acquired infections by multidrug-resistant organisms are important causes of patient morbidity and mortality and cost health care systems between $4.5 and $5.7 billion annually in the United States. 1,2 A common mechanism for antibiotic resistance used by multiple organisms is the secretion of extended-spectrum b-lactamase (ESBL) enzymes that hydrolyze the amide bond of the b-lactam ring, inactivating antibiotics such as penicillins and cephalosporins. Some of these enzymes also are capable of hy- drolyzing carbapenems, and therapeutic options to eradicate these strains are limited. 3,4 Klebsiella pneumoniae is a gram-negative pathogen that can be responsible for outbreaks of nosocomial infections. ESBLs are het- erogeneous (temoniera [TEM], sulfhydryl-variable [SHV], and others), and Klebsiella strains may carry multiple ESBLs. 5 Outbreaks may also be due to either the emergence of a clonal strain or the multiple strains circulating in a hospital. 6-9 The dynamic evolution of ESBLs requires tedious efforts to keep the medical community updated with the characterization and epidemiology of these or- ganisms. This makes identification and treatment in the outbreak setting challenging for both microbiologists and clinicians. * Address correspondence to Abdulaziz A. BinSaeed, MBBS, DFE, PhD, Depart- ment of Family & Community Medicine (34), College of Medicine, King Saud Uni- versity, PO Box 2925, Riyadh 11461, Saudi Arabia. E-mail address: [email protected] (A.A. BinSaeed). Conflicts of interest: None to report. Contents lists available at ScienceDirect American Journal of Infection Control journal homepage: www.ajicjournal.org American Journal of Infection Control 0196-6553/$36.00 - Copyright Ó 2014 by the Association for Professionals in Infection Control and Epidemiology, Inc. Published by Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.ajic.2013.09.028 American Journal of Infection Control 42 (2014) 277-82
Transcript of Extended-spectrum β-lactamase-producing Klebsiella pneumoniae in the neonatal intensive care unit:...

lable at ScienceDirect
American Journal of Infection Control 42 (2014) 277-82
Contents lists avai
American Journal of Infection Control
journal homepage: www.aj ic journal .org
American Journal of Infection Control
Major article
Extended-spectrum b-lactamase-producing Klebsiella pneumoniaein the neonatal intensive care unit: Does vancomycin play a role?
Ali M. Somily MBChB a, Sarah S. Alsubaie MBBS b, Abdulaziz A. BinSaeed PhD c,*,Armen A. Torchyan MPH c, Fahad A. Alzamil MBBS b, AbdulKarim I. Al-Aska MBBS d,Fatimah S. Al-Khattaf MBBS e, Lyla A. Khalifa MBBS e, Sahar I. Al-Thawadi MD f,Alwaleed A. Alaidan PhD f, Mohammed N. Al-Ahdal PhD f, Ahmed A. Al-Qahtani PhD f,Thomas S. Murray PhD g
aDepartment of Pathology, College of Medicine, King Saud University, Riyadh, Saudi ArabiabDepartment of Pediatrics, College of Medicine, King Saud University, Riyadh, Saudi ArabiacDepartment of Family and Community Medicine, College of Medicine, King Saud University, Riyadh, Saudi ArabiadDepartment of Medicine, College of Medicine, King Saud University, Riyadh, Saudi ArabiaeDepartment of Infection Control, College of Medicine, King Saud University, Riyadh, Saudi ArabiafDepartment of Infection and Immunity, Research Center, King Faisal Specialist Hospital and Research Center, Riyadh, Saudi ArabiagDepartment of Laboratory Medicine, Yale University School of Medicine, New Haven, CT
Key Words:AntibioticsColonizationInfectionOutbreakSaudi Arabia
* Address correspondence to Abdulaziz A. BinSaement of Family & Community Medicine (34), Collegeversity, PO Box 2925, Riyadh 11461, Saudi Arabia.
E-mail address: [email protected] (A.A. BinSaeeConflicts of interest: None to report.
0196-6553/$36.00 - Copyright � 2014 by the Associahttp://dx.doi.org/10.1016/j.ajic.2013.09.028
Background: Extended-spectrum b-lactamase (ESBL)-producing Klebsiella species cause worldwideproblems in neonatal intensive care units (NICUs). This study aimed to determine possible risk factors forinfection or colonization with ESBL-producing Klebsiella pneumoniae (ESBLKp) during an outbreak in theNICU.Methods: A retrospective cohort study was conducted among neonates admitted to the NICU of a teachinghospital in Riyadh, Saudi Arabia, during an outbreak of ESBLKp from April to July 2008. The incidencedensity ratio was calculated to determine possible predictors of ESBLKp colonization or infection.Results: During 2,265 person-days of follow-up of 118 neonates, 4 became infected, and 8 were colonizedwith ESBLKp. Univariate analyzes revealed that, among 14 neonates who were treated with vancomycin,9 (64.3%) developed infection or colonization with ESBLKp, whereas, among 104 neonates who were nottreated with vancomycin, 3 (2.9%) were affected, with an incidence density ratio of 4.22 (95% confidenceinterval: 1.47-5.15). Parenteral feeding and mechanical ventilation were found to be marginally signifi-cant risk factors.Conclusion: Treatment with vancomycin appears to be a risk factor for infection or colonization withESBLKp in the NICU setting.
Copyright � 2014 by the Association for Professionals in Infection Control and Epidemiology, Inc.Published by Elsevier Inc. All rights reserved.
Hospital-acquired infections by multidrug-resistant organismsare important causes of patient morbidity and mortality and costhealth care systems between $4.5 and $5.7 billion annually in theUnited States.1,2 A common mechanism for antibiotic resistanceused by multiple organisms is the secretion of extended-spectrumb-lactamase (ESBL) enzymes that hydrolyze the amide bond ofthe b-lactam ring, inactivating antibiotics such as penicillins and
ed, MBBS, DFE, PhD, Depart-of Medicine, King Saud Uni-
d).
tion for Professionals in Infection C
cephalosporins. Some of these enzymes also are capable of hy-drolyzing carbapenems, and therapeutic options to eradicate thesestrains are limited.3,4
Klebsiella pneumoniae is a gram-negative pathogen that can beresponsible for outbreaks of nosocomial infections. ESBLs are het-erogeneous (temoniera [TEM], sulfhydryl-variable [SHV], andothers), and Klebsiella strains may carry multiple ESBLs.5 Outbreaksmay also be due to either the emergence of a clonal strain or themultiple strains circulating in a hospital.6-9 The dynamic evolutionof ESBLs requires tedious efforts to keep the medical communityupdated with the characterization and epidemiology of these or-ganisms. This makes identification and treatment in the outbreaksetting challenging for both microbiologists and clinicians.
ontrol and Epidemiology, Inc. Published by Elsevier Inc. All rights reserved.
ROOM 1FeederGrower Room
ROOM4Isolation
ROOM 6
Isolation
ROOM 7
Nursing Station
CoffeeRoom
Doctors Room
Hand washing and gowns room
ROOM 2
ROOM 5
ROOM 3
Water sink
Water sink
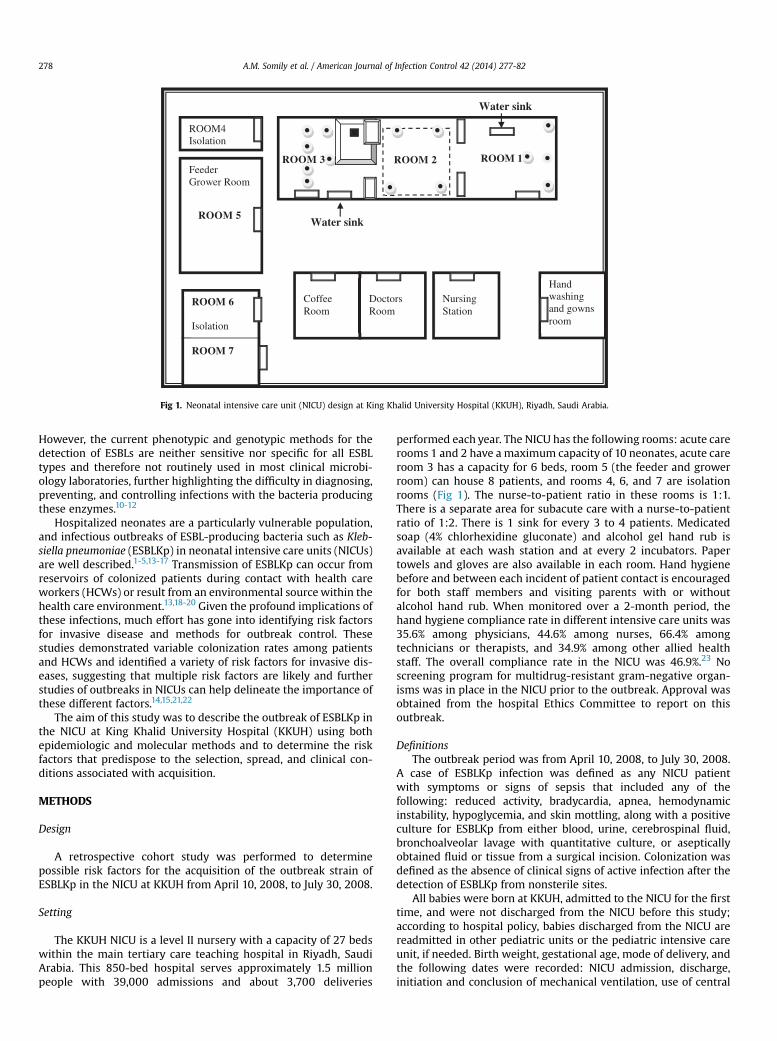
Fig 1. Neonatal intensive care unit (NICU) design at King Khalid University Hospital (KKUH), Riyadh, Saudi Arabia.
A.M. Somily et al. / American Journal of Infection Control 42 (2014) 277-82278
However, the current phenotypic and genotypic methods for thedetection of ESBLs are neither sensitive nor specific for all ESBLtypes and therefore not routinely used in most clinical microbi-ology laboratories, further highlighting the difficulty in diagnosing,preventing, and controlling infections with the bacteria producingthese enzymes.10-12
Hospitalized neonates are a particularly vulnerable population,and infectious outbreaks of ESBL-producing bacteria such as Kleb-siella pneumoniae (ESBLKp) in neonatal intensive care units (NICUs)are well described.1-5,13-17 Transmission of ESBLKp can occur fromreservoirs of colonized patients during contact with health careworkers (HCWs) or result from an environmental sourcewithin thehealth care environment.13,18-20 Given the profound implications ofthese infections, much effort has gone into identifying risk factorsfor invasive disease and methods for outbreak control. Thesestudies demonstrated variable colonization rates among patientsand HCWs and identified a variety of risk factors for invasive dis-eases, suggesting that multiple risk factors are likely and furtherstudies of outbreaks in NICUs can help delineate the importance ofthese different factors.14,15,21,22
The aim of this study was to describe the outbreak of ESBLKp inthe NICU at King Khalid University Hospital (KKUH) using bothepidemiologic and molecular methods and to determine the riskfactors that predispose to the selection, spread, and clinical con-ditions associated with acquisition.
METHODS
Design
A retrospective cohort study was performed to determinepossible risk factors for the acquisition of the outbreak strain ofESBLKp in the NICU at KKUH from April 10, 2008, to July 30, 2008.
Setting
The KKUH NICU is a level II nursery with a capacity of 27 bedswithin the main tertiary care teaching hospital in Riyadh, SaudiArabia. This 850-bed hospital serves approximately 1.5 millionpeople with 39,000 admissions and about 3,700 deliveries
performed each year. The NICU has the following rooms: acute carerooms 1 and 2 have a maximum capacity of 10 neonates, acute careroom 3 has a capacity for 6 beds, room 5 (the feeder and growerroom) can house 8 patients, and rooms 4, 6, and 7 are isolationrooms (Fig 1). The nurse-to-patient ratio in these rooms is 1:1.There is a separate area for subacute care with a nurse-to-patientratio of 1:2. There is 1 sink for every 3 to 4 patients. Medicatedsoap (4% chlorhexidine gluconate) and alcohol gel hand rub isavailable at each wash station and at every 2 incubators. Papertowels and gloves are also available in each room. Hand hygienebefore and between each incident of patient contact is encouragedfor both staff members and visiting parents with or withoutalcohol hand rub. When monitored over a 2-month period, thehand hygiene compliance rate in different intensive care units was35.6% among physicians, 44.6% among nurses, 66.4% amongtechnicians or therapists, and 34.9% among other allied healthstaff. The overall compliance rate in the NICU was 46.9%.23 Noscreening program for multidrug-resistant gram-negative organ-isms was in place in the NICU prior to the outbreak. Approval wasobtained from the hospital Ethics Committee to report on thisoutbreak.
DefinitionsThe outbreak period was from April 10, 2008, to July 30, 2008.
A case of ESBLKp infection was defined as any NICU patientwith symptoms or signs of sepsis that included any of thefollowing: reduced activity, bradycardia, apnea, hemodynamicinstability, hypoglycemia, and skin mottling, along with a positiveculture for ESBLKp from either blood, urine, cerebrospinal fluid,bronchoalveolar lavage with quantitative culture, or asepticallyobtained fluid or tissue from a surgical incision. Colonization wasdefined as the absence of clinical signs of active infection after thedetection of ESBLKp from nonsterile sites.
All babies were born at KKUH, admitted to the NICU for the firsttime, and were not discharged from the NICU before this study;according to hospital policy, babies discharged from the NICU arereadmitted in other pediatric units or the pediatric intensive careunit, if needed. Birth weight, gestational age, mode of delivery, andthe following dates were recorded: NICU admission, discharge,initiation and conclusion of mechanical ventilation, use of central

A.M. Somily et al. / American Journal of Infection Control 42 (2014) 277-82 279
vascular catheter, parenteral nutrition, signs and symptoms ofsepsis, microbiologic data, and antimicrobial use.
Our study included neonates who were admitted to the NICUduring the study period, stayed at least 24 hours, and had sur-veillance results (swabs of the nose, throat, axilla, groin, feces,or rectum), with a minimum of 1 sample on admission and at least1 sample per week of hospitalization. For incidence data, weincluded all babies with a positive culture for ESBLKp regardless ofwhether the baby had infection or colonization.
Surveillance cultures of infants, environment, and HCWsSurveillance cultures (swabs of the nose, throat, axilla, groin,
feces, or rectum) were obtained from neonates on admission andthen repeated if there was new exposure until discharge. Rectalswab or stool cultures were performed at least once a week, duringthe period of the outbreak. Hand screening of HCWs for the pres-ence of ESBLKp was performed on June 30, 2008, including allnurses and staff involved in patient management or milk formulapreparation. Environmental cultures were performed using pre-moistened swabs on respiratory therapy equipment, sinks, tapwater, diaper scales, and feeding formula. Because of the ongoingtransmission of ESBLKp, despite establishing a count of infected orcolonized infants, all HCWs who had direct contact with infants inthe main NICU were inspected for artificial nails and dermatitis.
Microbiology and strain typingBlood was inoculated into a BacT/ALERT pediatric bottle and
incubated in the BacT/ALERT automated system for 7 days (OrganonTeknica, Scarborough, Ontario, Canada). Rectal swab specimens orfeces (from all newborns in the NICU) were inoculated on Mac-Conkey agar (MAC) plates and incubated at 35�C for 24 to 48 hours.For environmental surveillance, sterile swabs (premoistened withsterile saline) were rubbed over the site of interest and then inocu-lated into nutrient broth and on MAC plates, then incubated at 35�Cfor 24 to 48 hours. After 24 hours, aliquots of the nutrient brothcultures were plated on MAC plates and incubated again at 35�C for24 to 48 hours. Both clinical and environmental samples were pro-cessed as routine clinical samples.
Milk formula preparations were sampled in aliquots of 0.1, 1.0,and 10 mL from each bottle and were inoculated into 15 tubes con-taining lactose (1% final concentration) broth and Durham tubes in afinal dilution of 1:50, 1:5, or 1:1, respectively. The cultures were incu-bated at 35�C for 24 to 48 hours and subcultured on MAC agar plates.
All suspected colonies, includingmucoid lactose fermenters thatgrew onMAC agar, were confirmed to be ESBLKp using a MicroScancard (MicroScan Walk Away-96; Siemens Healthcare Diagnostics,Deerfield, IL), and susceptibility testing was performed by the disk-diffusion method, according to Clinical and Laboratory StandardsInstitute (CLSI) guidelines. ESBL confirmation was obtained by thedouble-disk method and the E-test (bioMérieux, Marcy l’Etoile,France).17
Pulsed-field gel-electrophoresis (PFGE) method: Bacterial strainsPFGE of K pneumoniae was performed by a previously reported
method.24 DNA was digested with Xbal at 37�C for a minimum of 4hours. The digested DNA was electrophoresed in 1% agarose gel(Sigma, St Louis, MO) using TBE buffer in a CHEF-DR II cell (Bio-RadLaboratories, Hercules, CA) for 21 hours at 200 V with switchingtimes ramped from 1 to 20 seconds. The gels were stained withethidium bromide and photographed under ultraviolet illumina-tion. Lambda DNA concatemers (New England BioLabs, Ipswich,MA) were used as molecular weight markers.
The relatedness of K pneumoniae isolates and macrorestrictionprofiles were analyzed as described by Tenover et al.25 If the bacterialprofiles differed from each other by up to 3 bands, they were
considered closely related; if they differed by 4 to 6 bands, they wereconsidered possibly related; and, if they differed by 7 bands or more,they were considered to be different strains.
Infection control measuresIn addition to surveillance cultures, multiple infection control
strategies were implemented to control the outbreak. Carbape-nems were the first-line agents for the therapy of neonates withlate-onset sepsis. Third-generation cephalosporins were used onlyfor the treatment of microbiologically confirmed Pseudomonasaeruginosa infections susceptible to this agent. Enhanced cleaningof the unit, including sinks and faucets, was performed daily.
Three cohorts of infants were established in May. All babiesinfected or colonized with ESBLKp were placed on contact pre-caution until hospital discharge in rooms 1 and 2. A group ofdesignated nurses cared for these infants. The second cohort ofinfants, who were exposed to the case-infants, but had negativesurveillance cultures, was cared for in the feeder and grower roomby another group of designated nurses. The third cohort consistedof newly admitted babies, who were placed in room 3, away fromthe ESBLKp-positive and exposed babies. Another group of desig-nated nurses took care of them. Separate physician teams weremaintained for the first and third cohorts. Rooms were separatedphysically by partitions, and dedicated patient care supplies wereused for infected/colonized infants.
A twice-weekly meeting was held with the NICU staff to discussthe ongoing investigation and control measures. The importance ofhand hygiene with 4% chlorhexidine gluconate was emphasized atthe staff meetings.
Statistical analysisThe data were entered and analyzed through the IBM SPSS
Statistics for Windows, version 20.0 (IBM Corp, Armonk, NY). Inunivariate analysis, the incidence density ratio (IDR) was calculatedto determine the possible predictors of ESBLKp colonization orinfection. The time to ESBLKp colonization or infection was calcu-lated from the date of NICU admission. Infants without ESBLKpwere censored at the time of their discharge.
RESULTS
During the study period, a total of 118 neonates was admittedto the NICU. All of the admitted babies were confirmed to be eligibleand were included in the study. The study population, including24 (20.3%) neonates whose birth weight was less than 1,500 grams,70 (59.3%) neonates whose gestational age was less than 37 weeks,70 (59.3%) delivered via cesarean section, and 27 (22.9%) mechan-ically ventilated (Table 1), were all born in the same hospital andmoved to the NICU. During the 2,265 person-days of follow up,4 (3.4%) neonates became infected (1 bloodstream infection and3 lung infections diagnosed by tracheal aspirate), and 8 (6.8%) werecolonized with ESBLKp. The incidence density of infection orcolonization with ESBLKp was 5.3 per 1,000 patient-days. Themedian duration of NICU stay until ESBLKp infection or coloniza-tion was 37.5 (range, 6-93) days.
Univariate analyses revealed that, among 14 neonates whoweretreated with vancomycin, 9 (64.3%) developed infection or coloni-zation with ESBLKp, whereas, among 104 neonates who werenot treated with vancomycin, 3 (2.9%) were affected, with an IDR of4.22 (95% confidence interval [CI]: 1.47-5.15).
Parenteral feeding and mechanical ventilation were found tobe marginally significant risk factors for ESBLKp infection or colo-nization. During the study, about 31.3% of neonates who wereprovided with parenteral feeding had ESBLKp infection or coloni-zation, in comparison with 2.5% neonates who were not (IDR, 3.22;

Table 1Characteristics of patients at the time of admission and univariate analysis for risk factors for infection or colonization with extended-spectrum b-lactamase-producingKlebsiella pneumoniae
Variables Number of neonates Infected neonates Colonized neonates Person-days IDR (95% CI)
SexFemale 54 4 5 1,353 2.02 (0.55-7.47)Male 64 0 3 912 Reference
NationalitySaudi 107 4 8 2,177 1.00Other 11 0 0 88 Reference
Birth weight<1,500 g 24 2 5 1,042 1.62 (0.52-5.11)*�1,500 g 93 2 3 1,208 ReferenceN/A 1 0 0 15
Gestational age<37 weeks 70 4 8 1,925 1.00�37 weeks 48 0 0 340 Reference
Mode of deliveryC-section 70 2 7 1,371 1.91 (0.52-7.06)Vaginal 45 2 1 873 Reference
Decreased activityYes 22 3 1 716 1.18 (0.34-4.02)y
No 94 1 6 1,474 ReferenceN/A 2 0 1 75
Bradycardiaz
Yes 21 2 3 657 1.75 (0.55-5.51)No 97 2 5 1,608 Reference
ApneaYes 20 0 1 314 0.56 (0.07-4.38)No 98 4 7 1,951 Reference
Poor feedingYes 88 2 8 1,711 1.62 (0.35-7.39)No 30 2 0 554 Reference
Mechanical ventilationYes 27 4 5 1,191 2.69 (0.73-9.95)y
No 90 0 3 1,069 ReferenceN/A 1 0 0 5
Parenteral nutritionYes 32 4 6 1,331 3.22 (0.70-14.68)y
No 80 0 2 856 ReferenceN/A 6 0 0 78
Ampicillin þ gentamicinYes 58 0 5 1,132 0.71 (0.23-2.25)No 60 4 3 1,133 Reference
CefotaximeYes 6 1 2 330 1.95 (0.53-7.22)No 112 3 6 1,935 Reference
VancomycinYes 14 3 6 941 4.22 (1.14-15.59)No 104 1 2 1,324 Reference
bpm, beats per minute; C-section, cesarean section.*<1,500-g and �1,500-g categories were included in the analysis.yYes and no categories were included in the analysis.zFor term infants (37-42weeks gestational age):<80 bpm for>10 seconds, or a shorter episode if associatedwith color change, or<50 bpm for any length of time. For preterminfants: <90 bpm for >10 seconds or shorter if associated with color change or <50 bpm for any length of time.
A.M. Somily et al. / American Journal of Infection Control 42 (2014) 277-82280
95% CI: 0.70-14.68). Mechanical ventilation was also associatedwith increased risk of ESBLKp infection or colonization (33.3% vs3.3%, respectively), which increased 2.69 times per NICU-day (IDR,2.69; 95% CI: 0.73-9.95). Although not statistically significant, girlshad a 2.02-fold higher risk of ESBLKp infection or colonization perNICU-day (IDR, 2.02; 95% CI: 0.55-7.47) than boys.
There was no significant association (P > .05) between othervariables such as nationality, gestational age, mode of delivery,prescription of ampicillin or cefotaxime, having bradycardia,decreased activity, apnea, or poor feeding, and ESBLKp infection orcolonization. None of the environmental or HCW cultures werepositive for the outbreak strain.
DISCUSSION
Colonization or infection by ESBL-producing gram-negativebacteria, particularly K pneumoniae, have become common, and
outbreaks have been described frequently in neonatal, pediatric,and adult intensive care units.26,27 The gastrointestinal tract ofhospitalized patients can serve as an important reservoir forESBLKp. Patient-to-patient transmission can occur via hand car-riage by HCWs.28
The clustering of cases in April to June 2008 (Fig 2) comparedwith the baseline incidence of cases led us to hypothesize the ex-istence of an ongoing outbreak and to conduct an investigation ofcolonization and infection with this pathogen. PFGE of 5 initialisolates of ESBLKp provided evidence that 1 strain was responsiblefor both infection and colonization during the outbreak period.
In our study, we used univariate analysis and demonstrated thattreatment with vancomycin, parenteral nutrition, and mechanicalventilationwere significant risk factors for infection or colonizationwith ESBLKp in the NICUpopulation. In our hospital, the indicationsfor vancomycin use were late-onset sepsis because of methicillin-resistant staphylococci, such as Staphylococcus epidermidis or

Fig 2. Distribution of cases of extended-spectrum b-lactamase-producing Klebsiella infection and colonization.
A.M. Somily et al. / American Journal of Infection Control 42 (2014) 277-82 281
Staphylococcus aureus (MRSA), or a suspicion of central line-associated bloodstream infection as part of empirical therapy un-til culture results were available. Cefotaxime was used empiricallyto provide coverage for gram-negative species in late-onset sepsiswith either vancomycin or cloxacillin, whereas ampicillin alongwith gentamicin was used to treat neonates with suspected early-onset sepsis.
All 12 neonates with ESBLKp colonization or infection weretreated with vancomycin because of these indications, but theculture results did not reveal ESBLKp isolates. After completing thetreatment, 8 out of the 12 neonates were found to be colonizedwith ESBLKp, and 4 developed infection.
Grohskopf et al,29 in a study performed in the United States,found that gentamicin, ampicillin, and vancomycin were the mostcommon antimicrobial agents administrated to NICU patients. Theyalso found that the administration of vancomycin was empirical inover 50% of the cases.
Vancomycin exposure can cause relative decolonization of thenormal flora and then subsequent colonization with ESBL strainsthrough horizontal transmission. To our knowledge, the associationbetween vancomycin use and the risk of colonization with ESBLKpis of concern; such an association has been published in 2 studies sofar. Harris et al30 found an association between vancomycin usageand stool carriage of ESBL-producing Escherichia coli and Klebsiellaspp in a study conducted in the adult intensive care units at theUniversity of Maryland Medical Center in Baltimore, Maryland.Ofek-Shlomai et al31 found that treatment with vancomycin, bothfor a full 10-day course and for a short 3-day empirical treatmentcourse, was a statistically significant risk factor for gastrointestinalcolonization with ESBL-producing Klebsiella strains in prematurebabies.
Previous studies in the NICU setting have identified severalother risk factors associated with rectal colonization with ESBLKp.A case control study conducted in the NICU at the UniversitiKebangsaan Malaysia Medical Centre in Kuala Lumpur, Malaysia,identified gestational age, low birth weight, longer hospital stay,early-onset pneumonia, prior antibiotic use, and presence of anindwelling catheter as risk factors for rectal colonizationwith ESBL-producing strains of Klebsiella.14
In a study conducted in Brazil, the combined use of third-generation cephalosporins and aminoglycosides, as well as alonger NICU stay, were considered to be risk factors for ESBL-producing bacteria in the NICU.21 Another NICU study from Italyfound the total length of the stay and the combined use of ampi-cillin and gentamicinwere risk factors.32 Furthermore, colonizationwith ESBLKp can persist and be associated with infection after NICUdischarge.33
In our NICU, babies with gastrointestinal colonization or infec-tion with ESBLKp were isolated and cohorted. The outbreak endedwith the reemphasis of infection control practices and cohorting ofaffected neonates. Other NICU studies have used a variety of in-terventions with varying success rates, including modifyingempirical antibiotic use, active surveillance, and special clearing ofpotential environmental sources.13
Treatment with vancomycin appears to be a risk factor forinfection or colonization with ESBLKp in the NICU setting. To limitthe selective pressure on nosocomial flora and the emergence ofresistant strains, the restricted use of certain antibiotics, such asvancomycin, should be considered. Further exploration of this issuewill help infection preventionists in establishing scientificallybased infection prevention and control measures.
References
1. Stone PW, Larson E, Kawar LN. A systematic audit of economic evidence linkingnosocomial infections and infection control interventions: 1990-2000. Am JInfect Control 2002;30:145-52.
2. Stone PW, Gupta A, Loughrey M, Della-Latta P, Cimiotti J, Larson E, et al.Attributable costs and length of stay of an extended-spectrum b-lactamase-producing Klebsiella pneumoniae outbreak in a neonatal intensive care unit.Infect Control Hosp Epidemiol 2003;24:601-6.
3. Bradford PA. Extended-spectrum b-lactamases in the 21st century: character-ization, epidemiology, and detection of this important resistance threat. ClinMicrobiol Rev 2001;14:933-51.
4. Paterson DL, Bonomo RA. Extended-spectrum b-lactamases: a clinical update.Clin Microbiol Rev 2005;18:657-86.
5. Jacoby GA. Extended-spectrum b-lactamases and other enzymes providingresistance to oxyimino-b-lactams. Infect Dis Clin North Am 1997;11:875-87.
6. Bingen EH, Desjardins P, Arlet G, Bourgeois F, Mariani-Kurkdjian P, Lambert-Zechovsky NY, et al. Molecular epidemiology of plasmid spread amongextended broad-spectrum b-lactamase-producing Klebsiella pneumoniae iso-lates in a pediatric hospital. J Clin Microbiol 1993;31:179-84.
7. Wei ZQ, Chen YG, Yu YS, Lu WX, Li LJ. Nosocomial spread of multi-resistantKlebsiella pneumoniae containing a plasmid encoding multiple b-lactamases.J Med Microbiol 2005;54(Pt 9):885-8.
8. Miranda G, Castro N, Leanos B, Valenzuela A, Garza-Ramos U, Rojas T, et al.Clonal and horizontal dissemination of Klebsiella pneumoniae expressing SHV-5extended-spectrum b-lactamase in a Mexican pediatric hospital. J Clin Micro-biol 2004;42:30-5.
9. Bagattini M, Crivaro V, Di Popolo A, Gentile F, Scarcella A, Triassi M, et al.Molecular epidemiology of extended-spectrum b-lactamase-producing Klebsi-ella pneumoniae in a neonatal intensive care unit. J Antimicrob Chemother2006;57:979-82.
10. Pfaller MA, Segreti J. Overview of the epidemiological profile and laboratorydetection of extended-spectrum b-lactamases. Clin Infect Dis 2006;15:S153-63.
11. Royle J, Halasz S, Eagles G, Gilbert G, Dalton D, Jelfs P, et al. Outbreak ofextended spectrum b-lactamase-producing Klebsiella pneumoniae in a neonatalunit. Arch Dis Child Fetal Neonatal Ed 1999;80:F64-8.
12. Szabo D, Filetoth Z, Szentandrassy J, Nemedi M, Toth E, Jeney C, et al. Molecularepidemiology of a cluster of cases due to Klebsiella pneumoniae producing SHV-5 extended-spectrum b-lactamase in the premature intensive care unit of aHungarian hospital. J Clin Microbiol 1999;37:4167-9.

A.M. Somily et al. / American Journal of Infection Control 42 (2014) 277-82282
13. Gastmeier P, Groneberg K, Weist K, Ruden H. A cluster of nosocomial Klebsiellapneumoniae bloodstream infections in a neonatal intensive care department:identification of transmission and intervention. Am J Infect Control 2003;31:424-30.
14. Boo NY, Ng SF, Lim VK. A case-control study of risk factors associated withrectal colonization of extended-spectrum b-lactamase producing Klebsiella spin newborn infants. J Hosp Infect 2005;61:68-74.
15. Singh N, Patel KM, Leger MM, Short B, Sprague BM, Kalu N, et al. Risk ofresistant infections with Enterobacteriaceae in hospitalized neonates. PediatrInfect Dis J 2002;21:1029-33.
16. Garner JS, Jarvis WR, Emori TG, Horan TC, Hughes JM. CDC definitions fornosocomial infections, 1988. Am J Infect Control 1988;16:128-40.
17. Wikler MA, Clinical and Laboratory Standards Institute. Performance standardsfor antimicrobial susceptibility testing: sixteenth informational supplement.Wayne [PA]: Clinical and Laboratory Standards Institute; 2006.
18. Coovadia YM, Johnson AP, Bhana RH, Hutchinson GR, George RC, Hafferjee IE.Multiresistant Klebsiella pneumoniae in a neonatal nursery: the importance ofmaintenance of infection control policies and procedures in the prevention ofoutbreaks. J Hosp Infect 1992;22:197-205.
19. Gaillot O, Maruejouls C, Abachin E, Lecuru F, Arlet G, Simonet M, et al. Noso-comial outbreak of Klebsiella pneumoniae producing SHV-5 extended-spectrumb-lactamase, originating from a contaminated ultrasonography coupling gel.J Clin Microbiol 1998;36:1357-60.
20. Lalitha MK, Kenneth J, Jana AK, Jesudason MV, Kuruvilla KA, Jacobson K, et al.Identification of an IV-dextrose solution as the source of an outbreak of Kleb-siella pneumoniae sepsis in a newborn nursery. J Hosp Infect 1999;43:70-3.
21. Pessoa-Silva CL, Meurer Moreira B, Camara Almeida V, Flannery B, AlmeidaLins MC, Mello Sampaio JL, et al. Extended-spectrum b-lactamase-producingKlebsiella pneumoniae in a neonatal intensive care unit: risk factors for infectionand colonization. J Hosp Infect 2003;53:198-206.
22. Linkin DR, Fishman NO, Patel JB, Merrill JD, Lautenbach E. Risk factors forextended-spectrum b-lactamase-producing Enterobacteriaceae in a neonatalintensive care unit. Infect Control Hosp Epidemiol 2004;25:781-3.
23. Alsubaie S, Maither A, Alalmaei W, Al-Shammari AD, Tashkandi M, Somily AM,et al. Determinants of hand hygiene noncompliance in intensive care units. AmJ Infect Control 2013;41:131-5.
24. Balkhy HH, El-Saed A, Al Johani SM, Francis C, Al-Qahtani AA, Al-Ahdal MN,et al. The epidemiology of the first described carbapenem-resistant Klebsiellapneumoniae outbreak in a tertiary care hospital in Saudi Arabia: how far do wego? Eur J Clin Microbiol Infect Dis 2012;31:1901-9.
25. Tenover FC, Arbeit RD, Goering RV, Mickelsen PA, Murray BE, Persing DH, et al.Interpreting chromosomal DNA restriction patterns produced by pulsed-fieldgel electrophoresis: criteria for bacterial strain typing. J Clin Microbiol 1995;33:2233-9.
26. Hart CA. Klebsiellae and neonates. J Hosp Infect 1993;23:83-6.27. Villari P, Iacuzio L, Torre I, Scarcella A. Molecular epidemiology as an effective
tool in the surveillance of infections in the neonatal intensive care unit. J Infect1998;37:274-81.
28. Gupta A, Della-Latta P, Todd B, San Gabriel P, Haas J, Wu F, et al. Outbreak ofextended-spectrum b-lactamase-producing Klebsiella pneumoniae in a neonatalintensive care unit linked to artificial nails. Infect Control Hosp Epidemiol2004;25:210-5.
29. Grohskopf LA, Huskins WC, Sinkowitz-Cochran RL, Levine GL,Goldmann DA, Jarvis WR. Use of antimicrobial agents in United Statesneonatal and pediatric intensive care patients. Pediatr Infect Dis J 2005;24:766-73.
30. Harris AD, McGregor JC, Johnson JA, Strauss SM, Moore AC, Standiford HC,et al. Risk factors for colonization with extended-spectrum b-lactamase-producing bacteria and intensive care unit admission. Emerg Infect Dis 2007;13:1144-9.
31. Ofek-Shlomai N, Benenson S, Ergaz Z, Peleg O, Braunstein R, Bar-Oz B.Gastrointestinal colonization with ESBL-producing Klebsiella in pretermbabies: is vancomycin to blame? Eur J Clin Microbiol Infect Dis 2012;31:567-70.
32. Crivaro V, Bagattini M, Salza MF, Raimondi F, Rossano F, Triassi M, et al. Riskfactors for extended-spectrum b-lactamase-producing Serratia marcescens andKlebsiella pneumoniae acquisition in a neonatal intensive care unit. J Hosp Infect2007;67:135-41.
33. Venezia RA, Scarano FJ, Preston KE, Steele LM, Root TP, Limberger R, et al.Molecular epidemiology of an SHV-5 extended-spectrum b-lactamase inenterobacteriaceae isolated from infants in a neonatal intensive care unit. ClinInfect Dis 1995;21:915-23.









![Total Synthesis and Evaluation of [ψ[CH 2 NH]Tpg 4 ] Vancomycin Aglycon: Reengineering Vancomycin for Dual D -Ala- D - Ala and D -Ala- D -Lac Binding Brendan.](https://static.fdocument.org/doc/165x107/56649d1b5503460f949f12a1/total-synthesis-and-evaluation-of-ch-2-nhtpg-4-vancomycin-aglycon-reengineering.jpg)






