Protein Structure Fall 2011 Aaron Zampaglione. Protein Fold Rossmann Fold.

Volume 25Number 4October 1991
Janasi HK, et ai, eds. Fibrinogen, fibrin formation and fibrinolysis. New York: Walter de Gruyter 1986;4:185.
12. Soria J, Mirshahi MC, Mirshahi S, et a1. Soluble fibrin inplasma using a specific fibrin-monoclonal antibody directedagainst the N-terminal part ofthe beta chain. In: MatsudaM, Iwanaga S, Takada A, et ai, eds. Fibrinogen 4. Currentbasis and clinical aspects. Amsterdam: Excerpta Medica,1990:187-94.
13. Lotti T, Fabbri P, Panconesi E. The pathogenesis ofvenousleg ulcers [Letter]. J AM ACADDERMATOL 1987;16:877-9.
14. Ksander GA, Pratt BM, Desiletsavis P, et al. Inhibition ofconnective tissue formation in dermal wounds covered withsynthetic, moisture vapor permeable dressings and itsreversal by transforming growth factor (3. J Invest DermatoI1990;95:195-201.
15. Ksander GA, Sawamura SJ, Ogawa Y, et al. The effect ofplatelet releasate on wound healing in animal models. JAMACAD DERMATOL 1990;22:781-91.
16. Barath P, Fishbein MC, Cao J, et a1. Detection and localization of tumor necrosis factor in human atheroma. Am JCardioI1990;65:297-302.
17. Schirren ca, Scharffetter K, Hein R, et a1. Tumor necrosis factor a induces invasiveness of human skin fibroblastsin vitro. J Invest Dermatol 1990;94:706-10.
18. Polak B, Duperray A, Troesch A, et al. Biogenesis of the
Venous leg ulcers
vitronectin receptor inhumanendothelial cell: evidence thatthe vitronectin receptor and GPIIb-I1Ia are synthesized bya common mechanism. Blood 1989;73:1519-24.
19. Bevilacqua MD, Pober lS, Majeau GR, et al. RecombinantTNF-induces procoagulant activity in cultured humanvascular endothelium. Characterization and comparisonwith actions of interleukin-l, Proc Natl Acad Sci USA1986;83:4533-7.
20. Hebda PA, Eaglestein WH. The stimulatory effect oftransforming growth factor-beta and epidermal growthfactor on epidermal migration [Abstract]. Clin Res1986;34:755A.
21. Clark RAF. Cutaneous tissue repair: basic biologic considerations. I. J AM ACAD DERMATOL 1985;13:701-25.
22. Lammers AM, Van de KerkhofPCM, Schalwijk JS, et al.Elastase, a marker for neutrophils in skin infiltrates. Br JDermatoI1986;115:181-6.
23. Homsy R, Pelletier-Lebon P, TOOer JM, et al. Characterization ofhuman skin fibroblasts' elastase activity. JInvestDermatoI1988;91:472-7.
24. Croute F, Delaporte E, Gaucherand M, et al. Keratinocytefibroblast interactions: 11-1 and keratinocyte soluble factors enhance elastase activity of dermal fibroblasts [Abstract]. J Invest DermatolI990;94:392-3.
Detection of cytokine-induced protein ')I-immuneprotein-IO (')I-IPIO) in atypical melanocyticproliferationsBruce R. Smoller, MD,a, b and James Krueger, MDb Stanford, California, andNew York, New York
'Y-Immune protein-lO Cr-!PI0) is a cytokine whose expression has been shown to be inducedby interferon-'Y. Itis a member of a group ofclosely related cytokines (e.g., intedeukin 8 andplatelet factor 4) with chemotactic properties. 'Y-IPIO has been detected in keratinocytes,lymphocytes, monocytes, and endothelial cells in immunologically mediated processes, suchas positive tuberculin skin tests, and in growth-activated keratinocytes, such as in psoriasis.Keratinocytes in normal epidermis do not produce 'Y-IPIO. We tested the hypothesis that keratinocytes adjacent to dysplasticnevi andmelanomas would produce 'Y-IPI0, perhaps as partof an immune response to a tumor, and that this response would not be seen in ordinary melanocytic nevi. We used an affinity-purified, polycional rabbit anti-')'-IPI0 antibody to examine 10 nevi with moderate to severe histologic dysplasia, one superficial spreading melanoma,and 10 compound melanocytic nevi with no features ofdysplasia. As predicted, keratinocytessurrounding allof the cytologically atypical melanocytic lesions displayedstrong staining with'Y-IP10. There was no staining of keratinocytes adjacent to ordinary melanocytic nevi. Theobserved keratinocyte staining with 'Y-IPI0 may be related to a host immune response to antigenically abnormal cells. (J AM ACAD DERMATOL 1991;25:627-31.)
From tile Departments of Dermatology and Pathology, Stanford University Medical Center"; and the Departments of Pathology andMedicine, Division of Dermatology, New York Hospital-CornellUniversity Medical Center.b
Accepted for publication June 5,1991,Reprint requests: B. Smaller, MD, Department of Pathology, Stanford
University Medical Center, Stanford CA 94305.16/1/31409
627

628 Smoller and Krueger
Dysplastic nevi occupy an uncertain position inthe classification of melanocytic proliferations. I-5
The presence ofthese lesions is thought to representa marker fodncreased risk ofmelanoma developingin some patients.! This risk is most clearly defined inpatients with type D2 dysplastic nevus syndrome,those patients with dysplastic melanocytic nevi occurring in the setting of familial melanoma.2-4 Therisk for subsequent development of melanoma ismuch less certain in patients with sporadic dysplastic nevi (i.e., dysplastic melanocytic nevi occurringoutside the setting of familial melanoma).5, 6 Recently an epidemiologic study demonstrated premalignant potential in patients with a single sporadicdysplastic nevus.7 However, this observation is presently much less accepted.
Although there is less than total consensus on thesignificance of sporadic dysplastic nevi, many studies in the past decade have attempted to unify thediagnostic criteria of these lesions, both clinicallyand histologically. Recent studies have shown thatpathologists can reproducibly recognize featuresthat differentiate a dysplastic nevus from a common,acquired nevus and that correlate with the clinicalfeatures described in these lesions.8
I'-Immune protein-lO (I'-IPlO) is believed to bepart of a family of cytokines that includes plateletfactor 4 and interIeukin 8.9 These proteins havechemotactic properties. 1'-IF lO has been demonstrated within keratinocytes, monocytes, and endothelial cells after exposure to interferon-I'. 10 I'-IP 10has not been expressed in these same cells after exposure to a wide range of other cytokines, but not allsuch proteins have yet been tested. This protein hasrecently been demonstrated in keratinocytes in inflammatory conditions such as fixed drug eruptions,psoriasiform dermatitis of the acquired immunodeficiencysyndrome(AIDS), andseborrheicdermatitiS.II, 12 In these studies, it was suggested thatkeratinocyte expression of 1'-IP lOis a marker ofcytokine production by surrounding inflammatorycells and therefore evidence of an immune-mediatedprocess.
In this study, we have attempted to demonstratethat dysplastic nevi share with melanoma the abilityto induce an immune response within keratinocytesadjacent to the lesions by showing that they induce1'-IP10 expression in surrounding keratinocytes.
MATERIAL AND METHODS
We examined tissue from biopsy specimens received atthe New York Hospital--Cornell University Dermato--
Journal of theAmerican Academy of
Dermatology
pathology Laboratory with a clinical diagnosis of a pigmented lesion. Consecutively accessioned cases during a2-week period were selected for inclusion in the study, after routine histologic diagnosis. Ten consecutive lesionsdiagnosed as dysplastic nevi were chosen for inclusion inthe study. Thecriteria used for making this diagnosis weresimilar to those of Clark et al. 13 We required both architectural and cytologic atypia for a diagnosis of dysplasia.Architectural features of dysplasia included lateral extension of the junctional component of the lesion beyondthe dermal component, bridging ofadjacent rete ridges bynests of horizontally oriented melanocytes, abnormallyplaced nests of melanocytes between and along the sidesof rete ridges, increased numbers of single melanocytes,lamellar fibroplasia, concentric eosinophilic fibrosis, andevidence of host response (lymphocytes and dermal melanophages). We also insisted on some degree ofcytologicatypia, defined as enlargement of nuclei, variable hyperchromasia, and occasional prominence ofnucleoli. Not allarchitectural changes were present in each lesion diagnosed as dysplastic; however, cytologic atypia was presentin each lesion given the diagnosis. Lesions with minimaldegrees of the changes just listed were excluded from thestudy. Control tissue included 10 consecutive ordinarymelanocytic nevi that showed no architectural or cytologic atypia and one superficial spreading melanoma. Themelanoma was a Clark level II lesion and measured up to0.65 mm. in thickness. Itwas chosen as the positive control on the basis of architectural features of irregular nestformation, bridging of rete ridges, and dermal fibrosis,which closely resembled many of the dysplastic nevi examined in the present study. Four other melanomas ofvarying depths and Clark levels were also examined forstaining with the anti-")'-IPI°antibody but served as lessstringent controls because of variations in histologic pattern that made them less closely resemble the experimental lesions.
Additional 5 ,urn sections were cut from specimens oflesions selected for the study. Sections were deparaffinized and rehydrated. Sections were incubated with0.3% hydrogen peroxide to eliminate endogenous peroxidase activity. The avidin-biotin-immunoperoxidasemethod was used, and all sections were stained with anaffinity-purified rabbit antibody directed against the'Y·IP10 protein. The antibody (provided by Drs. A. Lus·ter and A. B. Gottlieb, Laboratory of Investigative Dermatology, Rockefeller University, New York City) wasused in a dilution of 1:50, and sections were incubatedovernight at 4° C. No protease pretreatment was used.After additional washings and incubations with the sec·ondary anti-rabbit IgG antibodies (Vector Laboratories,Burlingame, Calif.), the antibody complexes were local·ized with diaminobenzidine used as the chromagen. Additional sections, run in parallel but with omission of theprimary antibody, served as the negative. controls for allcases.

Volume 25Number 4October 1991 -y-IPlO in atypical melanocytic proliferations 629
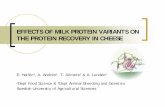
Fig. 1. Dysplastic nevus, stained with anti-')'-IPIO showing strong, diffuse staining of keratinocytes. There is no staining of melanocytes. (X160.)
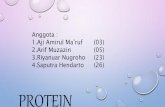
Fig. 2. Malignant melanoma, stained with anti-')'-IPlO showing strong cytoplasmic staining ofkeratinocytes in mid epidermis. Arrow points to positively stained keratinocyte. (X250.)
RESULTS
We examined 10 histologically and clinicallydysplastic nevi, one superficial spreading melanoma(Clark's level II), and 10 clinically and histologicallycommon acquired melanocytic nevi with antibodiesto /,-IP 10. Staining ofkeratinocytes surrounding themelanocytic lesions in all dysplastic nevi and surrounding the melanomas was strong and diffuse(Figs. 1 and 2). This staining was restricted largelyto the cytoplasm of keratinocytes. The staining waspresent in acanthotic regions of the epidermis, aswell as in areas of apparently normal thickness.
There was no apparent correlation between theamount of dermal inflammation and intensity ofstaining. All atypical melanocytic proliferations hadsome degree of dermal inflammatory infiltrate, butthe keratinocyte /'-IP lO expression was not limitedto areas overlying the inflammation. There was nostaining of melanocytes in any of the specimens examined. Focal inflammatory cells and endothelialcells within the dermis were decorated with the antibody.
None of the common acquired melanocytic nevishowed any keratinocyte staining with the -y-IPIO

630 Smaller and Krueger
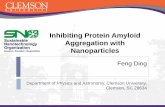
Fig. 3. Common acquired melanocytic nevus stainedwith anti-y-IPlO showing no staining of keratinocytes.(X160.)
antibody (Fig. 3). Two of 10 lesions had a scant dermal inflammatory infiltrate. There was no keratinocyte staining in these lesions. Areas of acanthosiswere present in several of these melanocytic nevi,similar to areas seen in the atypical melanocyticproliferations, but no keratinocyte expression of'Y-IPlO was seen in these areas within the ordinarynevi.
DISCUSSION
Our study demonstrated the presence of 'Y-IPlOin keratinocytes surrounding dysplastic nevi and asuperficial spreading melanoma. No such proteinexpression was seen in keratinocytes surroundingordinary nevi. Two explanations are possible forthese findings: keratinocytes are producing 'Y-IPlOin response to activated lymphocytes attracted to theatypical melanocytic proliferations, or keratinocytesare producing 'Y-IP10 as a direct response to a melanocyte-derived stimulus.
'Y-IPlO production in keratinocytes may be theresult of cytokines produced as part of the host immune response, which is almost always present to
Journal of theAmerican Academy of
Dermatology
some degree underlying dysplastic nevi and melanomas and is frequently absent in common acquirednevi. This would be analogous to the situation infixed drug eruptions,11 and presumably inpsoriasis,14 whereby the keratinocytes within theepidermis respond to activated lymphocytes by producing proteins not normally expressed. It is possible that the slight inflammatory response seen in twoof the common acquired melanocytic nevi did notinduce keratinocyte 'Y-IP10 production because thechronic inflammatory cells were not "activated." Ithas been shown that "resting" lymphocytes do notproduce cytokines such as interferon-')' and thus willnot stimulate keratinocytes to produce 'Y-IP1O. Furthermore, although an immune response was presentin all atypical melanocytic proliferations we examined, the amount of inflammation observed wasvariable and often relatively unimpressive. ')'-IPIOexpression did not appear to be directly related to theintensity of this cellular immune response, nor wasthe protein expression confined to epidermis immediately overlying dermal lymphocytes.
HLA class II expression has been reported to occur on melanoma cells, but to be absent in most normal melanocytic nevi. 15, 16 The spectrum of HLAclass IIexpression in dysplastic nevus cells is still notfully elucidated, in part because of technical problems of antigen recognition in paraffinizedsections. I?, 18 These HLA molecules could contribute directly to antitumor immunity, perhaps in theform of activating "resting" lymphocytes, and causethem to produce cytokines that, in turn, stimulatekeratinocyte production of 'Y-IP1O. This may be amechanism whereby the abnormal melanocytescause 'Y-IP10 expression by surrounding keratinocytes. In a similar fashion, Albino et al. 19 described partial transformation phenotypes ofhumanmelanocytes induced by ras oncogenes. This phenotype is, in part, characterized by HLA class II molecule expression. Because some, but not all, growthproperties of melanocytes are altered, they may beanalogous to nevus cells within dysplastic nevi,which are also growth-altered, but not fully transformed.
An alternative explanation for our observation isthat the "(·IPlO expression by keratinocytes surrounding dysplastic nevi and melanoma is a result ofdirect induction of the protein by the nests of atypical melanocytes. This would explain the finding ofdiffuse staining of keratinocytes with 'Y-IP10 overthe extent of the melanocytic lesions, independent of

Volume 25Number 4October 199\
dermal inflammation, with absence of 'Y-IP lOin keratinocytes far removed from the nests of melanocytes.
This last hypothesis suggests that keratinocytesare capable of responding to stimuli produced bymelanocytes and that melanocytes are capable ofstimulating production of an immune-related protein in keratinocytes. This interaction between keratinocytes and melanocytes appears to occur in thepres~nceof cytologically, and perhaps antigenically,atypIcal melanocytes.
REFERENCES
1. ~lark 'YH, Reimer RR, Greene M, et al. Origin of familIal mahgnant melanomas from heritable melanocytic lesions. Arch Dermatol 1976;732-8.
2. Greene MH. Dysplastic nevus syndrome. Hasp Prac1984;\9:92-108.
3. Elder DE, Goldman LI, Goldman SC, et al. Dysplastic nevus syndrome: a phenotype association of sporadic cutaneous melanoma. Cancer 1980;46:1787-94.
4. Murphy OF, Halpern A. Dysplastic melanocytic nevi:Normal variants or melanoma precursors? Arch Dermatol1990;126:519-21.
5. Piepkorn M. A hypothesis incorporating the histologiccharacteristics of dysplastic nevi into the normal biologicaldevelopment of melanocytic nevi. Arch Dermatol 1990;126:514-8.
6. Ackerman AB, Mihara 1. Dysplasia, dysplastic melanocytes, dy.splastic nevi, the dysplastic nevus syndrome andthe relatIOn between dysplastic nevi and malignant melanoma. Hum Pathol 1985;16:88-91.
7. Rivers lK, Kopf A W, Vinokur AF, et aL Clinical characteri~tics of malignant melanoma in persons with dysplasticnevI. Cancer 1990;65:1232-6.
8. Rhodes A~, M~hm MC Jr, Weinstock MA. Dysplasticmelanocytlc nevI: a reproducible histologic definition em-
'Y-1PIO in atypical melanocytic proliferations 631
phasizing cellular morphology. Mod Patho11989;2:306-19.9. Luster AD, Ravetch lV. Genomic characterization of a
gamma-interferon-inducible gene (IP-W) and identification of an interferon-inducible hypersensitive site. Mol CellBioI 1987;7:3723-31.
10. KaplanG, Luster AD, HancockG, etal. The expression of~ gamma-interferon-induced protein (IP-lO) in delayedImmune responses in human skin. 1 Exp Moo 1987'166:1098-108. '
11. ~moller .BR, Luster AD, Krane JF, et al. Fixed drug eruptIOns: eVidence ofa gamma-interFeron-mediated process. JCutan Pathol (In press.)
12. Smoller BR, McNutt NS, Gray MH, et al. Detection of thegamma-interferon-induced protein (IP-1 0) in psoriasiformdermatitis of AIDS. Arch DermatoI1990;126:1457-62.
13. Clark WH Jr, Elder DE, Guerry D, et al. A study of tumorprogression: the precursor lesions of superficial spreadingand nodular melanoma. Hum PathoI1984;15:1147-65.
14. Gottlieb AB, Luster AD, Posnett DN, et al. Detection of agamma interferon-induced protein IP-lO in psoriaticplaques. J Exp Med 1988;168:941-8.
15. Moretti S, Massolino R, Brogelli L, et al. Ki-67 antigen expression correlates with tumor progression and HLA-DRantigen expression in melanocytic lesions. J Invest Dermatal 1990;95:320-4.
16. Lopez-N~vot MA,. Garcia E, Romero C, et al. Phenotypicand ge~etIc analySIS ofHLA class I and HLA-DR antigenexpresSIOn on human melanomas. Exp Clin Immunogenet1988;5:203-12.
17. Elder DE, Rodeck U, Cardello F, et al. Antigenic profile oftumor progression stages in human melanocytic nevi andmelanomas. Cancer Res 1989;49:5091-6.
18. Guerry D IV, Alexander DA, Elder DE, et al. Interferongamma regulates the T cell response to precursor nevi andbiologically early melanoma. 1 ImmunoI1987;139:305-12.
19. Albino AP, Houghton AN, Eisinger M, et al Class II histocompatibility antigen expression in human melanocytestransformed by Harvey murine sarcoma virus and KirstenMSV retroviruses. J Exp Moo 1986;164:1710-22.