Calcitonin gene-related peptide (human α-CGRP) counteracts vasoconstriction in human subarachnoid...
4
ELSEVIER Neuroscience Letters 170 (1994) 67 70 NEUROSCIENCE LETTERS Calcitonin gene-related peptide (human -CGRP) counteracts vasoconstriction in human subarachnoid haemorrhage Roar JuuP, Svend Aakhus b, Knut Bj6rnstad b, Sven Erik Gisvold c, Alf O. Brubakk d, Lars Edvinsson ~'* Departments ~!f "Neurosurgery, bMedicine, "Anesthesia and aBiomedieal Engineering, University Hospital of Trondhebn, Trondheim, Norw~n" "Department of'Internal Medicine, Universi O' Hospital ~f Lund, S-221 85 Lund, Sweden Received 29 September 1993; Revised version received 26 January 1994: Accepted 28 January 1994 Abstract Calcitonin gene-related peptide (CGRP) is a neuropeptide co-stored with tachykinins (substance P, neurokinin A) in cerebrovas- cular sensory fibers in the trigeminal ganglion. Preceding studies on subarachnoid hemorrhage (SAH) revealed that an enhanced release of CGRP resulted in the selective loss of perivascular CGRR Therefore, the present study was designed to evaluate the effects of intravenous administration of human ~-CGRP on cerebral vasoconstriction in the postoperative course after SAH in 5 patients (8 infusions). Cerebral vasoconstriction was evaluated with transcranial Doppler sonography. The increase in the relationship between middle cerebral artery (MCA) velocity and internal carotid artery (ICA) velocity (the hemodynamic index) was used as an indicator of vasoconstriction and compared to the contralateral side. A significant reduction was found in the hemodynamic index during the CGRP infusion (4.3 + 0.5, P < 0.05) as to compared to before infusion (6.2 + 0.5). There was no measurable change in the hemodynamic index on the contralateral side. No significant change was observed in pulsatility index, blood pressure o1 consciousness during the peptide infusion. A significant increase in heart rate was observed during the infusion as compared to before and after infusion (90 + 4 vs. 76 + 5). Cardiac ultrasound data indicated a mean cardiac output increase of 1.9 liter/min, and a mean decrease in total peripheral resistance of 538 dynes s/cm5. The results obtained show that infusion of human c~-CGRP may induce normalisation of cerebrovascular tone in SAH. Key words: Calcitonin gene-related peptide; Subarachnoid haemorrhage; Doppler; Vasospasm; Trigemino-cerebrovascular system The cerebral circulation is supplied with sensory nerve fibres which originate mainly in the first division of the trigeminal ganglion [17]. The peptides stored in the trigemino-vascular system (substance P, neurokinin A and calcitonin gene-related peptide (CGRP) are released via an axonreflex-like mechanisms [13] which can be acti- vated in vasoconstrictive conditions such as that seen during vasospasm after a subarachnoid hemorrhage (SAH) [12] and in the headache phase of migraine at- tacks [7,8]. CGRP is released in parallel with the degree *Corresponding author. Status on admission was graded according to Hunt and Hess (HH) [10]. Time from operation to ~-CGRP infusion (Time op-CGRP) and out- come; outcome was classified after Teasdale and Jennett [16]. Patients receiving two infusions are marked with *; also noted at Time op- CGRP. 0304-394(//94/$7.00 c.C 1994 Elsevier Science Ireland Ltd. All rights reserved SSD1 0304-3940(94)00099-V of vasoconstriction after SAH in man [12]. In patients with a fatal outcome following the SAH (5-10 days post bleeding) there is a selective depletion of CGRP in the sampled artery, the middle cerebral artery [3,5]. On the basis of these clinical observations we have hypothesised that CGRP is released to counterbalance vasoconstric- tion, but in severe SAH the amount is not enough or when the ischemic sequale appears, the CGRP supply is exhausted. The present study was designed to test this hypothesis in the clinical situation by administration of human ~-CGRP to SAH patients with significant vaso- constriction. Patients. Five patients (3 males, 2 females, age 40-77 years) with vasoconstriction [middle cerebral artery (MCA) velocity exceeding 120 cm/s] in the postoperative course after SAH were investigated. The study was ap- proved by the ethical committee of the University of Trondheim. Departmental policy was followed in all pa-
Transcript of Calcitonin gene-related peptide (human α-CGRP) counteracts vasoconstriction in human subarachnoid...

E L S E V I E R Neuroscience Letters 170 (1994) 67 70
NEUROSCIENCE LETTERS
Calcitonin gene-related peptide (human -CGRP) counteracts vasoconstriction in human subarachnoid haemorrhage
Roar JuuP, Svend Aakhus b, Knut Bj6rnstad b, Sven Erik Gisvold c, Al f O. Brubakk d, Lars Edvinsson ~'*
Departments ~!f "Neurosurgery, bMedicine, "Anesthesia and aBiomedieal Engineering, University Hospital of Trondhebn, Trondheim, Norw~n" "Department of'Internal Medicine, Universi O' Hospital ~f Lund, S-221 85 Lund, Sweden
Received 29 September 1993; Revised version received 26 January 1994: Accepted 28 January 1994
Abstract Calcitonin gene-related peptide (CGRP) is a neuropeptide co-stored with tachykinins (substance P, neurokinin A) in cerebrovas-
cular sensory fibers in the trigeminal ganglion. Preceding studies on subarachnoid hemorrhage (SAH) revealed that an enhanced release of CGRP resulted in the selective loss of perivascular CGRR Therefore, the present study was designed to evaluate the effects of intravenous administration of human ~-CGRP on cerebral vasoconstriction in the postoperative course after SAH in 5 patients (8 infusions). Cerebral vasoconstriction was evaluated with transcranial Doppler sonography. The increase in the relationship between middle cerebral artery (MCA) velocity and internal carotid artery (ICA) velocity (the hemodynamic index) was used as an indicator of vasoconstriction and compared to the contralateral side. A significant reduction was found in the hemodynamic index during the CGRP infusion (4.3 + 0.5, P < 0.05) as to compared to before infusion (6.2 + 0.5). There was no measurable change in the hemodynamic index on the contralateral side. No significant change was observed in pulsatility index, blood pressure o1 consciousness during the peptide infusion. A significant increase in heart rate was observed during the infusion as compared to before and after infusion (90 + 4 vs. 76 + 5). Cardiac ultrasound data indicated a mean cardiac output increase of 1.9 liter/min, and a mean decrease in total peripheral resistance of 538 dynes s/cm 5. The results obtained show that infusion of human c~-CGRP may induce normalisation of cerebrovascular tone in SAH.
Key words: Calcitonin gene-related peptide; Subarachnoid haemorrhage; Doppler; Vasospasm; Trigemino-cerebrovascular system
The cerebral circulation is supplied with sensory nerve fibres which originate mainly in the first division of the trigeminal ganglion [17]. The peptides stored in the trigemino-vascular system (substance P, neurokinin A and calcitonin gene-related peptide (CGRP) are released via an axonreflex-like mechanisms [13] which can be acti- vated in vasoconstrictive conditions such as that seen during vasospasm after a subarachnoid hemorrhage (SAH) [12] and in the headache phase of migraine at- tacks [7,8]. C G R P is released in parallel with the degree
*Corresponding author.
Status on admission was graded according to Hunt and Hess (HH) [10]. Time from operation to ~ -CGRP infusion (Time op-CGRP) and out- come; outcome was classified after Teasdale and Jennett [16]. Patients receiving two infusions are marked with *; also noted at Time op- CGRP.
0304-394(//94/$7.00 c.C 1994 Elsevier Science Ireland Ltd. All rights reserved SSD1 0 3 0 4 - 3 9 4 0 ( 9 4 ) 0 0 0 9 9 - V
of vasoconstriction after SAH in man [12]. In patients with a fatal outcome following the SAH (5-10 days post bleeding) there is a selective depletion of C G R P in the sampled artery, the middle cerebral artery [3,5]. On the basis of these clinical observations we have hypothesised that C G R P is released to counterbalance vasoconstric- tion, but in severe SAH the amount is not enough or when the ischemic sequale appears, the C G R P supply is exhausted. The present study was designed to test this hypothesis in the clinical situation by administration of human ~ -CGRP to SAH patients with significant vaso- constriction.
Patients. Five patients (3 males, 2 females, age 40-77 years) with vasoconstriction [middle cerebral artery (MCA) velocity exceeding 120 cm/s] in the postoperative course after SAH were investigated. The study was ap- proved by the ethical committee of the University of Trondheim. Departmental policy was followed in all pa-

68 R. Juul cta/. /Neuroscience Letters 170 , 1994, 6 7 70
tients; early operation with clipping of the aneurysm, intensive care and intravenous infusion of the calcium entry blocker nimodipine at 2 mg/h for 10 days (Bayer AG, Germany). On admission the patients were classi- fied according to Hunt and Hess [10]. Neurological state was graded with Glasgow Coma Scale (GCS) [16].
Doppler recordings. Doppler recordings were per- formed with velocity registrations from both MCA and internal cerebral arteries (ICA) [1,2]. The hemodynamic index (V mean MCA/V mean ipsilateral ICA) was used as an indicator of cerebral vasoconstriction and per- formed by the same experimentator throughout the study (R.J). The equipment used was a TC 2-64 B (EME, Germany) with 2 MHz probes for transcranial velocity recordings and 4 MHz for carotid velocity recordings.
Transthoracic cardiac ultrasound with a Vingmed CFM 750 duplex ultrasound scanner supplied with a 3.25 MHz probe. Cardiac output and total peripheral resistance were determined as described by Skjaerpe et al. [14].
Infusion. When Doppler sonography indicated vaso- constriction in the postoperative course patients received synthetic human c~-CGRP (CB 003, Celltech, UK) dis- solved in 0.9% sodium chloride intravenously at an infu- sion rate of 0.6/1g/rain. Patients were monitored (Dop- pler) before infusion, immediately after the start of the infusion, with regular intervals during the infusion, and 1 h after the infusion was stopped. Infusion time varied between 1.5 and 52 h because of clinical response. Car- diac output was monitored using duplex ultrasound before and during infusion on six occasions. Blood pres- sure was monitored through a radial artery catheter con- nected to a Statham/Gould pressure transducer. Heart rate and consciousness (Glasgow Coma Scale) were monitored regularly.
Statistics. Statistics were evaluated by Student's t-test and correlation factor calculation using linear regression analysis. Mean data are given with S.E.M.
Clinical data. The clinical data on the individual pa- tients are given in Table 1. The five patients were in Hunt grade 2 4 upon admission [10]. The infusion started 1 or 2 days after the operation (in one subject at day 6 be-
Table 1 Clinical data on patients included in the study of human ~-CGRP infusion
Age (years) Sex HH Time op-CGRP Outcome
1 41 M 2 1 day Excellent 2 77 M 2 1 day Excellent 3 58* M 2 2 days, 3 days Excellent 4 40* F 3 6 days, 8 days Excellent 5 44* F 4 2 days, 7 days Good
Status on admission was graded according to Hunt and Hess (HH) [10]. Time from operation to ~-CGRP infusion (Time op-CGRP) and out- come; outcome was classified after Teasdale and Jennett [16], Patients receiving two infusions are marked with *; also noted at Time op- CGRP.
• Spasm side 7 ::1 Other side
..= 5
4
i3
1 i 0 I I i
Pre-infusion During infusion After infusion
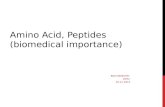
Fig. 1. Data collected for all eight infusions in five patients are shown with S.E.M. Hemodynamic index on vertical axis. The hemodynamic index values are given for the SAH side as well as the contralateral side. Compared to before infusion (6.2 + 0.5) a lower index value was found during infusion (4.3 + 0.5; *P < 0.05) on the symptomatic side. Values represent means _+ S.E.M., n = 8.
cause of development of vasoconstriction), The outcome of all five subjects was good to excellent. Infusion was given twice in three subjects.
Hemodynamic changes. The hemodynamic index changes occuring during infusion are summarized in Fig. 1. On the SAH side, the hemodynamac index was signifi- cantly higher than that on the non-spasm side (P < 0.05). The patterns of hemodynamic changes seen after admini- stration of human 0~-CGRP in the individual subjects are similar but with some inter-individual differences. Indi- viduals given infusion over relatively short time intervals had hemodynamic index decreases by up to 84%.
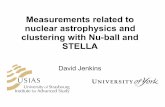
A significant mean drop by 31% was found in the hemodynamic index during the CGRP infusion (4.3 + 0.51 as compared to before the infusion (6.2 _+ 0.5) (P < 0.05) on the vasospastic side (Fig. 1). When com- paring the vasospastic side with the contralateral side in the same individuals, the significant difference dissap- peared. After cessation of the infusion the hemodynamic index returned towards the original values (P < 0.05). There was no significant changes on the contralateral side (3.0 + 0.4 vs 3.0 + 0.3) (Fig. 1). There were no changes in the pulsatility index, neither on the spasm side nor contralaterally (Fig. 2).
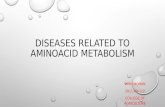
Cardiovascular changes. All subjects showed redden- ing of the skin during the peptide infusion. A significam increase was seen in the heart rate during the infusion (90 + 4 vs. 76 + 5 beats per min, P < 0.05) while blood pressure was unaltered (Fig. 3). These changes were cor- related with a mean increase of 1.9 liter/min in cardiac output and a mean decrease in systemic vascular resis- tance of 538 dynes s/cm 5.
Discussion. The present study has demonstrated clearly that parenteral administration of human a-

R. Juul et al. / Neuroscience Letters 170 (1994) 67 70 69
C G R P may reverse significantly the vasoconstriction seen after SAH, without any effect on the contralateral non-spasm side. During the infusion there was a tend- ency in some subjects towards a better clinical state, but it was not systematically evaluated and the infusion pe- riod was relatively short. After cessation, the hemody- namic index returned towards pre-injection values. Thus, as hypothetized, c~-CGRP may normalize the tone of preconstricted arteries such as those on the vasospastic side in human SAH.
The trigemino-vascular reflex is considered to be part of a defence reaction [13] which is activated to counter- balance unwanted cerebrovascular constriction with an enhanced release of the potent vasodilator CGRP. Sup- port for this view in the clinic comes from the demon- stration of increased levels of C G R P in cranial venous blood following SAH [12]. In fatal SAH there is deple- tion of perivascular C G R P (middle cerebral artery of man) which we have interpreted as due to exhaustion of the peptide supply causing loss of the reflex vasodilata- tion and deterioration of the patients [3,5]. Our observa- tion that C G R P might be involved in a reflex mechanism to counterbalance cerebrovascular constriction and the observation that the perivascular peptide supply is lost in subjects with severe vasospasm strongly suggests a therapeutic potential. The administration of synthetic human ~ - C G R P in the individual cases are promising, the subjects normalized their cerebral vessel tone during the infusion, albeit to a varying degree. In subjects re- ceiving ~ - C G R P infusion over a long time (up to 52 h), a slight increase in the hemodynamic index was noted. This may be due to the peptide concentration given, the location or the intensity of the vasoconstriction. In gen- eral, we found a significant decrease in the hemodynamic index by 31% during infusion as compared to the pre- infusion state. Since there was no change on the non-
• Spasm side
[] Other side
1.5
1.4
~.1.3 e-,
~1.2
1.1
1.0
0.9 I I I
Pre-infusion During infusion After infusion
Fig. 2. The internal carotid artery pulsatility index-PI (systolic veloc- ity-diastolic velocity/mean velocity) before, during and after infusion is shown. No significant changes were seen. Values represent means _+ S.E.M.. n = 8.
a
~ 1 0 0
E 90
o 8 0
70
0 ~: 60
~r
50 t i t Pre-infusion During infusion After infusion
b
~ 1 4 0
E ~ 1 3 0
2120
~110 2
100 I I I
Pre-infusion During infusion After infusion
Fig. 3. Cardiovascular parameters occuring during the infusion exper- iments, a: mean heart rate was significantly increased during the infu- sion (*P < 0.05). b: mean arterial blood pressure tended to fall but did not reach significance. Values represent means _+ S.E.M., n = 8.
spasm side it indicates that 0t-CGRP induces significant dilation mainly of constricted cerebral vessels. It is possi- ble that a higher dose of cz-CGRP would dilate also vessels contralaterally, however, the dilator response is seen sooner and more marked in the presence of precon- traction [3,4]. This view is in agreement with a parallel study in healthy volunteers who showed no changes in vessel diameter (MCA velocity) or cerebral blood flow after c~-CGRP infusion [15]. Other studies have shown increased common carotid and internal carotid artery velocity, indicating an increase in vessel diameter [11]. In human volunteers, infusion of 0t-CGRP has been found to result in an increase in cardiac output, tachycardia, hypotension and flushing [6,9]. In our study there was no change in pulsatility index or blood pressure. Thus, it is necessary to use a well titrated dose not to have all the pronounced peripheral circulatory effects that can be obtained with higher doses of c~-CGRP [9]. The increases in cardiac output and in heart rate were enough to bal- ance the decrease in total peripheral resistance as evi- denced by the unaltered blood pressure.

70 R. Juul et al./Neuroscience Letters 170 (1994) 07 70
Supported by the Swedish Medical Research Council (no. 05958) and Bayer AG, FRG.
[1] Aaslid, R., Huber, P. and Nornes, H., Evaluation of cerebrovas- cular spasm with transcranial Doppler ultrasound, .1. Neurosurg., 60 (1984) 37~,1.
[2] Aaslid, R., Markwalder, T.M. and Nornes, H., Noninvasive tran- scranial Doppler ultrasound recording of flow velocity in basal cerebral arteries, J. Neurosurg., 57 (1982) 769-774.
[3] Edvinsson, L., Ekman, R., Jansen, I., McCulloch, J., Mortensen, A. and Uddman, R., Reduced levels of calcitonin gene-related peptide-like immunoreactivity in human brain vessels after suba- rachnoid hemorrhage, Neurosci. Lett., 121 (1991) 151- 154.
[4] Edvinsson, L., Fredholm, B.B., Hamel, E., Jansen, I. and Verrec- chia, C., Perivascutar peptides relax cerebral arteries concomitant with stimulation of cyclic adenosine monophosphate accumulation or release of an endothelium-derived relaxing factor in the cat, Neurosci. Lett., 58 (1985) 213-218.
[5] Edvinsson, L., Juul, R. and Jansen, I., Perivascular neuropeptides (NPY, VIE CGRP and SP) in human brain vessels after sub- arachnoid haemorrhage, Acta Neurol. Scand., (1994) in press.
[6] Gennari, C, and Fischer, J.A., Cardiovascular action of calcitonin gene-related peptide in humans, Calcif. Tissue Int., 37 (1985) 581- 584.
[7] Goadsby, P.J. and Edvinsson, L., The trigeminovascular system and migraine: studies characterizing cerebrovascular and neu- ropeptide changes seen in humans and cats, Ann. Neurol., 33 (1993) 48--56.
[8] Goadsby, P.J., Edvinsson, L. and Ekman, R., Vasoactive peptide release in the extracerebral circulation of human during migraine headache, Ann. Neurol., 28 (1990) 183 187.
[9] Howden, C.W., Logue, C., Gavin, K., Collie, L. and Rubin, P.(.. Haemodynamic effects of intravenous human calcitonin gene- re- lated peptide in man, Clin. Sci,, 74 (1988) 413 418.
[10] Hunt, W.E. and Hess, R.M., Surgical risk as related to time o1 intervention in the repair of intracranial aneurysms, J. Neurosurg., 28 (1968) 14 20.
[11] Johnston, F.G., Bell, B.A., Miller, J.D., Haliburn, C., O'Shaugh- nessy, D., Riddell, A.J. and O'Laoire, S.A., The effect of calcitonin gene-related peptide on post-operative neurological deficits fol- lowing subarachnoid haemorrhage, Lancet, 335 (1990) 869-- 872.
[12] Juul, R., Edvinsson, L., Gisvold, S.E., Ekman, R., Brubakk, O. and Fredriksen, T.A., Calcitonin gene-retated peptide-Ll in sub- arachnoid hemorrhage in man. Signs of activation of the trigemino-cerebrovascular system?, Br. J. Neurosurg., 4 (1990) 171 180.
[13] McCulloch, J., Uddman, R., Kingman, T.A. and Edvinsson, L., Calcitonin gene-related peptide: functional role in cerebrovascular regulation, Proc. Natl. Acad. Sci. USA, 83 (1986) 5731- 5735.
[14] Skjaerpe, T., Hegrenaes, H. and lhlen, H., Cardiac output. In L. Hatle and B. Angelsen (Eds.), Doppler Ultrasound in Cardiology, Lea & Febiger, Philadelphia, 1985.
[15] Stanley, J., Martin, J.L., Richards, H., Lovick, A., Barton, M, and Pickard, J.D., Effects ofcalcitouin gene-related peptide on cerebral blood flow in healthy volunteers, J. Cereb. Blood Flow Metab., 11 (1991) 273.
[16] Teasdale, G. and Jennett, B., Assessment of coma and impaired consciousness. A practical scale, Lancet, 2 (1974) 81 84.
[17] Uddman, R. and Edvinsson, L., Neuropeptides in the cerebral circulation, Cerebrovasc. Brain Metab. Rev., 1 (1989) 230-252.