Blockade of tumor necrosis factor-α-converting enzyme improves experimental small intestinal damage...
10
ORIGINAL ARTICLE Blockade of tumor necrosis factor-a-converting enzyme improves experimental small intestinal damage by decreasing matrix metalloproteinase-3 production in rats HIROSHI MATSUMOTO 1 , HIDEKI KOGA 1,2 , MITSUO IIDA 2 , KEN-ICHI TARUMI 1 , MINORU FUJITA 1 & KEN HARUMA 1 1 Division of Gastroenterology, Department of Internal Medicine, Kawasaki Medical School, Kurashiki, Okayama, Japan, and 2 Department of Medicine and Clinical Science, Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japan Abstract Objective. Tumor necrosis factor (TNF)-a-converting enzyme (TACE), which has been purified, regulates maturity of TNF-a. Matrix metalloproteinases (MMPs) play a key role in various inflammatory conditions. The incidence of intestinal damage has increased, but the mechanism and treatment have not been well understood. The purpose of this study was to investigate the roles of TACE and MMP in indomethacin (Indo)-induced intestinal damage as well as the therapeutic effects of TACE inhibitor and selective MMP inhibitor (sMMPi) on this intestinal damage in rats. Material and methods. In the first experiment, serial changes in intestinal ulcers and the production of MMP were investigated. In the second experiment, we assessed the effect of three TACE and/or MMP inhibitors and the production of TNF-a, TACE, MMP-3, -9 and tissue inhibitor of MMP (TIMP)-1. The rats were divided into five groups: a control group, and four groups that received Indo alone, Indo plus TACE inhibitor (GM6001), Indo plus a selective MMP-3 inhibitor and Indo plus an MMP-9/13 inhibitor, respectively. Results. MMP-3 was overexpressed at 24 h after Indo administration, when intestinal injury was most prominent macroscopically and microscopically. GM6001 significantly decreased ulcer severity and suppressed MMP-3 in a dose-dependent fashion. The selective MMP-3 inhibitor dose-dependently ameliorated intestinal damage to the same degree as GM6001, but the MMP-9 inhibitor had no effect on the injury. Conclusions. MMP-3 inhibition ameliorates intestinal damage without apparently affecting either TNF-a or TACE production and the dose response curve suggests that the beneficial effect of the so-called TACE inhibitor is actually mainly mediated via MMP-3 inhibition rather than TNF-a inhibition. Key Words: Inflammation, matrix metalloproteinase (MMP)-3, matrix metalloproteinase (MMP) inhibitor, non-steroidal anti-inflammatory drugs (NSAIDs)-induced intestinal damage, tumor necrosis factor (TNF)-a, tumor necrosis factor (TNF)-a-converting enzyme (TACE, ADAM17, CD156b) Introduction It has been suggested that tumor necrosis factor (TNF)-a is an important mediator in the pathogen- esis of various inflammatory diseases, including inflammatory bowel disease (IBD) [1]. Two forms of TNF-a have been identified: a membrane-bound precursor 26 kD protein, and a 17 kD mature secreted form. The cleavage of cell-associated TNF-a is mediated by metalloproteinases, a disin- tegrin and metalloproteinase (ADAM) known as TNF-a-converting enzyme (TACE, ADAM17, CD156b) [2,3]. TACE shares a significant degree of structural homology with matrix metalloprotei- nase (MMP) in enzyme structures, particularly around zinc-containing active sites. Firm evidence showing TACE as the major TNF-a convertase has led to TACE attracting considerable interest as a specific therapeutic target in diseases known to benefit from anti-TNF-a treatment [4 6]. MMPs, a family of zinc-containing enzymes that, as a group, can degrade and remodel essentially all Correspondence: Hiroshi Matsumoto, MD, PhD, Division of Digestive Diseases, David Geffen School of Medicine at UCLA, MacDonald Research Building, MRL-2736, 675 Charles E. Young Circle Dr. South, Los Angeles, California 90095, USA. Fax: /1 310 8255 204. E-mail: [email protected] Scandinavian Journal of Gastroenterology, 2006; 41: 1320 1329 (Received 16 December 2005; accepted 3 March 2006) ISSN 0036-5521 print/ISSN 1502-7708 online # 2006 Taylor & Francis DOI: 10.1080/00365520600684571 Scand J Gastroenterol Downloaded from informahealthcare.com by University Library Utrecht on 04/08/13 For personal use only.
Transcript of Blockade of tumor necrosis factor-α-converting enzyme improves experimental small intestinal damage...

ORIGINAL ARTICLE
Blockade of tumor necrosis factor-a-converting enzyme improvesexperimental small intestinal damage by decreasing matrixmetalloproteinase-3 production in rats
HIROSHI MATSUMOTO1, HIDEKI KOGA1,2, MITSUO IIDA2, KEN-ICHI TARUMI1,
MINORU FUJITA1 & KEN HARUMA1
1Division of Gastroenterology, Department of Internal Medicine, Kawasaki Medical School, Kurashiki, Okayama, Japan,
and 2Department of Medicine and Clinical Science, Graduate School of Medical Sciences, Kyushu University, Fukuoka,
Japan
AbstractObjective. Tumor necrosis factor (TNF)-a-converting enzyme (TACE), which has been purified, regulates maturity ofTNF-a. Matrix metalloproteinases (MMPs) play a key role in various inflammatory conditions. The incidence of intestinaldamage has increased, but the mechanism and treatment have not been well understood. The purpose of this study was toinvestigate the roles of TACE and MMP in indomethacin (Indo)-induced intestinal damage as well as the therapeutic effectsof TACE inhibitor and selective MMP inhibitor (sMMPi) on this intestinal damage in rats. Material and methods. In thefirst experiment, serial changes in intestinal ulcers and the production of MMP were investigated. In the second experiment,we assessed the effect of three TACE and/or MMP inhibitors and the production of TNF-a, TACE, MMP-3, -9 and tissueinhibitor of MMP (TIMP)-1. The rats were divided into five groups: a control group, and four groups that received Indoalone, Indo plus TACE inhibitor (GM6001), Indo plus a selective MMP-3 inhibitor and Indo plus an MMP-9/13 inhibitor,respectively. Results. MMP-3 was overexpressed at 24 h after Indo administration, when intestinal injury was mostprominent macroscopically and microscopically. GM6001 significantly decreased ulcer severity and suppressed MMP-3 in adose-dependent fashion. The selective MMP-3 inhibitor dose-dependently ameliorated intestinal damage to the samedegree as GM6001, but the MMP-9 inhibitor had no effect on the injury. Conclusions. MMP-3 inhibition amelioratesintestinal damage without apparently affecting either TNF-a or TACE production and the dose�response curve suggeststhat the beneficial effect of the so-called TACE inhibitor is actually mainly mediated via MMP-3 inhibition rather thanTNF-a inhibition.
Key Words: Inflammation, matrix metalloproteinase (MMP)-3, matrix metalloproteinase (MMP) inhibitor, non-steroidal
anti-inflammatory drugs (NSAIDs)-induced intestinal damage, tumor necrosis factor (TNF)-a, tumor necrosis factor
(TNF)-a-converting enzyme (TACE, ADAM17, CD156b)
Introduction
It has been suggested that tumor necrosis factor
(TNF)-a is an important mediator in the pathogen-
esis of various inflammatory diseases, including
inflammatory bowel disease (IBD) [1]. Two forms
of TNF-a have been identified: a membrane-bound
precursor 26 kD protein, and a 17 kD mature
secreted form. The cleavage of cell-associated
TNF-a is mediated by metalloproteinases, a disin-
tegrin and metalloproteinase (ADAM) known as
TNF-a-converting enzyme (TACE, ADAM17,
CD156b) [2,3]. TACE shares a significant degree
of structural homology with matrix metalloprotei-
nase (MMP) in enzyme structures, particularly
around zinc-containing active sites. Firm evidence
showing TACE as the major TNF-a convertase has
led to TACE attracting considerable interest as a
specific therapeutic target in diseases known to
benefit from anti-TNF-a treatment [4�6].
MMPs, a family of zinc-containing enzymes that,
as a group, can degrade and remodel essentially all
Correspondence: Hiroshi Matsumoto, MD, PhD, Division of Digestive Diseases, David Geffen School of Medicine at UCLA, MacDonald Research Building,
MRL-2736, 675 Charles E. Young Circle Dr. South, Los Angeles, California 90095, USA. Fax: �/1 310 8255 204. E-mail: [email protected]
Scandinavian Journal of Gastroenterology, 2006; 41: 1320�1329
(Received 16 December 2005; accepted 3 March 2006)
ISSN 0036-5521 print/ISSN 1502-7708 online # 2006 Taylor & Francis
DOI: 10.1080/00365520600684571
Scan
d J
Gas
troe
nter
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Lib
rary
Utr
echt
on
04/0
8/13
For
pers
onal
use
onl
y.

extracellular matrix components, have a role in
connective tissue remodeling processes associated
with embryonic development, pregnancy, growth,
and wound healing [7,8]. MMPs are produced
mainly by myofibroblasts, but in intestinal tissue
of human IBD, they are also produced by submu-
cosal mononuclear cells which show positive expres-
sion of CD68 [9]. The production of MMPs is
stimulated by lipopolysaccharide (LPS) and pro-
inflammatory cytokines such as TNF-a and inter-
leukin (IL)-1. Consequent imbalance of MMPs with
a physiologic inhibitor, a tissue inhibitor of MMPs
(TIMPs), can result in degradation of the extra-
cellular matrix.
Inhibition of TACE and/or MMP is one antici-
pated approach in the treatment of inflammatory
disease [5�8]. Previous studies have demonstrated
that some potent broad-spectrum inhibitors of
MMPs, called TACE inhibitors, can also prevent
TNF-a release by inhibiting TACE. During clinical
trials, some inhibitors of TACE/MMP unfortunately
have shown adverse effects in patients with cancer or
rheumatoid arthritis, suggesting that these drugs
have too broad a range of MMPs suppression [10].
Therefore, development of more specific inhibitors
of MMP and TACE is needed, but the question of
which MMP is the most important therapeutic
target in intestinal inflammation remains unclear.
Furthermore, the effect of selective MMP inhibition
against experimental intestinal injury has not been
well defined.
We previously reported on the beneficial effects of
antibiotics, some anti-pro-inflammatory cytokine-
neutralizing antibodies, and immunosuppressive
agents against indomethacin (Indo)-induced intest-
inal injury [11�15]. This model is a suitable experi-
mental model showing small intestinal damage by
chemical agents, and has two immunopathological
characteristics: first, a non-steroidal anti-inflamma-
tory drug (NSAID)-induced small intestinal injury,
and the other is also deemed to be a small intestinal
ulcer model of IBD, because they showed the
T-helper (TH)-1-dominant intestinal inflammation
resembling IBD [16]. The aim of the present study
was to investigate the roles of TACE and MMPs in
such intestinal ulceration as well as the therapeutic
effects of the TACE inhibitor and selective MMP
inhibitor (sMMPi) on this experimental intestinal
injury. Among the whole cohort of MMPs, we
focused on MMP-3 and MMP-9 in this study,
because these MMPs were secreted not only by
mucosal myofibroblasts but also by monocyte/
macrophages whose number was dramatically in-
creased in the TH-1-dominant inflamed intestinal
mucosa.
Materials and methods
Animals
Male Wistar rats (weight 170 to 220 g, age
6�/7 weeks) were purchased from Charles River
Japan (Kanagawa, Japan) for use in this study. The
animals were maintained in a room with a controlled
temperature (mean9/SD, 239/38C) and a light�dark
cycle of 14�10 h. The rats were housed in plastic
cages, with a maximum of three animals per cage.
Standard pelleted laboratory formula and tap-water
were provided ad libitum . All experiments were
approved by the Animal Research Committee of
Kawasaki Medical School (Study no. 03-049, 2003)
and conducted in accordance with the ‘‘Guide for
the Care and Use of Laboratory Animals’’ of
Kawasaki Medical School.
Induction of small intestinal damage
The rats were weighed, randomized to one of four
inhibitor-treated groups or the control group, and
then anesthetized with an intraperitoneal injection of
sodium amobarbital (100 mg/kg). A 6-cm-long plas-
tic catheter was inserted into the colon, and 24 mg/
kg indomethacin (Indo) (Sigma Chemical Co., St.
Louis, Mo., USA) dissolved with 1% sodium car-
boxymethylcellulose was injected via the catheter.
Intrarectal Indo administration was chosen for this
study, because this method consistently produces
ulcerations located predominantly in the small
intestine [15].
Serial change in small intestinal ulcerations and MMP
production during development intestinal injury
The rats were sacrificed at 6 h, 12 h, 24 h, 3 days,
and 7 day after Indo administration. The small
intestines were removed and assessed macroscopi-
cally and histologically by the methods described
below. MMP production and activities were assessed
by Western blotting, zymography, and immunohis-
tochemistry.
Treatment with a TACE or one of two selective MMP
inhibitors
All animals were killed for evaluation of small
intestinal damage and production of TNF-a,
TACE, MMP-3, MMP-9, and TIMP-1 24 h after
receiving indomethacin. The rats were divided into
five groups as follows: no treatment (control); Indo
administration alone; Indo plus 0.2, 1, 10, or 30 mg/
kg of a TACE inhibitor (GM6001, Galardin; Cal-
biochem, Darmstadt, Germany) diluted with di-
methyl sulfoxide (DMSO); Indo plus 0.2, 1, or
5 mg/kg selective MMP-3 inhibitor VI (sMMP3i,
TACE/MMP3 inhibitor improved experimental intestinal damage 1321
Scan
d J
Gas
troe
nter
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Lib
rary
Utr
echt
on
04/0
8/13
For
pers
onal
use
onl
y.

Calbiochem) diluted with DMSO; Indo plus 0.2, 1,
or 5 mg/kg MMP-9/13 inhibitor II (MMP9i, Calbio-
chem) diluted with DMSO. Inhibitors were injected
intraperitoneally 3 h after Indo administration.
Macroscopic and microscopic assessments of longitudinal
ulceration of the small intestine
The small intestine was removed, opened by long-
itudinal incision, pinned flat on a wax block, washed
with saline, and fixed in 10% formalin for 48 h.
Fixed specimens were examined macroscopically
and microscopically for small intestinal damage.
Longitudinal ulcers were defined as �/10 mm long,
located on the mesenteric side of the lumen. As
previously described [15], macroscopic ulcerations
were evaluated by an ulcer index (UI) defined as the
ratio of the total length of longitudinal ulcers in the
small intestine to the total length of the small
intestine from the pylorus to the ileocecal junction.
Ulcers that were smaller than 10 mm in largest
dimension were not included. Tissue samples were
removed from the ulcers for histologic examination
as paraffin sections by a histopathologist who was
kept unaware of the treatment groups. All sections
were stained with hematoxylin and eosin (H&E). For
histologic assessment, we used a histologic damage
score (HDS) according to the modified criteria
reported by Vilaseca et al. [17]. The width of
ulceration was scored according to the following
criteria: 0, no ulcer; 1, below 3 mm; 2, 3 to 6 mm;
and 3, above 6 mm. The depth of ulceration was
scored as: 0, none; 1, mucosa; 2, submucosa; 3,
muscularis propria; or 4, serosa. Inflammatory cell
infiltration was scored as: 0, none; 1, mild; 2,
moderate; or 3, severe. Thrombi were scored as: 0,
absent; 1, present.
Collection of samples of intestinal ulcers
Tissue samples including ulcerations in the middle
portion of the small intestine were collected for
determination of protein production and activities
using the enzyme-linked immunosorbent assay
(ELISA), Western blotting, zymography, and im-
munohistochemistry. These samples were obtained
immediately after the rats were killed by amobarbital
overdose, and then washed with phosphate-buffered
saline (PBS), frozen in liquid nitrogen, and stored at
�/808C.
ELISA for TNF-a analysis
As described in previous studies [18], tissue was
homogenized in nine volumes of Greenberger lysis
buffer (300 mM NaCl, 15 mM Tris-HCl (pH 7.4),
2 mM MgCl2, 2 mM Triton X-100, Pepstain A
(20 ng/ml), leupeptin (20 ng/ml), and aprotonine
(20 ng/ml)). Tissue was lysed for 30 min on ice
followed by two centrifugations at 14,000 g for
10 min each. Homogenates were stored at �/208Cuntil further use. TNF-a concentrations were mea-
sured by the ELISA (R&D Systems, Abingdon,
England).
Zymography for MMP activity
Zymography was carried out in tissue homogenates
and conditioned media in accordance with the
published methods [19,20]. Tissue samples were
homogenized in sample buffer (20 mM Tris-HCl
(pH 7. 5), 0.01% Briji-35). After centrifugation at
48C and 10,000g for 20 min, supernatants were
collected from the samples. Protein concentrations
were measured using a bicinchoninic acid (BCA)
method. All samples were then adjusted to a uniform
total protein concentration, and added to triple
volumes of sodium dodecyl sulfate (SDS) zymogra-
phy buffer (0.5 M Tris-HCl (pH 6.8), SDS, 70%
glycerol, and 5% bromophenol blue (BPB)). Pro-
teins were separated on 12.5% polyacrylamide gels
(Bio-Rad, Hercules, Calif., USA) under non-redu-
cing, non-denaturing conditions with 0.4% gelatin/
casein as substrate (Sigma). The gels were then
washed in buffer (50 mM Tris-HCl (pH 7.5), 0.1 M
NaCl, 2.5% Triton X-100) for 90 min, and incu-
bated in reaction buffer (1 M Tris-HCl (pH 7.5),
1 M CaCl2, 1 mM ZnCl2, 2% NaN3, 2 mM
o-phenanthroline, and 200 mM phenylmethanesulfo-
nyl fluoride) at 378C for 30 h. Thereafter, they were
fixed and stained in 45% methanol, 10% acetic acid,
and 0.1% Coomassie blue R-250 (Sigma) for 2 h
and finally decolorized. Bands were determined as
resulting from the activity of MMP as opposed to
that of other proteinases by experiments using MMP
inhibitors in reaction buffers.
The relative molecular weights of the bands were
estimated by comparison to both molecular weight
standards and the uniform amount of active human
MMP-2, -3, and -9 (Wako, Osaka, Japan). Band
analysis was performed with a Macintosh (model
G4) computer using the public domain NIH Image
program (developed at the US National Institute of
Health and available via the Internet by anonymous
FTP from zippy.nimh.nih.gov or on a floppy disk
obtained from the National Technical Information
Service (Springfield, Va., USA; part number PB95-
500195GEI). Zymographic activity was measured by
densitometric analysis in 1-D gels using an external
density standard (Kodak, Rochester, N.Y., USA)
and NIH Image 1.62. We defined protein produc-
tion in the control group as 100%. Typical zymo-
1322 H. Matsumoto et al.
Scan
d J
Gas
troe
nter
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Lib
rary
Utr
echt
on
04/0
8/13
For
pers
onal
use
onl
y.

graphy gel illustrating the MMPs positive control is
shown in Figure 1.
Western immunoblotting
The frozen samples were homogenized in sample
buffer (20 mM Tris-HCl (pH 7.5), and 0.01% Briji-
35). After total protein amounts were measured by
BCA and then made uniform, samples were added
to SDS buffer (125 mM Tris-HCl (pH 6.8), 4%
SDS, 20% glycerol, 10% 2-mercaptoethanol,
0.002% BPB, and 0.01% protein inhibitor cocktail
set V (EDTA-free, Calbiochem), and heated to
1008C for 5 min. For measurement of TACE, the
samples were then added to the buffer (0.2% Nondit
P40, 100 mM 1,10 � phenanthroline, and 1 mM
dithiothreitol), and incubated at 08C for 60 min.
Samples were loaded (10 mg/lane) onto 10�12.5%
polyacrylamide gels. After sodium dodecyl sulfate-
polyacrylamide gel electrophoresis (SDS-PAGE),
proteins were transferred onto a PVDF membrane
(Hybond-P, Amersham, England) and detected
using mouse anti-human MMP-3, -9 (4 mg/ml;
Daiichi Fine Chem., Takaoka, Japan), anti-TACE
(1:1000; Oncogene Res, San Diego, Calif., USA), or
anti TIMP-1 (1:500; Daiichi Fine Chem.); followed
by peroxidase-linked-anti-mouse IgG secondary
antibody. By means of an enhanced chemilumines-
cence (ECL) detection system (Amersham), mem-
branes were exposed to appropriate film (Hyperfilm
ECL; Amersham). Band analysis was performed on
the Macintosh computer using the public domain
NIH Image program. We defined MMP activity in
control group as 100%.
Immunohistochemistry
Deparaffinized 4-mm sections were stained immuno-
histochemically (streptoavidin-biotin method) using
mouse anti- human MMP-3, or -9 antibody (1:800).
These had been recognized as cross-reacting with
corresponding rat MMPs. Endogenous peroxidase
activity was blocked by incubation in 1% H2O2 for
30 min at room temperature. After microwave-oven
antigen retrieval, the specimens were exposed to
anti-MMP antibodies, and then to the secondary
antibody and color development reagents. Nuclei
were counterstained with hematoxylin. Immunor-
eactive cells were counted at six random points at
either the edge or central area of ulceration.
Statistical analysis
All values were expressed as the means9/SD. Com-
parisons between groups were made using Student’s
t-test; p-values of less than 0.05 were considered
significant. Statistical analysis was performed using
Graph Pad Prism (version 4.00 for Macintosh;
GraphPad Software, San Diego, Calif., USA).
Results
Serial change in intestinal ulcerations and MMP
production during development of Indo-induced intestinal
damage
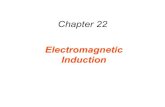
Both the UI and HDS were at their peak 24 h after
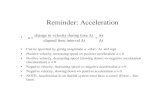
Indo administration (Figure 2A, B). MMP-3 pro-
duction and activities, assessed by Western blotting,
zymography, and immunohistochemistry were also
overexpressed at 24 h (Figure 3A, B, C, D), whereas
MMP-9 production and activities were not.
Both GM6001 and sMMP3i decreased the UI and
HDS dose-dependently, whereas MMP9i did not. In
the group treated with Indo alone, the UI and HDS
had respective values of 16.59/1.1 and 7.69/0.2
(Figure 4A, B). In the group treated with TACE
inhibitor, GM6001 significantly and dose-depen-
dently decreased both the UI and HDS. Using
GM6001 at the 30 mg/kg dose, no ulceration
occurred (UI, 0; HDS, 0.259/0.2), and we therefore
did not collect frozen samples or examine protein
production at 30 mg/kg of GM6001. sMMP3i also
had a beneficial effect, to almost the same degree as
GM6001, with a minimum UI of 1.09/0.3 and a
minimum HDS of 1.79/0.6 (5 mg/kg). Regarding
the HDS, the main effect of these two drugs was to
decrease the number of infiltrating inflammatory
cells (Figure 7A, B, C, D). In contrast, MMP9i did
not cause any significant decrease in either the UI or
HDS. Even the minimum UI and HDS levels were
still at 13.79/2.5 and 4.79/0.6.Figure 1. Typical zymography gel illustrating the standard of
matrix metalloproteinase (MMP).
TACE/MMP3 inhibitor improved experimental intestinal damage 1323
Scan
d J
Gas
troe
nter
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Lib
rary
Utr
echt
on
04/0
8/13
For
pers
onal
use
onl
y.

GM6001 dose-dependently suppressed produc-
tion of both TNF-a and TACE, whereas sMMP3i
did not. Production of both TNF-a and TACE in
the Indo alone group significantly increased beyond
production in the normal group. GM6001 sup-
pressed production in a dose-dependent manner
(Figure 5A, B). Minimum TNF-a and TACE
production rates in the GM6001-treated group
were 35% and 36.5%, respectively, at the 10-mg/kg
dose, when production in the Indo alone group was
defined as 100%. In contrast, sMMP3i did not
significantly suppress production (respective mini-
mum production rates, 68.7% and 90%).
Both GM6001 and sMMP3i down-regulated
MMP-3 activity and production, while up-regulating
TIMP-1 production. MMP-3 activity and production
in the Indo alone group increased significantly
beyond the finding in the normal group (Figure 6A,
Figure 2. Serial change in small intestinal ulcerations after indomethacin (Indo) administration. The ulcer index of the small intestine was
at its peak at 24 h after Indo administration (A). The histological damage score also was at its peak at 24 h after Indo administration (B).
*p B/0.01 versus control.
Figure 3. Serial change in matrix metalloproteinase (MMP) production of the small intestine after indomethacin (Indo) administration.
MMP-3 production assessed by Western blotting (A) and by zymography (B) was at its peak 24 h after Indo administration. In the
immunohistochemical assessment, the numbers of MMP-3 positive cells at the edge of the ulcer (C) and in the central area of the ulcer (D)
were also at their peak 24 h after Indo administration. *p B/0.01 versus MMP-3 control group, $p B/0.01 versus MMP-9 of control group.
1324 H. Matsumoto et al.
Scan
d J
Gas
troe
nter
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Lib
rary
Utr
echt
on
04/0
8/13
For
pers
onal
use
onl
y.

B, C). The maximum suppression by GM6001 was
99.5% and 99.1%, respectively, at the 10 mg/kg dose.
sMMP3i dose-dependently decreased MMP-3 activ-
ity and production to about the same degree as
GM6001. Maximum suppression was 85.1% and
99.5%, respectively, at the 5-mg/kg dose. GM6001
also dose-dependently down-regulated the produc-
tion and activity of MMP-9 (Figure 6D, E, F). In
contrast, there was no significant suppression with
sMMP3i. Both GM6001 and sMMP3i dose-depen-
dently up-regulated TIMP-1 production, with their
respective maximum values in the groups treated with
GM6001/sMMP3i being 22 and 31 times greater
than those in the normal group (data not shown).
Thus, the inhibitors changed the MMP-3/TIMP-1
balance to the degree that it resembled that in the
normal intestine. In addition, these drugs signifi-
cantly and dose-dependently decreased the number
of MMP-3- but not MMP-9- immunoreactive cells
both in the center and at the edge of the ulcerations.
MMP9i suppresses MMP-9 production, but not that of
TNF-a, TACE, MMP-3, or TIMP-1
MMP9i suppressed MMP-9 production, decreasing
the number of MMP-9-immunoreactive cells in the
center of the ulcerations, but had no effect on other
cytokines and MMP production. These findings do
not resemble those observed after treatment with
TACE inhibitor or sMMP3i (data not shown).
Discussion
Based on three observations made in this study, we
postulate that MMP-3 could be just as important as
the TACE and/or TNF-a protein in treating small
Figure 4. Effects of three inhibitors on indomethacin-induced intestinal ulceration. A. The macroscopic assessment ulcer index (UI); B.
microscopic assessment, and the histologic damage score (HDS). In the group treated with the tumor necrosis factor-a-converting enzyme
inhibitor (TACEi), GM6001 significantly decreased both UI and HDS in a dose-dependent manner. Selective matrix metalloproteinase-3
inhibitor (sMMP3i) ameliorated this enteropathy to a similar degree. Matrix metalloproteinase-9 inhibitor (MMP9i) did not have any
beneficial effect against intestinal ulceration. *p B/0.01 versus control, **p B/0.01 versus Indo alone.
Figure 5. TNF-a- and TNF-a-converting enzyme (TACE) production in intestinal ulcerative tissues treated with GM6001 and sMMP3i.
A. Concentration of TNF-a; B. Production of TACE. GM6001 significantly suppressed production of both TNF-a and TACE in a dose-
dependent manner; sMMP3i did not suppress either TNF-a or TACE. *p B/0.01 versus control, **p B/0.01 versus Indo alone, %%p B/0.05
versus Indo alone.
TACE/MMP3 inhibitor improved experimental intestinal damage 1325
Scan
d J
Gas
troe
nter
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Lib
rary
Utr
echt
on
04/0
8/13
For
pers
onal
use
onl
y.

intestinal damage with TACE/MMP inhibitors.
First, it was found that MMP-3 was involved in
the development of intestinal damage following Indo
administration. Second, two effective inhibitors
against this experimental injury, sMMP3i and a
TACE inhibitor, showed MMP-3 suppression. We
found that the TACE inhibitor, GM6001, along with
sMMP3i had a beneficial effect against this intestinal
injury, but not with MMP9i. Interestingly, the
efficacy of sMMP3i was equal to that of GM6001
in terms of longitudinal ulcerations of the small
intestine. These two effective drugs, sMMP3i and
the TACE inhibitor, had two effects in common
against experimental injury, but differed with respect
to another two. The common effects in this entero-
pathy were dose-dependent MMP-3 suppression
Figure 6. Matrix metalloproteinase (MMP) production and activities in intestinal ulcerative tissue treated with GM6001 or sMMP3i:
MMP-3 production (A, B, C): MMP-9 production (D, E, F). GM6001 significantly suppressed both production and activities of MMP-3
and MMP-9 in a dose-dependent manner. In contrast, sMMP3i dose-dependently suppressed only MMP-3, not MMP-9. MMP-9
production in the presence of these inhibitors was not decreased from that in the Indo alone group.
Figure 7. Histologic appearance of ulceration of the small intestine (H&E). Indomethacin-induced longitudinal ulceration of the small
intestine (A). Intestinal tissue treated with GM6001 at 30 mg/kg (B). Intestinal tissue treated with sMMP3i at 5 mg/kg (C). Intestinal
ulceration treated with MMP9i at 5 mg/kg (D).
1326 H. Matsumoto et al.
Scan
d J
Gas
troe
nter
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Lib
rary
Utr
echt
on
04/0
8/13
For
pers
onal
use
onl
y.

and TIMP-1 up-regulation. Differences involved
TNF-a and TACE production; GM6001, the
TACE inhibitor, suppressed the production of both
TNF-a and TACE, while sMMP3i did not suppress
production of either. Finally, an ineffective inhibitor,
MMP9i, show no MMP-3 suppression.
In the near future, small intestinal ulceration could
become a common gastrointestinal disease, because
the incidence of small intestinal damage that could
be induced mainly by NSAIDs and Crohn’s disease
(CD) could clinically increase [21,22]. Interestingly,
the small intestinal damage has been characterized
almost entirely by TH-1-dominant inflammation.
New methods of direct visualization of the small
bowel using a capsule or double-balloon endoscopy
have been developed and could also contribute to
making small intestinal ulceration more common
hereafter [23,24]. However, we have found very few
studies regarding a novel treatment for experimental
small intestinal ulcerations. Furthermore, there have
been no studies comparing the effectiveness of some
TACE/MMP inhibitors against intestinal damage.
The present study presents new information on the
effectiveness of three TACE/MMP inhibitors against
small intestinal damage.
Some studies have suggested that either MMP-3 or
MMP-9 is related to intestinal inflammation
[9,19,20,25,26]. However, there has been no evi-
dence to show MMPs, especially MMP-3 or MMP-
9, to be more important in intestinal damage and a
more effective therapeutic target MMP against in-
testinal damage. However, production of MMP-3
and/or MMP-9 has been reported to be greater in the
inflamed colonic mucosa of patients with CD than in
normal mucosa. In fetal intestinal tissue, the balance
of which resembles the immune balance in CD,
blockade of TNF-a decreased production of MMP-
3 [27]. In a study on IBD, inflammatory cytokines
such as TNF-a and IL-1b up-regulated MMP-3
production by monocytes which increased in number
in the submucosal layer [27]. TNF-a down-regulates
production of TIMP-1 that is a natural inhibitor of
MMP-3 [28]. Heuschkel et al. [19] described colonic
mucosal lesions in human IBD as showing MMP-3/
TIMP-1 imbalance. Baugh et al. [20], on the other
hand, showed that MMP-9 levels were elevated in
human IBD. However, our data might support the
hypothesis that MMP-3 is as important a protein as
TNF-a in treating TH-1-dominant intestinal inflam-
mation, although there is a difference between the
large intestine and small intestine.
In the present study, we used a TACE inhibitor,
GM6001, and two selective MMP inhibitors,
sMMP3i and MMP9i. GM6001 inhibited broad-
spectrum MMPs, MMP-1, -2, -3, -8, and -9, and
blocked the release of TNF-a [29]. Two selective
inhibitors have been shown to produce specificity
inhibition against, respectively with low concentra-
tions [30,31]. They might not have specific without
any cross-inhibition of MMP or TACE.
sMMP3i, 4-(4?-Biphenyl)-4-hydroxyaminobutyric
acid, is a potent and competitive inhibitor of MMP-
3, and no cross-inhibition has ever been reported in
rats. The functional groups, the oxime and carboxyl
groups, have been shown to interact with the active
site zinc of MMP. MMP9i, N-hydroxy-1-(4-
methoxyphenyl) sulfonyl-4-benzyloxycarbonylpiper-
azine-2-carboxamide, is a piperazine-based potent
inhibitor of MMP-9 (IC50�/1.9 nM) and MMP-13
(IC50�/1.3 nM). It inhibits MMP-1 and MMP-3 at
higher concentrations (IC50�/24 nM and 18 nM,
respectively). In this study, we ascertained that both
MMP3 production and TACE production were not
decreased significantly when high dosages of MMP9i
were used against experimental damage. These
results seem to confirm the evidence that MMP3
could be more effective than MMP9, TNF-a, and
TACE.
MMP-3 plays a central role in the MMP cascade
pathway and is a key enzyme that controls other
MMPs [7]. It is impossible to inhibit an MMP
enzyme alone with an MMP inhibitor, because the
MMP family has a cascade pathway that is activated
by any one of its members. MMP-3 suppression
could naturally cause other MMP suppression.
Therefore specificity against MMP-3 is lost in these
TACE/MMP inhibitors at high doses. In other
words, MMP-3 has powerful effects on the MMP
cascade pathway and could be an effective therapeu-
tic target against intestinal ulceration. This study
demonstrated that two effective inhibitors against
experimental injury, sMMP3i and a TACE inhibitor,
showed MMP-3 suppression. To study MMP-3
function, more specifically TACE/MMP production
needs to be evaluated using MMP-3 KO mice. In
addition, it is necessary to evaluate other MMP
production, especially that of MMP-7 and MMP-
12, as MMP-7 plays an immunodefensive role in the
colon, and MMP-12 is also associated with macro-
phages [7].
TACE has been of interest in the treatment of
inflammatory diseases characterized by TH-1-domi-
nant inflammation, where the key cytokine is TNF-a(examples: CD, rheumatoid arthritis) [4�6,28] be-
cause it is responsible for cleavage of transmem-
brane-domain-anchored TNF-a. Transmembrane
TNF, not soluble TNF, could be the critical form
of TNF for TNF signaling in IBD, because etaner-
cept, which binds only soluble TNF, was shown to
be ineffective in the treatment of moderate to severe
CD [32,33]. Transmembrane TNF, which was
mediated by TACE, was a potent inducer of the
TACE/MMP3 inhibitor improved experimental intestinal damage 1327
Scan
d J
Gas
troe
nter
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Lib
rary
Utr
echt
on
04/0
8/13
For
pers
onal
use
onl
y.

CD4CD45RBhi T-cell transfer model of colitis even
in the absence of its secreted form [34]. Another
TACE inhibitor (BB1101) also had a beneficial
effect in an experimental model of colitis [28,35].
In a clinical study of IBD, TACE activity was shown
to be up-regulated in inflamed colonic mucosal [36].
In our study, while the tested TACE inhibitor was
found to down-regulate TNF release as expected, it
was not anticipated that the inhibitor would also
down-regulate the production of TACE. There is a
possible explanation for this unexpected result;
down-regulation of TNF-a might cause down-reg-
ulation of the TACE protein. While Bzowska et al.
[37] reported that stimulation with TNF-a results in
increased levels of TACE mRNA and protein
expression, they showed that the increase in TACE
was accompanied by increased shedding of TNF
receptor in TNF-a-stimulated endothelial cells.
However, since we lack data on changes in TACE
expression being stimulated by TNF-a in intestinal
cells, future investigation is required.
Recently, Brynskov et al. [36] reported that
ulcerative colitis (TH-2-dominant inflammation)
showed a larger increase in TACE expression in
inflamed human colonic mucosa than that seen in
CD (TH-1-dominant inflammation). They tenta-
tively linked this unexpected result to inactivation
of TACE activity in CD mucosa catalyzed by other
MMPs as part of a self-regulatory mechanism.
Another possible explanation for these differences
in expression could be due to differences in the
production of TIMP-3, which inhibits TACE, in
inflammation. Only TIMP-3, as opposed to other
TIMPs, has been shown to inhibit TACE [38].
Overexpression of TIMP-3 has been reported in
ulcerations of the intestine [39]. Therefore, the
effects of the balance of TACE with that of TIMP-
3 and/or that of MMP-3 with TIMP-3 in inflamma-
tion and ulceration need to be investigated.
Pro-inflammatory cytokines could be involved in
the production of MMPs during the development of
intestinal injury. TNF-a is linked with NSAIDs, for
example Indo-induced intestinal injury in the rat
[14,16,40,41]. We previously reported that admin-
istration of anti-TNF-a, IL-6, and IL-1b neutraliz-
ing antibodies significantly ameliorated this
experimental enteropathy in a dose-dependent fash-
ion [14]. The maximum suppressive rates of UI by
these antibodies were respectively 43.0%, 49.6%,
and 59.7%. In addition, inhibition of enteropathy
with a combination of the three antibodies reached
up to 87.5%. In the present study, GM6001
completely abolished intestinal ulceration in parallel
with both 56% suppression of TNF-a and complete
suppression of MMP-3. Therapy with anti-TNF-ain patients with rheumatoid arthritis resulted in
decreased serum MMP-3 concentrations [42]. How-
ever, since we lack data concerning changes in
MMP-3 in CD patients treated with anti-TNF-aneutralizing antibodies or other therapies, future
investigation is required.
In summary, sMMP3i showed the same degree of
therapeutic effect as TACE inhibitor in Indo-
induced small intestinal damage in the rat, involv-
ing suppression of MMP-3. On the other hand,
MMP9i had no therapeutic effect on this entero-
pathy despite suppression of MMP-9. The TACE-
TNF-a-MMP-3/TIMP-1 network may be an
important inflammatory pathway in this experimen-
tal intestinal inflammation.
Acknowledgements
This study was a supported by a Grant-in-Aid (No.
13670574) for Scientific Research from the Ministry
of Education, Science and Culture, Japan. Further
funding was given through a gastrointestinal disease
grant from the Specially Selected Disease Project of
the Ministry of Health and Welfare of Japan, and a
Project Grant (No. 12-409) from Kawasaki Medical
School.
References
[1] Beutler BA. The role of tumor necrosis factor in health and
disease. J Rheumatol 1999;/Suppl 57:/16�21.
[2] Black RA, Rauch CT, Kozlosky CJ, Peschon JJ, Slack JL,
Wolfson MF, et al. A metalloproteinase disintegrin that
releases tumour-necrosis factor-alpha from cells. Nature
1997;/385:/729�33.
[3] Moss ML, Jin SL, Milla ME, Bickett DM, Burkhart W,
Carter HL, et al. Cloning of disintegrin metalloproteinase
that processes precursor tumour-necrosis factor-a. Nature
1997;/385:/733�5.
[4] Bazzoni F, Beutler B. The tumor necrosis factor ligand and
receptor families. N Engl J Med 1996;/334:/1717�25.
[5] van Deventer SJ. A place of TACE. Gut 2002;/51:/5�6.
[6] Shanahan F. Inflammatory bowel disease: immunodiagnos-
tics, immunotherapeutics, and ecotherapeutics. Gastroenter-
ology 2001;/120:/622�35.
[7] Park WC, Wilson CL, Lopez-Boado YS. Matrix metallo-
proteinases as modulators of inflammation and innate
immunity. Nat Rev Immunol 2004;/4:/617�29.
[8] Schuppan D, Hahn EG. Matrix metalloproteinases in the
gut: inflammation hits the matrix. Gut 2000;/47:/12�4.
[9] von Lampe B, Barthel B, Coupland SE, Riecken EO,
Rosewicz S. Differential expression of matrix metalloprotei-
nases and their tissue inhibitors in colon mucosa of patients
with inflammatory bowel disease. Gut 2000;/47:/63�73.
[10] Coussens LM, Fingleton B, Matrisian LM. Matrix metallo-
proteinase inhibitors and cancer: trials and tribulations.
Science 2002;/295:/2387�92.
[11] Matsumoto T, Iida M, Kuroki F, Hizawa K, Koga H,
Fujishima M. Effect of diet on experimentally induced
intestinal ulcer in rats: morphology and tissue leukotrienes.
Gut 1994;/35:/1058�63.
[12] Matsumoto T, Iida M, Nakamura S, Hizawa K, Kuroki F,
Fujishima M. Preventive effect of immunosuppressive agents
1328 H. Matsumoto et al.
Scan
d J
Gas
troe
nter
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Lib
rary
Utr
echt
on
04/0
8/13
For
pers
onal
use
onl
y.

against indomethacin-induced small intestinal ulcers in rats.
Dig Dis Sci 1994;/39:/787�95.
[13] Koga H, Aoyagi K, Matsumoto T, Iida M, Fujishima M.
Experimental enteropathy in athymic and euthymic rats:
synergistic role of lipopolysaccharide and indomethacin. Am
J Physiol (Gastrointest, Liver Physiol) 1999;/276:/G576�82.
[14] Tarumi K. Essential role of macrophages and macrophage-
related proinflammatory cytokines in indomethacin-induced
enteropathy in rats [English abstract in Japanese article].
Kawasaki Igakkaishi 2002;/28:/243�56.
[15] Matsumoto T, Iida M, Nakamura S, Kuroki F, Hizawa K,
Fujishima M. An animal model of longitudinal ulcer in the
small intestine induced by intracolonically administrated
indomethacin in rats. Gastroenterol Jpn 1993;/28:/10�7.
[16] Anthony A, Pounder RE, Dhillon AP, Wakefield AJ.
Similarities between ileal Crohn’s disease and indomethacin
experimental jejunal ulcers in the rat. Aliment Pharmacol
Ther 2000;/14:/241�5.
[17] Vilaseca J, Salas A, Guarner F, Rodriguez R, Malagelada JR.
Participation of thomboxane and other eicosanoid synthesis
in the course of experimental inflammatory colitis. Gastro-
enterology 1990;/98:/269�77.
[18] Lindsay J, Van Montfrans C, Brennan F, Van Devenrer S,
Drillenburg P, Hodgson H, et al. IL-10 gene therapy pre-
vents TNBS-induced colitis. Gene Ther 2002;/9:/1715�21.
[19] Heuschkel RB, MacDonald TT, Montelone G, Bajaj-Elliott
M, Smith JA, Pender SL. Imbalance of stromelysin-1 and
tissue inhibitor of matrix metalloproteinase (TIMP)-1 in the
mucosal lesions of children with inflammatory bowel disease.
Gut 2000;/47:/57�62.
[20] Baugh MD, Perry MJ, Hollander AP, Davies DR, Cross SS,
Lobo AJ, et al. Matrix metalloproteinase levels are elevated
in inflammatory bowel disease. Gastroenterology 1999;/117:/
814�22.
[21] Garcia Rodriguez LA. Variability in risk of gastrointestinal
complications with different nonsteroidal anti-inflammatory
drugs. Am J Med 1998;/104:/30S�4.
[22] Loftus EV Jr. Clinical epidemiology of inflammatory bowel
disease: incidence, prevalence, and environmental influ-
ences. Gastroenterology 2004;/126:/1504�17.
[23] Iddan G, Meron G, Glukhovsky A, Swain P. Wireless
capsule endoscopy. Nature 2000;/405:/417.
[24] Yamamoto H, Yano T, Kita H, Sunada K, Ido K, Sugano K.
New system of double-balloon enteroscopy for diagnosis and
treatment of small intestinal disorders. Gastroenterology
2003;/125:/1556�7.
[25] Kirkegaard T, Hansen A, Bruun E, Bryskov J. Expression
and localization of matrix metalloproteinases and their
natural inhibitors in fistulae of patients with Crohn’s disease.
Gut 2004;/53:/701�9.
[26] McKaig BC, McWilliam D, Watoson SA, Mahida YR.
Expression and regulation of tissue inhibitor of matrix
metalloproteinase-1 and matrix metalloproteinase by intest-
inal myofibroblasts in inflammatory bowel disease. Am J
Pathol 2003;/162:/1355�60.
[27] Pender SL, Tikle SP, Docherty AJ, Howie D, Wathen NC,
MacDonald TT. A major role of matrix metalloproteinases
in T cell injury in the gut. J Immunol 1997;/158:/1582�90.
[28] Colon AL, Menchen LA, Hurtado O, De Cristobal J,
Lizasoain I, Leza JC, et al. Implication of TNF-alpha
convertase (TACE/ADAM17) in inducible nitric oxide
synthase expression and inflammation in an experimental
model of colitis. Cytokine 2001;/16:/220�6.
[29] Galardy RE, Grobelny D, Foellmer HG, Fernandez LA.
Inhibition of angiogenesis by the matrix metalloprotease
inhibitor N-[2R-2-(hydroxamidocarbonymethyl)-4-methyl-
pentanoyl]]-L-tryptophan methylamide. Cancer Res 1994;/
54:/4715�8.
[30] Johnson LL, Bornemeier DA, Janowicz JA, Chen J, Pav-
lovsky AG, Ortwine DF. Effect of species differences on
stromelysin-1 (MMP-3) inhibitor potency. An explanation of
inhibitor selectivity using homology modeling and chimeric
proteins. J Biol Chem 1999;/274:/24881�7.
[31] Cheng M, De B, Almstead NG, Pikul S, Dowty ME,
Dietsch CR, et al. Design and synthesis of piperazine-based,
matrix metalloproteinase inhibitors. J Med Chem 1999;/42:/
2295�314.
[32] van Deventer SJ. Transmembrane TNF-alpha, induction of
apoptosis, and the efficacy of TNF-targeting therapies in
Crohn’s disease. Gastroenterology 2001;/121:/1242�6.
[33] Sandborn WJ, Hanauer SB, Katz S, Safdi M, Wolf DG,
Baerg RD, et al. Etanercept for active Crohn’s disease: a
randomized, double-blind, placebo-controlled trial. Gastro-
enterology 2001;/121:/1088�94.
[34] Corazza N, Brunner T, Buri C, Rihs S, Imboden MA,
Seibold I, et al. Transmembrane tumor necrosis factor is a
potent inducer of colitis even in the absence of its secreted
form. Gastroenterology 2004;/127:/816�25.
[35] Sykes AP, Bhogal R, Brampton C, Chander C, Whelan C,
Parsons ME, et al. The effect of an inhibitor of matrix
metalloproteinases on colonic inflammation in a trinitroben-
zenesulphonic acid rat model of inflammatory bowel disease.
Aliment Pharmacol Ther 1999;/13:/1535�42.
[36] Brynskov J, Foegh P, Pedersen G, Ellervik C, Kirkegaard T,
Bingham A, et al. Tumor necrosis factor-alpha converting
enzyme (TACE) activity in the colonic mucosa of patients
with inflammatory bowel disease. Gut 2002;/51:/37�43.
[37] Bzowska M, Jura N, Lassak A, Black RA, Bereta J. Tumour
necrosis factor-a stimulates expression of TNF-a converting
enzyme in endothelial cells. Eur J Biochem 2004;/271:/2808�20.
[38] Amour A, Slocombe PM, Webster A, Butler M, Knight CG,
Smith BJ. TNF-alpha converting enzyme (TACE) is inhib-
ited by TIMP-3. FEBS Lett 1998;/435:/39�44.
[39] Vaalamo M, Karjalainen-Lindberg ML, Saarialho-Kere U.
Distinct expression profiles of stromelysin-2 (MMP-10),
collagenase-3 (MMP-13), macrophage metalloelastase
(MMP-12), and tissue inhibitor of MMP-3 (TIMP-3) in
intestinal ulceration. Am J Pathol 1998;/152:/1005�14.
[40] Bertrand V, Guimbaud R, Tulliez M, Mauprivez C, Sogni P,
Couturier D, et al. Increase in tumor necrosis factor-aproduction linked to the toxicity of indomethacin for the
rat small intestine. Br J Pharmacol 1998;/124:/138594.
[41] Reuter BK, Wallace JL. Phosphodiesterase inhibitors prevent
NSAID enteropathy independently of effects on TNF-arelease. Am J Physiol (Gastrointest, Liver Physiol) 1999;/40:/
G847�54.
[42] Catrina AI, Lampa J, Ernestam S, af Klint E, Bratt J,
Klarekog L, et al. Anti-tumour necrosis factor (TNF)-alpha
therapy (etanercept) down-regulates serum matrix metallo-
proteinase (MMP)-3 and MMP-1 in rheumatoid arthritis.
Rheumatology 2002;/41:/484�9.
TACE/MMP3 inhibitor improved experimental intestinal damage 1329
Scan
d J
Gas
troe
nter
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Lib
rary
Utr
echt
on
04/0
8/13
For
pers
onal
use
onl
y.