Beta 2 agonists
79
BETA 2-AGONISTS Piyawadee Lertchanaruengrith, MD 30/09/2011
-
Upload
chulalongkorn-allergy-and-clinical-immunology-research-group -
Category
Health & Medicine
-
view
17 -
download
2
description
Beta 2 agonists Presented by Piyawadee Lertchanaruengrith, MD. 20110930
Transcript of Beta 2 agonists

BETA 2-AGONISTS
Piyawadee Lertchanaruengrith, MD
30/09/2011

Topic outlines
Structure & Function Relationship Non-bronchodilator Actions of β2–
Adrenergic Agonist Clinical Applications Safety issues β2–Adrenergic Agonist in Asthma
Guidelines

Structure & Function Relationship

Classification of β2-agonists
Ephedrine Epinephrine Isoproterenol
Short-acting non-selective: Metaproterenol, Fenoterol
Short-acting selective: Albuterol, Terbutaline
Long-acting selective: Formoterol, Salmeterol, Arformoterol, Carmoterol, Indacaterol
CATECHOLAMINE NON-CATHECHOLAMINE
Sorkness CA. In Middleton’s Allergy: Principles and Practice; 2009:1485-1503.

Modification of 3,4- hydroxyl
group on benzene ring
Prolonged bronchodilator
action
Sorkness CA. In Middleton’s Allergy: Principles and Practice; 2009:1485-1503.

Increasing the bulk of side chain
β2-adrenergic specificity
Increasing duration
of bronchodilation
Sorkness CA. In Middleton’s Allergy: Principles and Practice; 2009:1485-1503.

β2-adrenoreceptor
Long arm of chromosome 5
G protein-coupled receptors
Distribution Widely distributed in lung,
with high levels in central lung and alveolar region
Airway smooth muscle, epithelial cells, endothelial cells, type II cells
Mast cell, eosinophil, monocyte, alveolar macrophage, dendritic cells Johnson M. JACI 2006;117:18-24.

Intracellular signaling pathway
Johnson M. JACI 2006;117:18-24.
GTP
ATP
Phosphorylate keyregulatory proteins
that control muscle tone
-Inhibition of Ca2+ release from intracellular store-Reduction of membrane Ca2+ entry-Sequestration of intracellular Ca2+
Relaxation of airway smooth muscle

Mechanisms of Actions
Johnson M. Paediatric respiratory reviews 2001;2:57-62.

Summary of Structure and Function Relationship
ALBUTEROL FORMOTEROL SALMETEROL
Lipophilicity Hydrophilic Moderatelylipophilic
Most lipophilic
Onset of action Fast Fast Delayed
Duration of action Short Long Long
β2-agonist potency(Efficacy & receptor affinity)
Partial agonist(= Terbutaline)
Full agonist(= Isoproterenol, Fenoterol)
Partial agonist(Less than albuterol)
Mechanism of action
Accesses active site directly from the aqueous extracellular compartment
Forms a depot in cell membrane and progressively leach out (Duration-dose dependent)
Rapidly diffuses into cell membrane to active siteExosite(Duration-dose independent)
Sorkness CA. In Middleton’s Allergy: Principles and Practice; 2009:1485-1503.

Summary of Pharmacologic Attributes of Selected β2-agonists
β2-agonists Selectivity ratio(β1:β2
receptors)
Onset of action
(minutes)
Duration of action(hours)
Isoprenaline 1:1 2-5 < 20 minutes
Albuterol 1:1375 2-3 4-6
Fenoterol 1:120 2-4 4-6
Terbutaline nd 2-4 4-6
Salmeterol 1:85000 30 > 12
Formoterol 1:120 2-3 > 12
Sorkness CA. In Middleton’s Allergy: Principles and Practice; 2009:1485-1503.

Non-bronchodilator Actions of β2–Adrenergic Agonist

Non-bronchodilator actions
1. Increased mucociliary clearance - Increased ion & water secretion, ciliary beat frequency
- “Conflicting data; ? Clinical importance”
2. Suppression of microvascular permeability - 16 normal subjects histamine inhalation followed by sputum induction
by 4.5% hypertonic saline inhalation formoterol 18 mcg or placebo sputum β2-macroglobulin
- At 30 minutes after formoterol, the effect of histamine was reduced by 50% compared with placebo.
3. Inhibition of cholinergic neurotransmission
4. Protection of respiratory epithelium against bacteria
Sorkness CA. In Middleton’s Allergy: Principles and Practice; 2009:1485-1503.

Non-bronchodilator actions
5. Inhibition of mediator release: basophil, mast cell, lung tissue
- In vitro: Salmeterol blocks release of histamine, LTC4, LTD4, PGD2 from normal human lung tissues which were sensitized by serum of allergic donors
- In vitro: Salmeterol blocks TNF- α from human skin mast cell
6. Inhibition of function: - Eosinophil – In vitro: Salmeterol reduces plasma ECP after allergen
challenge
- Macrophage/DC - In vitro: Salbutamol inhibits production of IL-12
- T lymphocyte – In vitro: Salmeterol inhibits production of IFN-γ & IL-4
- Bronchial epithelial cells – In vitro: Formoterol + Budesonide inhibit production of GM-CSF & IL-8
* However, SABA & LABA should not be replaced ICS in terms of anti-inflammatory action *Sorkness CA. In Middleton’s Allergy: Principles and Practice; 2009:1485-1503.

Non-bronchodilator actions7. Priming the glucocorticoid receptor - Mitogen-activated protein kinases (MAPKs) pathway – result of
prolonged stimulation of β2–adrenergic receptor
Barnes PJ. Eur Respir J 2007;29:587-95.

β2-receptor Desensitization
Down-regulation of receptor after constant association with agonist molecule
Autoregulatory process Develops over days or weeks
Mechanisms Uncoupling of receptor from adenylate cyclase Internalization of uncoupled receptor Downregulation
Johnson M. JACI 2006;117:18-24.

β2-receptor Desensitization
Johnson M. JACI 2006;117:18-24.

β2-receptor Desensitization
Downregulation A net loss of cellular receptors Several mechanisms that are independent
of receptor phosphorylation receptor degradation
Transcription of β2–receptor gene is required to restore the membrane receptor
Hours of agonist exposure
Johnson M. JACI 2006;117:18-24.

β2-receptor Desensitization
Effects of β2-receptor Desensitization Decreased in unwanted receptor
stimulation Tremor: decreases after 2 weeks Palpitation Hyperglycemia, hypokalemia
? Loss of bronchodilator response
Johnson M. JACI 2006;117:18-24.

Objective: To determine whether regular use of salmeterol reduces the emergency effectiveness of albuterol
Patient ≥ 17 years, asthma with acute attack, 2 groups (match)1. Using salmeterol for chronic asthma control (57)2. Not using salmeterol for chronic asthma control (57)
Intervention & control
1st : Albuterol 2.5 mg NB every 20 minutes x 3 doses (33 each)2nd: Albuterol 5.0 mg NB every 20 minutes x 3 doses (24 each)
Primary outcome
Change of PEF % predicted before & after each aerosol
Salmeterol
Korosec M, et al. Am J Med 1999; 107:209-13.

39%
58%
46% 62%
Salmeterol vs controlP = 0.37
Korosec M, et al. Am J Med 1999; 107:209-13.
P < 0.001
P = 0.13
Salmeterol vs controlP = 0.81

FACET
Pauwels RA, et al. NEJM 1997;337:1405-11.
Objective: To evaluate the effects of adding inhaled formoterol to both lower and higher doses of the inhaled glucocorticoid budesonide
Patient 852 patients with asthma (FEV1 at baseline ≥ 50%) at least 6 months, 18-70 years, treat with ICS
Intervention & control
Run-in period: BUD 800 µg BID x 4 wkRandom to 4 groups:1. BUD 100 µg BID x 1 year2. BUD 100 µg BID + Formoterol 12 µg BID x 1 year3. BUD 400 µg BID x 1 year4. BUD 400 µg BID + Formoterol 12 µg BID x 1 year
Primary outcome
Rates of severe and mild exacerbations of asthma per patient per year
Formoterol

• Formoterol groups, am PEF was higher during the first days of treatment than subsequently (i.e., after day 3; P <.001)• ? Limited tolerance to bronchodilating effect of formoterol during theearly phase of regular treatment little or no clinical significance.
Pauwels RA, et al. NEJM 1997;337:1405-11.

LABAs: Desensitization
Occurs in Formoterol, but not Salmeterol
FACET study Little or no clinical significance ICSs did not prevent tolerance
Hypothesis? Agonist occupancy: Full (Formoterol), Partial
(Salmeterol) Salmeterol may maintain functional –receptor
through persistent elevation of gene transcription.
Sorkness CA. In Middleton’s Allergy: Principles and Practice; 2009:1485-1503.

Clinical Applications

Clinical Applications
SABAs Regular schedule or as-needed
LABAs Monotherapy or combination with ICSs Reduction or stop ICSs if LABAs were added Add-on LABAs or double dose ICSs ICS + LABAs or ICS + Montelukast

Objective: To compare the effects of regularly scheduled use of inhaled albuterol with those of albuterol used only as-needed
Patient 255 mild asthma patients (12-55 years, FEV1 ≥ 70%, PC20 ≤ 16 mg/ml), no ICS for 6 weeks
Intervention & Control
Run-in period: no ICS x 6 weeks
Albuterol MDI 2 puff qid daily (µg/d) + as-needed x 16 weeks (126/116)Placebo MDI 2 puff qid daily + Albuterol as-needed x 16 weeks (129/114)
Withdrawal period: Placebo X 4 weeks
Primary outcome
Morning peak expiratory flow
BAGS
Drazen JM et al. NEJM 1996;335:841-7.

Morning PEF did not change significantly during the treatment period in the scheduled or the as-needed treatment groups (P = 0.71)
Drazen JM et al. NEJM 1996;335:841-7As-needed use

LABA Monotherapy vs Continued Therapy With ICS in Patients With Persistent Asthma: A Randomized Controlled Trial SOC
Lazarus SC, et al. JAMA 2001;285:2583-93
Objective: To examine the effectiveness of salmeterol as replacement therapy in patients whose asthma is well controlled by low-dose TA
Patient 164 patients, 12-65 years, well controlled persistent asthma (FEV1 > 80%, PEF variability ≤ 20%) during a 6-week run-in period of treatment with TA 400 µg BID
Intervention 1. Triamcinolone MDI 400 µg BID X 16 weeks (54)2. Salmeterol MDI 42 µg BID X 16 weeks (54)
Control Placebo MDI 2 puffs BID X 16 weeks (56)
Primary outcome
Change in morning PEF from the final week of the run-in period (week 6) to the final week of the randomized treatment period(week 22).

AM PEF, increased in salmeterol and triamcinolone groupsand decreased initially then increased in placebo group
(no statistically significant differences either within or among 3 groups)
Lazarus SC, et al. JAMA 2001;285:2583-93

P=.004
P=.29
P=.001 P=.003
P=.04
Lazarus SC, et al. JAMA 2001;285:2583-93
Salmeterol group had more treatment failures and asthma
exacerbations than the triamcinolone group
P=.18

Greater increases in median sputum eosinophils
Patients with well-controlled persistent asthma by low doses of
TA cannot be switched to salmeterol monotherapy without risk of clinically significant loss of
asthma control
Lazarus SC, et al. JAMA 2001;285:2583-93
2.4%[0.0-10.6%]
−0.1%[−0.7% - 0.3%]
P = .001
Monotherapy could not berecommended in persistent
asthma

ICS Reduction and Elimination in Patients WithPersistent Asthma Receiving Salmeterol
SLIC
Objective: To determine whether ICS can be reduced or eliminated in patients with persistent asthma after adding LABA
Patient: 175 patients, 12-65 years with persistent asthma that was uncontrolled (FEV1 ≤ 80%, PEF variability >20%) during a 6-week run-in period of treatment with TA 400 µg BID
Intervention & Control
Salmeterol induction phase (2 wk)1. TA 400 µg BID + Placebo BID (21) Group I2. TA 400 µg BID + Salmeterol 42 µg BID(154) Group II
TA Reduction Phase (8 wk)1. Group I: TA 200 µg BID + Placebo BID (19) Placebo-minus2. Group II: TA 400 µg BID + Salmeterol 42 µg BID (74) Salmeterol-
plus3. Group II: TA 200 µg BID + Salmeterol 42 µg BID (74) Salmeterol-
minus
TA Elimination Phase (8 wk)1. Placebo-minus: Placebo TA + Placebo (18)2. Salmeterol-plus: TA 400 µg BID + Salmeterol 42 µg BID (71)3. Salmeterol-minus: Placebo TA + Salmeterol 42 µg BID (71)
Primary outcome: Time to asthma treatment failure in patients receiving salmeterol
Lemanske RF, Jr, et al. JAMA 2001;285;2594-603.

Lemanske RF, Jr, et al. JAMA 2001;285:2594-603.
Reduction phase: RR of treatment failure for patients in salmeterol-minus group compared with salmeterol-plus group was 2.2 (0.5-9.2) (P =.27)
Elimination phase: RR of treatment failure in salmeterol-minus group compared with salmeterol-plus group was 4.3 (2.0-9.2), (P = .001)
ICSs could safely undergo 50% reduction, but could not have ICSs eliminated

GOAL
Bateman ED, et al. AJRCCM 2004;170:836-44.
Objective: To determine proportion of patients who achieved well-controlled asthma with salmeterol/fluticasone combination compared with fluticasone alone
Patient 3421 patients, 12 years, asthma 6 months, reversibility of 15%, smoking pack years < 10 years, uncontrolled asthma 2 out of 4 weeks during run-in period
3 strata (ICS in 6 months prior to randomisation):
Stratum 1: Corticosteroid-naïve (S/F 550;F 548) Stratum 2: 500 µg Beclomethasone or equivalent (S/F 578;F 585) Stratum 3: >500 – 1000µg Beclomethasone or equivalent (S/F 579;F 576)

Study design for Strata 1 and 2
Seretide 50/100or FP 100
8- week control assessment
4- week control assessment
Phase I
Phase II
Seretide 50/250or FP 250
Seretide 50/500or FP 500
Step 1
Step 2
Step 3
Seretide 50/500 &oral prednisolone
Visit 1 2 3 4 5 6 7 8 9
Week -4 0 4 12 24 36 48 52 56
Bateman ED, et al. AJRCCM 2004;170:836-44.

Study design for Stratum 3
8- week control assessment
4- week control assessment
Phase I
Phase II
Seretide 50/250or FP 250
Seretide 50/500or FP 500
Step 1
Step 2
Seretide 50/500 &oral prednisolone
Visit 1 2 3 4 5 6 7 8 9
Week -4 0 4 12 24 36 48 52 56
Bateman ED, et al. AJRCCM 2004;170:836-44.

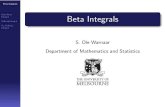
Well-controlled asthma: SFC versus FP Phase I: stratum 1 p = 0.039, strata 2 and 3 p < 0.001
Cumulative phase I and phase II: stratum 1 p = 0.003, strata 2 and 3 p < 0.001
65%71% 69%
52% 51%
33%
78%70% 75%
60%62%
47%
Bateman ED, et al. AJRCCM 2004;170:836-44.

Well Controlled Asthma
20
80
100
0
60
40
% of patients with a Well-controlled week
Week
Seretide
FP
-4 0 4 40 44 4812 16 24 28 32 36 528 20
All patients
77%
68%
Bateman ED, et al. AJRCCM 2004;170:836-44.

42%
31%32%
20% 19%
8%
Totally controlled asthma: SFC versus FP Phase I: all strata p < 0.001
Cumulative phase I and phase II: all strata p < 0.001
50%40%
44%
28% 29%
16%
Bateman ED, et al. AJRCCM 2004;170:836-44.

FACET
Pauwels RA, et al. NEJM 1997;337:1405-11.
Objective: To evaluate the effects of adding inhaled formoterol to both lower and higher doses of the inhaled glucocorticoid budesonide
Patient 852 patients with asthma (FEV1 at baseline ≥ 50%) at least 6 months, 18-70 years, treat with ICS
Intervention & control
Run-in period: BUD 800 µg BID x 4 wkRandom to 4 groups:1. BUD 100 µg BID x 1 year2. BUD 100 µg BID + Formoterol 12 µg BID x 1 year3. BUD 400 µg BID x 1 year4. BUD 400 µg BID + Formoterol 12 µg BID x 1 year
Primary outcome
Rates of severe and mild exacerbations of asthma per patient per year

Pauwels RA, et al. NEJM 1997;337:1405-11.
1 2 3 4

• FEV1 increased significantly in all groups during the run-in period• FEV1 increased further with the addition of formoterol • The higher dose of budesonide was associated with a significantly higherFEV1 than the lower dose
Pauwels RA, et al. NEJM 1997;337:1405-11.
Patients who have persistent symptoms despite treatment with ICSs, the addition
of formoterol to BUD Increasing dose of ICSs might be a more appropriate initial therapeutic step in patients with repeated severe
exacerbations

Bisgaard H, et al. Chest 2006;130:1733-43.
Objectives: To investigate whether budesonide/formoterol for maintenance and reliever therapy could reduce asthma exacerbations.
Patient 341 children, 4-11 years, with asthma ≥ 6 months, prebronchodilator FEV1 60-100% and 12% reversibility, uncontrolled with ICS
Intervention & Control
1. SMART: BUD/Formoterol 80/4.5 µg OD + BUD/Formoterol additional inhalations for symptom relief (≤ 7 as-needed inhalation/day) x 12 months (118)
2. Fixed combination: BUD/Formoterol 80/4.5 µg OD + Terbutaline 0.4 mg for rescue medication X 12 months (117)
3. Fixed-dose budesonide: BUD 320 µg OD + Terbutaline 0.4 mg for rescue medication x 12 months (106)
Primary outcome
Time to first exacerbation

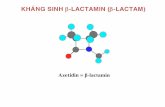
14%
38%
26%
SMART significantly prolonged the time to first exacerbation vs fixed-dose combination (p < 0.001) or fixed-dose budesonide (p =
0.02)
Bisgaard H, et al. Chest 2006;130:1733-43.

Bisgaard H, et al. Chest 2006;130:1733-43.

de Bilc J. et al. Pediatr Allergy Immunol 2009;20:763-71.
Objective: To compare efficacy and safety of salmeterol/fluticasone 50/100 µg BID with fluticasone 200 µg BID in children uncontrolled on low dose ICS.
Patient 584 children,4–11 yrs, with a clinical history of asthma for at least 6 months, reversibility in FEV1 ≥ 15%, currently receiving BDP 400 µg/day or equivalent
Intervention & Control
Run-in period: FP 100 µg BID x 4 wk not controlled ≥ 2 wk Randomization1. Salmeterol/fluticasone (SFC) 50/100 µg BID x 12
wk (160) 2. Fluticasone propionate (FP) 200 µg BID x 12 wk
(161)
Primary outcome
Mean change from baseline in morning PEF over 12 wk

Mean change differences between 2 groups: 7.06±3.01 (95% CI 1.7-13.5)(p = 0.012)
de Bilc J. et al. Pediatr Allergy Immunol 2009;20:763-71.

SFC is as effective as FP, at half the dose of ICS
de Bilc J. et al. Pediatr Allergy Immunol 2009;20:763-71.

At least one adverse event SFC: 87 (58%) subjects FP: 86(56%) subjects
Most common: headache and nasopharyngitis Serious adverse events
SFC group (2%): laryngotracheitis(1), asthma exacerbation (1) and concussion (1)
FP group (2%): wound infection (1), asthma exacerbation (1) and gastritis (1)
None of which were assessed as related to study
de Bilc J. et al. Pediatr Allergy Immunol 2009;20:763-71.

PACT
Sorkness C, et al. JACI 2007;119:64-72.
Objective: To compare the effectiveness of fluticasone monotherapy, fluticasone + salmeterol, and montelukast in achieving asthma control
Patient 285 children, 6-14 years, mild-moderate persistent asthma symptoms, FEV1 ≥ 80%, PC20 ≤ 12.5 mg/mL, not on controller medications ≥ 2 weeks before randomization
Intervention & Control
Run-in period: Placebo + Albuterol MDI x 2-4 weeksRandomization x 48 weeks1. Fluticasone monotherapy: Fluticasone 100 µg BID (96) 2. PACT combination: Fluticasone 100 µg/salmeterol 50 µg in
morning and salmeterol 50 µg evening (94)3. Montelukast monotherapy: Montelukast 5 mg in the
evening (95)
Primary outcome
Percent of asthma control days during the 48-week treatment period

% ACD -F 64.2% -C 59.6% -M 52.5%
Sorkness C, et al. JACI 2007;119:64-72.

Sorkness C, et al. JACI 2007;119:64-72.

Sorkness C, et al. JACI 2007;119:64-72.
• Improvements ACD: Both F & C > M• FEV1, FEV1/FVC, max bronchodilator response, ENO: F > C • Favor fluticasone monotherapy in treatingchildren with mild-moderate persistent asthma with FEV1 ≥ 80%

BADGERS
Lemanske RF, Jr, et al. NEJM 2010;362:975-85.
Objectives: To assess frequency of differential responses to 3 step-up treatments in children who had uncontrolled asthma while receiving low-dose ICSs
Patient 182 children, 6 -17 years, uncontrolled asthma while receiving Fluticasone 100 µg BID
Intervention & Control
Triple-crossover study (random order) x 16 weeks: 1. ICS step-up: Fluticasone 250 µg BID 2. LABA step-up: Fluticasone 100 µg BID + Salmeterol 50 µg of a
BID 3. LTRA step-up: Fluticasone 100 µg BID + Montelukast 5 or 10 mg
OD
Primary outcome
Differential response:- Oral prednisone (Total prednisone received during the period was ≤180 mg)- Asthma-control days (Annualized asthma-control days during the final 12 weeks was increased ≥ 31 days- FEV1 (FEV1 at the end ≥ 5%)

52%
34%
54%
32%P = 0.004
P = 0.02
Similar
Lemanske RF, Jr, et al. NEJM 2010;362:975-85.
LABA vs LTRA: Relative probabilityof best response 1.6(1.1-2.3);p = 0.004
LABA vs ICS: Relative probabilityof best response 1.71.7 (1.2-2.4);p=0.002

Higher childhood ACT scores (> 19) predict best response to LABA step-up
Race Hispanic & non-hispanic white: best response
to LABA Black: best response to LABA or ICS equally
LABA step-up was significantly more likely to provide the best response.
BADGERS
Lemanske RF, Jr, et al. NEJM 2010;362:975-85.

Safety issues

Nelson H, et al. Chest 2006;129:15-26.
Objectives: To compare the safety of salmeterol xinafoate or placebo added to usual asthma care
Patient 26,355 patients, > 12 years, asthma (Clinical judgment), no LABA, no β-blocker
Intervention Salmeterol MDI 42 µg BID + Usual care x 28 weeks
Control Placebo MDI BID + Usual care + Usual care x 28 weeks
Primary outcome
Respiratory-related deaths, or life-threatening experiences
SMART

Nelson H, et al. Chest 2006;129:15-26.

Asthma history and current nocturnal symptoms indicate greater disease
severity at baseline in the African-American subgroupNelson H, et al. Chest 2006;129:15-26.

Seretide
Salmeterol
Formoterol
Symbicort
Kramer JM. NEJM 2009;360(16):1592-5.

FDA Committee 2008
Age group Single agent Combination
4-11 years • Benefits did not outweigh the risks (paucity of randomized data)
• Benefits outweighed the risks for salmeterol/fluticasone (Slim majority)
Adolescent & adult
• Benefits did not out-weigh the risks • Label - Against using LABAs as monotherapy - LABAs should be added to ICSs only when ICSs alone proved inadequate for asthma control
• Adult: Benefits of combi-nation products outweighed the risks (unanimously for Advair &with 1 abstention for Symbicort)• Adolescent: Benefits outweighed the risks for both Products (Substantial majority)
Kramer JM. NEJM 2009;360(16):1592-5.

Chowdhury BA, Pan GD. NEJM 2010;362(13):1169-71.

• EPR 3: 2007• GINA 2010• GINA under five• PRACTALL
Asthma guidelines: β2-agonist

SABAs are the most effective medication for relieving acute bronchospasm.
Therapy of choice for relief of acute symptoms and prevention of EIB.
Regularly scheduled, daily, chronic use of SABA is not recommended.
Increasing use of SABA treatment or using SABA >2 days a week for symptom relief (not prevention of EIB) generally indicates inadequate control of asthma.
SABA




LABAs are not to be used as monotherapy for long-term control.
LABAs are used in combination with ICSs for long-term control and prevention of symptoms in moderate or severe persistent asthma (≥ step 3 care in children ≥ 5 years of age and adults) -- ? increased risk of severe exacerbations associated with the daily use of LABA.
- For patients ≥5 years of age who have moderate persistent asthma or asthma inadequately controlled on low-dose ICS increasing the ICS dose = adding LABA. - For patients ≥5 years of age who have severe persistent asthma or asthma inadequately controlled on step 3 care combination of LABA and ICS is the preferred therapy.
LABA may be used before exercise to prevent EIB.
The use of LABA for the treatment of acute symptoms is not currently recommended.
LABA

2009
LABAs cannot be recommended in this age group.
SABAs are the most effective bronchodilatorsand the preferred reliever treatment in children
≤ 5 years.

2010

GINA 2010
SABAs LABAs
Drug of choice for relief bronchospasm during exacerbation
LABAs should not be used as monotherapy
Prevention of EIB Most effective when combined with ICSs
Preferred treatment when medium dose of ICSs alone fails to achieve control
LABAs + ICSs may also be used to prevent EIB and may provide longer protection than SABAs

Bacharier LB, et al. Allergy 2008;63:5-34.
Treatment of choice for intermittent and acute asthma episodes in children, very young children and for preventing EIB.
Salbutamol, terbutaline, and formoterol have a favorable safety and efficacy profile in patients aged 2–5 years
SABA

Bacharier LB, et al. Allergy 2008;63:5-34.
Children > 2 years of age

Add-on controller therapy to ICS for partially controlled or uncontrolled asthma.
Efficacy is not well documented in children in contrast to adults, and use should be evaluated carefully.
Safety concerns suggest that use should be restricted to add-ontherapy to ICS when indicated.
Combination products of LABA and ICS may be licensed for use in children over 4–5 years, however, the effect of LABAs or combination products has not yet been adequately studied in young children under4 years.
LABABacharier LB, et al. Allergy 2008;63:5-34.

Take-home messages
Catecholamine structure has been modified to achieve greater β2 selectivity and a better pharmacologic profile.
Non-bronchodilator actions can be beneficial in the treatment of asthma, including glucocorticoid receptor priming.
SABAs are the drugs of choice for treating acute asthma symptoms and exacerbations and for preventing EIB.

Take-home messages
LABAs are useful in combination with inhaled corticosteroids for long-term control of asthma but should not be used as monotherapy.
Further studies are needed to definitively determine whether the addition of LABAs to ICSs increases the risk of serious asthma outcomes

Thank youfor your attention