Atorvastatin attenuates the paraquat-induced pulmonary inflammation via PPARγ receptors: A new...
40
Accepted Manuscript Atorvastatin attenuates the Paraquat-induced pulmonary inflammation via PPAR γ receptors: A new indication for Atorvastatin Hassan Malekinejad, Mona Khoramjouy, Rahim Hobbenaghi, Amir Amniattalab PII: S0048-3575(14)00112-6 DOI: http://dx.doi.org/10.1016/j.pestbp.2014.06.011 Reference: YPEST 3679 To appear in: Pesticide Biochemistry and Physiology Received Date: 19 March 2014 Accepted Date: 26 June 2014 Please cite this article as: H. Malekinejad, M. Khoramjouy, R. Hobbenaghi, A. Amniattalab, Atorvastatin attenuates the Paraquat-induced pulmonary inflammation via PPAR γ receptors: A new indication for Atorvastatin, Pesticide Biochemistry and Physiology (2014), doi: http://dx.doi.org/10.1016/j.pestbp.2014.06.011 This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Transcript of Atorvastatin attenuates the paraquat-induced pulmonary inflammation via PPARγ receptors: A new...

Accepted Manuscript
Atorvastatin attenuates the Paraquat-induced pulmonary inflammation viaPPAR γ receptors: A new indication for Atorvastatin
Hassan Malekinejad, Mona Khoramjouy, Rahim Hobbenaghi, AmirAmniattalab
PII: S0048-3575(14)00112-6DOI: http://dx.doi.org/10.1016/j.pestbp.2014.06.011Reference: YPEST 3679
To appear in: Pesticide Biochemistry and Physiology
Received Date: 19 March 2014Accepted Date: 26 June 2014
Please cite this article as: H. Malekinejad, M. Khoramjouy, R. Hobbenaghi, A. Amniattalab, Atorvastatin attenuatesthe Paraquat-induced pulmonary inflammation via PPAR γ receptors: A new indication for Atorvastatin, PesticideBiochemistry and Physiology (2014), doi: http://dx.doi.org/10.1016/j.pestbp.2014.06.011
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customerswe are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, andreview of the resulting proof before it is published in its final form. Please note that during the production processerrors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.

1
Atorvastatin attenuates the Paraquat-induced pulmonary inflammation via PPAR γγγγ receptors: A
new indication for Atorvastatin
Hassan Malekinejad a, *
, Mona Khoramjouy a, Rahim Hobbenaghi
b, Amir Amniattalab
c
a Department of Pharmacology & Toxicology, Faculty of Veterinary Medicine, Urmia University,
Urmia, Iran
b Department of Pathology, Faculty of Veterinary Medicine, Urmia University, Urmia, Iran
c Department of Pathology, Islamic Azad University, Urmia Branch, Urmia, Iran
Running title: Atorvastatin exerts anti-inflammatory effect
*Corresponding to:
Malekinejad H.
Department of Pharmacology & Toxicology, Faculty of Veterinary Medicine, P.O.Box: 1177,
Urmia University, Urmia, Iran.
Tel: +98 441 279 2608
Fax: +98 441 277 1926

2
Abstract
This study was carried out to highlight the role of PPAR γ receptors and atorvastatin’s protective
effect on paraquat (PQ)-induced inflammation in the lungs. Forty-two male Wistar rats were
exposed either against saline as control or PQ (3.5 mg/kg, IP) as test groups for 14 days. The test
groups were nominated as: PQ, pioglitazone (PGT, 10 mg/kg, orally), atorvastatin (STN, 10
mg/kg, orally), PGT+STN, PGT+GW9662 (1 mg/kg) and STN+GW9662 (1 mg/kg).
PGT and STN significantly (P < 0.05) reduced the PQ-elevated myeloperoxidase activity, nitric
oxide and malondialdehyde contents of the lungs and IL-6 and TNF-α concentrations in serum.
Histopathological studies revealed alveolar edema and hemorrhages along with hyaline exudates
in alveoli confirming that PGT and STN reduced the damages. Immunohistochemistry studies
showed that the PQ-induced inflammation resulted in a severe recruitment of CD68+
macrophages, which PGT and STN remarkably diminished them. STN regulated the PQ-up-
regulated COX-2 expression. The antagonistic effect of GW9662 as an absolute antagonist of
PPAR γ receptors on anti-inflammatory effect of STN in the regulation of COX-2 expression
was observed. These data provide a molecular proof(s) of the STN-produced protective effects
on the PQ-induced pulmonary inflammation, which is antagonized by PPAR γ antagonist
indicating its anti-inflammatory effects via PPARγ receptors. Moreover, a new indication for
atorvastatin is suggested.
Key Words: Antagonist; Combination therapy; Cyclooxygenase-2; Paraquat; Pro-inflammatory
Cytokine

3
1. Introduction
Pulmonary inflammation (PI) is a primary reaction to the pathological symptoms, occurring
during various forms of respiratory diseases. It is believed that in the different forms of respiratory
diseases, several cell types are playing role. For instance; it has been reported that the main cells involve
in asthma are eosinophils, mast cells, and CDC4+ lymphocytes. However, in chronic obstructive
pulmonary disease (COPD), the most inflammatory cells are neutrophils, macrophages and lymphocytes
[1]. Activation of cells involved in the initiation of PI, leads to the release of pro-inflammatory
mediators and cytokines such as TNF-α, IL-1β, and IL-13, which ultimately results in pathological
alterations including vascular leakage, bronchial smooth muscle contraction, inflammatory cells
accumulation, mucus hypersecretion in asthmatic patients and some changes in the proteinase–
antiproteinase system, oxidative stress and airway remodeling in COPD cases [2].
Paraquat (PQ) as a known herbicide is used worldwide for controlling of weeds in corn and vegetables
farms and fruit orchards before harvesting. Paraquat easily binds to clay and organic materials in soil
and is slowly biodegraded [3]. In mammals, it accumulates largely in the lungs and to a lesser extent in
the liver, kidney and the heart. The most common reason of death in PQ-poisoned humans and animals
is respiratory disorder due to mainly oxidative stress and pulmonary fibrosis [4]. Moreover, the known
cellular mechanisms for PQ-induced pulmonary damages are the P-450 reductase-dependent formation
of reactive oxygen species and peroxidation of membrane lipids in pulmonary cells [5].
Peroxisome proliferator-activated receptors (PPARs) are transcription factors that among them PPARγ
regulates various metabolic pathways and cellular proliferation. Previous reports, however, indicated
that PPARs agonists also exhibited anti-inflammatory and immunomodulatory effects. Recently, Belvisi
and Hele (2008) reviewed the effects of PPARα and PPARγ agonists on various cell types within the
lung and highlighted that PPARα agonists affected the T-lymphocytes, eosinophils and macrophages,
while PPARγ agonists mainly affected the neutrophils, macrophages, fibroblasts and epithelial cells
combined with T-lymphocytes and eosinophils [6]. The anti-inflammatory effects of PPARγ and

4
PPARα have been reported in both in vitro and in vivo models [7]. These effects are mainly due to
ability of PPAR α and γ in regulation of the inflammatory genes expression after binding as a
heterodimer to the retinoid X receptors (RXRs). RXR is expressed widely in monocytes/macrophages
[8]. The anti-inflammatory effect of PPARγ ligands including 15d-PGJ2 through reducing the
inflammatory cells infiltration and edema in the lungs has been already reported [9].
The beneficial pleiotropic effects of statins include their immunemodolatory, anti-inflammatory and
their regulatory effects on coagulation system in addition to their main cholesterol lowering effect.
Previous epidemiological studies are indicating a lower mortality among statin users following
pneumonia [10]. There are several mechanisms for anti-inflammatory action of statins, including the
cholesterol lowering and reducing the stability of lipid raft formation and subsequent effects on the
activation and regulation of immune cells preventing the prenylation of signaling molecules and
subsequent down-regulation of gene expression; resulting in reduced cytokine, chemokine and adhesion
molecule production, and antioxidant effects with a ability to scavenge oxygen-derived free radicals
[11].
As the PQ-induced pulmonary inflammation characteristics have not fully been understood, therefore in
this study we firstly aimed to highlight the cellular and biochemical impact of PQ-induced pulmonary
inflammation. Additionally, there is an increasing data indicating the role of PPARγ in the regulation of
inflammation and at the same time regulatory effect of statins on the PPARs expression. The possible
pathway involved in statin’s anti-inflammatory effect on the PQ-induced PI was further investigated. To
compare the anti-inflammatory effect of atorvastatin and highlight its molecular pathway, the effect of
pioglitazone as a known agonist of PPARγ was also studied.
2. Materials and Methods
2.1. Chemicals

5
1, 1'-dimethyl-4, 4'-bipyridilium dichloride (Paraquat, PQ), GW9662 (M6191, antagonist of PPARγ
receptors), Pioglitazone HCl (P6910), atorvastatin, sulfanilamide and N-(1-naphthyl)
ethylenediamine.2HCL were purchased from Sigma-Aldrich (Germany). Trizol was obtained from
Invitrogen, Life Technologies (The Netherlands). Thiobarbituric acid, phosphoric acid (85%), dimethyl
sulfoxide (DMSO), ethanol and sodium nitrite were obtained from Merck (Germany). N-butanol was
obtained from Carl Roth, GmbH Co. (Germany).
2.2. Experimental animals
This study was performed on 42 male and healthy Wistar rats (180-200 g), 10-12 weeks old, kept at the
animal center of Urmia University. The animals were provided with food and water ad libitum and kept
in ventilated room at 22 ± 2 °C with a 12 h light/dark cycle. The performed experiments on animals
were in accordance with the guidelines of the ethical committee for research on laboratory animals of
Urmia University (AECVU/126/2013).
2.3. Experimental design
After a week acclimation, the animals were assigned into control and test groups. Before the
experimental procedures, all animals were weighed and these procedures were repeated at the end of
study to evaluate any changes in the body weight gain (BWG). Animals in the control group received an
equivalent volume of saline (1ml/kg, b.w.) similar to the PQ solution in the test groups. The animals in
test groups received PQ (dissolved in sterilized saline) at 3.5 mg/kg, (b.w.) dose level intraperitoneally
for 14 consecutive days [5]. The animals in test group sub-grouped (n = 6) based on received
compound(s) during the experiment as follow:
A) PQ group; animals in this group along with PQ received saline (1 ml/kg, at 15:00, p.m.);
B) PGT group; animals in this group along with PQ were treated with PGT (10 mg/kg, orally, at
13:00, p.m.);

6
C) STN group; animals in this group along with PQ were treated with atorvastatin (10 mg/kg,
orally, at 13:00, p.m.);
D) PGT + STN; animals in this group along with PQ were treated with PGT (10 mg/kg, orally, at
13:00, p.m.) and atorvastatin (10 mg/kg, orally, at 11:00, a.m.);
E) PGT + GW; animals in this group along with PQ were treated with PGT (10 mg/kg, orally, at
13:00, p.m.) and GW9662 (GW; 1 mg/kg, i.p., 11:00, a.m.);
F) STN + GW; animals in this group along with PQ were treated with STN (10 mg/kg, orally, at
13:00) and GW9662 (GW; 1 mg/kg, i.p., at 11:00, a.m.).
The selected dose levels for PGT and STN were based on previous reports [12].
2.4. Serum preparation and tissue collection
On day 15, immediately after a light anesthesia with diethyl ether, blood samples were collected directly
from the heart and left to clot at room temperature for 10-20 minutes, and then were centrifuged at 3000
× g for 10 min to obtain the serum. After blood collection, the animals were euthanized using overdose
injection of sodium pentobarbital (200 mg/kg, b.w., i.p.) and the lung tissues were dissected
immediately. The collected tissue samples were divided into two parts and the first part after washing
with chilled saline, were snap frozen in liquid nitrogen and then immediately were stored at -70 °C for
further biochemical and molecular analysis. The second part of the samples was preserved in 10%
buffered formaldehyde for further histopathological and immunohistological examinations.
2.5. Malondialdehyde (MDA) determination
To determine the lipid peroxidation rate in the control and test groups, the MDA content of the lung
samples was measured using the thiobarbituric acid (TBA) reaction as described previously [13].
Briefly, 0.2-0.3 g of the lung samples were homogenized in ice-cooled KCl (150 mM), and then the
mixture was centrifuged at 3000 × g for 10 min; 0.5 ml of the supernatant was mixed with 3 ml

7
phosphoric acid (1% V/V) and then after vortex mixing, 2 ml of 6.7 g L−1 TBA was added to the
samples. The samples were heated at 100 °C for 45 min, and then chilled in ice. After addition of 3 ml
N-butanol, the samples were centrifuged at 3000 × g for 10 min. The absorbance of supernatant was
measured spectrophotometerically (Pharmacia, Novaspec II, Biochrom, England) at 532 nm and the
amount calculated according to the simultaneously prepared calibration curve using MDA standards.
The amount of MDA was expressed as nmol per mg of protein. The protein content of the samples was
assessed based of Lowery et al., (1951) method [14].
2.6. Myeloperoxidase activity
Myeloperoxidase (MPO), as a biochemical indicator of neutrophil infiltration, was measured in the
collected lung samples as previously described [15]. In brief, the specimens were homogenized in 10
mM potassium phosphate buffer (pH 7.0), containing 0.5% hexadecyl trimethyl ammonium bromide and
centrifuged at 20,000 × g for 30 min at 4 ºC. A solution of 1.6 mM tetramethyl benzidine and 0.1 mM
H2O2 was added and reacted with an aliquot of the supernatant. The rate of change in optical density was
measured at 650 nm spectrophotometerically. One unit of MPO activity was defined as that degrading 1
µmol of H2O2 per min at 37 ºC and was expressed as units per milligram of tissue sample (U/mg tissue).
2.7. Nitric Oxide (NO) measurement
The total NO content of the lung samples was measured according to the Griess reaction [16]. In Griess
reaction, nitric oxide rapidly is converted into the more stable nitrite and then in an acidic environment
nitrite is converted to HNO2. In reaction with sulphanilamide, HNO2 forms a diazonium salt, which
reacts with N-(1-naphthyl) ethylenediamine.2HCl to form an azo dye that can be detected by absorbance
at a wavelength of 540 nm. The NO content of the examined organs was expressed as nmol per mg of
protein in samples.

8
2.8. Determination of inflammatory cytokines
The serum level of IL-6 and TNF-α were measured by ELISA technique, using high sensitivity enzyme
immuno-assay rat specific kits (rat IL-6 Quantikine ELISA kit, R6000B, R&D systems, Abington, UK
and rat TNF-α kit from BD OPTEIA, BD Bioscience) according to manufacturer instructions. Both
cytokines levels were reported as pg/ml. Absorbance was measured using a microtiter plate reader at 450
nm (Statfax 2100, USA). The assay sensitivity for IL-6 and TNF-α were 36 and 4.59 pg/ml,
respectively. Inter- and intra-assay coefficients of variation were 8.1 and 8.8% and 7.4 and 3.5 % for IL-
6 and TNF-α, respectively.
2.9. Histopathological and Immunohistological examinations
Tissue samples from the lungs that previously had been stored in 10% buffered formaldehyde, were
embedded in paraffin and 5-6 µm sections were cut using a rotary microtome and stained with
Hematoxiline & Eosin for routine histologic examination. To evaluate the level of damages following
exposure to PQ and/or PQ plus various treatments, indices such as alveolar edema and hemorrhages,
emphysema, mononuclear inflammatory cells infiltration and the presence of hyaline exudate were
scored numerically. The evaluation criteria were as follows: zero for no detectable lesion, 1 for mild
changes, 2 for moderate changes and 3 for severe damages. For each animal in the tests and control
groups at least three slides were prepared and scored.
Immunohistochemistry was performed to identify macrophages as one of the inflammatory cells in
damaged tissue. The procedures of immunohistochemical staining were performed on the basis of
standard protocol of manufacturer with the EnVision+ Dual Link System-HRP (horseradish peroxidase)
staining technique. Stages of immunostaining which were performed included: The tissue sections were
cut in 3 µm of thickness and then were located on the silanized slides S3003 (Dako, USA) for drying
and attaching them together for 1 hour. Next, the slides were put in xylene, absolute and 96% ethanol
respectively and washed. The tissue sections were placed in Tris - EDTA Buffer (TBS, pH 9.0) and

9
immersed by 3% H2O2 in methanol for 10 minutes for quenching endogenous peroxidase. Then the
slides were transferred into microwave for antigen retrieval. First the machine was set to maximum
power to take the buffer to spot welding. Then microwave power was reduced to 40% and the sections
were incubated in this situation for 15 minutes. Since discharging the sections with buffer, they were
incubated in room temperature to cool them down. After washing by water and TBS, environments of
tissues were defined by Dako pen. They were incubated in a dark humid room and surface of tissues
coated by primary antibody perfectly. The primary antibody which were used, were ready-to-use (RTU)
formation including: monoclonal mouse anti-human CD68 (Clone KP1) (Dako Denmark A/S). After
washing by TBS for 5 minutes and incubating in humid room, the sections were coated by labeled
polymer with peroxidase (secondary antibody). Temperature of humid room was 37 ºC. Then the
sections were washed by TBS for 5 minutes twice. For staining, tissue surfaces were coated by
chromogen plus 3,3-diamino benzidine (DAB) substrate solution (1 drop chromogen in 1 ml substrate)
and incubated in humid room which temperature was regulated in 37 ºC for 10 minutes. Other
procedures were performed routinely and the sections counterstained by Harris haematoxylin for 1
minute and the slides mounted by mounting media.
2.10. RNA Isolation and RT-PCR
To evaluate the effect of PQ on COX-2 mRNA level, tissue samples from the lung were collected and
snap frozen in liquid nitrogen and then stored at -70 °C until RNA isolation. Total RNA was isolated
from pooled samples homogenates for the control and test groups (n=6) using the standard TRIZOL
method [17]. To avoid genomic DNA contamination extra care was taken when the colorless aqueous
phase collected after chloroform extraction. The RNA amount was determined spectrophotometrically
(260 nm and A260/280=1.8-2.0), and the samples were stored at -70 °C. For RT-PCR, cDNA was
synthesized in a 20µl reaction mixture containing 1µg RNA, oligo(dT) primer (1µl), 5×reaction buffer
(4µl), RNAse inhibitor (1µl), 10mM dNTP mix (2µl) and M-MuLV Reverse Transcriptase (1µl)

10
according to the manufacturer’s protocol (Fermentas). The cycling protocol for 20 µl reaction mix was
5 min at 65 °C, followed by 60 min at 42°C, and 5 min at 70 °C to terminate the reaction. We run the
PCR reaction with using specific RT-PCR primers –which stated in below- on RNA samples and no
PCR bands were observed indicating that the RNA samples are free from genomic DNA.
2.11. Second Strand cDNA Synthesis
The RT-PCR reaction was carried out in a total volume of 25µl containing PCR master mix (12.5 µl),
FWD and REV specific primers (each 0.5 µl), cDNA as a template (1µl) and nuclease free water
(10.5µl). PCR conditions were run as follows: general denaturation at 95 °C for 3 min, 1 cycle, followed
by 40 cycles of 95 °C for 20s; annealing temperature (63 °C for GAPDH and 59°C for COX-2) for 30s;
elongation: 72 °C for 1 min and 72°C for 5 min.
The products of RT-PCR were separated on 1.5 % agarose gels containing ethidium bromide and
visualized using Gel Doc 2000 system (Bio-Rad). The density of RT-PCR bands were quantified by
using the software of Molecular Analyst (Bio-Rad, the Netherlands) and normalized based on the
density of corresponding GAPDH bands. The RT-PCR reaction and subsequent electrophoresis were
performed three times and the averages of numerical densitometric values along with standard deviation
were calculated. The specific primers for Ratus COX-2 and GAPDH were designed [18, 19], and
manufactured by CinnaGen (CinnaGen Co. Tehran, Iran). Primers pairs for RT-PCR were as depicted
in Table1.
2.12. Statistical analyses
The mean and standard deviations of measured parameters were calculated. The obtained results were
analyzed using Graph Pad Prism software (version 2.01.; Graph Pad software Inc. San Diego,
California). The comparisons between groups were made by analysis of variance (ANOVA) followed by

11
Bonferroni post hoc test. For comparing the graded degree of pathological findings between groups, the
Kruskal-Wallis test was used. A P value <0.05 was considered significant.
3. Results
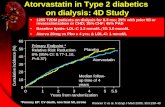
3.1. Atorvastatin reduced the PQ-induced body weight loss
The clinical symptoms such as nasal and eyes bloody discharges along with soundness breathing were
observed in the PQ-exposed animals. During the 14 consecutive days experiment period and in
particular during the second week of study, animals which in addition of PQ were treated with various
compounds, showed different clinical symptoms indicating abnormalities in the respiratory system.
Except the animals which received STN, all others demonstrated in a lesser extent the same symptoms,
which the non-treated PQ-exposed rats showed. Moreover, the PQ-exposed animals demonstrated the
highest level of body weight loss, while PGT and STN administration alone but not in combination
resulted in a significant (P<0.05) reduction of PQ-induced body weight loss (Figure 1). We did not
obtain results to support any synergism or potentiation of protective effects between two test compounds
when they were co-administered. Those animals which received GW9662 before the PGT and/or STN,
showed enhanced body weight loss and the level of body weight loss in group of animals that received
GW9662 and STN was found very similar to the non-treated PQ-exposed animals.
3.2. PGT and STN lowered the PQ-enhanced MDA contents in the lungs
To evaluate the pro-oxidant effect of PQ in exposed animals, the lipid peroxidation and its end product
level (MDA content) were determined in the lung tissue. The obtained results showed a significant
(P<0.05) increase of MDA content in the PQ-exposed animals compared to the control group. We found
that both PGT and STN in individual but not in combination therapy reduced the MDA level.
Administration of GW9662 before the PGT did not result in a significant change compared to the PGT

12
administration, while a remarkable increase in the MDA content of lungs was obtained in the group of
animals which received GW9662 before the STN administration (Figure 2).
3.3. PGT and STN reduced the PQ-enhanced Myeloperoxidase activity and NO level in the lungs
The NO content of lungs in the PQ-exposed animals was elevated. By contrast all other groups of
animals that were treated with various copounds, showed a significant (P<0.05) reduction in the NO
level. Nevertheless, the lowest level of NO was found in the animals which were treated with STN. Co-
administration of PGT and STN not only could not lower the NO concentrations more than each
individuaal compound, but also resulted in a significant (P<0.05) elevation of NO level compared to
each individuals. Only pre-treatment of the STN-received animals with GW9662 resulted in a significant
elevation of NO concentration (Figure 3-A).
PQ exposure for 14 days resulted in a significant elevation of myeloperoxidase activity in the lung tissue
when compared with the control group. PGT and STN (2-fold stronger than PGT) reduced the MPO
activity in the lung tissue after 14 days. The highest level of MPO as a biomarker of neutrophil
infiltration was recorded in the group of animals, which received both test compounds simultaneously.
Antagonism phenamena was studied on MPO activity in the lungs and results indicated a significant
antagonistic effect of GW9662 against STN (Figure 3-B).
3.4. PGT and STN declined the Anti-inflammatory mediators
Inflammatory condition which was produced by PQ, resulted in a significant (P<0.05) elevation of both
pro-inflammatory mediators of IL-6 and TNF-α in the PQ-exposed animals when compared to the
control rats. Administration of PGT for 14 days only lowered the TNF-α level. By contrast, STN
successfully could reduce the PQ-enhanced concentrations of both pro-inflammatory mediators in serum
(Figure 4-A and 4-B). Again, we failed to show antagonistic effect of GW9662 against PGT in the PQ-

13
exposed animals, while the administration of GW9662 before the STN, was able to revers the STN-
reduced level of both pro-inflammatory cytokines.
3.5. PQ-induced pulmonary inflammation recruited macrophages and neutrophils
The normal histological feature of the lung from the healthy rats is demonstrated in figures 5-A.
Histopathological findings in the lungs of the PQ-exposed animals represented severe hemorrhages,
alveolar edema, hyperplasia and remarkable infiltration of macrophages and mononuclear cells in
interstitial tissue (Figure 5-B). Although the PQ-induced damages were reduced remarkably in the PGT-
and in particular STN-treated animals, however, alveolar edema, hyaline exudates within the alveoli and
the presence of macrophages in the PGT-received group and emphysema along with macrophage
infiltration in interstitial tissue were observed (Figure 5-C and 5-D). Co-administration of PGT and STN
resulted in severe hemorrhages, mononuclear immune cells infiltration around the vessels and re-
epithelialization alveoli (Figure 5-E). Pre-treatment of the rats with GW9662 before PGT and /or STN
worsened the PQ-damages and hyperplasia of the airways along with the infiltration of immune cells
have been demonstrated (Figure 5-F and 5-G).
To confirm the type of inflammatory cells, immunohistochemistry examinations were performed and the
presence of numerous intra cytoplasmic CD68 positive macrophages in the PQ-exposed rats was
identified. Although a few CD68 positive macrophages were found in the PGT-treated group, however
we were not able to show such macrophages in the STN-received animals. Other groups of the current
study did not show the CD68 positive macrophages within the lung parenchyma (Figure 6-A to G).
3.6. PGT and STN regulated the PQ-induced COX-2 expression in the lungs
The COX-2 expression at the mRNA level was assessed in the lung tissue after 2 weeks exposure to PQ
and the results showed that the COX-2 expression was up-regulated significantly in the PQ exposed
animals. PGT alone and in combination with STN was not able to regulate the PQ-up-regulated COX-2

14
expression, while STN administration resulted in a remarkable down regulation of COX-2 gene in the
lung tissue. GW9662 pre-treatment could not change the COX-2 expression in animals, which received
PGT but resulted in a significant up-regulation of COX-2 expression in the STN-treated rats (figure 7-
B). The expression profile of GAPDH as control gene is depicted in figures 7-A. The levels of mRNA
were expressed as the ratio of integrated density values (IDV) of COX-2 mRNA level to GAPDH
mRNA levels (Figure 7-C).
4. Discussion
In this study our results showed that both the PPARγ agonist (pioglitazone) and atorvastatin were able to
attenuate the PQ-induced pulmonary inflammation. Additionally, our results indicated that STN in all
experiments demonstrated a potent anti-inflammatory effect compared to that of pioglitazone. The
antagonistic studies suggest that STN exert its anti-inflammatory effect on PQ-induced inflammation
through the PPARγ receptors as the pre-treatment with GW 9662 could significantly reverse the STN
effects.
Our daily observations indicated that the PQ- induced lesions in respiratory system and in the bucal
cavity resulted in a remarkable reduction in body weight gain compared to the control group. Apart from
clinical injuries in the respiratory and upper part of gastrointestinal systems, another explanation for
body weight loss might be the PQ-induced anorexia, which might indirectly have been produced due to
generated inflammatory mediators that act on feeding centers [20]. Although PGT could reduce the PQ-
induced body weight loss, STN was able to recover the body weight loss significantly suggesting that
STN is more specifically acting on the PQ-induced injuries.
Our results confirmed that the PQ-induced pulmonary damage accompanied with an elevated lipid
peroxidation rate. Both PGT and STN could lower the concentration of produced MDA suggesting their
anti-lipid peroxidation properties. Anti-lipid peroxidation effect of atorvastatin has been demonstrated in

15
the prevention of liver steatosis [21]. At the same time the antioxidant effect of PGT in the reduction of
iron-induced lipid peroxidation has also been reported [22].
To gain insight and understand the cellular and molecular mechanism(s) of the PQ-induced pulmonary
inflammation, the type of cells and consequently their produced cytokines level were examined. We
performed an enzymatic assay to test the presence and any changes in the neutrophils population in the
lungs. Our findings indicated that the PQ-induced inflammation in the lungs resulted in a significant
enhancement of MPO activities suggesting an increase of neutrophils infiltration. The mechanism of the
recruitment of these cells to the lungs was also investigated. It is well documented that when damage in
the lung becomes too severe, the immune cells and/or other pulmonary parenchymal cells release
mediators that recruit inflammatory cells [23]. Indeed our results about the cytokines release support the
presence of inflammatory cells in the lungs. The infiltration of inflammatory cells such as neutrophils in
the lung confirmed the increased oxidant injury which was presented by the enhanced MDA production
and may also indicate their phagocytic action in clearing of the airways [24]. At the same time the
presence of inflammatory cells such as neutrophils and also macrophages (characterized by using an
immunohistochemistry technique) resulted in releasing of reactive oxygen and nitrogen species. Our
findings support this pathway in the PQ-induced inflammatory cascade that in parallel to the infiltration
of inflammatory cells (neutrophils and macrophages) in the lungs, release of both pro-inflammatory
cytokines including TNF-α and IL-6 and the generation of NO were elevated significantly. There is
evidence indicating that in addition to neutrophils and macrophages, alveolar type II epithelial cells
secrete NO in response to inflammatory cytokines [25]. The cytokine responses have been reported in
the Cd-induced inflammation by an increase of IL-6 release from the epithelial cells and TNF-α from
macrophages [26]. The histopathological and immunohistochemistry studies confirmed the biochemical
findings and the changes included hemorrhages, alveolar edema and infiltration of macrophages and
mononuclear cells in the interstitial tissue suggesting a pulmonary inflammation. Similar to the PQ-
induced pulmonary inflammation, previous reports indicated that in the LPS-induced pulmonary

16
inflammation, there is marked infiltration of neutrophils in the perivascular and intra-bronchiolar areas
[27]. The accumulation of CD68+ macrophages is confirming an inflammation and supports the NO
generation enhancement. The expression of cyclooxygenase-2 at mRNA level as another biomarker of
inflammation was also studied and the results showed that a significant up-regulation of COX-2
expression occurred in the lungs of non-treated PQ-exposed animals. Similar results have been reported
from in vitro and in vivo studies indicating up-regulation of COX-2 and elevation of the NO generation
in RAW 264.7 macrophages exposed to lipopolysaccharide and in rats exposed to nitrogen mustard for
28 days [28].
The second part of the current study was devoted to highlight the anti-inflammatory effect of
atorvastatin and to compare it with PGT as a known agonist of PPARγ receptors. Peroxisome
proliferative activated receptor-γ, known as a ligand-activated transcription factor serves as a target for
inflammation [29]. Our hypothesis was that PPARγ receptors were involved in mediation of the PQ-
induced pulmonary inflammation. Accordingly, we used PGT to overcome the inflammatory reactions
and indeed our findings supported this hypothesis as the PGT administration resulted in antioxidant
system improvement, cytokines release decline, reduction of the macrophages and neutrophils
infiltration and down regulation of the COX-2 expression in the lungs. These findings suggest that the
PGT- induced anti-inflammatory effect -at least partly- is mediated via PPARγ, as pretreatment with the
absolute antagonist of these receptors (GW9662) reversed partly the PGT anti-inflammatory effects.
Previous studies showed that in addition to adipose tissue, PPARγ is expressed in the lung epithelium,
submucosa, and airway smooth muscles [30]. There are also many reports indicating that the anti-
inflammatory effect of PGT is mediated via PPARγ receptors. For example, the neuroprotective effect of
PGT on iron-induced inflammatory reactions was found to be mediated via PPARγ [22]. Our findings in
the current study are supported by previous studies where it has been demonstrated that the PGT
administration in iron-exposed rats resulted in a significant decrease in pro-inflammatory cytokines,
inhibition of iNOS and COX-2 level and more importantly inhibition of iron-induced oxidative stress

17
[31, 32]. Our results also showed that PGT both decreased the PQ-elevated pro-inflammatory cytokines
and regulated the COX-2 up-regulation. Additionally, we found that PGT clearly declined the MDA and
NO concentrations in the lungs indicating it’s anti-oxidative and anti-nitrosative properties. Therefore, it
may concluded that PGT via the inhibition of oxidative and nitrosative stress and reduction of
inflammatory cells (macrophages and neutrophils) and pro-inflammatory cytokines (TNF-α and IL-6)
could attenuate the PQ-induced inflammatory reaction in the lungs. The majority of above mentioned
anti-inflammatory effects were reversed by the pre-treatment with GW9662 as known antagonist of
PPARγ suggesting that PGT via PPARγ reduce the PQ-induced inflammation. It is interesting to note
that GW9662 was not able to antagonize the PGT-regulated COX-2 expression. The possible reason for
this finding may relate to the fact that PGT in addition to PPARγ can activate another isoform of the
PPAR family including PPARα [33]. There are supporting data indicating the anti-inflammatory effect
of simvastatin on a zymosan-induced non-septic shock experimental model, which was mediated via
PPARα receptors [34]. Therefore, the COX-2 expression in the lungs might be regulated by both
isoforms of PPARs. Thus, by using GW9662 as a pure antagonist of PPARγ, we failed to reverse the
PGT-induced regulatory effect on COX-2 expression.
Since administration of PPARγ agonists such as PGT may result in hypoglycemia in non-diabetic cases
and due to the fact that statins by activating the PPARγ resulting in anti-inflammatory effects in various
cells such as endothelial cells and macrophages, we selected atorvastatin to investigate it’s anti-
inflammatory effect on the PQ-induced pulmonary inflammation [35-39]. Our findings regarding the
atorvastatin anti-inflammatory effects confirmed the previous reports and extended our understanding
towards its beneficial effects on the PQ-induced pulmonary inflammation. The powerful anti-
inflammatory effect of STN in this study was characterized by its potency in the reduction of pro-
inflammatory cytokines release, MPO activity and NO concentration, inflammatory cells infiltration,
and in regulating of the COX-2 expression. Our findings strongly support the idea that atorvastatin anti-
inflammatory effect on PQ-induced inflammation is mediated via PPARγ as the pretreatment with

18
GW9662 could revers all STN-induced effects. Anti-inflammatory effect of statins via PPARγ has been
well documented in both in vivo and in vitro models. Lee and co-workers (2010) showed that statins
suppressed the pro-inflammatory cytokines release in cultured gallbladder epithelial cells exposed to
lipopolysaccharide by activation of PPARγ [40]. It seems STN not only by reducing the TNF-α and IL-6
levels, blocks the NF-κb activity, but also directly by activating the PPARγ is able to reduce the NF-κb
activity and ultimately exert its anti-inflammatory effect [36]. We showed that STN lowered
significantly the PQ-elevated TNF-α and IL-6 concentrations. It has been well established that TNF-α as
a pro-inflammatory cytokine activates other cytokines and induces the expression of adhesive
molecules. On the other hand, IL-6 acts as a coordinator of acute phase responses and functions as a
strong leukocyte accumulator in the inflammation site. Histopathological results of the current study
confirmed that STN was likely to reduce the neutrophils infiltration and consequently lowering the MPO
activity in the PQ-exposed animals. Previous studies showed that simvastatin by activation of PPARγ
and inhibition of Nf-κB could reduce the TNF-α and IL-6 production and lower the MPO activity due to
preventing from neutrophils infiltration in the myocardium [41]. MPO in addition to being an important
biomarker of neutrophils infiltration may react with NO to generate reactive nitrogen species. We found
that STN not only reduced the NO concentration in the lung, but also lowered the MPO activity
suggesting that statins pleiotropic property may be partly attributed to their capability in suppression of
MPO activity. The down-regulation of MPO gene expression has been reported in human macrophages
treated with simvastatin [42]. We showed that atorvastatin remarkably down-regulated the PQ-induced
COX-2 expression in the lung, which was antagonized by GW9662 (PPARγ antagonist) indicating the
clear pathway of atorvastatin’s anti-inflammatory effect. The inhibitory effect of simvastatin and
atorvastatin on COX-2 protein expression in TNF-α−exposed human epithelial cells has been reported
[43]. Although there is no direct previous report about the COX-2 expression in the lung tissue and
specifically in the PQ-exposed animals, Wu et al. (2005) demonstrated that atorvastatin was able to
reduce the COX-2 mRNA and the PGE2 production in human pulmonary epithelial cells [44]. The

19
unexpected finding of present study was that the co-administration of PGT and STN did not result in
attenuation of the PQ-induced biochemical, histopathological and molecular damages in the lung. By
contrast, we found that the co-administration of both compounds reduced the potency of individuals in
the improvement of PQ-induced injuries indicating incompatibilities between these two substances. To
minimize the possible chemical incompatibility between two compounds when the combination therapy
was proposed, PGT and STN were administered separately and with 2 h interval. However, the results
indicated that the combination therapy failed to improve the PQ-induced injuries suggesting that either
two compounds reduced the absorption of each other in the gastrointestinal tract or interaction between
two substances occurred due to interference in biotransformation reactions. Our findings about the
combination therapy is not in agreement with report which showed that co-administration of
pioglitazone and atorvastatin increased myocardial 15-deoxy-delta-12,14-PGJ2, an endogenous ligand
of PPARγ levels in the rat [12]. Difference in target tissue (Heart vs lungs) and the strategy of the
treatment (pretreatment vs protective regimen) may explain this discrepancy.
5. Conclusions
We discovered that the PQ-induced inflammation is governed by massive infiltration of inflammatory
cells including neutrophils and macrophages, which in turn resulted in tremendous elevation of MPO
activity and NO content. Moreover, increased lipid peroxidation and inflammatory cytokines confirmed
pulmonary inflammation. It has also been highlighted that the PQ-induced pulmonary inflammation
could be protected by PGT and STN administration. Since understanding the mechanism(s) of
pulmonary inflammation could help to develop effective therapeutic compounds, therefore we state that
atorvastatin exert its protective effect via PPARγ receptors.
Acknowledgements: The authors are grateful to Dr. Ali Rezaei-Golmishe (Urmia University, Urmia,
Iran) for his generous help.
Conflict of interest: there is no conflict of interests.
Foundation: this study was conducted without any specific found.

20
References
[1]. W.I. De Boer, V.K. Alagappan, H.S. Sharma, Molecular mechanisms in chronic obstructive
pulmonary disease: potential targets for therapy. Cell Biochem. Biophys. 47 (2007)131-148.
[2]. S.T. Holgate, R. Polosa, Treatment strategies for allergy and asthma. Nat. Rev. Immunol. 8 (2008)
218-230.
[3]. V.L. Shopova, V.Y. Dancheva, P.T. Salovsky, A.M. Stoyanova, T.H. Lukanov, Protective effect of
U-74389G on paraquat induced pneumotoxicity in rats. Environ. Toxicol. Pharmacol. 24 (2007) 167-
173.
[4]. M. Tomita, T. Okuyama, H. Katsuyama, K. Hidaka, T. Otsuki, T. Ishikawa,. Gene expression in rat
lungs during early response to paraquat-induced oxidative stress. Int. J. Mol. Med. 17 (2006) 37–44.
[5]. H. Malekinejad, F. Rahmani, F. Hassanpour, Influences of sub-acute exposure to paraquat on
cytochrome P450 3A2 expression in rat liver and lungs. Pestic. Biochem. Physiol. 96 (2010) 149-154.
[6]. M.G. Belvisi, D.J.Hele, Peroxisome Proliferator-Activated Receptors as Novel Targets in Lung
Disease. Chest. 134 (2008) 152-157.
[7]. L. Dubuquoy, S. Dharancy, S. Nutten, S. Pettersson, J. Auwerx, P. Desreumaux, Role of peroxisome
proliferator-activated receptor gamma and retinoid X receptor heterodimer in hepatogastroenterological
diseases. Lancet. 360 (2002) 1410–1408.
[8]. A. Trifilieff, A. Bench, M. Hanley, D. Bayley, E. Campbell, P.Whittaker, PPAR-α and -γ but not -d
agonists inhibit airway inflammation in a murine model of asthma: in vitro evidence for an NF-kB
independent effect. Br. J. Pharmacol. 139 (2003) 163–171.
[9]. T. Genovese, S. Cuzzocrea, R. Di Paola, E. Mazzon, C. Mastruzzo, P. Catalano Effect of
rosiglitazone and 15-deoxy-D12,14-prostaglandin J2 on bleomycin-induced lung injury. Eur. Respir. J.
25 (200) 225–234.

21
[10]. R.W. Thomsen, A. Riis, J.B. Kornum, S. Christensen, S.P. Johnsen, H.T. Sorensen, Preadmission
use of statins and outcomes after hospitalization with pneumonia: population-based cohort study of
29,900 patients. Arch. Intern. Med. 168 (2008) 2081-2087.
[11]. A.H. Wagner, T. Kohler, U. Ruckschloss, I. Just, M.Hecker, Improvement of nitric oxide-
dependent vasodilatation by HMG-CoA reductase inhibitors through attenuation of endothelial
superoxide anion formation. Arterioscler. Thromb. Vasc. Biol. 20 (2000) 61-69.
[12]. Y. Ye, S.P. Nishi, S. Manickavasagam, Y. Lin, M.H. Huang, J.R. Perez-Polo, B.F. Uretsky, Y.
Birnbaum, Activation of peroxisome proliferator-activated receptor-g (PPAR-γ) by atorvastatin is
mediated by 15-deoxy-delta-12,14-PGJ2. Prostaglandins Other Lipid Mediat. 8 (2007) 43-53.
[13]. W.G. Jr Niehaus, B.Samuelsson, Formation of malonaldehyde from phospholipid arachidonate
during microsomal lipid peroxidation. Eur. J. Biochem. 6 (1968) 126-130.
[14]. O.H. Lowry, N.J. Rosebrough, A.L. Farr, R.J. Randall, Protein measurement with the Folin phenol
reagent. J. Bio. Chem. 193 (1951) 265-275.
[15]. S. Cuzzocrea, A. Ianaro, N.S. Wayman, E. Mazzon, B. Pisano, L. Dugo, I. Serraino, R. Di Paola,
P.K. Chatterjee, M. Di Rosa, A.P. Caputi, C. Thiemermann,The cyclopentenone prostaglandine 15-
deoxy-delta (12, 14)-PGJ2 attenuates development of colon injury caused by dinitrobenzene sulphonic
acid in the rat. Br. J. Pharmacol. 138 (2003) 678-688.
[16]. L.C. Green, D.A. Wagner, J. Glogowski, P.L. Skipper, J.S. Wishnok, S.R. Tannenbaum, Analysis
of nitrate, nitrite, and [15N] nitrate in biological fluids. Ana. L. Biochem. 126 (1982) 131-138.
[17]. P. Chomczynski, N.Sacchi, The single-step method of RNA isolation by acid guanidinium
thiocyanate-phenol-chloroform extraction: twenty-something years on. Nat. Protoc. 1 (2006) 581–585.
[18]. A.V. Ershov, N.G.Bazan, Induction of cyclooxygenase-2 gene expression in retinal pigment
epithelium cells by photoreceptor rod outer segment phagocytosis and growth factors. J. Neurosci. Res.
58 (1999) 254-261.

22
[19]. M. Shibata, T. Hariya, M. Hatao, T. Ashikaga, H. Ichikawa, Quantitative polymerase chain
reaction using an external control mRNA for determination of gene expression in a heterogeneous cell
population. Toxicol. Sci. 49 (1999) 290-296.
[20]. B.K. Edmonds, G.L. Edwards, The area postrema is involved in paraquat induced conditioned
aversion behavior and neuroendocrine activation of the hypothalamic–pituitary–adrenal axis. Brain Res.
712 (1996) 127–133.
[21]. W. Samy, M.A. Hassanian, Paraoxonase-1 activity, malondialdehyde and glutathione peroxidase
in non-alcoholic fatty liver disease and the effect of atorvastatin. Arab. J. Gastroenterol. 12 (2011) 80–
85.
[22]. H.C. Yu, S.F. Feng, P.L. Chao, A.M. Lin, Anti-inflammatory effects of pioglitazone on iron-
induced oxidative injury in the nigrostriatal dopaminergic system. Neuropathol. Appl. Neurobiol. 36
(2010) 612–622.
[23]. J.G. Wagner, R.A. Roth, Neutrophil Migration Mechanisms, with an Emphasis on the Pulmonary
Vasculature. Pharmacol. Rev. 52 (2000) 349–374.
[24]. D.M. Hyde, L.A. Miller, R.J. McDonald, M.Y. Stovall, V. Wong, K.E. Pinkerton, C.D. Wegner, R.
Rothlein, C.G. Plopper, Neutrophils enhance clearance of necrotic epithelial cells in ozone-induced lung
injury in rhesus monkeys. Am. J. Physiol. 277 (1999) L1190- L1198.
[25]. R. Manzer, J. Wang, K. Nishina, G. McConville, R.J. Mason, Alveolar Epithelial Cells Secrete
Chemokines in Response to IL-1_ and Lipopolysaccharide but Not to Ozone. Am. J. Respir. Cell Mol.
Biol. 34 (2006) 158–166.
[26]. M. Låg, D. Rodionov, J. Øvrevik, O. Bakke, P.E. Schwarze, M. Refsnes, Cadmium-induced
inflammatory responses in cells relevant for lung toxicity: Expression and release of cytokines in
fibroblasts, epithelial cells and macrophages. Toxicol. Lett. 193 (2010) 252–260.

23
[27]. Z. Haskova, B. Hoang, G. Luo, L.A. Morgan, A.N. Billin, F.C. Barone, B.G. Shearer, M.E. Barton,
K.S. Kilgore, Modulation of LPS-induced pulmonary neutrophil infiltration and cytokine production by
the selective PPARb/d ligand GW0742. Inflamm. Res. 57 (2008) 314–321.
[28]. D. Laskin, R. Malaviya, A. Venosa, A. Gow, D. Heck, J. Laskin, Role of reactive nitrogen species
(RNS) generated via inducible nitric oxide synthase in vesicant-induced lung injury and inflammation.
Abstracts Niox. 27 (2012) S2–S50.
[29]. J. Berger, D.E. Moller, The mechanisms of action of PPARs. Annu. Rev. Med. 53 (2002) 409-435.
[30]. O. Braissant, F. Foufelle, C. Scotto, M. Dauça, W. Wahli, Differential expression of peroxisome
proliferator-activated receptors (PPARs): tissue distribution of PPARα, β, and γ in the adult rat.
Endocrinology. 137 (1996) 354–366.
[31]. Y. Zhao, A. Patzer, T. Herdegen, P. Gohlke, J. Culman, Activation of cerebral peroxisome
proliferator-activated receptors gamma promotes neuroprotection by attenuation of neuronal
cyclooxygenase-2 overexpression after focal cerebral ischemia in rats. FASEB. J. 20 (2006) 1162–1175.
[32]. B. Xing, T. Xin, R.L. Hunter, G. Bing, Pioglitazone inhibition of lipopolysaccharide-induced
nitric oxide synthase is associated with altered activity of p38 MAP kinase and PI3K/Akt. J.
Neuroinflammation. 5 (2008) 5:4.
[33]. G. Orasanu, Q. Ziouzenkova, P.R. Devchand, V. Nehra, O. Hamdy, E.S. Horton, J. Plutzky , The
peroxisome proliferator-activated receptor-g agonist pioglitazone represses inflammation in a
peroxisome proliferator-activated receptor-a dependent manner in vitro and in vivo in mice. J. Am. Coll.
Cardiol. 52 (2008) 869-881.
[34]. B. Rinaldi, M. Donniacuo, E. Esposito, A. Capuano, L. Sodano, E. Mazzon, et al. PPARα mediates
the anti-inflammatory effect of simvastatin in an experimental model of zymosan-induced multiple
organ failure. Br. J. Pharmacol. 163 (2011) 609–623.

24
[35]. Z. Hussein, J.M. Wentworth, A.J. Nankervis, J. Proietto, P.G. Colman, Effectiveness and side
effects of thiazolidinediones for type 2 diabetes: real-life experience from a tertiary hospital. Med. J.
Aust. 181 (2004) 536–539.
[36]. M. Jasin´ska, J. Owczarek, D. Orszulak-Michalak, Statins: a new insight into their mechanisms of
action and consequent pleiotropic effects. Pharmacol. Rep. 59 (2007) 483–499.
[37]. R. Paumelle, C. Blanquart, O. Briand, O. Barbier, C. Duhem, G. Woerly, F. Percevault, J.C.
Fruchart, D. Dombrowicz, C. Glineur, B. Steals, Acute anti-inflammatory properties of statins involve
peroxisome proliferator-activated receptor-alpha via inhibition of the protein kinase C signaling
pathway. Circ. Res. 98 (2006) 361–369.
[38]. A. Planavila, J.C. Laguna, M. Va´zquez-Carrera, Atorvastatin improves peroxisome proliferator-
activated receptor signaling in cardiac hypertrophy by preventing nuclear factor-kappa B activation.
Biochim. Biophys. Acta. 1687 (2005) 76–83.
[39]. O. Grip, S. Janciauskiene, S. Lindgren, Atorvastatin activates PPAR-gamma and attenuates the
inflammatory response in human monocytes. Inflamm. Res. 51 (2002) 58–62.
[40]. J. Lee, E.M. Hong, D.H. Koh, M.H. Choi, H.J. Jang, S.H. Kae, H.S. Choi, HMG-CoA Reductase
Inhibitors (Statins) Activate Expression of PPARa/PPARg and ABCA1 in Cultured Gallbladder
Epithelial Cells. Dig. Dis. Sci. 55 (2010) 292–299.
[41]. Y. Shen, H. Wu, C. Wang, H. Shao, H. Huang, H. Jing, D. Li , Simvastatin attenuates
cardiopulmonary bypass-induced myocardial inflammatory injury in rats by activating peroxisome
proliferator-activated receptor γ. Eur. J. Pharmacol. 649 (2010) 255–262.
[42]. A.P. Kumar, W.F. Reynolds, Statins downregulate myeloperoxidase gene expression in
macrophages. Biochem. Biophys. Res. Commun. 331 (2005) 442–451.

25
[43]. M. Massaro, A. Zampolli, E. Scoditti, M.A. Carluccio, C. Storelli, A. Distante, R. De Caterina,
Statins inhibit cyclooxygenase-2 and matrix metalloproteinase-9 in human endothelial cells: anti-
angiogenic actions possibly contributing to plaque stability. Cardiovasc. Res. 86 (2010) 311–320.
[44]. S. Wu, S. Duan, S. Zhao, Y. Cai, P. Chen, X. Fang , Atorvastatin reduces lipopolysaccharide-
induced expression of cyclooxygenase-2 in human pulmonary epithelial cells. Respir. Res. 6 (2005) 27.

26
Table 1: neuclotid sequences, anneling tempratures and products size for primers used in RT-PCR
Target Gene Primer Sequence (5’-3’) Product Size (bp) AT (°C)
COX-2 FWD: TGGTGCCGGGTCTGATGATG 252 59
REW: GCAATGCGGTTCTGATACTG
GAPDH FWD: GTTACCAGGGCTGCCTTCTC 167 63 RVS: GGGTTTCCCGTTGATGACC
AT: annealing temperature, bp: base pair
Table 2: Effect of pioglitazone and atorvastatin on histological architecture of the lungs in the PQ-exposed rats; mean values ± SD are given.
Groups Hemorrhages MNIC-Infiltration Hyaline Exudate presence
C 0.0 a 0.0 a 0.0 a PQ 8.4 ± 1.4 b 7.2 ± 1.2 b 6.4 ± 0.9 b PGT 5.4 ± 0.6 c 6.2 ± 1.7 b 5.8 ± 1.4 b STN 3.4 ± 0.8 d 4.4 ± 0.7 c 3.2 ± 1.2 c PGT + STN 7.7 ± 2.1b 6.7 ± 1.4 b 5.8 ± 1.3 b PGT + GW9662 5.9 ± 1.4 c 6.4 ± 1.6 b 6.2 ± 1.8 b STN + GW9662 7.7 ± 2.1b 6.9 ± 1.1b 5.9 ± 0.7 b
abcd: values in same column with different superscripts differ significantly ( P < 0.05). C = Control, PQ = Paraquat, PGT = Pioglitazone, STN = Atorvastatin, MNIC = Mono-nuclear inflammatory cells

27
Figure Legends:
Fig. 1:Fig. 1:Fig. 1:Fig. 1: Effect of PGT and STN on the PQ-reduced body weight gain (g), data is given as Mean ± SD
(n=6). * is indicating a significant difference (P<0.05) between the control and PQ-exposed groups and
# represents a significant difference between the non-treated PQ-exposed and treated groups.
Fig. 2:Fig. 2:Fig. 2:Fig. 2: Effect of PGT and STN on the PQ-elevated lipid peroxidation rate in the lungs, Data is given as
Mean ± SD (n=6). * is indicating a significant difference (P<0.05) between the control and PQ-exposed
groups and # represents a significant difference between the non-treated PQ-exposed and treated groups.
Figure 3Figure 3Figure 3Figure 3: Effect of PGT and STN on: (A) the PQ-elevated NO concentration and (B) the MPA activity
in the lungs, Data is given as Mean ± SD (n=6). * is indicating a significant difference (P<0.05) between
the control and PQ-exposed groups and # represents a significant (P<0.05) difference between the non-
treated PQ-exposed and treated groups. #† indicate a significant difference (P<0.01) between the non-
treated PQ-exposed and treated groups.
Figure 4Figure 4Figure 4Figure 4: Effect of PGT and STN on: (A) the PQ-elevated serum level of IL-6 and (B) TNF-α, Data is
given as Mean ± SD (n=6). * is indicating a significant difference (P<0.05) between the control and PQ-
exposed groups and # represents a significant difference (P<0.05) between the non-treated PQ-exposed
and treated groups. #† indicate a significant difference (P<0.01) between the non-treated PQ-exposed
and treated groups.
Figure 5Figure 5Figure 5Figure 5: Photomicrograph of rat's Lungs, (A) control; normal alveoli with non-edematous connective
tissue, (B) PQ-exposed group; interstitial inflammation and thickening along with severe hemorrhages
(tin arrows), hyperplasia in airways (tick arrows) and mono-nuclear inflammatory cells along with
macrophages infiltration (arrow head) are seen, (C) PGT-treated group: Emphysema and hyaline
exudate in alveoli (tin arrows), edema and interstitial inflammation (tick arrow) and increased number of
macrophages (arrow head) are shown, (D) STN-treated animals; reduced hyaline exudate and alveolar
edema (tin arrow), declined edema and interstitial inflammation (tick arrow) and few macrophages and

28
mono-nuclear inflammatory cells (arrow head) are demonstrated, (E) PGT and STN received rats;
accumulation of hyaline exudate inside the alveoli and injured vessels (tin arrows), presence of
inflammatory cells around injured vessels and airways (tick arrow) and re-epithelialization of alveoli
(arrow head) are seen, (F) PGT plus GW9662 treated animals; edematous alveoli and hyaline exudate
(tin arrow), increasing number of inflammatory cells around the hyperplastic airway (tick arrow) and the
presence of lymphocytes and macrophages inside the alveoli are represented, and (G) STN plus
GW9662 treated animals; increased hemorrhages and accumulated hyaline exudate inside the alveoli (tin
arrow), severe hyperplasia in airways (tick arrow) and interstitial inflammation along with mono-nuclear
inflammatory cells infiltration (arrow head) are observed. Hematoxylin & Eosin staining, 100X and
scale = 50 µm
Figure 6Figure 6Figure 6Figure 6: Photomicrograph of rat's Lungs, (A) control; normal alveoli with no CD68 positive
macrophages, (B) PQ-exposed animals; the presence of numerous intra cytoplasmic CD68 positive
macrophages (arrow) within lung parenchyma are represented. The numbers of CD68 positive
macrophages have been reduced remarkably in the PGT-treated (C) and STN-received (D) animals.
Despite of the cumulative presence of other inflammatory cells in the lungs of PGT and STN co-
administered (E), PGT plus GW9662 received (F) and STN plus GW9662 treated(G) animals, no CD68
positive macrophages was detected. Immunohistocemical staining, scale = 20 µm
Figure 7: Effect of PGT and STN on: (A) the GAPDH (167 bp) and COX-2 (252 bp) mRNA levels in
the lungs tissue, the levels of COX-2 and GAPDH mRNA were evaluated by semi-quantitative RT-
PCR, and (B) represents the density of COX-2 mRNA in the lungs that were measured by densitometry
and normalized to GAPDH mRNA expression level. Results were expressed as integrated density values
(IDV) of COX-2 mRNA level. * is indicating a significant difference (P<0.05) between the control and
PQ-exposed groups and # represents a significant difference between the non-treated PQ-exposed and
treated groups.

Figure 1
-40
-30
-20
-10
0
10
20
30
40
50B
od
y W
eig
ht
Ga
in (
g)
#
#
#
*

Figure 2
0.00
0.50
1.00
1.50
2.00
2.50
3.00
3.50
4.00
4.50
MD
A [
nm
ol/
mg
of
pro
tein
]*
#
#
#

Figure 3
(A)
(B)
0
20
40
60
80
100
120
140
160
NO
[n
mo
l/m
g o
f p
rote
in] *
#
##
##
0
10
20
30
40
50
60
70
80
90
MP
O [
U/m
g o
f p
rote
in]
*
#
#
#†
#

Figure 4 (A)
(B)
0
50
100
150
200
250
IL-6
(p
g/m
l)
*
##
#
0
10
20
30
40
50
60
70
TN
F- αα αα
(pg
/ml)
*
##
#†
#

Figure 5
(A) (B)
(C) (D)
(E) (F)
(G)

Figure 6
(A) (B)
(C) (D)
(E) (F)
(G)

Figure7
(A) (B)
(C)
0.00
0.10
0.20
0.30
0.40
0.50
0.60
0.70
0.80
CO
X-2
/GA
PD
H
* #
#
#
#
#
GAPDH (176 bp)
COX-2 (252 bp)

29
Table 1: neuclotid sequences, anneling tempratures and products size for primers used in RT-PCR
Target Gene Primer Sequence (5’-3’) Product Size (bp) AT (°C)
COX-2 FWD: TGGTGCCGGGTCTGATGATG 252 59 REV: GCAATGCGGTTCTGATACTG
GAPDH FWD: GTTACCAGGGCTGCCTTCTC 167 63 REV: GGGTTTCCCGTTGATGACC

30
Table 2: Effect of pioglitazone and atorvastatin on histological architecture of the lungs in the PQ-
exposed rats; mean values ± SD are given. Groups Hemorrhages MNIC-Infiltration Hyaline Exudate presence
C 0.0 a 0.0 a 0.0 a PQ 8.4 ± 1.4 b 7.2 ± 1.2 b 6.4 ± 0.9 b PGT 5.4 ± 0.6 c 6.2 ± 1.7 b 5.8 ± 1.4 b STN 3.4 ± 0.8 d 4.4 ± 0.7 c 3.2 ± 1.2 c PGT + STN 7.7 ± 2.1b 6.7 ± 1.4 b 5.8 ± 1.3 b PGT + GW9662 5.9 ± 1.4 c 6.4 ± 1.6 b 6.2 ± 1.8 b STN + GW9662 7.7 ± 2.1b 6.9 ± 1.1b 5.9 ± 0.7 b abcd: values in same column with different superscripts differ significantly ( P < 0.05). C = Control, PQ = Paraquat, PGT = Pioglitazone, STN = Atorvastatin, MNIC = Mono-nuclear inflammatory cells

31
Highlights: This study highlighted:
1- Paraquat produces respiratory inflammation via PPARγ receptor;
2- Biochemical and immunohistochemical alterations in the lungs following PQ-intoxication were clarified;
3- Atorvastatin reduced significantly the PQ-induced alteration in the lung tissue;
4- Atorvastatin induced protection against PQ-induced damages was found to mediated through PPARγ
receptors



![SolarNeutrinos - SLAC National Accelerator Laboratory · The solar neutrino problem has been present since early 1970 [2], well be- fore the first indication of the atmospheric neutrino](https://static.fdocument.org/doc/165x107/5e61b908bc7bcf5faa095535/solarneutrinos-slac-national-accelerator-laboratory-the-solar-neutrino-problem.jpg)