APPARENT MINERALOCORTICOID EXCESS AND DEFICIENT 11β-OXIDATION OF CORTISOL IN A YOUNG FEMALE
10
Clinical Endocrinology (1 984) 21, 505-5 14 APPARENT MINERALOCORTICOID EXCESS AND IN A YOUNG FEMALE DEFICIENT 11b-OXIDATION OF CORTISOL H. I. J. HARINCK, P. VAN BRUMMELEN, A. P. VAN SETERS AND A. J. MOOLENAAR Departments of Endocrinology, Nephrology and Chemical Pathology, Uniiiersity Hospital, Leiden, The Netherlands (Received 16 February 1984: reoised 29 May 1984: accepted8 June 1984) SUMMARY A 19-year-old female, known to have had hypertension and hypokalemic alkalosis since the age of 9 months, was found to have suppressed renin, negligible plasma and urinary aldosterone and low plasma levels of other known sodium-retaining steroids. Despite the normal plasma cortisol the urinary excretion of 17-oxosteroids and 17-oxogenic steroids was low as was the cortisol secretion rate, suggesting a diminished metabolic clearance of cortisol. This was confirmed by the demonstration of a prolonged tt of I4C-cortisol. The abnormally high urinary excretion ratios of cortisol to cortisone, tetrahydracor- tisol to tetrahydrocortisone and 1 l-hydroxy-aetiocholanolone to 1 I-oxy-aetio- cholanolone indicate that the diminished cortisol breakdown is the result of deficient 1 1 /J-oxidation. Moreover, the urinary excretion of free cortisol was elevated, probably due to diminished tubular reabsorption of cortisol. Hypoka- lemic alkalosis did not respond to spironolactone, but was partly corrected by amiloride. No response to dexamethasone was observed, but dexamethasone combined with aminogluthetimide normalized blood pressure and serum K. These findings support the involvement of a sodium-retaining, kaliuretic steroid in this rare syndrome. Hypertension with suppressed renin and hypokalemic alkalosis is usually caused by overproduction of aldosterone or one of the other known mineralocorticoids, such as deoxycorticosterone (DOC) and 1 8-hydroxy-deoxycorticosterone (1 8-OH-DOC) (Big- lieri, 198 1). However, in some cases no mineralocorticoid excess can be demonstrated. Liddle et al. (1963) described a family with a primary abnormality of renal tubular sodium transport that causes a syndrome with similar characteristics. More recently, another syndrome of apparent mineralocorticoid excess was reported (Ulick et al., 1977; Shackleton et al., 1980; Fiselier et al., 1982).In these patients a defect in Correspondence: H. I. J. Harinck, Department of Endocrinology, University Hospital, Rijnsburgerweg 10, 2333 AA Leiden, The Netherlands. 505
-
Upload
h-i-j-harinck -
Category
Documents
-
view
218 -
download
3
Transcript of APPARENT MINERALOCORTICOID EXCESS AND DEFICIENT 11β-OXIDATION OF CORTISOL IN A YOUNG FEMALE

Clinical Endocrinology (1 984) 21, 505-5 14
APPARENT MINERALOCORTICOID EXCESS AND
IN A YOUNG FEMALE DEFICIENT 11b-OXIDATION OF CORTISOL
H. I. J. HARINCK, P. VAN BRUMMELEN, A. P. VAN SETERS AND
A . J . MOOLENAAR
Departments of Endocrinology, Nephrology and Chemical Pathology, Uniiiersity Hospital, Leiden, The Netherlands
(Received 16 February 1984: reoised 29 May 1984: accepted8 June 1984)
SUMMARY
A 19-year-old female, known to have had hypertension and hypokalemic alkalosis since the age of 9 months, was found to have suppressed renin, negligible plasma and urinary aldosterone and low plasma levels of other known sodium-retaining steroids. Despite the normal plasma cortisol the urinary excretion of 17-oxosteroids and 17-oxogenic steroids was low as was the cortisol secretion rate, suggesting a diminished metabolic clearance of cortisol. This was confirmed by the demonstration of a prolonged tt of I4C-cortisol. The abnormally high urinary excretion ratios of cortisol to cortisone, tetrahydracor- tisol to tetrahydrocortisone and 1 l-hydroxy-aetiocholanolone to 1 I-oxy-aetio- cholanolone indicate that the diminished cortisol breakdown is the result of deficient 1 1 /J-oxidation. Moreover, the urinary excretion of free cortisol was elevated, probably due to diminished tubular reabsorption of cortisol. Hypoka- lemic alkalosis did not respond to spironolactone, but was partly corrected by amiloride. No response to dexamethasone was observed, but dexamethasone combined with aminogluthetimide normalized blood pressure and serum K. These findings support the involvement of a sodium-retaining, kaliuretic steroid in this rare syndrome.
Hypertension with suppressed renin and hypokalemic alkalosis is usually caused by overproduction of aldosterone or one of the other known mineralocorticoids, such as deoxycorticosterone (DOC) and 1 8-hydroxy-deoxycorticosterone ( 1 8-OH-DOC) (Big- lieri, 198 1). However, in some cases no mineralocorticoid excess can be demonstrated. Liddle et al. (1963) described a family with a primary abnormality of renal tubular sodium transport that causes a syndrome with similar characteristics.
More recently, another syndrome of apparent mineralocorticoid excess was reported (Ulick et al., 1977; Shackleton et al., 1980; Fiselier et al., 1982). In these patients a defect in
Correspondence: H. I. J. Harinck, Department of Endocrinology, University Hospital, Rijnsburgerweg 10, 2333 AA Leiden, The Netherlands.
505

506
the metabolism of cortisol was demonstrated, although the relation between this steroidal abnormality and the clinical picture has not been fully elucidated (New el ul.. 1982). In this paper we present another case of this rare syndrome together with further evidence for the steroid dependency of the low renin hypertension and hypokalemic alkalosis.
H . I. J. Harinck et al.
CASE REPORT
This Caucasian patient (A) was first admitted to the hospital at the age of 9 months, because of failure to thrive and hypertension (blood pressure l 5 O / l O O mmHg). She exhibited hypokalemia (serum K: 3.0 mmol/l) hypernatraemia (serum Na: 149 mmol/l) and metabolic alkalosis (capillary pH: 7.58; bicarbonate: 32 mmol/l). No diagnosis was made. A low-sodium diet and potassium supplements were prescribed, resulting in partial improvement of the hypertension and hypokalemia. During subsequent admissions in her childhood, a suppressed plasma renin activity was demonstrated, but primary hyperal- dosteronism was excluded by the finding of a low urinary excretion of aldosterone. Her physical and mental development were normal; menarche was at the age of 13 years.
The patient returned to our hospital for re-evaluation of her condition at the age of 19 years. She was still on a low-sodium diet (20 mmol Na/day) and potassium supplements. At physical examination she appeared very slender (height: 1.53 m; weight: 40 kg), but was otherwise normal. Blood pressure ranged from 120/80 to 145/100 mmHg. Mild arterial stretching was present in the ocular fundi. An electrocardiogram showed changes consistent with hypokalemia. The thickness of the left ventricular wall (9.5 mm) and the intraventricular septum (1 1 mm), as measured by echocardiography, was at the upper limit of normal, suggesting left ventricular hypertrophy.
Laboratory investigations: serum Na, 143 mmol/l; serum K, 3.2 mmol/l; serum CI, 97 mmol/l; capillary pH, 7.55 and bicarbonate, 30 mmol/l. Urinalysis, creatinine clearance, liver function tests, serum T4 and T3-resin uptake were normal. While on a Na intake of 50 mmol/day. plasma renin activity (PRA) was 12 ng/lO m1/3 h (normal range 115-595 ng/lO m1/3 h). Plasma levels of aldosterone (PA), DOC, 18-OH-DOC, corticosterone and 18-hydroxy-corticosterone were subnormal or in the low-normal range (Table 1). Plasma
Table I . Basal plasma levels of corticosteroids and their response to intramuscular administration of ACTH and dexamethasone
ACTH Dexamethasone
Baseline 8 h post 24 h post
Doc 0 2 4 2 7 2.0 18-OH-DOC <0-03 0.84 0 67 Corticosterone 5.3 32.3 22.1 18-OH-Corticosterone 0.32 1.0 0.52 Aldosterone 0.07 0.13 0.13 1 1-Deoxycortisol 3.2 7.8 7.9 Cortisol 0.37 0.78 0.69
(2 mg/d) day 10
0.15 0.09
0 I 2 0.07 1.7 0.03
19.4
Normal range (nmol/l)
~
0.12-0.41 0.09-0.38
3.8-23.7 0 4 6 1 . 2 0 , 0 8 4 6 7
0.16450* 0.87-5-8
DOC. deoxycorticosterone; 18-OH-DOC, 18-hydroxy-deoxycorticosterone. * pnol:l.

Hypertension and de3cient cortisol metabolism 507
Table 2. Urinary steroids of patient A before and during administration of ACTH, hydrocortisone and dexamethasone and basal values of a hypothyroid patient (patient B) and normal females (range; mean & 1 SD)
Patient A Normal females (n=16, age
ACTH hydrocortisone dexamethasone Patient B 17-28 years) Basal (day 1) (day 1) (day 10) Basal Basal
Free cortisol (n mo1/24 h) 17-0s (pmo1/24 h) 17-OGS (pmo1/24 h) PD (pmo1/24 h) PT (pmo1/24 h) A + E (pmo1/24 h) OHA (pmo1/24 h) OHEjOE (pmol/pmol) E/A (pmol/pmol)
306 9.0
11 0.28 0.50 2.4 0.88 2.6 0.57
1140 39
22.5 0.41 1 .o 4.1 2.1
12.5 0.51
2600
139 0.16 0.24 2.4 5.1 72 0.54
30.5 29 15 5.2 0.53 0.03 2.9 0.23 6.0 0.54
70 9.3 26 0.56 I .o 2.3 0.29 0.83 6.1
55-200 14-59 28-63
0.78-9.8 1.8& 1.04
18.4 4.75 2.65 k 0.58 0.17 & 0.24 0.98 & 0.27
Abbreviations: PD, pregnanediol; PT, pregnanetriol; A, androsterone; E, aetiocholanalone; OHA. 1 l-hydrox- yandrosterone; OHE, I I-hydroxy-aetiocholanolone; OE, 1 I-oxy-aetiocholanolone.
cortisol levels exhibited a normal circadian rhythm (0800 h, 0.37; 1700 h, 0.13; 2300 h, 0.08 pmol/l). The urinary excretion of 17-oxogenic steroids (17-OGS) and 17-oxosteroids (1 7-0s) was far below normal (Table 2, Figs 1, 2). Plasma levels of gonadotrophins, oestrogens and progesterone and the urinary excretion of oestrogens were normal as were changes during the menstrual cycle (data not given). Salivary sodium-potassium ratio was decreased (0.15; normal range 0.60-3.30). Erythrocytes had a normal Na and K content and the total and ouabain-sensitive fluxes of these electrolytes were also normal. A CT scan revealed normal adrenal glands. Both parents and her brother had a normal blood pressure and normal serum K levels.
METHODS
The patient was hospitalized for 32 days for a series of short-term tests (first study period). Upon discharge she was placed on an amiloride regimen; 3 months later she was readmitted for further evaluation (second study period). She was on a constant diet, that was analyzed for electrolyte content. An increase in Na intake during the first study period was obtained by adding NaCl capsules to her diet. Blood pressure was measured every three hours after the patient had been supine for 10 min. Venous blood samples and saliva were taken at 8 h, when the patient was still in the supine position and body weight was measured daily before breakfast. Daily 24 hour urine collections were obtained for measurement of creatinine and electrolytes. Urinary 17-0s and 17-OGS were measured as proposed by the Medical Research Council (1963). Pregnanediol (PD), Pregnanetriol (PT) and the individual 17-0s were assayed by gas-liquid chromatography (GLC) after enzymatic hydrolysis and solvolysis (Moolenaar & van Seters, 1971). Urinary and plasma cortisol were estimated by radioimmunoassay as were PRA and PA (Drayer & Benraad, 1970; de Man et al., 1980). Plasma DOC, 18-OH-DOC, corticosterone, 18-OH-corticos- terone and 1 1 -deoxycortisol were measured by radioimmunoassay after extraction and

508 H . I . J . Harinck et a/ .
1 L O BLOOD PRESSURE 100 mmHg
6 0
P R A ng/ 3 h/ 10 ml 12 12 16
160
intoke URINARY
No' mmoi iaoy
STEROIDS
days I I I I I 5 1 I I I I 101 1 I I 151 I 1 I I 201 I I I I 251 1 I I I 30, 1
A ' 8 ' C
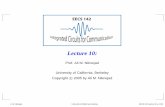
Fig. 1. Serum K, plasma renin activity. urinary sodium. potassium and 17-OGS as well as blood pressure and body weight during various periods of treatment.
paper chromatographic purification (Hoefnagels ef al.. 1978). ACTH assays were carried out with an Amersham Kit. Cortisol secretion rate wasestimated according to the method of Norymberski er ul. (l953), using 17-OGS excretion before and after the administration of 25 mg hydrocortisone four times daily for 3 days. 14C-cortisol (2.3 pCi, Amersham) was administered intravenously. The IT-cortisol metabolites were extracted with dichloro- methane (unconjugated steroids) and then with ethylacetate after hydrolysis with glucuronidase. Paper chromatography was performed in a toluene : methanol : water system, 4: 3 : 1 (by vol). Blood samples (with 'H-cortisol added to correct for losses) were extracted with dichloromethane and developed in the same system. For comparison 14C-cortisol studies of a normal Caucasian female control and a Caucasian woman with primary hypothyroidism (T4 < 10 nmol/l, TSH 50 mU/l) were also performed.The assay of cortisol-binding globulin (CBG) was kindly performed in the Rega Institute, Louvain, Belgium (van Baelen & de Moor, 1974). Erythrocyte Na and K content and ouabain- sensitive Na and K fluxes after cold treatment were measured as described by Post & Jolly (1957).
RESULTS Clinical biudies
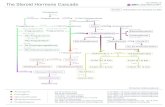
Mean daytime and night-time blood pressure, body weight, serum K and urinary excretion of K. Na and 17-OGS are shown in Figs 1 and 2.

Hyper tension and deficient coy t is01 metabolism
I
509
I
DEXAMETHASONE. 2 rng Id I AMINOGLUTETHIHIDE. 1 grnldl
AMILORIOE, 10 rng Id]
a
I
1LO BLOOD PRESSURE 100 rnrnHg
A B C
36 PRA ng/3 hr/mrnl 53 52
URINARY dietary Na‘ intake rnrnol /day
STEROIDS prnol /day
First study period Baseline period
Dietary Na intake (50 mmol/day) was more than twice the amount she used at home. K intake was 70 mmol/day. The rise in urinary Na excretion was accompanied by a transient increase in urinary K excretion and a drop in serum K from 3.2 to 2.3 mmol/l. Blood pressure (1 30/85 mmHg) was slightly elevated for this slender girl. See Fig. 1 a.
ACTH test A single i.m. injection of 1 mg synthetic 1-24 ACTH (Synacthen depot) induced a
pronounced rise in the plasma levels of all adrenal steroids measured (Table 1). The urinary excretion of 17-OGS and 17-0s rose two to threefold (Table 2) and reached levels normally obtained as basal values. No rise in blood pressure or drop in serum K was found after this short-term stimulation of the adrenal cortex. In fact a decrease in urinary K excretion and slight increase in serum K to 2.9 mmol/l were observed. See Fig. 1 b.
Dexamethasone administration When dexamethasone (2 mg/d) was given for 12 d, slight increases in body weight and
blood pressure were observed. No changes in serum K or urinary Na and K were seen. It should be noted that despite an increase in dietary Na intake to 100 mmol/d, serum K remained above the levels found in the baseline period. PA (0.07 nmol/l) and PRA (12

510 H . I . J. Harinck et al.
ng/lO m1/3 h) remained low. Low values of plasma cortisol (0.03 pmol/l) and urinary free cortisol (29 nmol/d) indicate a proper intake of dexamethasone. See Fig. lc.
Spironolactone administration Treatment with spironolactone (200 mg/d for 5 d) normalized blood pressure (1 15/70
mmHg). Neither serum K nor the urinary Na/K ratio showed significant changes and PA (0.13 nmol/l) and PRA (16 ng/lO m1/3 h) remained low.
Am ilor ide adm in is I ru t ion Administration of amiloride (1 0 mg/d) was immediately followed by a transient
natriuresis and potassium retention. Serum K rose to 4.3 mmol/l and blood pressure ( I 20/70 mmHg) remained normal.
The patient was then discharged; a regimen of amiloride (10 mg/d) and a dietary Na intake of 100 mmol/d were prescribed.
Second study period Long-term amiloride treatment
The patient was readmitted three months later. Dietary Na and K intake were maintained at 90 and 95 mmolid, respectivcly. Mean blood pressure was 130/80 mmHg. Serum K (3.2 mmol/l) was again subnormal and PRA (36 ng/lO m1/3 h) and PA (0.14 nmol/l) were still low. Discontinuation of amiloride treatment resulted in a decrease in serum K to 2.5 mmol/l. See Fig. 2a.
A dm in is tra t ion of urn in og lir te t h im ide and ilesame tliasone Aminoglutethimide (1000 mg/d) and dexamethasone (2 nig/d) were given simul-
taneously. After an initial fall, urinary Na excretion increased markedly. There was a slight drop in blood pressure (120/70 mmHg) and body weight. Urinary K decreased, serum K rose gradually to 4.2 mmol/l and alkalosis was corrected (pH 7.40; bicarbonate, 24 mmol/l). Salivary Na/K ratio rose slightly from 0.15 to 0.20. As expected the levels of PA (0.1 1 mmol/l), plasma cortisol (0.06 pmol/l) and ACTH (20 U/1; normal range 2&80) and urinary excretion of free cortisol (30 nmolid) were low during this period. PRA increased to 53 ng/lO m1/3 h, but remained low. During ongoing treatment serum K decreased to 3.4 mmol/l. See Fig. 2b.
Administration of aldosterone and discontintration o ~ a ~ i i r i o ~ l i i t e t ~ i i ~ i i d e Intravenous administration of 0.5 mg aldosterone over 12 h did not result in a
pronounced drop in serum K or major changes in the urinary Na/K ratio. Aminoglutethi- midc was then discontinued because of complaints of' dizziness. During treatment with dexamethasone alone serum K decreased further to 2.9 mmol/l. See Fig. 2c.
Outputient ,follon* up
After discharge spironolactone (up to 300 mg/d) was administered for 3 months and Na intake was around 100 mmolid. These dosages of spironolactone induced troublesome side effects, including disturbed menstruation and headache. Neither serum K (2.4-3.0 mmol/l) nor blood pressure (130-1 50 mmHg systolic; 90-100 mmHg diastolic) norma-

Hypertension and deficient cortisol metabolism 51 1
lized. The patient has now been taking amiloride (1 5 mg/d) for 3 years. Na intake is still around 100 mmol/d. On this regimen blood pressure remains slightly elevated (140-160 mmHg systolic, 95-100 mmHg diastolic) and serum K varies between 3 4 4 . 1 mmol/l.
Cortisol metabolism
Low basal values were obtained for the excretion of 17-OGS and 17-0s (Table 2, Figs 1, 2) and the cortisol secretion rate (8 mg/24 h), whereas free cortisol excretion was elevated (Table 2). Plasma cortisol (Table I), ACTH (40 IU/l) and CBG (41.9 mg/l; normal range 33-50) were normal. The plasma disappearance rate of ''C-cortisol was prolonged (t! 109 min; normal range 6&90) and 14C-excretion was delayed when compared with the normal control (Table 3). 14C-activity in a dichloromethane extract without prior hydrolysis did not greatly differ from that for the normal control. Highly abnormal values were obtained for cortisol and the three radioactive Czl-cortisol metabolites measured (Table 4). The excretion of cortisol (1.89% dose) and tetrahydrocortisol (THF) (20.104 dose) was increased, while the excretion of cortisone (0.06% dose) and tetrahydrocortisone (THE) (1.34% dose) was decreased. The resulting cortisol/cortisone and THF/THE ratios were more than ten times the normal values.
GLC of basal urinary steroids (Table 2) showed decreased values for pregnanediol, pregnanetriol and all individual 1 l-oxo- and 11-desoxo-17-0s which increased on ACTH administration, but remained low compared with normal basal values. The most striking abnormality was the relative increase in basal 1 1 -hydroxy-aetiocholanolone (OHE) as compared with 1 1-oxy-aetiocholanolone (OE). These 1 1-0x0-I 7-0s are mainly derived from cortisol and cortisone, respectively, and to a much lesser degree from 11-OH- androstenedione. Therefore, the high OHE/OE ratio also reflects a predominance of cortisol over cortisone. This abnormality was aggravated by the administration of ACTH and hydrocortisone and persisted during dexamethasone treatment. The E/A ratio was normal implying a normal 5P/a-reduction of the A-ring.
Similar studies were performed for a hypothyroid patient (B), with an even longer plasma t+ of cortisol. GLC-fractionation showed a normal OHE/OE ratio and an increased-E/A ratio, which is characteristic of this condition (Gordon & Southren, 1977).
Table 3. Plasma t i of ''C-cortisol and t i of urinary excretion of I4C-activity for patient A, a hypothyroid patient (B) and a normal female control (26 years)
Patient A Patient B Normal control
Blood ti (min) I09 129 16 Urine (% of dose excreted)
Day 1 76.1 67.1 90.1 Day 2 10.1 15.6 1.9 Day 3 2.1 3.9 ~
Day 4 0.2 1.4 -
tf (days) 0.4 0.5 @2*
* Approximation from observation over 2 days.

512 H . I. J . Harinck et al.
Table 4. Quantification o f urinary “C-cortisol and major cortisol metabolites of dose administered) and excretory ratios of cortisol to cortisone and T H F to THE after paper chromatography (first 24 h) for patient A, patient B and
normal control
Patient A Patient B Normal control
Total urine MeC12 extract Cortisol Cortisone Ethylacetate extract after hydrolysis
T H F THE
Cortisol ‘Cortisone T H F THE
86.4 67-7 4.7 1.4 1.9 0.11 0.06 0.25
20.1 7.7 1.3 5.3
31.5 0.46 15.0 1.4
90.1 3.0 0.59 0.66
12.8 10.9 0.89 1.2
Moreoever free cortisol and i4C-cortisol excretion were normal, which is markedly different from the elevated values found for the patient under study.
DISCUSSION
This young woman exhibits a syndrome of apparent mineralocorticoid excess associated with a deficient peripheral metabolism of cortisol, as first described in two children by Ulick et al. (1977) and further documented in three other children up to now (Werder et al., 1974; Shackleton et al., 1980; Fiselier et al., 1982). Sodium-dependent hypertension and hypokalemic alkalosis with suppressed plasma renin were first documented at the age of 9 months, but mineralocorticoid excess was never demonstrated. In the present study we confirmed a considerably prolonged plasma t i of cortisol, indicating a diminished metabolic clearance rate (MCR) of cortisol.
Two major catabolic reactions are rate-determining for the MCR of cortisol: A-ring reduction (formation of THF and allo-THF) and 1 lp-oxidation. The latter reaction produces cortisone (and subsequently THE), which is metabolized considerably faster than cortisol (Peterson, 1959). The normal excretion of the sum of THF and THE after administration of i4C-cortisol to our patient argues against a defect in A-ring reduction. In fact, the abnormally high urinary ratios ofcortisol to cortisone, T H F to THE and OHE to OE provide strong evidence for diminished 1 Ifl-oxidation. In contrast to the patients described by Ulick et al. (1979) and by Shackleton et al (1980) increased 5a-reduction could not be demonstrated.
Subnormal CSR and a corresponding decrease in urinary excretion of 17-OGS and 17-OS, despite normal plasma levels of cortisol and CBG, are a consequence of the diminished MCR of cortisol and the resultant suppression of the pituitary-adrenal axis. A similar pattern i s known from other conditions with a prolonged t: of cortisol such as hepatic failure and hypothyroidism (Peterson, 1960; Gordon & Southren, 1977). However those conditions present with increased EjA ratios (Bardin & Paulsen, 1981)

Hypertension and dejcient cortisol metabolism 513
and with normal (Peterson, 1960; Brien, 1976) or subnormal cortisol excretion (McCann & Fulton, 1975). The urinary excretion of free cortisol was elevated in our patient. This was also noted by Shackleton et af. (1980) who attributed this finding to the prolonged plasma tt of cortisol. The normal cortisol excretion in our hypothyroid patient (Patient B, table 4) with an even longer tt of cortisol argues against this explanation. As plasma cortisol and CBG and the creatinine clearance were normal in the case under study we propose diminished tubular cortisol reabsorption as the cause of increased cortisol excretion. This latter abnormality might be causally related to diminished renal 1 1P-oxidation of filtered cortisol (Hellman et a/ . , 1971).
The relation between deficient cortisol metabolism and low renin hypertension and hypokalemia has been the subject of many speculations. All patients studied, including our case, showed subnormal production of known mineralocorticoids. The lack of response to spironolactone and dexamethasone in some cases has cast doubt on the involvement of steroids in this syndrome.
In our patient hypokalemia did not respond to spironolactone, whereas amiloride, an inhibitor of tubular ion transport, was effective. This resembles the pattern of drug response observed in ‘Liddle’s syndrome’ (Liddle et al., 1963). However the normal erythrocyte Na permeability, the low salivary Na/K ratio and negative family history of our patient are not compatible with this syndrome (Wang et al., 1981). Moreover normalization of blood pressure and serum K after the combined administration of dexamethasone and aminogluthetimide indicates the involvement of a sodium-retaining kaliuretic steroid, although an extensive search by Ulick et al., (1979), did not reveal overproduction of such a compound.
Excessive sensitivity of mineralocorticoid receptors to steroids could be another mechanism, but this seems unlikely since only minor changes in serum K or blood pressure were seen after the administration of aldosterone to our patient. Recently, New et a/. (1 982) proposed that cortisol itself may have an abnormally high mineralocorticoid activity as a result of an abnormal affinity of cortisol for mineralocorticoid receptors. Diminished degradation of receptor-bound cortisol may explain the relation between defective cortisol metabolism and symptoms of mineralocorticoid excess. Although attractive, this hypothesis cannot explain the lack of response to dexamethasone, unless mineralocorticoid receptor activation is maintained by minute amounts of cortisol. In our opinion the difference in response to dexamethasone alone and to the combined administration of dexamethasone and aminogluthetimide re-emphasizes the partici- pation of an ACTH-independent mineralocorticoid. This study further shows that the 1 ID-oxidation defect of cortisol, resulting in a unique steroid diagram, enables the quick recognition of these patients by chromatographic estimation of C19- and C21-steroid metabolites in a basal 24 h urine sample.
ACKNOWLEDGEMENTS
The authors thank Professor Th. J. Benraad who performed the assays of PRA and mineralocorticoids and Professor Dr H. H. van Gelderen for referring the patient. We also thank the nursing staff and the technical staff of the Clinical Investigation Unit, University Hospital, Leiden and Mrs H. Belier-Lakeman for assistance in preparing the manuscript.

513 H. I. J. Huriiick et ul.
R E F E R E N C E S
BARDIN. C.W. & PAULSEN, C.A. (1981) The Testes. In Te.vrhook qf Endocrinolog). (ed. R.H.J. Williams). pp. 293-354. Saunders, Philadelphia.
BIGLIERI. E.G. (1981) Enzymatic disorders and hypertension. In Etidor,rine Hyperiension (eds. E.G. Biglieri & M . Schambelan). pp. 453463 Clinics in Endocrinology and Metabolism. 10:3. Saunders, Philadelphia.
BRIEN. T.G. ( 1976) The adrenocortical status of patients with thyroid disease. Clinical Endocrinology. 5,97-99. DE MAN. A.J.M., HOFMAN. J.A., RosuorEN. F.M.A.. Ross. H.A. 7 BENRAAD. TH.J. (1980) A direct
radio-immunoassay for plasma a1dosterone:significance of endogenous cortisol. Netherland.? Journal of Medicine, 23, 79-83.
DRAYEK, J.I.M. & BENRAAD. THJ. (1975) The reliability of the measurement of plasma renin activity by radio-immunoassay. Clinica Cltitnicu Acta. 61, 309-324.
FISELIER. T.J.W.. OTTEN. B.J., MONSENS. L.A.H.. HONOUR. J.W. & V A N MUNSTER, P.J.J. (1982) Low-renin, low-aldosterone hypertension and ahnormal cortisol metabolisni in a 19-month-old child. Hormone Reseurch. 16, 107-1 14.
GORDON. G.G. & SouTHnEs. A.L. (1977) Thyroid-hormone effects on steroid-hormone metabolism. Bulletin qf rhc N e w York Academy of Medicine. 53, 241 259.
HELLMAN. L., NAKADA, F.. ZUMOFF, B.. FUKUSHIMA. D., BRADLOW. H.L. & GALLAGHER, T.F. (1971) Renal capture and oxidation of cortisol in man. Journal u/ Clinical €trr!ocritiolog~~ arid Metuholistn, 33, 52-62.
HOEFNAGEI.S, W.H.L.. HOFMAN, J.A.. SMALS, A.G.H.. DRAYER, J.I.M.. KLOPPENBORG. P.W.C. & BENRAAD, TH.J. ( 1 978) Dexamethasone-responsive hypertension in young women with suppressed renin and aldosterone. Lancer. i, 741-743.
LIDDLE, G.W.. BLEDSOSE. T. & COPPACE, W.S. (1963) A familial renal disorder simulating primary aldosteronism, but with negligible aldosterone secretion. Trunsucrions of the Association of Anierican Piiysicans, 76, 199-2 13.
MCCANN. V.J. & FULTON. 1.1. (1975) Cortisol metabolism in chronic liver disease. Journul qf Clinical Endocrinology and Meiuholisrn. 40, 1038-1044.
MEDICAL RESEARCH COUNCIL COMMITTEE ON CLINICAL ENDOCRlNOLOCiY (1963) A standard method of estimating 17-oxosteroids and 1 7-oxogenic steroids. Lancet, i, 1415-1419.
MOOLENAAR, A.J. & V A N SETERS. A.P. (1971) Gaschromatographic determination of steroids in the urine of patients with Cushing’s syndrome. Aria Endorinologicu. 67. 303-3 15.
NEW. M.I., OBERFIELU. S.E.. CAREY. R.. GREIGH. F.. ULICK. S . & LEVINE. L.S. (1982) A genetic defect in cortisol metabolism as the basis for the syndrome of apparent mineralocorticoid excess. In Endocrinologj of Hypertension. Serono Symposion (eds. F. Mantero. E.G. Biglieri & C.R.W. Edwards). SO, 85-101.
NORYMBERSKI. J.K., STUBB, R.D. & WEST. H.J (1953) Assessment of adrenocorticoid activity by assay of 17-ketogenie steroids in urine. Lancer. i. 1276.
PETERSON. R.E. (1959) Metabolism of adrenocorticosteroids in man. Annals of die New York Acadenly of Sciences. 82, 846853.
PETERSON. R.E. (1960) Adrenocortical steroid metabolism and adrenal cortical function in liver disease. Journal of Clinical Investigations. 39, 320-329.
POST. R.L. & JOI.I.Y, P.C. (1957) The linkage of sodium. potassium and ammonium active transport across the erythrocyte membrane. Biochimica er Biopliysica Acta. 25, 1 18-128.
SHACKLETON. C.H.L.. HONOUR. J.W.. DILLON. M .J.. CHANTLER. C. & JONES. R.W.A. ( 1980) Hypertension in a four-year-old child: gab chromatographic and mass spectrometric evidence for deficient hepatic metabolism of steroids. Journal of Clinical EndocrirroloK~. and Merabolisnl. 50, 786792.
ULICK, S.. RAMIREZ. L.C. & NEW, M.1. (1977) An abnormality in steroid reductivemetabolism associated with a hypertensive syndrome. Joirrnal of Clinical Endocrinolog? find Metabolism. 44, 799-802.
ULICK, s.. LEVINC, L.S.. GUNCZKEn. P.. ZANCONATA. G., RAMIREZ. L.C.. RAUH, w . , RBsLEn, A,, BRADLOW, H.C. & N E W , M.1. (1979) A syndrome of apparent mineralocorticoid excess associated with defects in the peripheral metabolism of cortisol. Journal qf Clrnrcal Endocrinologj, and Meraboli.rm, 49, 757-764.
VAN BAELEN, H. & DE MOOR. P. (1974) Immunochemical quantification of human transcortin. Journal ofClinica1 Endocrinology utid Mrtaholi.wi, 39, 16C163.
WAX.C..CHAN,T.K..YEUNG. R.T.T..COC,HLAN, J.P..SCOGGINS, B.A.&STOCKIGT, J.R.(1981)Theeffectof triamterene and sodium intake on renin, aldmterone. and erythrocyte sodium transport in Liddle’s syndrome. Journal of Clinicul Endocrrnologx rind Metubolism, 52, 1027-1032.
WERDER. E.. ZACHMANN. M.. VOLLMIN. J.A.. WEYkwr, R. & PRAUER, A. (1974) Unusual steroid cxcretion in a child with low-renin hypertension. Research in Sreroid.5, 6. 385-389.