An inhibitor of the protein kinases TBK1 and IKK-ε improves obesity-related metabolic dysfunctions...
11
© 2013 Nature America, Inc. All rights reserved. ARTICLES NATURE MEDICINE ADVANCE ONLINE PUBLICATION Although the molecular events underlying the relationship between obesity and insulin resistance remain uncertain 1–4 , numerous studies have implicated an inflammatory link 5–7 . Obesity produces a state of chronic, low-grade inflammation in liver and fat accompanied by the local secretion of cytokines and chemokines that attenuate insu- lin action. Knockout or pharmacological inhibition of inflammatory pathways can disrupt the link between genetic- or diet-induced obes- ity and insulin resistance, suggesting that local inflammation is a key step in the generation of cellular resistance to important hormones that regulate metabolism 7–11 . The nuclear factor-κB (NF-κB) transcriptional program is activated in obese fat and liver and, to a lesser extent, in muscle and seems to have an important role in the development of insulin resistance 12–15 . NF-κB activation is triggered by phosphorylation of the regulatory protein IκB. Four different IκB kinases (IKKs) have been identified: IKK-α, IKK-β, IKK-ε and TBK1. A role for IKK-α and IKK-β in NF-κB activation has been firmly established, but whether TBK1 and IKK-ε regulate the pathway remains uncertain 16–18 . However, the genes encoding both of these kinases contain κB regulatory sites in their promoter regions, and activation of the NF-κB transcrip- tional pathway induces their expression 19 , suggesting that they may act downstream of this transcriptional pathway. We recently reported that expression of both Tbk1 and Ikbke mRNA and TBK1 and IKK-ε protein are increased during a high-fat diet (HFD) in adipose tissue, and the expression of IKK-ε is increased in liver 15 . Moreover, deletion of the Ikbke gene rendered mice partially resistant to the HFD-dependent development of obesity, insulin resistance, hepatic steatosis and inflammation, leading us to search for small- molecule inhibitors of these kinases as a potential therapeutic option to treat these conditions. We report here the identification of one such compound, amlexanox, which had been previously developed for the treatment of asthma, allergic rhinitis and aphthous ulcers but has an unclear mechanism of action 20,21 . Administration of this selec- tive TBK1 and IKK-ε inhibitor to obese mice produces reversible weight loss and improved insulin sensitivity, reduced inflammation and attenuated hepatic steatosis without affecting food intake. These data suggest that IKK-ε and TBK1 are part of a counterinflammatory process that sustains energy storage in the context of insulin resist- ance 22 . Disruption of this process by amlexanox thus increases adap- tive energy expenditure and restores insulin sensitivity. Because of the apparent safety of this drug in patients, we propose that it undergo study for the treatment of obesity, type 2 diabetes and nonalcoholic fatty liver disease in patients. RESULTS Obesity increases IKK-« and TBK1 activity through NF-kB In a previous study 15 we reported that the mRNA levels of both Ikbke and Tbk1 are elevated in white adipose tissue (WAT) from 1 Life Sciences Institute, University of Michigan, Ann Arbor, Michigan, USA. 2 Department of Internal Medicine, University of Michigan, Ann Arbor, Michigan, USA. 3 Department of Molecular and Integrative Physiology, University of Michigan, Ann Arbor, Michigan, USA. 4 Gene Expression Laboratory, Salk Institute for Biological Sciences, La Jolla, California, USA. 5 Storr Liver Unit, Westmead Millennium Institute and University of Sydney, Westmead Hospital, Westmead, New South Wales, Australia. 6 Howard Hughes Medical Institute, Salk Institute for Biological Sciences, La Jolla, California, USA. 7 Department of Medicine, University of California San Diego, San Diego, California, USA. 8 Present addresses: Muscle Metabolism Discovery Performance Unit, GlaxoSmithKline, Research Triangle Park, North Carolina, USA (S.-H.C.), Institute of Endocrinology, Diabetes and Metabolism, Rambam Health Care Campus, Haifa, Israel (N.M.W.) and Medical Oncology Division, Washington University School of Medicine, Saint Louis, Missouri, USA (I.H.). 9 These authors contributed equally to this work. Correspondence should be addressed to A.R.S. ([email protected]). Received 12 January 2012; accepted 26 December 2012; published online 10 February 2013; doi:10.1038/nm.3082 An inhibitor of the protein kinases TBK1 and IKK-ε improves obesity-related metabolic dysfunctions in mice Shannon M Reilly 1,9 , Shian-Huey Chiang 1,8,9 , Stuart J Decker 1 , Louise Chang 1 , Maeran Uhm 1–3 , Martha J Larsen 1 , John R Rubin 1 , Jonathan Mowers 1–3 , Nicole M White 1,8 , Irit Hochberg 1,8 , Michael Downes 4 , Ruth T Yu 4 , Christopher Liddle 4,5 , Ronald M Evans 4,6 , Dayoung Oh 7 , Pingping Li 7 , Jerrold M Olefsky 7 & Alan R Saltiel 1–3 Emerging evidence suggests that inflammation provides a link between obesity and insulin resistance. The noncanonical I kB kinases IKK-« and TANK-binding kinase 1 (TBK1) are induced in liver and fat by NF-kB activation upon high-fat diet feeding and in turn initiate a program of counterinflammation that preserves energy storage. Here we report that amlexanox, an approved small-molecule therapeutic presently used in the clinic to treat aphthous ulcers and asthma, is an inhibitor of these kinases. Treatment of obese mice with amlexanox elevates energy expenditure through increased thermogenesis, producing weight loss, improved insulin sensitivity and decreased steatosis. Because of its record of safety in patients, amlexanox may be an interesting candidate for clinical evaluation in the treatment of obesity and related disorders.
-
Upload
terrysaurus -
Category
Documents
-
view
54 -
download
2
description
Old drug may point the way to new treatments for diabetes and obesityANN ARBOR—Researchers at the University of Michigan's Life Sciences Institute have found that amlexanox, an off-patent drug currently prescribed for the treatment of asthma and other uses, also reverses obesity, diabetes and fatty liver in mice.The findings from the lab of Alan Saltiel, the Mary Sue Coleman director of the Life Sciences Institute, are scheduled to be published online Feb. 10 in the journal Nature Medicine."One of the reasons that diets are so ineffective in producing weight loss for some people is that their bodies adjust to the reduced calories by also reducing their metabolism, so that they are 'defending' their body weight," Saltiel said. "Amlexanox seems to tweak the metabolic response to excessive calorie storage in mice."Different formulations of amlexanox are currently prescribed to treat asthma in Japan and canker sores in the United States. Saltiel is teaming up with clinical-trial specialists at U-M to test whether amlexanox will be useful for treating obesity and diabetes in humans. He is also working with medicinal chemists at U-M to develop a new compound based on the drug that optimizes its formula.The study appears to confirm and extend the notion that the genes IKKE and TBK1 play a crucial role for maintaining metabolic balance, a discovery published by the Saltiel lab in 2009 in the journal Cell."Amlexanox appears to work in mice by inhibiting two genes—IKKE and TBK1—that we think together act as a sort of brake on metabolism," Saltiel said. "By releasing the brake, amlexanox seems to free the metabolic system to burn more, and possibly store less, energy."Using high-throughput chemical screening at LSI's Center for Chemical Genomics to search for compounds that inhibit IKKE and TBK1, the researchers hit upon an approved off-patent drug: amlexanox. They then demonstrated that amlexanox had profound beneficial effects in both genetic and dietary-induced obese mice. The chemical lowered the weight of obese mice and reversed related metabolic problems such as diabetes and fatty liver."These studies tell us that, at least in mice, the IKKE/TBK1 pathway plays an important role in defending body weight by increasing storage and decreasing burning of calories, and that by inhibiting that pathway with a compound, we can increase metabolism and induce weight loss, reverse diabetes and reduce fatty liver," Saltiel said.The drug has been on the market in Japan for more than 25 years.However, the researchers don't yet know if humans respond with the same pathway, or if the discovery of amlexanox's effectiveness in mice can lead to a compound that is safe and effective for treating obesity and diabetes in humans."We will be working hard on that," Saltiel said.Saltiel's search for a drug targeting the IKKE/TBK1 pathway was supported by the Life Science Institute's Innovation Partnership, which provides philanthropic funding and business mentorship to help move promising research toward commercialization.The research was also supported by the National Institutes of Health, the Michigan Diabetes Research and Training Center, the Michigan Institute for Clinical and Health Research, and the Nathan Shock Center in the Basic Biology of Aging.Additional authors were Shannon M. Reilly, Shian-Huey Chiang, Stuart J. Decker, Louise Chang, Martha J. Larsen, John R. Rubin, Nicole M. White and Irit Hochberg from the Life Sciences Institute; Maeran Uhm and Jonathan Mowers from the Life Sciences Institute and Departments of Internal Medicine and Molecular and Integrative Physiology at the University of Michigan; Michael Downes, Ruth Yu and Ronald M. Evans from the Salk Institute for Biological Sciences; Christopher Liddle from the Storr Liver Unit, Westmead Millennium Institute and University of Sydney, Australia; and Dayoung Oh, Pingping Li, and Jerrold M. Olefsky from the Department of Medicine, Un
Transcript of An inhibitor of the protein kinases TBK1 and IKK-ε improves obesity-related metabolic dysfunctions...

©20
13 N
atu
re A
mer
ica,
Inc.
All
rig
hts
res
erve
d.
a r t i c l e s
nature medicine advance online publication �
Although the molecular events underlying the relationship between obesity and insulin resistance remain uncertain1–4, numerous studies have implicated an inflammatory link5–7. Obesity produces a state of chronic, low-grade inflammation in liver and fat accompanied by the local secretion of cytokines and chemokines that attenuate insu-lin action. Knockout or pharmacological inhibition of inflammatory pathways can disrupt the link between genetic- or diet-induced obes-ity and insulin resistance, suggesting that local inflammation is a key step in the generation of cellular resistance to important hormones that regulate metabolism7–11.
The nuclear factor-κB (NF-κB) transcriptional program is activated in obese fat and liver and, to a lesser extent, in muscle and seems to have an important role in the development of insulin resistance12–15. NF-κB activation is triggered by phosphorylation of the regulatory protein IκB. Four different IκB kinases (IKKs) have been identified: IKK-α, IKK-β, IKK-ε and TBK1. A role for IKK-α and IKK-β in NF-κB activation has been firmly established, but whether TBK1 and IKK-ε regulate the pathway remains uncertain16–18. However, the genes encoding both of these kinases contain κB regulatory sites in their promoter regions, and activation of the NF-κB transcrip-tional pathway induces their expression19, suggesting that they may act downstream of this transcriptional pathway.
We recently reported that expression of both Tbk1 and Ikbke mRNA and TBK1 and IKK-ε protein are increased during a high-fat diet (HFD)
in adipose tissue, and the expression of IKK-ε is increased in liver15. Moreover, deletion of the Ikbke gene rendered mice partially resistant to the HFD-dependent development of obesity, insulin resistance, hepatic steatosis and inflammation, leading us to search for small-molecule inhibitors of these kinases as a potential therapeutic option to treat these conditions. We report here the identification of one such compound, amlexanox, which had been previously developed for the treatment of asthma, allergic rhinitis and aphthous ulcers but has an unclear mechanism of action20,21. Administration of this selec-tive TBK1 and IKK-ε inhibitor to obese mice produces reversible weight loss and improved insulin sensitivity, reduced inflammation and attenuated hepatic steatosis without affecting food intake. These data suggest that IKK-ε and TBK1 are part of a counterinflammatory process that sustains energy storage in the context of insulin resist-ance22. Disruption of this process by amlexanox thus increases adap-tive energy expenditure and restores insulin sensitivity. Because of the apparent safety of this drug in patients, we propose that it undergo study for the treatment of obesity, type 2 diabetes and nonalcoholic fatty liver disease in patients.
RESULTSObesity increases IKK-« and TBK1 activity through NF-kBIn a previous study15 we reported that the mRNA levels of both Ikbke and Tbk1 are elevated in white adipose tissue (WAT) from
1Life Sciences Institute, University of Michigan, Ann Arbor, Michigan, USA. 2Department of Internal Medicine, University of Michigan, Ann Arbor, Michigan, USA. 3Department of Molecular and Integrative Physiology, University of Michigan, Ann Arbor, Michigan, USA. 4Gene Expression Laboratory, Salk Institute for Biological Sciences, La Jolla, California, USA. 5Storr Liver Unit, Westmead Millennium Institute and University of Sydney, Westmead Hospital, Westmead, New South Wales, Australia. 6Howard Hughes Medical Institute, Salk Institute for Biological Sciences, La Jolla, California, USA. 7Department of Medicine, University of California San Diego, San Diego, California, USA. 8Present addresses: Muscle Metabolism Discovery Performance Unit, GlaxoSmithKline, Research Triangle Park, North Carolina, USA (S.-H.C.), Institute of Endocrinology, Diabetes and Metabolism, Rambam Health Care Campus, Haifa, Israel (N.M.W.) and Medical Oncology Division, Washington University School of Medicine, Saint Louis, Missouri, USA (I.H.). 9These authors contributed equally to this work. Correspondence should be addressed to A.R.S. ([email protected]).
Received 12 January 2012; accepted 26 December 2012; published online 10 February 2013; doi:10.1038/nm.3082
An inhibitor of the protein kinases TBK1 and IKK-ε improves obesity-related metabolic dysfunctions in miceShannon M Reilly1,9, Shian-Huey Chiang1,8,9, Stuart J Decker1, Louise Chang1, Maeran Uhm1–3, Martha J Larsen1, John R Rubin1, Jonathan Mowers1–3, Nicole M White1,8, Irit Hochberg1,8, Michael Downes4, Ruth T Yu4, Christopher Liddle4,5, Ronald M Evans4,6, Dayoung Oh7, Pingping Li7, Jerrold M Olefsky7 & Alan R Saltiel1–3
Emerging evidence suggests that inflammation provides a link between obesity and insulin resistance. The noncanonical IkB kinases IKK-« and TANK-binding kinase 1 (TBK1) are induced in liver and fat by NF-kB activation upon high-fat diet feeding and in turn initiate a program of counterinflammation that preserves energy storage. Here we report that amlexanox, an approved small-molecule therapeutic presently used in the clinic to treat aphthous ulcers and asthma, is an inhibitor of these kinases. Treatment of obese mice with amlexanox elevates energy expenditure through increased thermogenesis, producing weight loss, improved insulin sensitivity and decreased steatosis. Because of its record of safety in patients, amlexanox may be an interesting candidate for clinical evaluation in the treatment of obesity and related disorders.

©20
13 N
atu
re A
mer
ica,
Inc.
All
rig
hts
res
erve
d.
a r t i c l e s
� advance online publication nature medicine
HFD-fed mice as compared to normal-chow diet (NCD) controls, whereas Ikbke mRNA is elevated in liver. Immune complex assays revealed that both IKK-ε and TBK1 kinase activity were elevated in livers from HFD-fed mice (Fig. 1a). In the adipose tissue, we also found higher kinase activity, even when normalized to the elevated protein expression. We found this elevated expression after 6–7 weeks of HFD feeding, directly correlating with the onset of inflammatory macrophage infiltration in adipose tissue and liver (data not shown).
We modeled inflammation in 3T3-L1 cells by treating differentiated adipocytes with the inflammatory cytokine tumor necrosis factor α (TNF-α)23. Chronic TNF-α treatment increased the mRNA levels of both kinases (Fig. 1b). These effects were prevented by pretreatment of cells with the IKK-β inhibitor compound VIII24. Furthermore, TNF-α produced a dose-dependent increase in IKK-ε protein expres-sion in these cells, as well as downregulation of peroxisome prolifera-tor activated receptor-γ (PPAR-γ). TNF-α also produced increased phosphorylation of TBK1 at Ser172, which is associated with activa-tion (Fig. 1c).
To investigate whether inflammatory signals are responsible for the induction of these kinases in vivo, we treated HFD-fed mice with the PPAR-γ agonist rosiglitazone or the ω-3 fatty acid GPR120 agonists eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA). Both rosiglitazone and ω-3 fatty acids reduce the inflammation and insulin resistance associated with obesity25. Diet supplemented with ω-3 fatty acids markedly attenuated the HFD-induced elevation in the expres-sion of IKK-ε mRNA and protein expression in both WAT and liver (Fig. 1d,e). Treatment of obese mice with rosiglitazone also reduced expression of Ikbke in adipocytes as well as in the stromal vascular fraction of WAT (Fig. 1f). Because neither rosiglitazone nor ω-3 fatty acid diet supplementation caused weight loss25, the elevated expres-sion of these kinases from high-fat feeding is probably the result of inflammation rather than a direct result of obesity.
Amlexanox is an inhibitor of IKK-« and TBK1Because deletion of the Ikbke gene in mice produced partial resistance to the effects of a HFD15, we screened a library of 150,000 chemi-cal compounds to search for inhibitors of IKK-ε using recombinant
baculoviral-expressed, purified full-length IKK-ε with myelin basic protein (MBP) as a substrate and identified amlexanox as a high-affinity inhibitor (Fig. 2a). This previously discovered drug of unknown mechanism is used to treat asthma and allergic rhinitis in Japan and aphthous ulcers in the United States20,21.
Dose-response experiments revealed that amlexanox blocked IKK-ε activity with a half-maximal inhibitory concentration (IC50) of approximately 1–2 µM (Fig. 2b). Amlexanox also blocked the activ-ity of TBK1 at approximately the same concentrations but had no effect on IKK-α or IKK-β and at these concentrations did not block any other kinases from a broad panel representing most kinase fami-lies. TBK1 and IKK-ε share an overall 65% sequence similarity and are 72% identical in the ATP-binding region. Inhibition of IKK-ε or TBK1 (data not shown) by amlexanox was competitive for its substrate ATP (Fig. 2c), indicating that it interacts with the enzymes in the ATP-binding site. This is consistent with a model of the compound docked in the presumed ATP-binding pocket of TBK1 (Fig. 2d) on the basis of its published structure26.
Amlexanox increased the phosphorylation of TBK1 at Ser172 in 3T3-L1 adipocytes and blocked polyinosinic:polycytidylic acid (poly I:C)-stimulated phosphorylation of interferon responsive factor-3 (IRF3), a presumed substrate of IKK-ε and TBK1 (ref. 27 and Fig. 2e). Reduced IRF3 phosphorylation was also produced by the previously identified IKK-ε and TBK1 inhibitor Cay10576 (cayman)28. Furthermore, cayman treatment of RAW264.7 macro-phages stimulated with lipopolysaccharide (LPS) or poly I:C also blocked the phosphorylation of IRF3 and stimulated the phosphory-lation of TBK1 at Ser172 (Fig. 2f). The phosphorylation of TBK1 was also increased in peritoneal macrophages derived from Ikbke knock-out mice (data not shown), which was probably caused by blockade of feedback inhibition of the pathway29, as evidenced by higher IKK-β phosphorylation in cayman-treated RAW264.7 cells.
Amlexanox produces reversible weight loss in obese miceWe fed C57BL/6 mice a diet of 45% fat and gavaged them daily with a vehicle control or with 25 or 100 mg per kg body weight amlexanox and monitored their body weight (Fig. 3a). Serum concentrations of the drug exceed 5 µM at these doses30. Treatment of mice with
cTNF-α(ng ml–1)
0 1 10 100
pTBK1
TBK1
IKK-ε
PPAR-γ
Akt0
1
2
3
4
Liver WAT
*
#
IKK
-ε a
ctiv
ity (
AU
)
0
1
2
3
Liver WAT
TB
K1
activ
ity (
AU
)
a
*
*
NCD HFD
0
1
2
3
4
5
Ikbke Tbk1Rel
ativ
e ge
ne e
xpre
ssio
n
No treatment TNF-α TNF-α + compound VIII Compound VIII
b
*
†
*†
0
1
2
3
4
5
Liver WAT
Rel
ativ
e ge
ne e
xpre
ssio
n
NCDHFD HFD + ω-3 FA
d
†
*
†
* f
00.050.100.150.200.25
SVF Adipocytes
Rel
ativ
e ge
neex
pres
sion
HFD HFD + rosiglitazone
* *
e ω-3 FA
pTBK1
TBK1
IKK-ε
RalA
Figure 1 Induction of IKK-ε and TBK1 in obese mice is a result of increased inflammation. (a) TBK1 and IKK-ε activity in the liver and WAT of NCD-fed or HFD-fed mice. n = 4 per group. *P < 0.05 for NCD compared to HFD, #P < 0.1 for NCD compared to HFD (Student’s t test). AU, arbitrary units. (b) Expression of Ikbke and Tbk1 in differentiated 3T3-L1 cells without treatment or treated with TNF-α, compound VIII or both TNF-α and compound VIII. Results are representative of multiple experiments. *P < 0.05 for no treatment compared to treatment with TNF-α only, †P < 0.05 for treatment with TNF-α compared to TNF-α plus compound VIII (analysis of variance (ANOVA) with Tukey-Kramer post hoc analysis). (c) IKK-ε, TBK1 and PPAR-γ protein expression and TBK1 phosphorylation at Ser172 (pTBK1) after TNF-α treatment. Results were replicated in more than three experiments. Akt was used as a loading control. (d) Ikbke expression in liver and WAT of NCD-fed or HFD-fed mice with or without ω-3 fatty acids (FA). †P < 0.05 for NCD compared to HFD, *P < 0.05 for HFD compared to HFD plus ω-3 FA. n = 9 per group (ANOVA with Tukey-Kramer post hoc analysis). (e) IKK-ε protein expression and TBK1 phosphorylation at Ser172 in HFD-fed mice with and without ω-3 FA. RalA was used as a loading control. (f) Ikbke expression in adipocytes and stromal vascular fraction (SVF) of mice fed HFD or HFD plus rosiglitazone. *P < 0.05 for HFD compared to HFD plus rosiglitazone (Student’s t test). n = 8 in the HFD group, n = 4 in the HFD plus rosiglitazone group. All data in the figure are shown as the mean ± s.e.m.

©20
13 N
atu
re A
mer
ica,
Inc.
All
rig
hts
res
erve
d.
a r t i c l e s
nature medicine advance online publication �
either dose of amlexanox prevented the weight gain produced by a HFD; drug-treated mice maintained weights equivalent to those of vehicle-treated mice on a control diet through 12 weeks. There was no effect of the drug on food intake, either at the beginning or end of the study (Fig. 3b).
We also evaluated amlexanox in mice with established obesity (Fig. 3c and Supplementary Fig. 1). Treatment with amlexanox pro-duced a 10-g weight loss in HFD-fed obese mice after only 4 weeks of treatment with no further effect thereafter. Moreover, escalation of the dose at this time point had no further effect on weight (data not shown). Withdrawal of the drug after 8 weeks of treatment restored weight gain, and the mice returned to their original weights after 6–8 weeks (Fig. 3c). Weight loss during the treatment phase was accompanied by more than a 6-g reduction in overall mass of adi-pose tissue, as well as an 80% decrease in fasting leptin concentration, whereas the concentrations of serum triglycerides, free fatty acids and cholesterol were unchanged (Fig. 3d and data not shown).
To determine whether the effects of amlexanox could be seen in another model of obesity, we treated ob/ob mice31,32 with 100 mg per kg body weight of amlexanox or vehicle control and monitored their body weight (Fig. 3e). Although the drug had no effect on food intake, amlexanox produced a 7- to 8-g weight loss after 4 weeks of treatment. Amlexanox also caused a significant decrease in adipose tissue mass in these mice and an increase in circulating adiponectin concentrations (Fig. 3f,g).
Because amlexanox had no effect on food intake, we reasoned that the weight loss was the result of increased energy expenditure. We thus used metabolic cages to monitor energy expenditure in diet-induced
obese (DIO) mice treated with or without amlexanox. Four-week treatment of DIO mice with 25 mg per kg body weight amlexanox resulted in significantly (P < 0.001) higher oxygen consumption as compared to treatment with vehicle control, which is consistent with an increase in energy expenditure (Fig. 3h). Exhaled carbon dioxide was also significantly (P = 0.001) higher in the amlexanox-treated mice, and their respiratory exchange ratio remained unchanged compared to control-treated mice (Supplementary Fig. 2), although amlexanox had no effect on NCD-fed mice, in which neither IKK-ε nor TBK1 was induced. Together, these data suggest that amlexanox might induce an increase in thermogenesis in obese mice. Amlexanox treatment produced an approximate 1 °C increase in body temp-erature compared to HFD-fed vehicle-treated mice, restoring the temperatures to those of NCD-fed mice (Fig. 3i).
Amlexanox improves insulin sensitivity in obese miceTo assess in more detail the metabolic impact of amlexanox treatment, we treated DIO mice with 25 mg per kg body weight amlexanox or vehicle control for 8 weeks either before or after obesity was estab-lished and then assessed their metabolic parameters. Mice treated with amlexanox concurrently with a HFD had improved glucose tol-erance after obesity was established, with an approximate 30–40% reduction in the area under the curve for glucose (Fig. 4a). Treatment of mice with amlexanox after established DIO reversed the elevations in fasting serum insulin concentrations caused by the HFD, suggest-ing improved insulin sensitivity (Fig. 4b). Insulin tolerance tests revealed that amlexanox treatment significantly improved insulin sensitivity in mice with established DIO, as indicated by a restoration
0
0.4
0.6
0.8
1.0
1.2
1.4
–0.2 –0.1 0 0.1 0.2 0.3 0.4
Act
ivity
–1 (
pMB
P–1
)
ATP–1 (µM–1)
VehicleAmlexanox (1 µM) Amlexanox (3 µM) Amlexanox (10 µM)
a e
d
b
c
IKK-ε
TBK1
[32P
]-M
BP
f
pTBK1
TBK1
pIRF3
IRF3
pIKK-β
IKK-β3.23
3.08
2.88
LPS Poly I:C
IKK-ε
RalA
IKK-βpTBK1
TBK1
pIRF3
IRF3
IKK-ε
RalA
Poly I:C
Amlexanox (µM)
Amlexanox (µM)O
O
O
OH
N NH2
Cayman (µM)
Cayman (µM) 1020 1020 1020
– – –
– 0.5 1.0 2.5 5.0 12.5 25 50
– – – – ––– – – – – – –
121 2 4 1 2 4
25 50 12 25 50
Thr156
Lys38
0.2
0
Figure 2 Amlexanox is a specific inhibitor of IKK-ε and TBK1. (a) Diagram of the chemical structure of amlexanox. (b) Dose-response relationship of amlexanox inhibition of IKK-ε and TBK1 activity as determined by MBP phosphorylation showing an IC50 of approximately 1–2 µM. Results were replicated in more than three experiments. (c) Lineweaver-Burk plot showing competition of amlexanox with ATP for inhibition of IKK-ε. Results are representative of three experiments. (d) Model of amlexanox binding to the ATP-binding site of TBK1. Top, surface model showing the binding of amlexanox in the active site of TBK1; bottom, hydrogen bonding of amlexanox (cyan) in the active site of TBK1. (e) TBK1 phosphorylation (pTBK1) at Ser172 and IRF3 phosphorylation at Ser396 (pIRF3) in 3T3-L1 adipocytes treated with amlexanox or cayman and with or without poly I:C. Results were replicated in more than three experiments. RalA was used as a loading control. (f) IRF3, IKK-β (pIKK-β) and TBK1 phosphorylation in RAW264.7 cells treated with or without cayman, LPS and poly I:C. Results were replicated in multiple experiments. RalA was used as a loading control.

©20
13 N
atu
re A
mer
ica,
Inc.
All
rig
hts
res
erve
d.
a r t i c l e s
� advance online publication nature medicine
in insulin responsiveness to the levels of NCD-fed mice (Fig. 4c and Supplementary Fig. 3a). Amlexanox did not affect insulin sensitivity in NCD-fed mice. After 4 weeks of treatment, amlexanox produced marked improvements in glucose tolerance (Fig. 4d) and insulin sen-sitivity (Fig. 4e and Supplementary Fig. 3b) in ob/ob mice.
We used hyperinsulinemic-euglycemic clamp studies to investi-gate the tissue-specific effects of amlexanox on insulin sensitivity. Consistent with improved overall insulin sensitivity, the glucose infu-sion rate was significantly higher in amlexanox-treated mice than in vehicle-treated mice (Fig. 4f and Supplementary Fig. 3c). Insulin-mediated suppression of hepatic glucose production was substantially enhanced by amlexanox treatment (Fig. 4g). However, we found no change in glucose turnover rate (Fig. 4h). Amlexanox treatment had no effect on glucose handling in NCD-fed mice (Supplementary Fig. 3d–g). These results indicate that the liver is an important target of amlexanox in mediating improved insulin sensitivity. Furthermore, these results support the action of amlexanox through IKK-ε and
TBK1, both of which are induced in the liver by HFD. Amlexanox-treated mice showed enhanced insulin-mediated suppression of serum free fatty acids, which is indicative of increased suppression of adipose tissue lipolysis (Fig. 4i). Moreover, although the basal phos-phorylation of hormone-sensitive lipase (HSL) was higher in adipose tissue from amlexanox-treated mice than vehicle-treated mice, the dephosphorylation of HSL produced by insulin was enhanced after amlexanox treatment compared to vehicle-treated mice on HFD (Supplementary Fig. 3h). Phosphorylation of Akt in response to insulin was also enhanced in amlexanox-treated mice compared to vehicle-treated controls, indicating improved insulin sensitivity in WAT (Supplementary Fig. 3i).
Amlexanox reverses hepatic steatosis in obese miceWe treated DIO mice with 25 mg per kg body weight amlexanox or vehicle control for 8 weeks and examined their livers postmortem (Fig. 5a). The hepatomegaly normally observed in HFD-fed mice
h
2000
2500
3000
3500
4000
4500
6 p.m. 6 a.m. 6 p.m. 6 a.m. 6 p.m. 6 a.m.
VO
2 (m
l kg–1
h–1
)
NCD vehicle NCD amlexanox(25 mg per kg)
30
32
34
36
38
HFD amlexanox(25 mg per kg)
HFD vehicleNCD vehicle
Cor
e te
mpe
ratu
re (
°C)
i
2000
2500
3000
3500
4000
4500
6 p.m. 6 a.m. 6 p.m. 6 a.m. 6 p.m. 6 a.m.
VO
2 (m
l kg–1
h–1
)HFD vehicle HFD amlexanox
(25 mg per kg)
0
20
40
60
80
Fat Lean Fluid
Percentage body w
eight0
10
20
30
40
50
Body Fat Lean Fluid
Wei
ght (
g)
d
†
*
†*
† *
†*
† *
† *
NCD vehicle HFD vehicleHFD amlexanox (25 mg per kg)NCD amlexanox (25 mg per kg)
0
10
20
30
40
Bod
y fa
t (g)
Amlexanox(100 mg per kg)
Vehicle
f*
0
10
20
30
40
Adi
pone
ctin
(µg
ml–1
)
g
*
Amlexanox(100 mg per kg)
Vehicle30354045505560
0 2 4 6 8 10 12B
ody
wei
ght (
g)Duration of daily gavage (weeks)
Vehicle
Amlexanox (100 mg per kg)
e
HFD amlexanox (25 mg per kg)HFD vehicle
b
Foo
d in
take
(m
g pe
r g)
0
50
100
150
200
NCD vehicle
30
35
40
45
50
55
0 2 4 6 8 10 12 14 16
Bod
y w
eigh
t (g)
Duration of daily gavage (weeks)
HFD vehicle
HFD withdrawal
HFD amlexanox
cHFD amlexanox(100 mg per kg)
HFD vehicle
0
20
40
60
80
100
Foo
d in
take
(m
g pe
r g)
a
20
25
30
35
40
45
50
55
0 5 10 15 20 25
Bod
y w
eigh
t (g)
Duration of daily gavage (weeks)
NCD vehicle
HFD vehicle
HFD amlexanox(25 mg per kg) HFD amlexanox(100 mg per kg)
Figure 3 Daily amlexanox gavage both prevents and reverses diet- induced or genetic obesity. (a) Body weight of mice treated preventatively with 25 mg per kg body weight amlexanox, 100 mg per kg amlexanox or vehicle control. n = 5 per group. (b) Food intake after 1 week of treatment (left) or 6 weeks of preventative gavage (right) with vehicle in NCD-fed mice and HFD-mice or with amlexanox in HFD-fed mice. n = 7 per group. (c) Body weight of mice treated with amlexanox or vehicle control and mice in which treatment was withdrawn after eight weeks. n = 7 per group. (d) Total (left) and relative (right) fat and lean body mass of mice in each treatment group. n = 4 for the NCD groups, n = 8 for the HFD groups. (e) Body weight of ob/ob mice gavaged with amlexanox or vehicle control. n = 8 per group. (f) Total body fat mass of ob/ob mice gavaged with amlexanox or vehicle control. n = 6 per group. (g) Serum adiponectin concentrations in ob/ob mice gavaged with amlexanox or vehicle control. n = 8 per group. (h) Oxygen consumption (VO2) of mice in each treatment group. n = 4 for the NCD groups, n = 8 for the HFD groups. The HFD-fed amlexanox-treated mean values were significantly higher than the HFD-fed vehicle-treated mean values during all three light and dark cycles; P < 0.05 (Student’s t test). (i) Core body temperature in NCD-fed mice gavaged with vehicle or amlexanox and in HFD-fed mice gavaged with vehicle or amlexanox. *P < 0.05 for HFD-fed vehicle-treated controls compared to HFD-fed amlexanox-treated mice, †P < 0.05 for NCD-fed vehicle-treated controls compared to HFD-fed vehicle-treated controls (ANOVA with Tukey-Kramer post hoc analysis). *P < 0.05 for ob/ob vehicle-treated controls compared to ob/ob amlexanox-treated mice (Student’s t test). All data in the figure are shown as the mean ± s.e.m. or as a dot plot showing each data point and the mean.

©20
13 N
atu
re A
mer
ica,
Inc.
All
rig
hts
res
erve
d.
a r t i c l e s
nature medicine advance online publication �
was largely reversed by the drug, with a greater than 20% reduction in liver weight (Fig. 5b). Moreover, triglyceride content in the liver was more than 50% lower in the amlexanox-treated mice compared to mice treated with vehicle control. Hepatic glycogen content, which is elevated in HFD-fed mice, was reduced by amlexanox (Fig. 5c). Large lipid droplets were apparent by H&E staining in the livers from vehicle- treated control DIO mice but were largely disseminated by treatment with amlexanox, which is consistent with the marked reductions in triglycerides, glycogen and liver weight (Fig. 5d). These benefi-cial reductions in hepatic lipids were reversed in livers from mice that were taken off amlexanox treatment and continued on a HFD (Fig. 5e). Steatosis was also resolved in ob/ob mice treated with the drug (Supplementary Fig. 4a–c).
To further investigate the hepatosteatotic phenotype, we measured the expression of key metabolic and inflammatory genes in the livers of NCD-fed, HFD-fed and amlexanox-treated HFD-fed (control) mice. Mice treated with amlexanox had lower expression of certain key lipogenic genes compared to control mice, including those encod-ing fatty acid synthase (Fasn), malic enzyme 1 (Me1), acetyl CoA carboxylase (Acaca) and stearyl CoA desaturase 1 (Scd1) (Fig. 5f). Indicative of a higher lipid load, HFD was associated with higher expression of Ppara, Pparg, Cd36, Fabp4 (encoding fatty acid bind-ing protein 4) and Lpl (encoding lipoprotein lipase). The expression of these genes was lower in amlexanox-treated and NCD-fed mice. Gluconeogenic gene expression was modestly higher in HFD-fed mice and was not lower with amlexanox treatment. Glycolytic genes, the expression levels of which were higher in HFD-fed mice relative to
NCD-fed mice, were expressed at lower levels in amlexanox-treated mice (Fig. 5g). In addition, we found lower levels of HFD-induced expression of several inflammatory genes, including Tnfa, Cxcl10 and Ccl5 (also known as Rantes), which encode proinflammatory cytokines (Fig. 5h), Ccl2 (also known as Mcp1) and Ccl3 (also known as Mip-1α), which encode chemotactic factors, and Emr1 and Itgax (also known as F4/80 and Cd11c), which encode markers of macrophage infiltration. Expression of Cybb, encoding cytochrome b-245, β-polypeptide, which is involved in the microbicidal oxidase system of phagocytes, was lower in the drug-treated group. Genetic measures of hepatosteatosis were similarly lower in ob/ob mice (Supplementary Fig. 4d,e).
Amlexanox reduces adipose tissue inflammation in obese miceInfiltration of inflammatory macrophages into WAT was markedly lower in amlexanox-treated mice compared to vehicle-treated controls, as assessed by H&E staining (Fig. 6a). This amlexanox- dependent reduction in the appearance of macrophages in crown-like structures33 was accompanied by a marked attenuation in the levels of mRNAs encoding key inflammatory genes in adipose tissue, including Tnfa, Ccl2, Ccl3, Itgax and Emr1 (Fig. 6b). We also mea-sured the concentration of cytokines in the serum of control and amlexanox-treated mice. Although the drug had no effect on the circu-lating concentrations of Mcp1 or Rantes, the concentrations of TNF-α, IL-1α and Mip-1α were lower (Fig. 6c). Serum concentrations of the anti-inflammatory cytokine IL-10 (ref. 34) were higher in amlexanox-treated mice compared to controls. We found higher expression of fat
0
50
100
150
0 30 60 90 120 150 180
Per
cent
age
of b
asal
blo
od g
luco
se
Minutes after insulin injection
Vehicle
Amlexanox (100 mg per kg)e
** * * * *
0
100
200
300
400
500
0 30 60 90 120
Blo
od g
luco
se (
mg
dl–1
)
Minutes after glucose gavage
NCD vehicle HFD amlexanox(25 mg per kg)
a
* * *
† †
†† †
†
#
# #
HFD vehicle
0
100
200
300
400
500
600
0 20 40 60 80 100 120
Blo
od g
luco
se (
mg
dl–1
)
Minutes after glucose gavage
d
**
* *
Vehicle Amlexanox (100 mg per kg)
0
20
40
60
80
100
120
0 30 60 90 120
Per
cent
age
of b
asal
blo
od g
luco
se
Minutes after insulin injection
NCD vehicle NCD amlexanox (25 mg per kg) HFD vehicle HFD amlexanox (25 mg per kg)
c
** *
Fas
ting
bloo
d gl
ucos
e (m
g dl
–1)
Fas
ting
insu
lin (
ng m
l–1)
b
†
0
2
4
6
8
10
*
80
100
120
140
160
180
200
HFD amlexanox(25 mg per kg)HFD vehicle
NCD vehicle
f
0
1,000
2,000
3,000
4,000
AU
C G
IG0–
120
min
(m
g pe
r kg
)
Vehicle
Amlexanox(50 mg per kg)
*
0
1
2
3
4
Fol
d su
ppre
ssio
nof
ser
um F
FA
i Vehicle
Amlexanox(50 mg per kg)
*
h
0
10
20
30
40
50
Glu
cose
turn
over
rat
e (
mg
per
kg p
er m
in)
Vehicle
Amlexanox(50 mg per kg)
0
20
40
60
80
100
Per
cent
age
supp
ress
ion
of H
GP
Vehicle
Amlexanox(50 mg per kg)
*
g
0
5
10
15
20
25
Pre Post
HG
P (
mg
per
kg p
er m
in)
Vehicle
Amlexanox(50 mg per kg)
*
Figure 4 Amlexanox treatment improves insulin sensitivity and glucose tolerance. (a) Oral glucose tolerance test in the preventative treatment group. n = 5 per group. (b) Fasting blood glucose and serum insulin concentrations in each treatment group. n = 8 per group. (c) Insulin tolerance test in each treatment group. n = 8 per group. (d) Oral glucose tolerance test of ob/ob mice gavaged with amlexanox or vehicle control. n = 8 per group. (e) Insulin tolerance test in ob/ob mice gavaged with amlexanox or vehicle control. n = 8 per group. (f–i) Hyperinsulinemic-euglycemic clamp in amlexanox-treated (50 mg per kg body weight) and vehicle-treated HFD-fed mice. n = 9 per group. (f) Area under the curve (AUC) for glucose infusion rate during clamp (GIR0–120 min). (g) Hepatic glucose production (HGP) before (pre) and after (post) the clamp (left) and percentage suppression of hepatic glucose production (right). (h) Glucose turnover rate during the clamp. (i) Fold suppression of serum free fatty acid (FFA) concentrations during the clamp. *P < 0.05 for HFD-fed vehicle-treated controls compared to HFD-fed amlexanox-treated mice or ob/ob vehicle-treated controls compared to ob/ob amlexanox-treated mice, †P < 0.05 for NCD-fed vehicle-treated controls compared to HFD-fed vehicle-treated controls (ANOVA with Tukey-Kramer post hoc analysis (a–c) or Student’s t test (d–i)). All data in the figure are shown as the mean ± s.e.m. or as a dot plot showing each data point and the mean.

©20
13 N
atu
re A
mer
ica,
Inc.
All
rig
hts
res
erve
d.
a r t i c l e s
� advance online publication nature medicine
cell–enriched proteins such as Slc2a4 and Pparg, which are indicative of improved insulin sensitivity, in WAT from amlexanox-treated mice (Fig. 6b). The expression of uncoupling protein 1 (UCP1) was also higher in the adipose tissue of amlexanox-treated DIO mice as compared to HFD-fed vehicle-treated controls (Fig. 6d).
To evaluate whether amlexanox might control energy metabolism by directly affecting inflammation, we examined the effects of the drug on primary macrophages or the cultured RAW267.2 macro-phage cell line. The addition of amlexanox did not affect macrophage migration in a wound-healing assay performed in RAW267.2 cells (Supplementary Fig. 5a). Bone marrow–derived and peritoneal macrophages from Ikbke knockout mice were slightly more responsive to the effects of LPS in inducing the expression of various cytokines (Supplementary Fig. 5b–d). We also evaluated the effect of these inhibitors on poly I:C– or TNF-α–stimulated NF-κB activation in adipocytes and found a slight increase in the activation of NF-κB after pretreatment with the IKK-ε and TBK1 inhibitors (Supplementary Fig. 5e). Moreover, bone marrow transplant from Ikbke-deficient mice into wild-type mice on a HFD did not influence weight or insulin sensitivity (data not shown). Together with the increase in TBK1
phosphorylation induced by the inhibitors described in Figure 2, these data indicate that inhibition of IKK-ε and TBK1 does not directly block the proinflammatory effects of cytokines or LPS on inflammatory signaling or the NF-κB pathway but, rather, may pre-vent feedback inhibition that is a consequence of elevated expression of TBK1 and IKK-ε. Thus, these noncanonical kinases do not act as IκB kinases and are not directly proinflammatory. However, IKK-ε and TBK1 may attenuate the inflammatory response without elimi-nating it. Thus, the induction of these ‘counterinflammatory’ kinases may contribute to the generation of low-grade, sustained inflamma-tion in obesity by preventing its resolution.
Amlexanox promotes energy expenditure in adipose tissueTo discern whether amlexanox directly influences phosphorylation in vivo, we first examined a number of proteins known to undergo hyperphosphorylation in states of obesity. As previously described35, phosphorylation of proteins in the mammalian target of rapamycin complex1 (mTORC1) pathway such as S6K and S6 were elevated in response to a HFD; this increase was largely attenuated in amlexanox-treated DIO mice (Fig. 6d and Supplementary Fig. 6a,b).
HFD amlexanoxHFD vehicled NCD vehicle HFD withdrawalHFD amlexanoxe HFD vehicle
a b
ND vehicle HFD vehicle HFD amlexanox
Live
r gl
ycog
en(µ
g gl
ucos
e pe
r m
g)
c
*
0
10
20
30
40
HFD amlexanox(25 mg per kg)
HFD vehicle
*
†
Live
r tr
igly
cerid
e (
mg
per
g)
†
*
Live
r m
ass
(g)
0
1
2
3
0
100
200
300
400
HFD amlexanox (25 mg per kg)NCD vehicle
h
0
1
2
3
4
Tnfa Cxcl10 Ccl5 Emr1 Itgax Ccl2 Ccl3 Cybb
Rel
ativ
e ge
ne e
xpre
ssio
n
*
†
*
†
^
†*
†
*
†
*
†
*
†
*
†
NCD vehicle HFD vehicle HFD amlexanox (25 mg per kg)
0
1
2
3
4
Fasn Me1 Acaca Scd1 Ppara Pparg Cd36
Rel
ativ
e ge
ne e
xpre
ssio
n
NCD vehicle HFD vehicle HFD amlexanox (25 mg per kg)f g
0
1
2
3
4
G6pc Pck1 Pklr Gck
Rel
ativ
e ge
ne e
xpre
ssio
n
†
†
*
†
*
†
*
†
*
†
*
†
*
†
*
†
*
†
*
†
*
#
*
Fabp4 Lpl
NCD vehicle HFD vehicle HFD amlexanox(25 mg per kg)
HFD vehicle
Figure 5 Amlexanox treatment reverses hepatic steatosis. (a) Macroscopic pictures of the livers of mice in each group indicated. Scale bar, 1 cm. (b) Total liver weight and triglyceride content of NCD-fed mice or HFD-fed mice gavaged with vehicle or amlexanox. n = 6 per group. (c) Liver glycogen content in HFD-fed mice treated with amlexanox or vehicle. n = 5 per group. (d,e) Representative images of H&E-stained livers in the groups indicated. Scale bars, 2 mm. (f–h) Expression of lipid metabolism genes (f), glucose metabolism genes (g) and inflammatory genes and macrophage markers (h) in the livers of mice in each treatment group. n = 6 per group. *P < 0.05 for HFD-fed vehicle- treated controls compared to HFD-fed amlexanox-treated mice, †P < 0.05 for NCD-fed vehicle-treated controls compared to HFD-fed vehicle-treated controls, #P < 0.1 for NCD-fed vehicle-treated controls compared to HFD-fed vehicle- treated controls (ANOVA with Tukey-Kramer post hoc analysis (b) or Student’s t test (c,f–h)). All data in the figure are shown as the mean ± s.e.m. or as a dot plot showing each data point and the mean.

©20
13 N
atu
re A
mer
ica,
Inc.
All
rig
hts
res
erve
d.
a r t i c l e s
nature medicine advance online publication �
Amlexanox also blocked induction of IKK-ε and TBK1 protein by a HFD in adipose tissue. This finding was consistent with the fact that overexpression of wild-type but not kinase-inactive TBK1 in cells enhanced the stimulation of S6K phosphorylation by insulin, whereas knockdown of Ikbke or Tbk1 in 3T3-L1 adipocytes lowered the amount of insulin-stimulated S6 phosphorylation (Supplementary Fig. 6c). In adipose tissue from HFD-fed mice, HSL phosphorylation was lower, which is consistent with the well-established desensitization of the β-adrenergic pathway in this tissue during obesity36. Amlexanox treatment prevented the reduction in HSL phosphorylation associ-ated with a HFD (Fig. 6d and Supplementary Fig. 6a,b).
In vehicle-treated control mice on a HFD, brown adipose tissue (BAT) accumulated large lipid droplets and acquired some of the features of white fat. Brown fat reverted to its normal appearance in amlexanox-treated mice (Supplementary Fig. 6d), with a corresponding reversal of HFD-induced triglyceride accumulation (Supplementary Fig. 6e). After withdrawal of amlexanox treatment, lipids again accu-mulated in the BAT, reverting to the HFD phenotype of control obese mice (Supplementary Fig. 6f). UCP1 protein expression was also markedly elevated in the BAT of amlexanox-treated mice (Fig. 6e and Supplementary Fig. 6g). Expression of the brown fat–specific markers Prdm16, Ppargc1a, Ppargc1b, Cidea and Ucp1 was higher in
amlexanox-treated mice (Fig. 6f). There was also an increase in the expression of cytochrome oxidases and Elovl3, which are involved in lipid metabolism in the BAT. Amlexanox treatment reduced IKK-ε and TBK1 protein expression in BAT (Fig. 6g and Supplementary Fig. 6h). We also found reduced signaling through the mTORC1 pathway in BAT of amlexanox-treated mice as compared to controls. Ex vivo treatment with amlexanox acutely stimulated lipid oxidation and oxygen consumption in BAT explants from HFD-fed mice, support-ing a direct effect of amlexanox on energy expenditure (Fig. 6h,i).
To evaluate the roles of IKK-ε and TBK1 in mediating the effects of the drug, we treated Ikbke knockout mice with amlexanox and monitored their weight loss and insulin sensitivity. The weight loss produced by amlexanox was equivalent between wild-type and Ikbke knockout mice, indicating that the upregulation of TBK1 in these mice may compensate for IKK-ε inhibition (Supplementary Fig. 7a). We also monitored insulin sensitivity by intermittent insulin toler-ance tests over several weeks of treatment (Supplementary Fig. 7b). Although Ikbke knockout mice were more insulin sensitive than their wild-type littermates, the drug produced an additional improvement, achieving the insulin sensitivity observed in wild-type mice treated with amlexanox. Improvements in insulin sensitivity preceded weight loss, indicating that improved insulin sensitivity may not be secondary
0
0.5
1.0
1.5
2.0
Tnfa
Ccl3
Ccl2
Ccl5
Cxcl10
Il10
Itgax
Emr1
Slc2a4
Pparg
Rel
ativ
e ge
ne e
xpre
ssio
n
Vehicle
Amlexanox (100 mg per kg)
a b
**
**
*
0
100
200
300
400
500
600
Il-10 Il-
1αM
cp1
Mip-
1α
Rante
s
TNF-α
Ser
um c
ytok
ine
(pg
ml–1
)
VehicleAmlexanox (100 mg per kg)
c
*
*
*
*
Vehicle Amlexanox
* *
0
2
4
6
Fasted Fed
Rel
ativ
eph
osph
oryl
atio
n
0
5
10
15
Fasted Fed
Rel
ativ
eph
osph
oryl
atio
n
d
0
0.5
1.0
1.5
2.0
pTBK1
Rel
ativ
eph
osph
oryl
atio
n
0
1
2
3
4
UCP1 IKK-ε TBK1
Rel
ativ
e pr
otei
n le
vels
(nor
mal
ized
to c
ontr
ol) Vehicle
Amlexanox (25 mg per kg)*
* *
*
pS6 pHSL
* *
*
*
VehicleAmlexanox
0
50
100
150
200
WT DKOOC
R (
pmol
min
–1 p
er w
ell)
*
j
0
20
40
60
80
100
Lipi
d ox
idat
ion
rate
(c.p
.m. m
g–1 h
–1)
VehicleAmlexanox
h
*
0
20
40
60
80
100
120
NCD HFD
OC
R (
nmol
min
–1 g
–1)
VehicleAmlexanox
i
*
0
0.5
1.0
1.5
2.0
pTBK1 pS6
Rel
ativ
eph
osph
oryl
atio
n
0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
IKK-ε TBK1 S6
Rel
ativ
e pr
otei
n le
vels
(nor
mal
ized
to c
ontr
ol)
VehicleAmlexanox (25 mg per kg)
g
*
*
*
0
1
2
Prdm16
Ppargc1a
Ppargc1b
Cidea
Ucp1
Cox7a1
Cox7a2
Cox8b
Elvol3
Rel
ativ
e G
ene
expr
essi
on (
AU
)
VehicleAmlexanox (25 mg per kg)
f
*** * * * *
*
*
eHFD vehicle HFD amlexanox
Figure 6 Amlexanox reduces inflammation and increases energy expenditure in adipose tissue. (a) Representative images of H&E-stained sections from WAT of ob/ob mice treated with vehicle control or amlexanox. Scale bars, 1 mm. (b) Expression of inflammatory genes and macrophage markers in WAT from ob/ob mice gavaged with vehicle control or amlexanox. n = 6 per group. (c) Serum cytokine concentrations in ob/ob mice gavaged with vehicle control or amlexanox. n = 6 per group. (d) Quantified amounts of protein and phosphorylation in WAT from mice treated with amlexanox or vehicle control (see also Supplementary Fig. 6b). (e) BAT stained for UCP1 in HFD-fed vehicle-treated controls and amlexanox-treated mice. Scale bars, 200 µm. (f) Expression of BAT-specific markers in BAT. n = 8 per group. AU, arbitrary units. (g) Quantified amounts of protein and phosphorylation in BAT from mice treated with amlexanox or vehicle control (see also Supplementary Fig. 6h). (h) Lipid oxidation rate in ex vivo BAT treated with amlexanox or vehicle control. n = 6 per group. (i) Oxygen consumption rate (OCR) in ex vivo BAT from NCD-fed and HFD-fed mice treated with amlexanox or vehicle control. n = 5 per group. (j) Oxygen consumption rate in wild-type (WT) and Ikbke and Tbk1 double-knockout (DKO) MEFs treated with amlexanox or vehicle control. n = 5 wells per group. *P < 0.05 for vehicle-treated controls compared to amlexanox-treated mice (Student’s t test). All data in the figure are shown as the mean ± s.e.m.

©20
13 N
atu
re A
mer
ica,
Inc.
All
rig
hts
res
erve
d.
a r t i c l e s
� advance online publication nature medicine
to weight loss. Taken together with the data in Figure 4, which show that the effects of amlexanox are comparable to those of other insulin-sensitizing drugs such as the thiazolidinediones37, these results suggest that amlexanox is a bona fide insulin sensitizer.
As Tbk1 knockout mice are not viable, we used mouse embryonic fibroblasts (MEFs) to further investigate the importance of these kinases in the specificity of amlexanox. Treatment of wild-type MEFs with amlexanox produced a dose-dependent increase in the phospho-rylation of TBK1 and the P65 NF-κB subunit, presumably because of feedback inhibition27. Both effects were absent in Ikbke and Tbk1 double-knockout MEFs (Supplementary Fig. 7c–e). However, MEFs with single knockout of either Ikbke or Tbk1 retained respon-siveness to amlexanox. In Ikbke knockout MEFs, we found TBK1 phosphorylation and degradation of IκB after amlexanox treat-ment, whereas Tbk1 knockout MEFs showed robust phosphoryla-tion of IKK-β in response to amlexanox treatment. Amlexanox also enhanced oxygen consumption in wild-type but not Ikbke and Tbk1 double-knockout MEFs, indicating that the energy expenditure- promoting effect of amlexanox is mediated specifically through inhi-bition of both IKK-ε and TBK1 (Fig. 6j). Taken together, these data suggest that amlexanox elicits its effects though specific inhibition of both IKK-ε and TBK1.
DISCUSSIONCompelling evidence has accrued over the past few years that both genetic and dietary forms of rodent obesity are accompanied by the generation of low-grade inflammation in key metabolic tissues, which serves as an important link between obesity and sustained insulin resistance7–11. Almost all rodent models of obesity-induced insulin resistance are associated with chronic inflammation, and a strong cor-relation between insulin resistance and inflammatory markers in stud-ies of several patient groups has been shown38–41. This inflammation is generally low grade and is accompanied by macrophage switching from a type 2 to a type 1 polarization state34,42,43, as well as the pres-ence of additional inflammatory cells44–47. Inhibition of inflammatory signaling by knockout of key pathways in obese mice can disrupt the link between obesity and insulin resistance11,48–55. Likewise, differ-ent anti-inflammatory pharmacological and genetic approaches can also reduce insulin resistance in rodents and patients56–58. Coculture studies and neutralizing antibodies directed against different proin-flammatory cytokines have demonstrated in vitro that inflammatory signals derived from M1-polarized macrophages can desensitize cells to insulin through different mechanisms23.
Although the molecular links between inflammation and insulin resistance are not yet completely understood, it is clear that the NF-κB program has a key role13. Disruption of NF-κB signaling by targeted knockout of the canonical IκB kinase IKK-β gene or pharmacologi-cal inhibition of this pathway can restore insulin sensitivity in obese states. However, the roles of the noncanonical IKKs, TBK1 and IKK-ε in this process are less well understood. Our previous studies indicated that deletion of the Ikbke gene partially restored insulin sensitivity and reduced weight in mice fed a HFD despite having no apparent effect on NF-κB signaling, although the relevant mechanism was not defined15. Here we describe amlexanox, a newly identified chemical inhibitor of IKK-ε and TBK1 that reproduces many of these effects. Administration of this compound to mice reduced weight, insulin resistance, inflammation and steatosis in three different obese mouse models. These effects are apparent within 3–4 weeks after starting drug therapy and are reversible. They are probably attributed to increased triglyceride hydrolysis and oxidation, along with reduced lipogenesis
and glycogenesis. Signaling pathways that modulate these processes are attenuated in vitro by the addition of amlexanox or another struc-turally unrelated inhibitor to cultured adipocytes.
The precise mechanisms by which amlexanox produces these bene-ficial effects in obese rodents have not yet been completely elucidated. Although amlexanox is known to be a mast cell stabilizer of unknown mechanism20, and depletion of mast cells may have beneficial meta-bolic effects59, most of the in vivo and in vitro evidence points to a role for the drug in increasing expenditure of energy while reducing its storage in adipocytes and hepatocytes. Furthermore, the lack of a phenotype in wild-type mice reconstituted with Ikbke knockout bone marrow indicates that the role of IKK-ε in bone marrow-derived cells such as mast cells and macrophages is less important than its role in other cell types such as adipocytes and hepatocytes. Although IKK-ε and TBK1 expression is elevated as part of the inflammatory program downstream of NF-κB, the kinase targets of the drug do not seem to be direct participants in the increased inflammatory program. In fact, the reduced inflammation observed in vivo with amlexanox treatment may be an indirect effect of improved metabolic disease or, perhaps, of elimination of a feedback pathway that maintains inflammation at low levels such that inflammation is permitted to resolve. Moreover, despite the fact that administration of amlexanox to obese mice restores insulin sensitivity, these compounds are not direct insulin sensitizers in vitro. Phosphorylation analyses indicate that IKK-ε and TBK1 may co-opt signaling pathways that drive energy conservation in the context of insulin resistance, ensuring that energy expenditure is kept in check by producing catecholamine resistance in adipose tissue, in the process reducing HSL phosphorylation and UCP1 expression while also increasing mTOR signaling to drive lipogenesis and glycogen synthesis. Thus, together these data suggest that expression of TBK1 and IKK-ε by obesity-dependent inflam-mation may conserve energy during the transition from an insulin- dependent to an insulin-independent state of nutrient storage. Moreover, it is probable that the improvement in insulin resist-ance produced by treatment with amlexanox results from reducing excessive energy storage while preventing homeostatic feedback loops (such as mTOR) that block insulin receptor signaling60.
Amlexanox seems to be a relatively safe drug with a long history of use in patients. As such, there might be an interesting opportunity for repurposing this agent for diabetes and obesity. Future clinical studies will be needed to explore this possibility and validate the hypothesis that these noncanonical IκB kinases contribute to counterinflamma-tory actions that sustain metabolic disease.
METHODSMethods and any associated references are available in the online version of the paper.
Note: Supplementary information is available in the online version of the paper.
ACkNOWLEDgMENTSWe thank J. Hung and X. Peng for excellent technical assistance and members of the Saltiel laboratory for helpful discussions. This work was supported by US National Institutes of Health grants DK60597 and 60591 to A.R.S., F32DK09685101 to S.M.R., F30DK089687 to J.M. and R24DK090962 to A.R.S., J.M.O. and R.M.E. R.M.E., M.D. and R.T.Y. are supported by the Leona M. and Harry B. Helmsley Charitable Trust. We thank S. Akira (Department of Host Defense, Research Institute for Microbial Diseases, Osaka University, Osaka, Japan) for providing MEFs. We also acknowledge support from the Michigan Diabetes Research and Training Center (DK020572), Michigan Institute for Clinical and Health Research (UL1-RR024986), Nathan Shock Center, Michigan Metabolic Phenotyping Core and Michigan Nutritional Obesity Research Center (DK089503).

©20
13 N
atu
re A
mer
ica,
Inc.
All
rig
hts
res
erve
d.
a r t i c l e s
nature medicine advance online publication �
AUTHOR CONTRIBUTIONSA.R.S. and S.M.R. wrote the manuscript. S.M.R. created figures. S.M.R. produced the data in Figures 1e, 3e,i, 4f–i, 5c,f–h and 6c–j and in Supplementary Figures 1, 2c–h, 5b,e,g,h and 6a,b. S.-H.C. produced the data in Figures 3a–d,f–h,j, 4a–e, 5a,c–e and 6a,b and in Supplementary Figures 2a,b, 3 and 5a,d,f. S.J.D. and M.J.L. performed the screen identifying amlexanox as an IKK-ε inhibitor. L.C. and S.J.D. produced the data in Figures 1b and 2b,c,f. M.U. produced the data in Figures 1a and 2e and in Supplementary Figures 5c and 6c–e. J.R.R. produced the images in Figure 1d. J.M. produced the data in Figure 1c. N.M.W. produced the data in Supplementary Figure 4a–d. I.H. produced the data in Supplementary Figure 4e. M.D., R.T.Y., C.L. and R.M.E. contributed data not shown, which was instrumental in generating Figure 5f–h. D.O. produced the data in Figure 1d and the samples for Figure 1e. P.L. produced the data in Figure 1f under the guidance of J.M.O.
COMPETING FINANCIAL INTERESTSThe authors declare no competing financial interests.
Published online at http://www.nature.com/doifinder/10.1038/nm.3082. Reprints and permissions information is available online at http://www.nature.com/reprints/index.html.
1. Taniguchi, C.M., Emanuelli, B. & Kahn, C.R. Critical nodes in signalling pathways: insights into insulin action. Nat. Rev. Mol. Cell Biol. 7, 85–96 (2006).
2. Reaven, G.M. The insulin resistance syndrome: definition and dietary approaches to treatment. Annu. Rev. Nutr. 25, 391–406 (2005).
3. Reaven, G.M. Why Syndrome X? From Harold Himsworth to the insulin resistance syndrome. Cell Metab. 1, 9–14 (2005).
4. Stumvoll, M., Goldstein, B.J. & van Haeften, T.W. Type 2 diabetes: principles of pathogenesis and therapy. Lancet 365, 1333–1346 (2005).
5. Biddinger, S.B. & Kahn, C.R. From mice to men: insights into the insulin resistance syndromes. Annu. Rev. Physiol. 68, 123–158 (2006).
6. Doria, A., Patti, M.E. & Kahn, C.R. The emerging genetic architecture of type 2 diabetes. Cell Metab. 8, 186–200 (2008).
7. Olefsky, J.M. & Glass, C.K. Macrophages, inflammation, and insulin resistance. Annu. Rev. Physiol. 72, 219–246 (2010).
8. Li, P. et al. Functional heterogeneity of CD11c-positive adipose tissue macrophages in diet-induced obese mice. J. Biol. Chem. 285, 15333–15345 (2010).
9. Lumeng, C.N. & Saltiel, A.R. Inflammatory links between obesity and metabolic disease. J. Clin. Invest. 121, 2111–2117 (2011).
10. Gregor, M.F. & Hotamisligil, G.S. Inflammatory mechanisms in obesity. Annu. Rev. Immunol. 29, 415–445 (2011).
11. Hotamisligil, G.S. Endoplasmic reticulum stress and the inflammatory basis of metabolic disease. Cell 140, 900–917 (2010).
12. Wunderlich, F.T. et al. Hepatic NF-κB essential modulator deficiency prevents obesity-induced insulin resistance but synergizes with high-fat feeding in tumorigenesis. Proc. Natl. Acad. Sci. USA 105, 1297–1302 (2008).
13. Arkan, M.C. et al. IKK-β links inflammation to obesity-induced insulin resistance. Nat. Med. 11, 191–198 (2005).
14. Goldfine, A.B. et al. The effects of salsalate on glycemic control in patients with type 2 diabetes: a randomized trial. Ann. Intern. Med. 152, 346–357 (2010).
15. Chiang, S.H. et al. The protein kinase IKKε regulates energy balance in obese mice. Cell 138, 961–975 (2009).
16. Chau, T.L. et al. Are the IKKs and IKK-related kinases TBK1 and IKK-epsilon similarly activated? Trends Biochem. Sci. 33, 171–180 (2008).
17. Chariot, A. The NF-κB–independent functions of IKK subunits in immunity and cancer. Trends Cell Biol. 19, 404–413 (2009).
18. Kawai, T. & Akira, S. Signaling to NF-κB by Toll-like receptors. Trends Mol. Med. 13, 460–469 (2007).
19. Kravchenko, V.V., Mathison, J.C., Schwamborn, K., Mercurio, F. & Ulevitch, R.J. IKKi/IKKε plays a key role in integrating signals induced by pro-inflammatory stimuli. J. Biol. Chem. 278, 26612–26619 (2003).
20. Makino, H., Saijo, T., Ashida, Y., Kuriki, H. & Maki, Y. Mechanism of action of an antiallergic agent, amlexanox (AA-673), in inhibiting histamine release from mast cells. Acceleration of cAMP generation and inhibition of phosphodiesterase. Int. Arch. Allergy Appl. Immunol. 82, 66–71 (1987).
21. Bell, J. Amlexanox for the treatment of recurrent aphthous ulcers. Clin. Drug Investig. 25, 555–566 (2005).
22. Saltiel, A.R. Insulin resistance in the defense against obesity. Cell Metab. 15, 798–804 (2012).
23. Lumeng, C.N., Deyoung, S.M. & Saltiel, A.R. Macrophages block insulin action in adipocytes by altering expression of signaling and glucose transport proteins. Am. J. Physiol. Endocrinol. Metab. 292, E166–E174 (2007).
24. Karin, M., Yamamoto, Y. & Wang, Q.M. The IKK NF-κB system: a treasure trove for drug development. Nat. Rev. Drug Discov. 3, 17–26 (2004).
25. Oh, D.Y. et al. GPR120 is an omega-3 fatty acid receptor mediating potent anti-inflammatory and insulin-sensitizing effects. Cell 142, 687–698 (2010).
26. Ma, X. et al. Molecular basis of Tank-binding kinase 1 activation by transautophosphorylation. Proc. Natl. Acad. Sci. USA 109, 9378–9383 (2012).
27. Clark, K., Takeuchi, O., Akira, S. & Cohen, P. The TRAF-associated protein TANK facilitates cross-talk within the IκB kinase family during Toll-like receptor signaling. Proc. Natl. Acad. Sci. USA 108, 17093–17098 (2011).
28. Bamborough, P. et al. 5-(1H-Benzimidazol-1-yl)-3-alkoxy-2-thiophenecarbonitriles as potent, selective, inhibitors of IKK-εn kinase. Bioorg. Med. Chem. Lett. 16, 6236–6240 (2006).
29. Clark, K. et al. Novel cross-talk within the IKK family controls innate immunity. Biochem. J. 434, 93–104 (2011).
30. Torii, H. et al. Metabolic fate of amoxanox (AA-673), a new antiallergic agent, in rats, mice, guinea-pigs and dogs. Jpn. Pharmacol. Ther. 13, 4933–4954 (1985).
31. Friedman, J.M. Modern science versus the stigma of obesity. Nat. Med. 10, 563–569 (2004).
32. Friedman, J.M. & Halaas, J.L. Leptin and the regulation of body weight in mammals. Nature 395, 763–770 (1998).
33. Weisberg, S.P. et al. Obesity is associated with macrophage accumulation in adipose tissue. J. Clin. Invest. 112, 1796–1808 (2003).
34. Lumeng, C.N., Bodzin, J.L. & Saltiel, A.R. Obesity induces a phenotypic switch in adipose tissue macrophage polarization. J. Clin. Invest. 117, 175–184 (2007).
35. Um, S.H. et al. Absence of S6K1 protects against age- and diet-induced obesity while enhancing insulin sensitivity. Nature 431, 200–205 (2004).
36. Seals, D.R. & Bell, C. Chronic sympathetic activation: consequence and cause of age-associated obesity? Diabetes 53, 276–284 (2004).
37. Olefsky, J.M. & Saltiel, A.R. PPARγ and the treatment of insulin resistance. Trends Endocrinol. Metab. 11, 362–368 (2000).
38. Pradhan, A.D., Manson, J.E., Rifai, N., Buring, J.E. & Ridker, P.M. C-reactive protein, interleukin 6, and risk of developing type 2 diabetes mellitus. J. Am. Med. Assoc. 286, 327–334 (2001).
39. Festa, A., D′Agostino, R. Jr., Tracy, R.P. & Haffner, S.M. Elevated levels of acute-phase proteins and plasminogen activator inhibitor-1 predict the development of type 2 diabetes: the insulin resistance atherosclerosis study. Diabetes 51, 1131–1137 (2002).
40. Blackburn, P. et al. Postprandial variations of plasma inflammatory markers in abdominally obese men. Obesity (Silver Spring) 14, 1747–1754 (2006).
41. Aron-Wisnewsky, J. et al. Human adipose tissue macrophages: m1 and m2 cell surface markers in subcutaneous and omental depots and after weight loss. J. Clin. Endocrinol. Metab. 94, 4619–4623 (2009).
42. Schenk, S., Saberi, M. & Olefsky, J.M. Insulin sensitivity: modulation by nutrients and inflammation. J. Clin. Invest. 118, 2992–3002 (2008).
43. Odegaard, J.I. & Chawla, A. Alternative macrophage activation and metabolism. Annu. Rev. Pathol. 6, 275–297 (2011).
44. Nishimura, S. et al. CD8+ effector T cells contribute to macrophage recruitment and adipose tissue inflammation in obesity. Nat. Med. 15, 914–920 (2009).
45. Winer, S. et al. Normalization of obesity-associated insulin resistance through immunotherapy. Nat. Med. 15, 921–929 (2009).
46. Feuerer, M. et al. Lean, but not obese, fat is enriched for a unique population of regulatory T cells that affect metabolic parameters. Nat. Med. 15, 930–939 (2009).
47. Winer, D.A. et al. B cells promote insulin resistance through modulation of T cells and production of pathogenic IgG antibodies. Nat. Med. 17, 610–617 (2011).
48. Nakamura, T. et al. Double-stranded RNA–dependent protein kinase links pathogen sensing with stress and metabolic homeostasis. Cell 140, 338–348 (2010).
49. Summers, S.A. Sphingolipids and insulin resistance: the five Ws. Curr. Opin. Lipidol. 21, 128–135 (2010).
50. Vandanmagsar, B. et al. The NLRP3 inflammasome instigates obesity-induced inflammation and insulin resistance. Nat. Med. 17, 179–188 (2011).
51. Saberi, M. et al. Hematopoietic cell-specific deletion of toll-like receptor 4 ameliorates hepatic and adipose tissue insulin resistance in high-fat–fed mice. Cell Metab. 10, 419–429 (2009).
52. Wellen, K.E. et al. Coordinated regulation of nutrient and inflammatory responses by STAMP2 is essential for metabolic homeostasis. Cell 129, 537–548 (2007).
53. Lesniewski, L.A. et al. Bone marrow–specific Cap gene deletion protects against high-fat diet–induced insulin resistance. Nat. Med. 13, 455–462 (2007).
54. Holland, W.L. et al. Inhibition of ceramide synthesis ameliorates glucocorticoid-, saturated-fat-, and obesity-induced insulin resistance. Cell Metab. 5, 167–179 (2007).
55. Shi, H. et al. TLR4 links innate immunity and fatty acid-induced insulin resistance. J. Clin. Invest. 116, 3015–3025 (2006).
56. Solomon, D.H. et al. Association between disease-modifying antirheumatic drugs and diabetes risk in patients with rheumatoid arthritis and psoriasis. J. Am. Med. Assoc. 305, 2525–2531 (2011).
57. Hundal, R.S. et al. Mechanism by which high-dose aspirin improves glucose metabolism in type 2 diabetes. J. Clin. Invest. 109, 1321–1326 (2002).
58. Zhang, X. et al. Selective inactivation of c-Jun NH2-terminal kinase in adipose tissue protects against diet-induced obesity and improves insulin sensitivity in both liver and skeletal muscle in mice. Diabetes 60, 486–495 (2011).
59. Liu, J. et al. Genetic deficiency and pharmacological stabilization of mast cells reduce diet-induced obesity and diabetes in mice. Nat. Med. 15, 940–945 (2009).
60. Zick, Y. Ser/Thr phosphorylation of IRS proteins: a molecular basis for insulin resistance. Sci. STKE 2005, pe4 (2005).

©20
13 N
atu
re A
mer
ica,
Inc.
All
rig
hts
res
erve
d.
nature medicine doi:10.1038/nm.3082
ONLINE METHODSReagents. All chemicals were obtained from Sigma-Aldrich unless otherwise stated. Antibodies to IKK-ε (2690), TBK1 (3013), pTBK1 (Ser172; 5483), IKK-α and IKK-β (2684), pIKK-α and pIKK-β (Ser176; 2687), AKT (9272), pAKT (Ser473; 9272), S6K (2708, diluted 1:250), pS6K (Thr389; 9205), S6 (2317), pS6 (Ser235 and Ser236; 2211), IRF3 (4302), pIRF3 (Ser396; 4947), HSL (4107), pHSL (Ser563; 4139, or Ser660; 4126) and PPAR-γ (2443) were purchased from Cell Signaling. RalA-specific antibody (610222) was obtained from BD Bioscience. UCP1-specific antibody (UCP11-A, diluted 1:250 for WAT detec-tion) was obtained from Alpha Diagnostics. All antibodies were diluted 1:1,000 unless otherwise noted. Enhanced chemiluminescence reagents were pur-chased from NEN, Inc. EDTA-free protease inhibitor tablet was purchased from Roche Diagnostics.
Animals and animal care. We fed wild-type male C57BL/6 mice a HFD consist-ing of 45% of calories from fat (D12451 Research Diets Inc.) starting at 8 weeks of age for 12–24 weeks, and we maintained NCD-fed male C57BL/6 controls on normal chow diet consisting of 4.5% fat (5002 Lab Diet). We fed the C57BL/6 mice diets containing ω-3 fatty acids as previously described25. Rosiglitazone treatment was administered for 3 weeks by addition of the compound to the diet in mice that had been on HFD for 16 weeks. Each mouse consumed on average 3.5 mg per kg body weight rosiglitazone per day. Amlexanox was administered by daily oral gavage. For the prevention groups, amlexanox (25 mg per kg or 100 mg per kg body weight) administration was begun concurrently with HFD feeding at 8 weeks of age. For the treatment groups, 25 mg per kg body weight amlexanox treatment was begun at 20 weeks of age after 12 weeks of HFD. To test the effect of amlexanox withdrawal, mice in the treatment group were switched from amlexanox gavage to vehicle control after 8 weeks of amlexanox treatment. We fed control and ob/ob mice a normal chow diet and gavaged them with 100 mg per kg body weight amlexanox or vehicle control beginning at 10 weeks of age. Mice were housed in a specific pathogen-free facility with a 12-h light, 12-h dark cycle and given free access to food and water. All animal use was in compliance with the Institute of Laboratory Animal Research Guide for the Care and Use of Laboratory Animals and approved by the University Committee on Use and Care of Animals at the University of Michigan and University of California San Diego.
Food intake. The remaining weight of food provided was determined daily for singly housed mice. Daily food consumption was calculated from a 3-d average.
Energy expenditure and respiratory quotient. C57BL/6 mice in the amlexanox treatment group were placed in metabolic cages. The University of Michigan Metabolic Phenotyping Core measured oxygen consumption (VO2), carbon dioxide production (VCO2) and spontaneous motor activity during 3 consecu-tive days using the Comprehensive Laboratory Monitoring System (Columbus Instruments), an integrated open-circuit calorimeter equipped with an optical beam activity monitoring system53. Values presented are normalized to body weight. The respiratory quotient was calculated by dividing the carbon dioxide production by the oxygen consumption. We used the mean values for the light and dark cycles to analyze statistical significance.
Body composition. The University of Michigan Metabolic Phenotyping Core used nuclear magnetic resonance analysis to quantify body fat, lean body mass and fluid content in ob/ob mice and C57BL/6 mice in the amlexanox treatment group.
Hyperinsulinemic-euglycemic clamp. C57BL/6 mice were placed on HFD starting at 8 weeks of age, and starting at 16 weeks of age, the mice were gavaged daily with 50 mg per kg body weight amlexanox or vehicle control. After 4 weeks of treatment, the right jugular vein and carotid artery were surgically catheterized, and mice were given 5 d to recover from the surgery. During this recovery period, amlexanox was delivered in drinking water. On the day of the clamp, a final oral gavage treatment was performed. After a 5- to 6-h fast, hyperinsulinemic clamp studies were performed on conscious mice using the protocol adopted from the Vanderbilt Mouse Metabolic Phenotyping Center by the University of Michigan Animal Phenotyping Core consisting of a
90-min equilibration period followed by a 120-min experimental period (t = 0 to t = 120 min). Insulin was infused at 4.0 mU per kg body weight per min. This experiment was performed at the University of Michigan Metabolic Phenotyping Core. We measured serum free fatty acid concentrations using the colorimetric NEFA-HR(2) kit (Wako).
Core body temperature. We performed rectal temperature measurements using a YSI 4600 Precision thermometer (YSI, Inc.).
Blood chemistry analysis. Blood glucose was measured by OneTouch Ultra Glucometer. Plasma from mice fasted for 6 h was isolated from whole blood collected into heparinized tubes. We used an insulin ELISA kit (Crystal Chem Inc.) to measure serum insulin concentrations. Leptin and adiponectin con-centrations were measured by ELISA kits purchased from Cayman Chem Inc. We quantified serum cytokine concentrations using luminex technology in a multianalyte panel plate purchased from Millipore. Additionally, we measured TNF-α concentrations using ELISA kits purchased from R&D Systems.
Glucose and insulin tolerance tests. For glucose tolerance tests, after a 6-h fast, we gavaged mice with glucose at a dose of 1.5 g per kg body weight (C57BL/6 mice) or 1.2 g per kg body weight (ob/ob mice). For insulin tolerance tests, mice were fasted for 3 h and then given an intraperitoneal injection of insulin (1.2 units per kg body weight for C57BL/6 mice and 2.0 units per kg body weight for ob/ob mice). We measured the basal blood glucose level and then at 15, 30, 45, 60, 90, 120 and 180 min from tail blood using the OneTouch Ultra glucometer (Lifescan).
Tissue lipid content. We isolated liver lipids by ethanolic KOH saponification and BAT lipids by chloroform extraction and then quantified triglyceride con-centrations using the Triglyceride Reagent kit (Thermo Scientific).
Liver glycogen content. We digested liver tissue in a 30% potassium hydro-xide solution and then precipitated glycogen using 70% ethanol. After three washes (resuspend pellet in water, then add ethanol to 70% and centrifuge down the pellet) to remove any traces of glucose, we digested glycogen by addition of amyloglucosidase. Released glucose was quantified using a colori-metric kit (Wako).
Stromal vascular fraction (SVF) and adipocyte isolation. We digested excised WAT in PBS containing 1% BSA and 1 mg ml−1 type II collagenase for 30 min at 37 °C with gentle agitation. The cell suspension was filtered through a 100-µm filter and then centrifuged at 700g for 5 min to separate floating adipocytes from the SVF pellet. We washed floating adipocytes twice with PBS containing 1% BSA and collected the SVF pellets after each wash.
Western blot analysis. We homogenized tissues in lysis buffer (50 mM Tris, pH 7.5, 5 mM EDTA, 250 mM sucrose, 1% NP-40, 2 mM dithiothreitol (DTT), 1 mM sodium vanadate, 100 mM NaF, 10 mM Na4P2O7 and freshly added protease inhibitor tablet) and then incubated them for 1 h at 4 °C15. We cen-trifuged crude lysates at 14,000g for 15 min twice and determined the protein concentration using BioRad Protein Assay Reagent. Samples were diluted in SDS sample buffer. Bound proteins were resolved by SDS-PAGE and transferred to nitrocellulose membranes (Bio-Rad). Individual proteins were detected with the specific antibodies and visualized on film using horseradish peroxidase–conjugated secondary antibodies (Bio-Rad) and Western Lightning Enhanced Chemiluminescence (Perkin Elmer Life Sciences). Alternatively, infrared flu-orescent secondary antibodies were used for detection and quantification of specific protein on the Odyssey CLx imager (LI-COR).
Histochemistry. Tissues were fixed in formalin for 3 d. The University of Michigan Cancer Center Research Histology Laboratory performed histology. A 1:100 dilution of the UCP1-specific antibody (UCP11, Alpha Diagnostics) at 10 µg ml−1 was used for immunohistochemical detection of UCP1 protein.
Gene expression analysis. We rinsed isolated mouse tissues in PBS and then froze them in liquid nitrogen and stored them at −80 °C until extraction.

©20
13 N
atu
re A
mer
ica,
Inc.
All
rig
hts
res
erve
d.
nature medicinedoi:10.1038/nm.3082
We extracted total RNA from liver, WAT and BAT tissues, as well as differentiated 3T3-L1 cells, using the RNeasy Lipid Tissue Kit (Qiagen) according to the manufacturer’s instructions with the inclusion of a DNase digestion step. We extracted total RNA from bone marrow–derived macrophages and SVF cells using the RNeasy Kit (Qiagen) with a DNase step. We used the Superscript First-Strand Synthesis System for RT-PCR (Invitrogen) with random primers for reverse transcription. Real-time PCR amplification of the complementary DNA was performed on samples in triplicate with Power SYBR Green PCR Master Mix (Applied Biosystems) using the Applied Biosystems 7900HT Fast real-time PCR System. We chose Adrp (also known as Plin2) and GAPDH as the internal controls for normalization after screening several candidate genes; their expression was not substantially affected by experimental conditions. The sequences of all primers used in this study are listed in Supplementary Table 1. Data were analyzed using the 2−∆∆CT method, and the control sample value was normalized to 1. Other data were quantified using an internal stand-ard curve. Statistical significance was determined using the unpaired hetero-scedastic Student’s t test with one averaged sample value per mouse.
Lipid oxidation rate. We excised intrascapular BAT and placed it in DMEM with 2% BSA with or without 50 µM amlexanox then incubated it at 37 °C for 1 h, after which we changed the medium to DMEM with 2% BSA, 0.25 mM carnitine, 0.2 mM palmitic acid and trace levels of 3H-palmitic acid and incubated it for 1 more hour at 37 °C and then collected the medium and isolated the aqueous faction. Lipid oxidation was determined by the conver-sion of 3H-palmitic acid to 3H2O.
IKK-« and TBK1 in vitro kinase assays. We performed in vitro kinase assays by incubating purified kinase (IKK-ε or TBK1) in kinase buffer containing 25 mM Tris (pH 7.5), 10 mM MgCl2, 1 mM DTT and 10 µM ATP for 30 min at 30 °C in the presence of 0.5 µCi γ-[32P]-ATP and 1 µg MBP per sample as a substrate. We stopped the kinase reaction by adding 4× SDS sample buffer and boiling for 5 min at 95 °C. Supernatants were resolved by SDS-PAGE, transferred to nitrocel-lulose and analyzed by autoradiography using a Typhoon 9410 phosphorimager (GE Lifesciences). We quantified the bands using ImageQuant.
IKK-« and TBK1 immunocomplex kinase assay. We collected liver and WAT from C57BL/6 mice on NCD or HFD and homogenized the tissues using a Dounce homogenizer with lysis buffer containing 50 mM Tris (pH 7.5), 150 mM NaCl, 2 mM EDTA, 5 mM NaF, 25 mM β-glycerophosphate, 1 mM sodium orthovanad-ate, 10% glycerol, 1% Triton X-100, 1 mM DTT and 1 mM PMSF in the presence of protease inhibitors (Roche Diagnostics). We incubated tissue cell lysates for 1 h at 4 °C and cleared them by spinning at 13,000 r.p.m. for 15 min at 4 °C in a table-top centrifuge. Each 1 mg of lysate was subjected to immunoprecipitation using 5 µl of undiluted rabbit polyclonal antibody to TBK1 or IKK-ε for 1.5 h at 4 °C. We harvested immunocomplexes by incubation with ProtA beads (Roche Diagnostics) for 2 h at 4 °C. We washed immunoprecipitates once with lysis buffer and three times with wash buffer containing 20 mM 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid (HEPES) (pH 7.4), 50 mM NaCl, 20 mM β-glycerophosphate, 1 mM sodium orthovanadate, 5 mM NaF, 10 mM MgCl2 and 1 mM DTT. We performed an in vitro kinase assay using the immunoprecipitated kinases as described above. Relative amounts of MBP phosphorylation were
detected by autoradiograph and normalized to the amounts of IKK-ε or TBK1 kinase detected in the immunoprecipitate by immunoblotting.
Cell culture. 3T3-L1 fibroblasts (American Type Culture Collection) were cultured in 10% neonatal calf serum in DMEM for proliferation and 10% FBS in DMEM for differentiation. We grew the cells to confluence and then induced differentiation 2 d later with 500 µM 3-isobutyl-1-methylxanthine, 250 nM dexamethasone and insulin (1 µg ml−1) for 3 d followed by insulin-only treatment for 2 d. We routinely used cells within 7 d after completion of the differentiation process and only used cultures in which >90% of cells showed adipocyte morphology. We serum starved 3T3-L1 adipocytes with 0.5% FBS in DMEM before treatment. TNF-α treatments (50 ng ml−1, unless otherwise noted) were performed during the 24 h before harvest and after pretreatment with the IKK-β inhibitor compound VIII (EMD Biosciences) for 1 h where indicated. We pretreated 3T3-L1 adipocytes for 1 h with amlexanox at the given concentrations and then treated them with 20 µg ml−1 of poly I:C for 1 h. Alternatively, we treated 3T3-L1 adipocytes with 50 µM forskolin for 15 min after a 30-min amlexanox pretreatment. We treated cells with or without 10 nM of insulin for 15 min. We determined glycerol release into the superna-tant (DMEM without phenol red) using a colorimetric assay. We serum starved RAW264.7 cells with 0.5% FBS in DMEM medium and pretreated them with or without Cay10576 (Cayman Chemical). The cells were then treated with LPS (0.5 µg ml−1) or poly I:C (50 µg ml−1) for 1 h. We harvested the cells for total RNA and analyzed them by real-time PCR. We also resolved cell lysates by SDS-PAGE and analyzed them by immunoblotting using the indicated antibodies. Wild-type and Ikbke Tbk1 double-knockout and Ikbke or Tbk1 single-knockout MEFs were kindly provided by S. Akira. Cells were cultured in DMEM with 10% FBS and serum starved in 0.5% FBS for 12 h before treat-ment. TNF-α treatment (50 ng ml−1) was performed for 15 min at the end of a 2-h pretreatment with amlexanox.
Oxygen consumption rate. The Michigan Metabolic Phenotyping Core and Michigan Nutritional Obesity Research Center measured oxygen consumption in cells and ex vivo tissue using an extracellular flux analyzer (model XF24-3, Seahorse Bioscience).
Molecular modeling of amlexanox in the TBK1 ATP-binding site. We mod-eled amlexanox into the known structure of the TBK1 catalytic domain (Protein Data Bank ID codes 4EUT and 4EUU and ref. 26). The best fit of amlexanox in the active site of TBK1 was obtained using AutoDock Vina.
Statistical analyses. Averaged values are presented as the mean ± s.e.m. When comparing two groups, we determined statistical significance using Student’s t test. When more than two groups were investigated, we first performed an analysis of variance (ANOVA) to establish that not all groups were equal. After a statistically significant ANOVA result, we performed between-group compari-sons using the Tukey-Kramer post hoc analysis. ANOVA and Tukey-Kramer tests were performed using Stata version 12.0.
Additional methods. Detailed methodology is described in the Supplementary Methods.






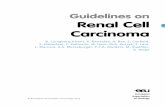
![Effect of an NF-κB Inhibitor on the Cell Population in the ... files NSR...‡2-[(aminocarbonyl)amino]-5-(4-fluorophenyl)-3-thiophenecarboxamide, an IkB kinase-2 (IKK-2) inhibitor](https://static.fdocument.org/doc/165x107/601b189320a986674c0e7c53/effect-of-an-nf-b-inhibitor-on-the-cell-population-in-the-nsr-a2-aminocarbonylamino-5-4-fluorophenyl-3-thiophenecarboxamide.jpg)