FAST FORWARD FESTIVAL 3 | ΣΤΙΣ (ΣΥΝ)ΟΡΙΑΚΕΣ ΠΕΡΙΟΧΕΣ ΤΗΣ ΤΕΧΝΗΣ

Acute Heart Failure: Management algorithms
J. ParissisJ. Parissis
Athens, Greece

ESC Guidelines for the Diagnosis and Treatment of
Acute and Chronic Heart Failure 2008
© 2008 The European Society of Cardiology

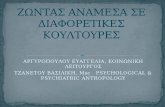
ΟΞΕΙΕΣ ΕΠΙ∆ΕΙΝΣΕΙΣ ΤΗΣ ΚΑΡ∆ΙΑΚΗΣ ΑΝΕΠΑΡΚΕΙΑΣ
ΕΠΙ∆ΕΙΝΝΟΥΝ ΤΗΝ ΚΑΡ∆ΙΑΚΗ ΛΕΙΤΟΥΡΓΙΑΕΠΙ∆ΕΙΝΝΟΥΝ ΤΗΝ ΚΑΡ∆ΙΑΚΗ ΛΕΙΤΟΥΡΓΙΑ
Discharge status and Discharge status and
chronic optimization
may prevent worsening
Ventr
icula
r fu
nction
Acute event
With each event,
hemodynamic alterations
contribute to progressive
Ventr
icula
r fu
nction
Acute eventcontribute to progressive
ventricular dysfunction
Time
Gheorghiade M, De Luca L, Fonarow G, et al. Am J Cardiol 2005.

ΣΥΝ∆ΡΟΜΑ ΟΞΕΙΑΣ ΚΑ: Η ΣΤΑΧΤΟΠΟΥΤΑ ΤΗΣ
ΚΑΡ∆ΙΑΚΗΣ ΑΝΕΠΑΡΚΕΙΑΣ
• Decompensated Chronic HF
• Pulnonary Edema• Pulnonary Edema
• Hypertensive HF
• Cardiogenic Shock• Cardiogenic Shock
• Isolated Right HF
• ACS and HF
ESC Classification, EHJ 2008.

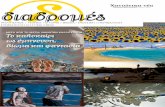
Η ΑΛΛΕΠΙΚΑΛΥΨΗ Τ�Ν ΣΥ∆ΡΟΜ�Ν Ο∆ΗΓΕΙ ΣΕ
∆ΑΙΦΟΡΕΤΙΚΗ ΑΝΤΙΠΡΟΣ�ΠΕΥΣΗ ΤΟΥΣ ΣΤΙΣ
ΚΑΤΑΓΑΦΕΣΚΑΤΑΓΑΦΕΣ
4%7%
1%
ALARM�HFEHS HFII
3%11%
39%
7%
12%
11%
4%
16%
65%
37%
AdHF Pulmonary oedema Cardiogenic shock
Hypertensive HF Right HF High cardiac output failure
Pulmonary oedema (16% vs. 37%) and cardiogenic shock (4% vs. 12%)
were significantly different between the two studies. were significantly different between the two studies.
EHS HF II: 3,580 patients, ALARM.HF: 4,953 patients (1911 AdHF, 1820 p.oed, 581 C.shock, 365 Hyp AHF,
222 RV AHF, 54 High cardiac output)

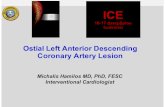
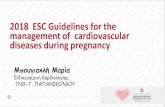
Η ΣΥΣΤΟΛΙΚΗ ΑΡΤΗΡΙΑΚΗ ΠΙΕΣΗ ΕΙΣΟ∆ΟΥ ΕΙΝΑΙ Ο
ΙΣΧΥΡΟΤΕΡΟΣ ΠΡΟΓΝ�ΣΤΙΚΟΣ ΠΑΡΑΓΟΝΤΑΣ
EFICA Study
1.0
EFICA Study
High SBP
Surv
ival ra
te,
%
68%
0.5
Normal SBP
Cardiogenic shock
Surv
ival ra
te,
%
38%
0
Cardiogenic shock
Surv
ival ra
te,
%
17%
0
0 100 200 300 400
Number of days
Zannad F, Mebazaa A, et al. Eur J Heart Fail 2006;8:697/705.

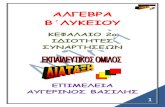
ΤΑΞΙΝΟΜΗΣΗ ΑΝΑΛΟΓΑ ΜΕ ΤΗΝ ΑΡΧΙΚΗ
ΣΥΣΤΟΛΙΚΗ ΑΡΤΗΡΙΑΚΗ ΠΙΕΣΗ
Acute Heart Failure
SBP >140 mmHg SBP <140 mmHg
Acute Heart Failure
Hypertensive
(cardiovascular)
SBP >140 mmHg SBP <140 mmHg
Non�Hypertensive
(Cardiac)(cardiovascular) (Cardiac)
90< SBP <140 mmHg SBP ≤90 mmHg• 43"50 % of ADHF cases
• Usually elderly women
with preserved LVEF
Normotensive Hypotensive
with preserved LVEF
• In"hospital mortality: <2%
• 48"50 % of AHF cases
• Usually decompensation of
• 2"8 % of AHF cases
• Includes cardiogenic• Usually decompensation of
chronic HF with depressed
LVEF
• In"hospital mortality: 8"10%
• Includes cardiogenic
shock (CS)
• In"hospital mortality: >15%
(>30% in CS)
Triposkiadis F, Parissis J, Starling R, et al. Exp Opin Investig Drugs 2009;18:1"13.

ΟΞΕΙΑ ΚΑ ΜΕ ΣΥΣΤΟΛΙΚΗ ΑΡΤΗΡΙΑΚΗ ΠΙΕΣΗ >90 mm
Hg: ∆ΥΟ ∆ΙΑΦΟΡΕΤΙΚΟΙ ΚΛΙΝΙΚΟΙ ΦΑΙΝΟΤΥΠΟΙ
Cardiovascular Failure
• High blood pressure
Cardiac Failure
• Normal blood pressure
• Rapid worsening
• Pulmonary congestion
• PCWP acutely increased
• Gradual worsening (days)
• Systemic rather than pulmonary
congestion• PCWP acutely increased
• Rales: present
• Severe radiographic congestion
• Weight gain minimal
• PCWP chronically high
• Rales: may be absent
• Radiographic congestion may • Weight gain minimal
• LVEF relatively preserved
• Response to therapy:
relatively rapid
• Radiographic congestion may
be present
• Weight gain significant (edema)
• LVEF usually lowrelatively rapid • LVEF usually low
• Response to therapy: continue
to have systemic congestion
in spite of the initial symptomatic
responseresponse
Gheorghiade M. Am J Cardiol 2005;96[suppl]:11G217G.


Clinical Assessment of Acute Heart Failure
SyndromesSyndromes
Nohria et al. Am J Cardiol 2005;96[suppl]:32G–40G

Acutely decompensated Heart Failure
High jugular venous
pressure Pulmonary congestion/pressure Pulmonary congestion/
oedema
Haemodynamic findings:Low cardiac output (C.I < 2.5 L/min)
High PCW'pressure (>16 mmHg)Peripheral
Vasoconstriction
High PCW'pressure (>16 mmHg)
High systemic vascular resistence

ΑΞΙΑ ΤΗΣ ∆ΙΑΦΟΡΙΚΗΣ ΠΙΕΣΗΣ ΣΤΗΝ ΠΡΟΒΛΕΨΗ ΤΗΣ ΑΞΙΑ ΤΗΣ ∆ΙΑΦΟΡΙΚΗΣ ΠΙΕΣΗΣ ΣΤΗΝ ΠΡΟΒΛΕΨΗ ΤΗΣ
ΚΑΡ∆ΙΑΚΗΣ ∆ΥΣΛΕΙΤΟΥΡΓΙΑΣ
• Pulse Pressure
Systolic BP� Diastolic BP
• Proportional Blood Pressure
• Systolic BP – Diastolic BP = ≤ 25%• Systolic BP – Diastolic BP = ≤ 25%
Systolic BP
= CI ≤ 2.2 = CI ≤ 2.2
L/min/M2
(JAMA 1989;261:884)(JAMA 1989;261:884)

Rapid Assessment of Hemodynamic Status
LowNO
Warm & Dry
Warm & Wet
Low
Perfusion
at Rest
O & Dry
Cold & Cold &
67%
YES
Cold & Wet
Cold & Dry
28%5%
NO YES
S28%5%
Congestion at Rest
Nohria,J Cardiac Failure 2000;6:64

Clinical assessment identifies hemodynamic profiles that predict
outcomes in patients admitted with HFoutcomes in patients admitted with HF
Nohria et al. JACC 2003;41:1797$1804

ΕΙΝΑΙ ΧΡΗΣΙΜΟΣ Ο ∆ΕΞΙΟΣ ΚΑΘΕΤΗΡΙΑΣΜΟΣ;
NO
(Stevenson, et al. JAMA 2005;294:1625(Stevenson, et al. JAMA 2005;294:1625��1633)1633)

ESC Ο∆ΗΓΙΕΣ ΓΙΑ ΤΗ ΧΡΗΣΗ ΤΟΥ ΚΑΘΕΤΗΡΑ
ΜΕΤΡΗΣΗΣ ΠΙΕΣΕ�Ν ΠΝΕΥΜΟΝΙΚΗΣ ΑΡΤΗΡΙΑΣ
• Usually unnecessary for diagnosis
• Distinguish between a cardiogenic and non,cardiogenic • Distinguish between a cardiogenic and non,cardiogenic
mechanism in complex patients with concurrent cardiac and
pulmonary disease
• In hemodynamically unstable patients not responding to • In hemodynamically unstable patients not responding to
traditional treatment,
• In patients with combination of congestion and hypoperfusion
• Level IIa, LoE C
ESC Guidelines. EHJ 2008.

∆ΙΑΓΝ�ΣΗ ΟΞΕΙΑΣ ΚΑ ΣΕ ΑΣΘΕΝΕΙΣ ΜΕ ∆ΥΣΠΝΟΙΑ
ΒΑΣΙΣΜΕΝΗ ΣΤΑ ΕΠΙΠΕ∆Α Τ�Ν ΝΑΤΡΙΟΥΡΗΤΙΚ�Ν
ΠΕΠΤΙ∆Ι�ΝΠΕΠΤΙ∆Ι�Ν
Clinical examination,
ECG, Chest X&rayECG, Chest X&ray
Natriuretic peptidesNatriuretic peptides
BNP 100&400 pg/ml
NT&proBNP
BNP <100 pg/ml
NT&proBNP
BNP >400 pg/ml
NT&proBNPNT&proBNP
400&2000 pg/ml
NT&proBNP
<400 pg/ml
NT&proBNP
>2000 pg/ml
Uncertain diagnosisChronic HF unlikely Chronic HF likelyUncertain diagnosisChronic HF unlikely Chronic HF likely
ESC Guidelines. EHJ 2008.

ΕΚΤΙΜΗΣΗ ΝΑΤΡΙΟΥΡΗΤΙΚ�Ν ΠΕΠΤΙ∆Ι�Ν ΣΤΑ
∆ΙΑΦΟΡΕΤΙΚΑ ΚΛΙΝΙΚΑ ΣΕΝΑΡΙΑ ΤΗΣ ΟΞΕΙΑΣ ΚΑ
No congestion Congestion
Warm and dry Warm and wet
>600 pg/ml for BNP
>6000 pg/ml for NT*proBNP
>600 pg/ml for BNP
>6000 pg/ml for NT*proBNP Adequate perfusion at rest
Warm and dry
BNP 100�400
Warm and wet
BNP ≥600
Cool and dry Cool and wet
>6000 pg/ml for NT*proBNP >6000 pg/ml for NT*proBNP
Low perfusion at restCool and dry
BNP 400�1000
Cool and wet
BNP ≥1000ΥΨΗΛΕΣ ΤΕΛΟ∆ΙΑΣΤΟΛΙΚΕΣ ΠΙΕΣΕΙΣ ΑΡ ΚΟΙΛΙΑΣΥΨΗΛΕΣ ΤΕΛΟ∆ΙΑΣΤΟΛΙΚΕΣ ΠΙΕΣΕΙΣ ΑΡ ΚΟΙΛΙΑΣ
Omland T. Crit Care Med 2008;36:S17.

BACH TRIAL
2.8
AHFMR�proANP adds
additional information on AHF
MR
pro
AN
P
2.4
2.6
AHF
Arrhythmia ACS
additional information on
standard of care in the
diagnosis of acute
AHF
proANP
10 M
Rp
roA
NP
2.0
2.2Pneumonia
OtherCOPD
Pulm. Emb.
Arrhythmia ACS diagnosis of acute
congestive heart failure.
The use of MR�proANP
pneumonia
MR�proANP
Log
10
1.8
Chest Pain
Bronchitis
Influenza
The use of MR�proANP
together with PCT
supports the differential
diagnosis of pneumonia
Log10MR
1.4 1.2 1.0 0.8 0.6 0.4
1.4
1.6Asthma diagnosis of pneumonia
and congestive heart
failure.Log10 PCT
failure.Log10PCT

Future diagnostic algorithm
Patient suspected to have LVDPatient suspected to have LVDPatient suspected to have LVDPatient suspected to have LVD
LVD LVD BNPBNPNormal Normal
LVD LVD
unlikelyunlikely
IncreasedIncreased
Grey Zone Grey Zone
Low MRLow MR"" IncreasedIncreasedLow MRLow MR""
proANP proANP
LVD LVD
High MRHigh MR""
proANPproANP
EchocardiogramEchocardiogramLVD LVD
unlikelyunlikely

ΣΗΜΑΝΤΙΚΟΤΕΡΟΙ ΠΡΟΓΝ�ΣΤΙΚΟΙ
∆ΕΙΚΤΕΣ ΣΤΗΝ ΟΞΕΙΑ ΚΑ∆ΕΙΚΤΕΣ ΣΤΗΝ ΟΞΕΙΑ ΚΑ
• Advanced age
• Low blood pressure
• Low LVEF
• Low sodium and • Low sodium and
• High urea and creatinine serum levels
• High Troponin • High Troponin
• High levels of natriuretic peptides
are adverse prognostic factors in AHF. are adverse prognostic factors in AHF.

EVIDENCE EVIDENCE
BASED BASED
MEDICINEMEDICINE

Typical patient in HF trials
Young ~ 65 years old
Typical patient in HF trials
Young ~ 65 years old
70�80% men70�80% men
With Systolic dysfunction
w/o comorbiditiesw/o comorbidities

• Woman 75 years old
• Obese
• Hypertensive
• Diabetic
• Creatinine 2.1 mg/dl
• Chronic atrial fibrillation
• Mild COPD
• EF 40'45%

EMOTION EMOTION
BASED BASED
MEDICINEMEDICINE

Therapeutic targets in AHF syndromes
Goals of Treatment in AHF
Immediate (ED/ICU/CCU)
Improve symptoms
Restore oxygenation
Improve organ perfusion and haemodynamics
Limit cardiac/renal damage
Minimize ICU length of stay
Intermediate (in hospital)
Stabilize patient and optimize treatment strategy
Initiate appropriate (life%saving) pharmacological therapyInitiate appropriate (life%saving) pharmacological therapy
Consider device therapy in appropriate patients
Minimize hospital length of stay
Long�term and predischarge management
Plan follow%up strategy
Educate and initiate appropriate lifestyle adjustments
Provide adequate secondary prophylaxis
Prevent early readmission
Improve quality of life and survival
ESC Guidelines 2008.
Improve quality of life and survival

Goals for Treatment of Acutely Decompensated Heart Failure
ClinicalHemodynamic
SBP > 80 mm Hg
No orthopnea
SBP > 80 mm Hg
PCWP < 15 mm Hg
ClinicalHemodynamic
No orthopnea
No peripheral edema
No hepatomegaly/ascites
JVP < 8 cm
PCWP < 15 mm Hg
RAP < 8 mm Hg
SVR < 1200 dyne%s%cm%5
JVP < 8 cm
Warm extremities
JVP = jugular venous pressure.

Management of pulmonary congestion
A) Hypertensive HF
• Vasodilators are recommended with close monitoring and • Vasodilators are recommended with close monitoring and
low�dose diuretic treatment in patients with volume overload
or pulmonary oedema
B) Pulmonary oedemaB) Pulmonary oedema
• NIV
• Vasodilators are recommended when BP is normal or high, • Vasodilators are recommended when BP is normal or high,
and diuretics in patients with volume overload or fluid
retention
• Morphine is usually indicated, especially when dyspnoea is • Morphine is usually indicated, especially when dyspnoea is
accompanied by pain and anxiety
• Intubation and mechanical ventilation may be required to
ESC Guidelines 2008.
achieve adequate oxygenation

Vasodilators or Diuretics Driven Treatment
in Acute Hypetensive HFin Acute Hypetensive HF
• 110 AHF pts, O2 10 l/min, Morphine 3mg
• Group A: Furosemide 40mg �ISDN 3mg iv every 3min
• Group B: Furosemide 80mg every 15min, ISDN 1mg/h,+1mg every 15min, ISDN 1mg/h,+1mg every 10min
• Treated until SpO2 >96% or MAP�30% or MAP <90 mmHg
• Results: • Results:
• Mechanical ventilation needed in 13/40%
• AMI 17/37%• AMI 17/37%
• Mortality 1/3
• Composite primary end point 25%/46%end point 25%/46%
Cotter et al, Lancet 1998

Indications and dosing of vasodilators
Vasodilator Indication Dosing Main side effects Other
Glyceryl
trinitrate,
Acute heart
failure, when
Start 20 �g/min,
increase to
Hypotension,
headache
Tolerance on
continuous trinitrate,
5"
mononitrate
failure, when
blood pressure is
adequate
increase to
200 �g/min
headache continuous
use
Isosorbide
dinitrate
Acute heart
failure, when
Start with
1 mg/h, increase
Hypotension,
headache
Tolerance on
continuous ESC recommendation class I, Level of evidence B dinitrate failure, when
blood pressure is
adequate
1 mg/h, increase
to 10 mg/h
headache continuous
use
Nitroprusside Hypertensive
crisis, cardiogenic
0.3"5 �g/kg/min Hypotension,
isocyanate toxicity
Drug is light
sensitive
ESC recommendation class I, Level of evidence B
crisis, cardiogenic
shock combined
with intoropes
isocyanate toxicity sensitive
Nesiritidea Acute
decompensated
heart failure
Bolus 2 �g/kg |
infusion 0.015"
0.03 �g/kg/min
Hypotension
heart failure 0.03 �g/kg/min
ESC Guidelines on AHF 2008.
a Limited sales approval in ESC countries.

Non�invasive ventilation
Indications
• Non�invasive ventilation (NIV) refers to all modalities that• Non�invasive ventilation (NIV) refers to all modalities that
assist ventilation without the use of an endotracheal tube but
rather with a sealed face�mask
• NIV with positive endexpiratory pressure (PEEP) should be • NIV with positive endexpiratory pressure (PEEP) should be
considered as early as possible in every patient with acute
cardiogenic pulmonary oedema and hypertensive AHF as it
improves clinical parameters including respiratory distressimproves clinical parameters including respiratory distress
• Class of recommendation IIa, level of evidence B

CPAP: Beneficial effects on mortality
Meta�analysis Meta�analysis
of 12 studies
Total 160�240 /groupTotal 160�240 /group
Mortality reducedMortality reduced
from 22% to 11%
RR 0.53 RR 0.53
(95% CI 0.35�0.81)
Masip et al. JAMA 2005;294:3124�3130

3CPO Multicenter Trial: Primary end�point
Cumulative
Survival
1.0
0.9 Non�invasive
Standard
Oxygen Therapy
Ventilation
0.8
Oxygen TherapyP=0.685
0 10 20 30Days

Non�Invasive Ventilation in ACPE
Masip J, Mebazaa A, Filippatos G. N Engl J Med 2008

Inotropes in clinical practice
• Inotropic agents should be considered in patients with low• Inotropic agents should be considered in patients with low
output states, in the presence of signs of hypoperfusion or
congestion despite the use of vasodilators and/or diuretics to
improve symptomsimprove symptoms
• Class of recommendation IIa, level of evidence B

Available inotropic agents
Dobutamine: cl IIa, Level evidence BDobutamine: cl IIa, Level evidence B
PDEIs: cl IIb, Level evidence B
Dopamine: cl IIb, Level evidence C
PDEIs: cl IIb, Level evidence B
Dopamine: cl IIb, Level evidence C
Levosimendan: cl IIa,Level evidence B Levosimendan: cl IIa,Level evidence B
ESC Guidelines 2008.

Hazard Ratios for Patients With a History of CHF
Appeared to Favor Levosimendan
Day, Group
Interaction
p�value
Favors
Levosimendan
Favors
Dobutamine
5 Previous history of CHFNo previous history of CHF
14 Previous history of CHFNo previous history of CHF
0.053
No previous history of CHF
31 Previous history of CHFNo previous history of CHF 0.046
90 Previous history of CHFNo previous history of CHF
180 Previous history of CHFNo previous history of CHF
0,1 1 10
No previous history of CHF
0.5 2
88% had history of CHFHazard Ratio (95% CI)
88% had history of CHF
12% had no previous history of CHF
European Journal of Heart Failure Advance Access published January 21, 2009.
Hazard Ratio (95% CI)

Hazard Ratios for Patients on β�Blockers at Baseline
Appeared to Favor Levosimendan
Favors
LevosimendanDay, Group
Favors
Dobutamine
Interaction
p�value
5 β�blocker users*β�blocker non�users
14 β�blocker users*β�blocker non�users
p�value = 0.01 0.014
β�blocker non�users
31 β�blocker users*β�blocker non�users
90 β�blocker users*β�blocker non�users
180 β�blocker users*β�blocker non�users
0 0,5 1 1,5 2
Hazard ratio (95% CI)
β�blocker non�users
Hazard ratio (95% CI)
* Within 24 hours of study drug infusion.
European Journal of Heart Failure Advance Access published January 21, 2009.

SURVIVE: Mean Change from Baseline in BNP
0
�300
�200
�100
0
Mean c
hange f
rom
baselin
e
�500
�400
�300
Dobutamine
Levosimendan
Mean c
hange f
rom
baselin
e
�800
�700
�600
�500
Mean c
hange f
rom
baselin
e
�800
0 1 2 3 4 5 6
Days since start of study drug infusion
For comparison between treatment groups at all time points (P<0.0001).
Due to the skewness in the data, median percent change is presented versus mean percent change from baseline.

Levosimendan, Compared to Dobutamine, Reduces Enzymatic
Markers Associated with Liver Congestion And Right Heart Failure: Markers Associated with Liver Congestion And Right Heart Failure:
A SURVIVE Subanalysis
5
10
Dif
fere
nce
(L
ev
os
ime
nd
an
–
Do
bu
tam
ine
) in
Ch
an
ge
Fa
vo
rsDo
bu
tam
ine
80 75 111Baseline, ", IU/L
0.008 0.002 <0.001P)value*
80 75 11180 75 111Baseline, ", IU/L
0.008 0.002 <0.001P)value*
)10
)5
0
5
Dif
fere
nce
(L
ev
os
ime
nd
an
Do
bu
tam
ine
) in
Ch
an
ge
Fro
m B
as
eli
ne
, IU
/L† AST APALT
Fa
vo
rsDo
bu
tam
ine
Le
vo
sim
en
dan
)30
)25
)20
)15
Dif
fere
nce
(L
ev
os
ime
nd
an
Do
bu
tam
ine
) in
Ch
an
ge
Fro
m B
as
eli
ne
, IU
/L
Day 1 Day 3 Day 5Day 1 Day 3 Day 5
Le
vo
sim
en
dan
)35
)30
Dif
fere
nce
(L
ev
os
ime
nd
an
Do
bu
tam
ine
) in
Ch
an
ge
Day 1 Day 3 Day 5Day 1 Day 3 Day 5
*P)value from repeated measures ANCOVA model for treatment effect, model also included
effects for time (all were p<0.05) and treatment)by)time interaction (all were p=NS). †Point
estimates from ANCOVA model with baseline as covariate. Error bars are standard errors.
Nikolaou M, Parissis J, Mebazza A, presented at ESC congress Paris France 2011.

Istaroxime: a Na/K�ATPase inhibitor with positive
lusitropic properties
Sabbah et al. Am J Cardiol 2007;99:41A
Adamson et al. J Cardiovasc Pharmacol 2003;42:169

Changes in hemodynamic and other measures in the
HORIZON�HF trial, three dosages of IV istaroxime vs
placeboplacebo�g/kg/min
Parameter 0.5, n=29
1.0, n=30
1.5, n=30 Placebo, n=31 n=29 n=30 n=31
PCWPa (mm Hg) 3.2b 3.3c 4.7d 0.0
Systolic BP (mm Hg) +4.9 +8.3b +15.6d +1.3Systolic BP (mm Hg) +4.9 +8.3 +15.6 +1.3
MAP (mm Hg) +2.2 +3.3 +7.5c +0.9
LVEDV (mL) +2.9 6.4 14.1b +3.9
QTc (ms) 25.7e 38.0e 49.2e 2.4QTc (ms) 25.7e 38.0e 49.2e 2.4
a. Primary end pointb. p<0.05b. p<0.05c. p<0.01 d. p<0.001e. p=0.0001PCWP=pulmonary capillary wedge pressureMAP=mean arterial pressure
Gheorghiade M et al. J Am Coll Cardiol 2008; 51:2276�2285.
MAP=mean arterial pressureLVEDV=left ventricular end%diastolic volume; QTc=corrected QT interval

Relaxin Mechanisms of ActionRelaxin Mechanisms of Action
• Vasodilation
• NO, cGMP effectorsRelaxin • NO, cGMP effectors
• Induction of NOS II/III
• Upregulation of endothelial endothelin type B receptor, which mediates
Relaxin
type B receptor, which mediates vasodilation
• Preferential dilation of constricted vessels
• Relaxin%upregulated ETB receptors act as vasodilating ET%1 sink
• Anti�inflammatory• Anti�inflammatory
• Down%modulation of inflammatory cytokines linked to outcome in HF (TNF%α, TGF%β)
• Other: Anti�ischemic, Anti�apoptotic, Anti�fibrotic
Teichman, SL, et al. Heart Fail Rev 2009; Dschietzig, T, et al. Pharmacol Therap 2006

Rapid Dyspnea Improvement through 24 hours
(Likert Scale)(Likert Scale)
Proportion of Patients with Moderate/Marked
Improvement in Dyspnea at 6, 12 and 24 hrImprovement in Dyspnea at 6, 12 and 24 hr
40
45
50 p = 0.04
25
30
35
Pa
tie
nts
(%
)
10
15
20
25
Pa
tie
nts
(%
)
Placebo 10 30 100 2500
5
10
Relaxin (mcg/kg/d)
J Teerlink RELAX�AHF ACC 2009

ΧΕΙΡΙΣΜΟΣ ΤΝ ΑΣΘΕΝΝ ΜΕ ΟΞΕΙΑ ΚΑ ΠΟΥ
ΘΕΡΑΠΕΥΟΝΤΑΙ ΜΕ ΑΜΕΑ Η ΑΝΤ ΥΠΟ∆ΟΧΕΝ ΘΕΡΑΠΕΥΟΝΤΑΙ ΜΕ ΑΜΕΑ Η ΑΝΤ ΥΠΟ∆ΟΧΕΝ
ΑΓΓΕΙΟΤΕΝΣΙΝΗΣ
• ACEIs are not indicated in the early stabilization of patients
with AHF
• There is no consensus on the ideal timing for initiation of • There is no consensus on the ideal timing for initiation of
ACEI/ARB therapy in AHF. In general, it is recommended that
treatment with these agents should be initiated before
discharge from hospitaldischarge from hospital
• Patients on ACEIs/ARBs admitted with worsening HF should
be continued on this treatment whenever possible
• Class of recommendation I, level of evidence A

Use of betablockers during acute exacerbation of HF
• The dose of βblocker may need to be reduced temporarily
or omitted, although generally treatment should not be
stopped, unless the patient is clinically unstable with signs stopped, unless the patient is clinically unstable with signs
of low output
• Treatment may be interrupted or reduced in the presence of• Treatment may be interrupted or reduced in the presence of
complications (bradycardia, advanced AV block,
bronchospasm, or cardiogenic shock) or in cases of severe
AHF and an inadequate response to initial therapy
• Class of recommendation IIa, level of evidence B
ESC Guidelines 2008.

ΕΠΙ∆ΡΑΣΗ ΤΗΣ ΣΥΝΕΧΙΣΗΣ Η ΑΠΟΣΥΡΣΗΣ ΤΟΥ Β�
ΑΝΑΣΤΟΛΕΑ ΣΤΗ ΕΠΙΒΙ�ΣΗ ΤΗΣ ΟΞΕΙΑΣ ΚΑ
Findings from the OPTIMIZE�HF Program
Fonarow, et al. JACC 2008;52:190.
Post�discharge survival by beta�blocker treatment groups

Degree of Renal Damage in Patients Admitted for Decompensated HF
50
35
40
45
50
Males
20
25
30
35Males
Females
5
10
15
20
0
5
Nml GFR Moderate Renal
Failure
Mild SevereKidney
Damage100,000
Admissions>90 60$89eGFR 30$59 15$29 >15
Admissions
ADHERE

What is the evidence for ‘renal impairment’ in the ALARM�HF
patient population?patient population?
Renal status in all AHF patients vs ADCHF vs De Novo
43%50%
20%25%
10%
37%43%
27%
15% 16% 14%20%
30%
40%
50%
10%15% 14%
0%
10%
20%
History of CRDHistory of CRD
Initial serum creatinine >1.5mg/dL
Renal failure complicationRenal failure complication
Sample = All AHF patients (4,953) vs ADCHF (3,161) vs De Novo AHF patients (1,792)
J Parissis on behalf of Steering Committee

“HOT” POINTS INDICATE A RISK FOR
ACUTE RENAL FAILURE IN CHFACUTE RENAL FAILURE IN CHF
• Persistently low urinary sodium
• Concomitant increase of hepatic enzymes and BUN (Risk of hepatonephric syndrome) (Risk of hepatonephric syndrome)
• Increased plasma urea/creatinine ratio and uric acid (discontinuation of ACEi?)
• Mean arterial pressure <80 mmHg
• Hyponatremia (max neurohormonal activation)
• Changes in effective circulating volume (fever, blood • Changes in effective circulating volume (fever, blood loss, decrease in dietary salt, etc.)
• Other: angiogaphic contrast, older age, diabetes, major surgery, use of NSADs surgery, use of NSADs

Optimizing treatment of renal dysfunction according
to BUN/CRE Ratio
CO BUN/CRE
to BUN/CRE Ratio
CO BUN/CRE
VasodilatorsCorrect volume
Stop ACEi
Vasodilators
Inotropes
hemofiltration
DRY WET
PCWP Wt (kg)
DRY WET
PCWP Wt (kg)

Cardiorenal syndromeCardiorenal syndrome�� Overcoming the resistance Overcoming the resistance
to diureticsto diureticsto diureticsto diuretics
1.1. Increase furosemide dose Increase furosemide dose 1.1. Increase furosemide dose Increase furosemide dose
2.2. Stop ACEiStop ACEi
3.3. Use continuous iv furosemideUse continuous iv furosemide
4.4. Add metolazoneAdd metolazone4.4. Add metolazoneAdd metolazone
5.5. Add dopamine at 2Add dopamine at 2��3 mcg/kg3 mcg/kg
6.6. Add vasodilators or inotropes according to SBPAdd vasodilators or inotropes according to SBP6.6. Add vasodilators or inotropes according to SBPAdd vasodilators or inotropes according to SBP
7.7. Start ultrafiltrationStart ultrafiltration
8.8. Insert IABPInsert IABP
9.9. Insert another deviceInsert another device9.9. Insert another deviceInsert another device

The role of CVP in renal worsening in ADHF patients
Mullens, et al. J Am Coll Cardiol 2009;53:589�96.

Ultrafiltration (UF) Versus Usual Care (UC)
for Patients with AHF: RAPID�CHF Trialfor Patients with AHF: RAPID�CHF Trial
• The early application • The early application
of UF for patients with
CHF was feasible, well�
tolerated, and resultedtolerated, and resulted
in significant weight loss
and fluid removal
• A larger trial is underway
UF UC
• A larger trial is underway
to determine the relative
efficacy of UF versus
standard care in ADHF
p=0.001
p=0.01
n=40n=40
Bart et al. JACC 2005;46:2043

UNLOAD: Freedom From Rehospitalization UNLOAD: Freedom From Rehospitalization
for HF
100 �
Pe
rce
nta
ge o
f P
ati
en
ts
Fre
e F
rom
Re
ho
sp
ita
lizati
on Ultrafiltration Arm (16 Events)
80 �
60 �
40 �
Pe
rce
nta
ge o
f P
ati
en
ts
Fre
e F
rom
Re
ho
sp
ita
lizati
on
Standard Care Arm (28 Events)
40 �
20 �
10 20 30 40 50 60 70 80 90
Pe
rce
nta
ge o
f P
ati
en
ts
Fre
e F
rom
Re
ho
sp
ita
lizati
on
P=.037
0 10 20 30 40 50 60 70 80 90
Days
No. Patients at Risk
Ultrafiltration Arm 88 85 80 77 75 72 70 66 64 45
0
Standard Care Arm 86 83 77 74 66 63 59 58 52 41
Costanzo MR et al. J Am Coll Cardiol. 2007;49:675�683.

Peripheral Ultrafiltration
• Ultrafiltration should be considered to reduce fluid overload
(pulmonary and/or peripheral oedema) in selected patients
and correct hyponatraemia in symptomatic patients
refractory to diuretics.
• Class of recommendation IIa, level of evidence B• Class of recommendation IIa, level of evidence B
Key evidence
• Although earlier studies suggested only temporary benefit,• Although earlier studies suggested only temporary benefit,
more recent trials have demonstrated sustained effects.
The most appropriate selection criteria have not been
established. However, technological advances facilitate established. However, technological advances facilitate
ultrafiltration and will probably increase experience in this
population.

Therapeutic Algorithm (I)
Hypertensive AHF (SBP>140 mmHg)
• A) Restoration of low oxygen saturation (>95% in patients without COPD • A) Restoration of low oxygen saturation (>95% in patients without COPD or >90% in patients with COPD ) using oxygen supply or CPAP/BiPAP or mechanical ventilation.
• B) Alleviation of patient anxiety and pain using iv analgesics (e.g. morphine).
• C) Improvement of pulmonary congestion using high doses of iv vasodilators and low doses of iv diuretics.
• D) Restoration of sinus rhythm or achievement of a satisfactory heart rate control in the co-existence of atrial fibrillation (or other supra-ventricular tachycardias) using electroversion or anti-arrhythmics (e.g. digoxin, tachycardias) using electroversion or anti-arrhythmics (e.g. digoxin, amiodarone).
Filippatos, Parissis. Acute Heart Failure. OXFORD Handbook 2010

Treatment algorithm (II)
Normotensive AHF (140>SBP>90 mmHg)
• A) Improvement of fluid overload using high doses of iv diuretics (consider combination of different classes of diuretics in resistant (consider combination of different classes of diuretics in resistant cases)
• B) Reduction of elevated cardiac filling pressures and afteload (if • B) Reduction of elevated cardiac filling pressures and afteload (if SBP>100 mmHg) using low doses of iv vasodilators (e.g. nitrates) with a parallel close monitoring of SBP.
• C) Improvement of peripheral organ hypoperfusion using iv inotropes (e.g. levosimendan, dobutamine) in cases resistant to the above therapies or as initial approach in the cases with low output symptoms and 120>SBP>90 mmHg.symptoms and 120>SBP>90 mmHg.
• D) Mechanical improvement of fluid status using devices of peripheral hemofiltration in patients with worsening of renal function under the recommended iv medications.recommended iv medications.
Filippatos, Parissis. Acute Heart Failure. OXFORD Handbook 2010

Treatment Algorithm (III)
Hypotensive AHF (SBP <90 mmHg) *Hypotensive AHF (SBP <90 mmHg) *
• A) Evaluation of fluid status using pulmonary artery catheter (exclusion of hypovolemia).
• B) Restoration of SBP and peripheral hypoperfusion using iv vassopressors (e.g high doses of dopamine and/or dobutamine, norepinephrine).
• C) Improvement of coronary and peripheral perfusion using mechanical support (implantation of intra+aortic balloon counterpulsation or other portable devices).
• D) Improvement of oliguria/anouria using portable devices of peripheral hemofiltration in resistant cases to the above strategies.
* Revasc and IABP in ACS
Filippatos, Parissis. Acute Heart Failure. OXFORD Handbook 2010

What is hot in new ESC guidelines?
• Combination of AHF and CHF guidelines • Combination of AHF and CHF guidelines
• The role of ACS in classification
• The role of biomarkers in diagnosis (cut off values for • The role of biomarkers in diagnosis (cut off values for
rule out)
• The short and long term management
• Guidelines for the use new devices and machines• Guidelines for the use new devices and machines
• Guidelines for the background treatment of AHF
(ACEi/ARBs, beta blockers)(ACEi/ARBs, beta blockers)

What is not?
• Overlapping of 6 conditions in ESC classification (reconsider • Overlapping of 6 conditions in ESC classification (reconsider
a new one based on SBP)
• Absence of cut"off values of biomarkers according to
different clinical scenarios and their role as therapeutic different clinical scenarios and their role as therapeutic
targets – The role of multi"marker strategy ?
• No specific guidelines for the use of iv inotropes in AHF
patients with special conditions or co"morbidities (renal patients with special conditions or co"morbidities (renal
dysfunction, ACS, high BNP, on beta"blocker therapy)
• Absence of Class I therapies for AHF (in contrast to CHF)• Absence of Class I therapies for AHF (in contrast to CHF)