ΕΠΙΠΛΟΚΕΣ ΚΑΙ ΑΝΤΙΜΕΤΩΠΙΣΗ ΤΟΥΣ ΜΕΤΑ ΑΠΟ TAVR. · •TAVR...
35
ΕΠΙΠΛΟΚΕΣ ΚΑΙ ΑΝΤΙΜΕΤΩΠΙΣΗ ΤΟΥΣ ΜΕΤΑ ΑΠΟ TAVR. ΕΙΝΑΙ ΑΝΑΓΚΑΙΟ ΤΟ ΥΒΡΙΔΙΚΟ ΧΕΙΡΟΥΡΓΕΙΟ? Ματθαίος Παναγιώτου MD FETCS Διευθυντής καρδιοχειρουργικής METROPOLITAN HOSPITAL ΠΑΝΕΛΛΗΝΙΑ ΣΕΜΙΝΑΡΙΑ ΟΜΑΔΩΝ ΕΡΓΑΣΙΑΣ EKE ΘΕΣΣΑΛΟΝΙΚΗ 2017
Transcript of ΕΠΙΠΛΟΚΕΣ ΚΑΙ ΑΝΤΙΜΕΤΩΠΙΣΗ ΤΟΥΣ ΜΕΤΑ ΑΠΟ TAVR. · •TAVR...
ΕΠΙΠΛΟΚΕΣ ΚΑΙ ΑΝΤΙΜΕΤΩΠΙΣΗ ΤΟΥΣ ΜΕΤΑ ΑΠΟ TAVR.
ΕΙΝΑΙ ΑΝΑΓΚΑΙΟ ΤΟ ΥΒΡΙΔΙΚΟ ΧΕΙΡΟΥΡΓΕΙΟ?
Ματθαίος Παναγιώτου MD FETCSΔιευθυντής καρδιοχειρουργικής
METROPOLITAN HOSPITAL
ΠΑΝΕΛΛΗΝΙΑ ΣΕΜΙΝΑΡΙΑ ΟΜΑΔΩΝ ΕΡΓΑΣΙΑΣ EKE ΘΕΣΣΑΛΟΝΙΚΗ 2017
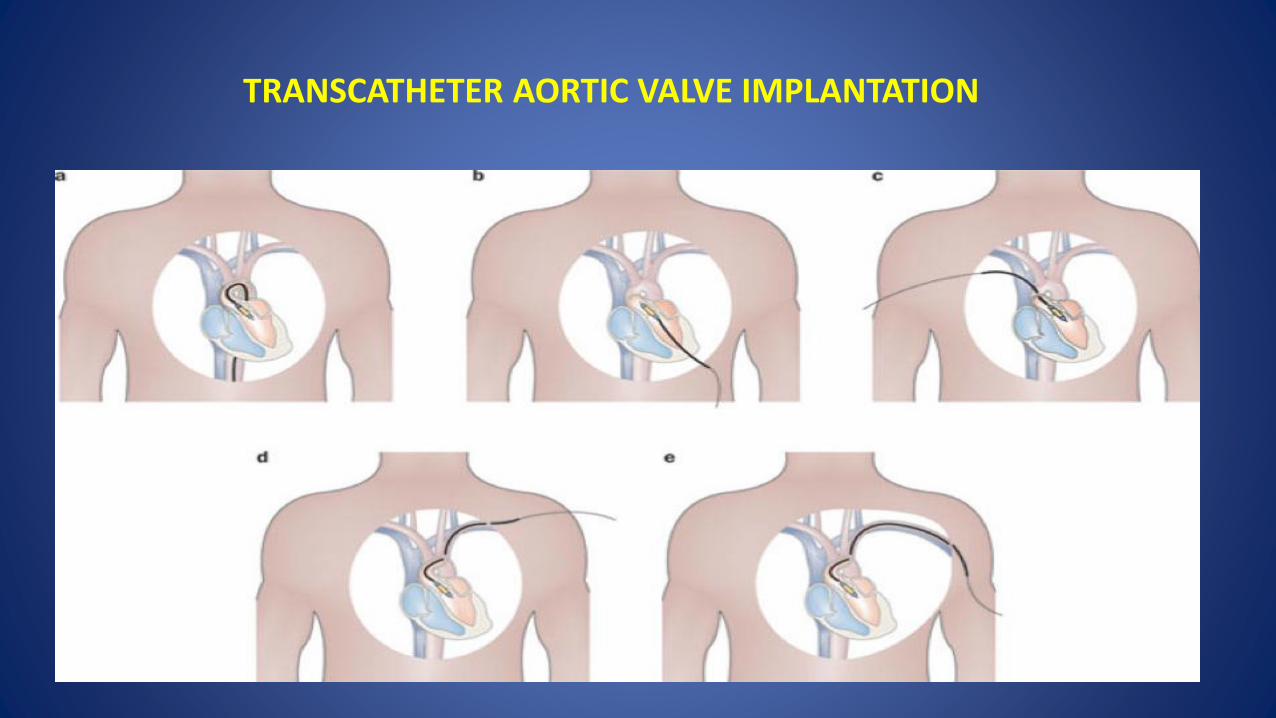
TRANSCATHETER AORTIC VALVE IMPLANTATION
• TAVR evolved from an experimental procedure to clinical routine
• This has created a strong drive to perform TAVR not only in specialized centers but also in any interventional unit.
RAISED QUESTIONS • Is TAVI similar or better than SAVR in patients at high
risk?
• Is the adoption of TAVI justified for patients at lower surgical risk?
• Do we need a surgical support?
• Is a ‘flying’ surgical team sufficient to cover complications during and after TAVR?
• Is a Hybrid theater necessary ?
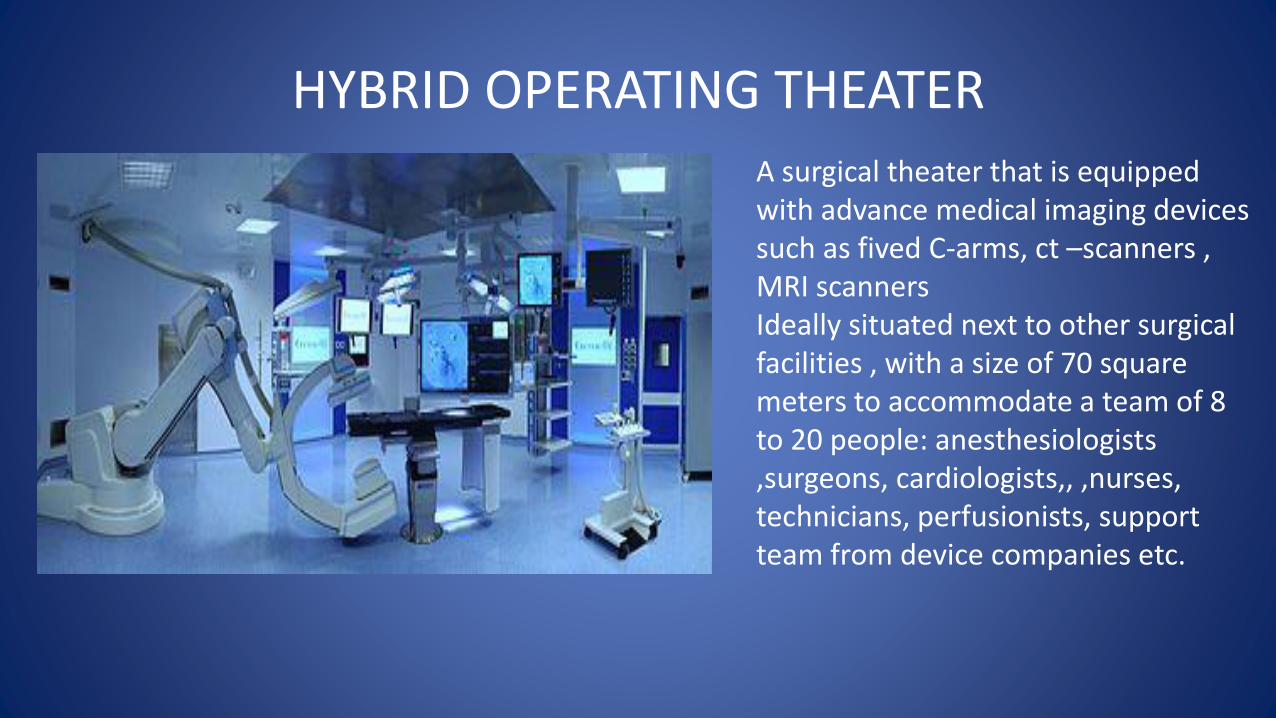
HYBRID OPERATING THEATER
A surgical theater that is equipped with advance medical imaging devices such as fived C-arms, ct –scanners , MRI scannersIdeally situated next to other surgical facilities , with a size of 70 square meters to accommodate a team of 8 to 20 people: anesthesiologists ,surgeons, cardiologists,, ,nurses, technicians, perfusionists, support team from device companies etc.

TAVR Procedural complications
• Access –site related complications • Valve embolization ( aortic, left ventricle)• Central valvular aortic regurgitation• Paravalvular aortic regurgitation• Complete heart block• Stroke (Ischemic, hemorrhagic• Coronary occlusion • Annular rupture• Ventricular perforation• Shock , hemodynamic collapse
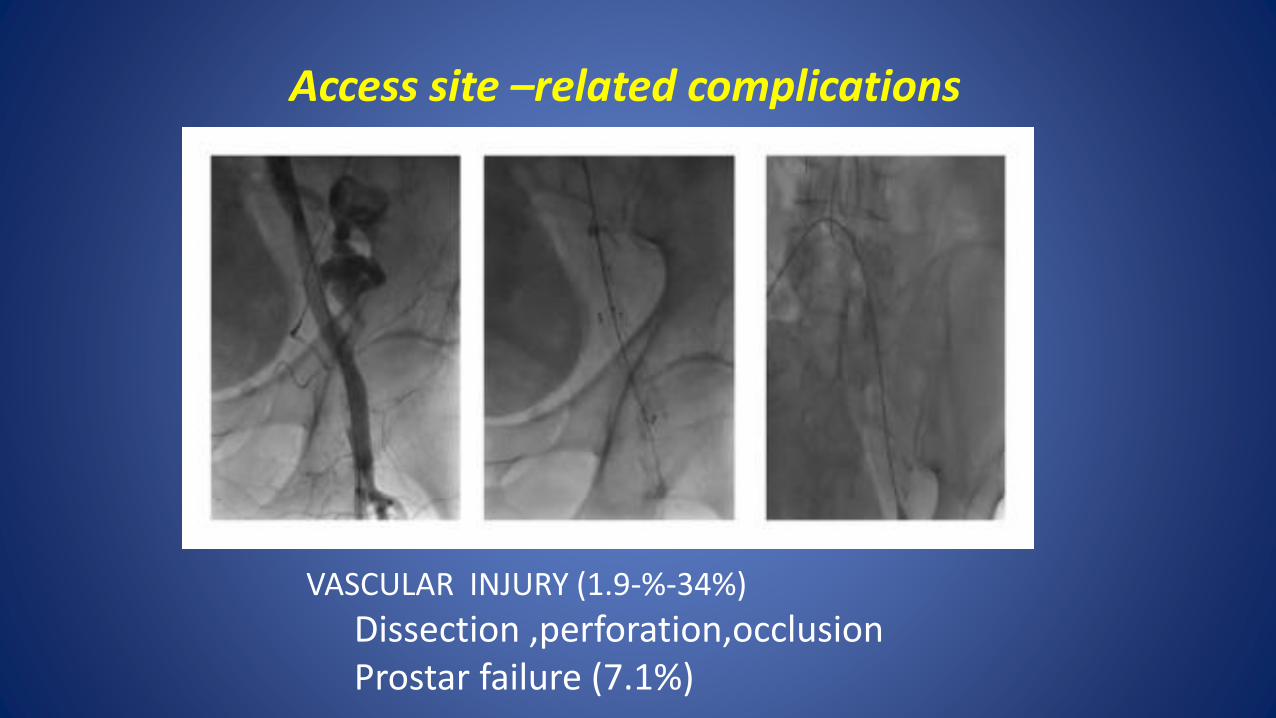
Access site –related complications
VASCULAR INJURY (1.9-%-34%)
Dissection ,perforation,occlusionProstar failure (7.1%)
CENTRAL VALVULAR AORTIC REGURGITATION
• Prosthesis underexpansion or rupture
• Malfunctioning leaflet damage during crimping or implantation
• Usually self-limited
• Gentle probing of leaflets with a soft wire or catheter
• Delivery of a second TAVR device ( valve-in-valve)
PARAVALVULAR AORTIC REGURGITATION ≥ grade 2(1-47%)
• Post-deployment balloon dilatation
• Repositioning of valve if low (recapture , snare)
• Delivery of a second TAVR device
• Percutaneous vascular closure devises(Amplatzer vascular plug)
• SAVR
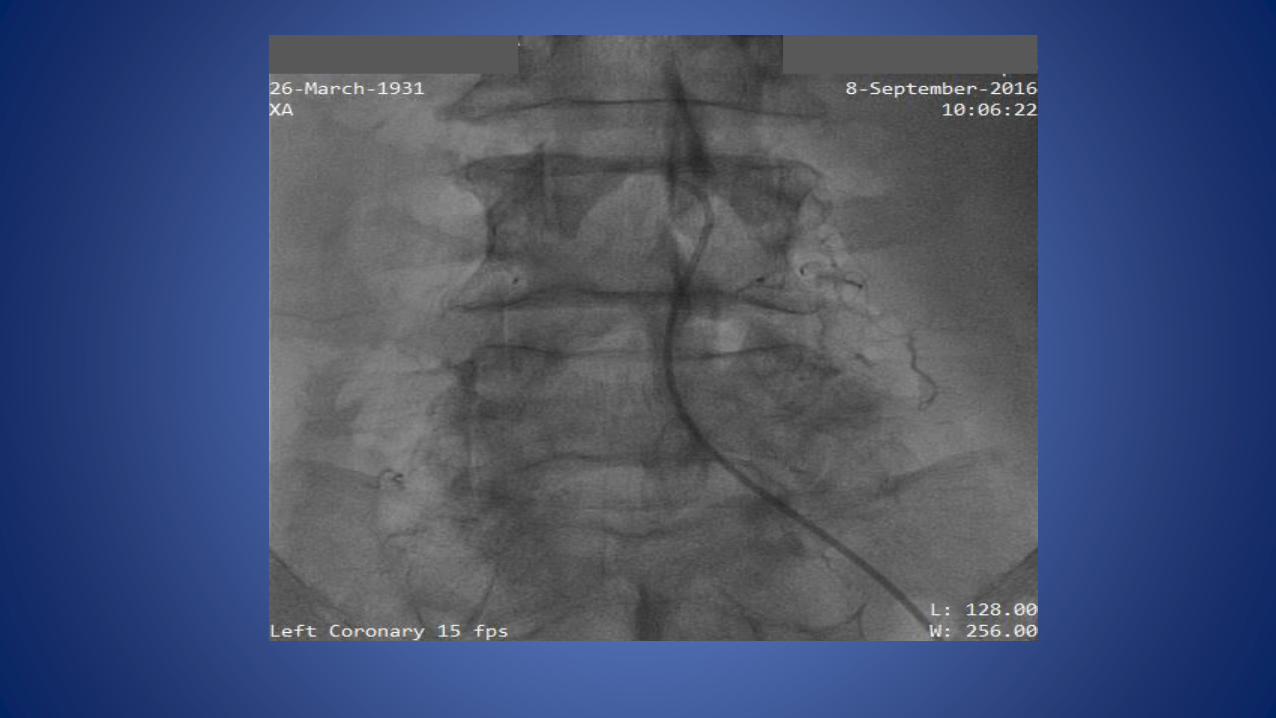
ACUTE CORONARY OCCLUSION (0.6-4.1%)
• Low –lying (≤ 10mm) coronary ostia.
• Extensive annular calcification
• Small aortic root ( sinuses of Valsalva of similar or even smaller diameter of aortic annulus)
• PCI ( easier if coronaries already wired before valve implantation)
• CABG
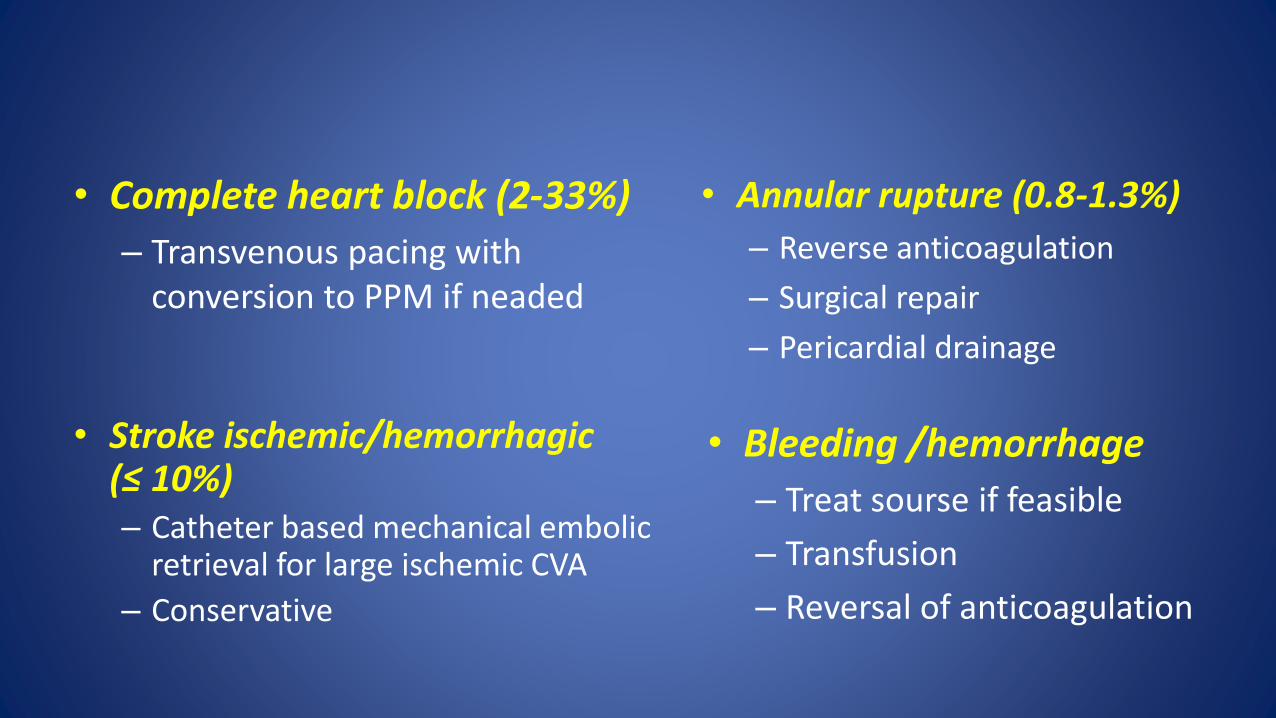
• Complete heart block (2-33%)
– Transvenous pacing with conversion to PPM if neaded
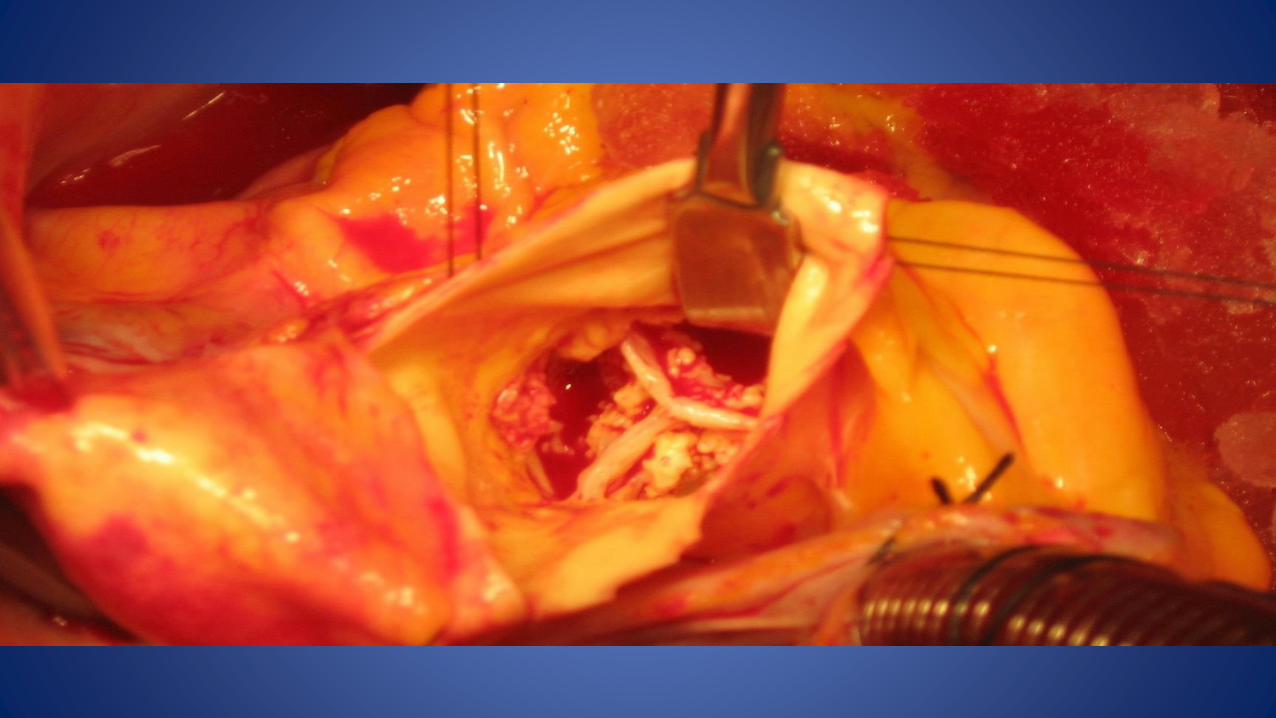
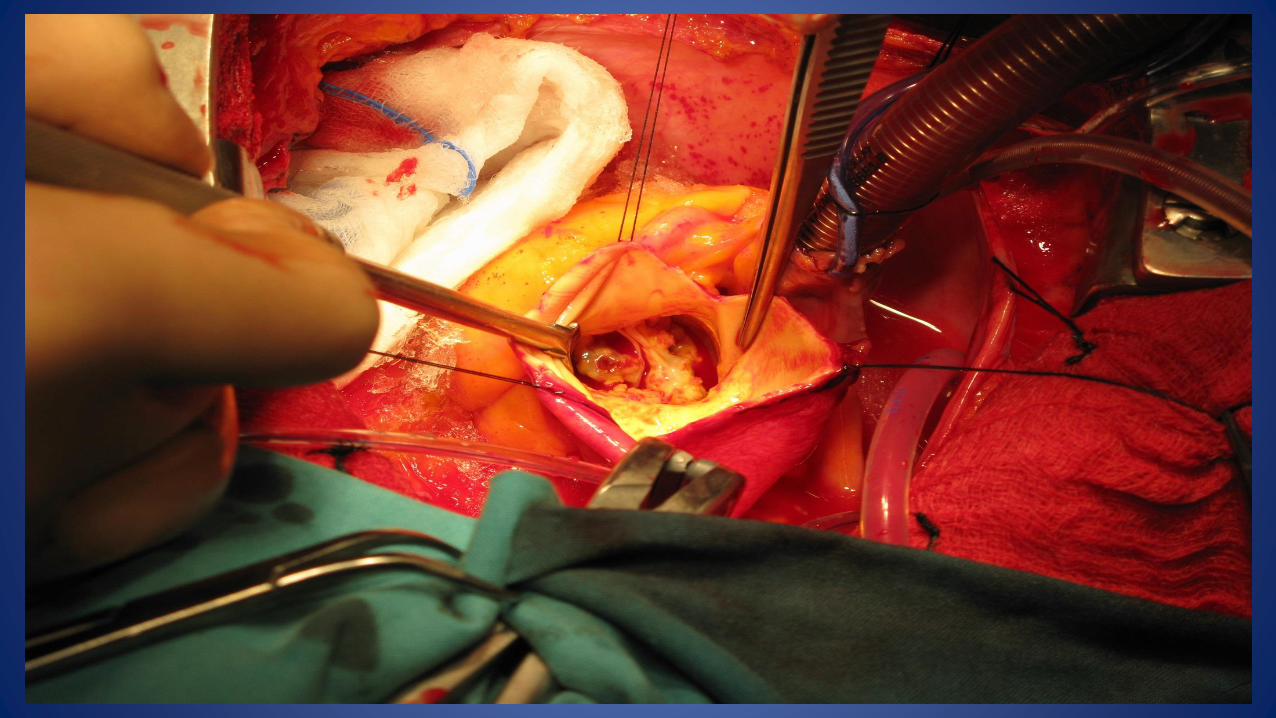
• Annular rupture (0.8-1.3%)
– Reverse anticoagulation
– Surgical repair
– Pericardial drainage
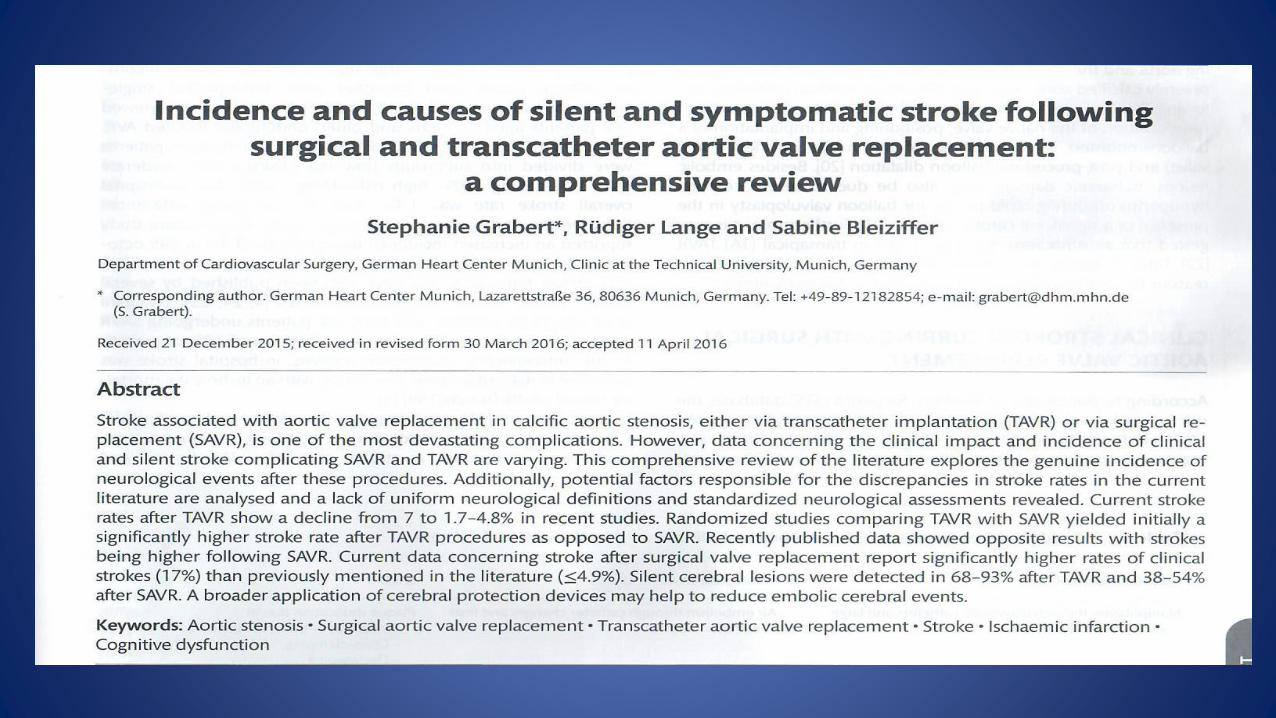
• Stroke ischemic/hemorrhagic (≤ 10%)– Catheter based mechanical embolic
retrieval for large ischemic CVA
– Conservative
• Bleeding /hemorrhage
– Treat sourse if feasible
– Transfusion
– Reversal of anticoagulation
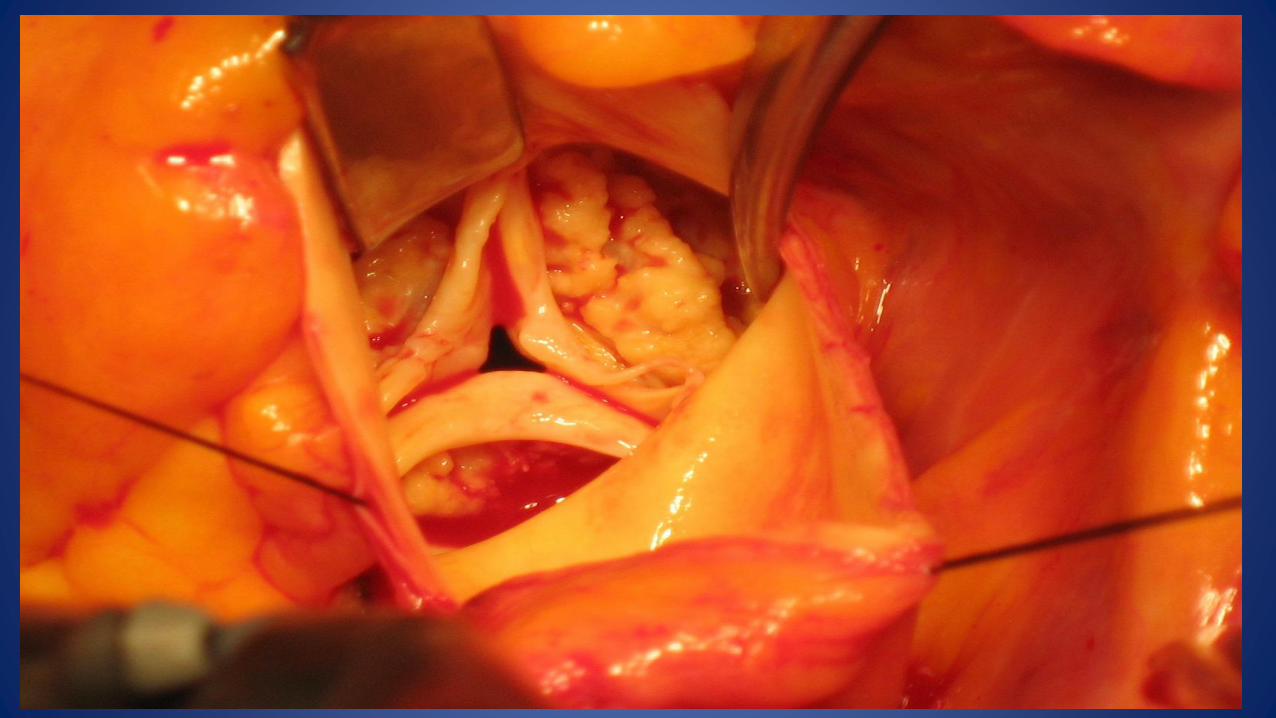
ACUTE MITRAL VALVE INJURY
• In deep implantation-impinging upon mitral curtain
• Uncommon
• Most likely with the TA-TAVI
• Some cases of gradual erosion of the anterior leaflet
VENTRICULAR PERFORATION
• Reverse anticoagulation
• Surgical repair
• Pericardial drainage
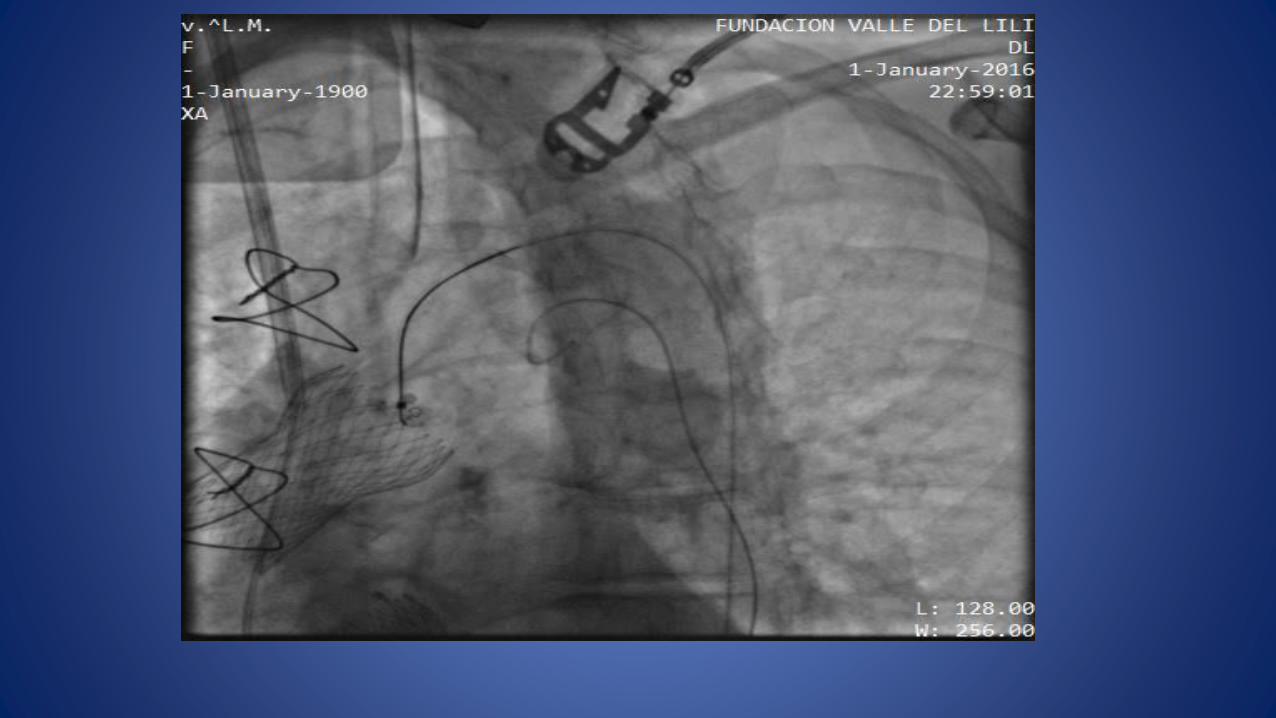
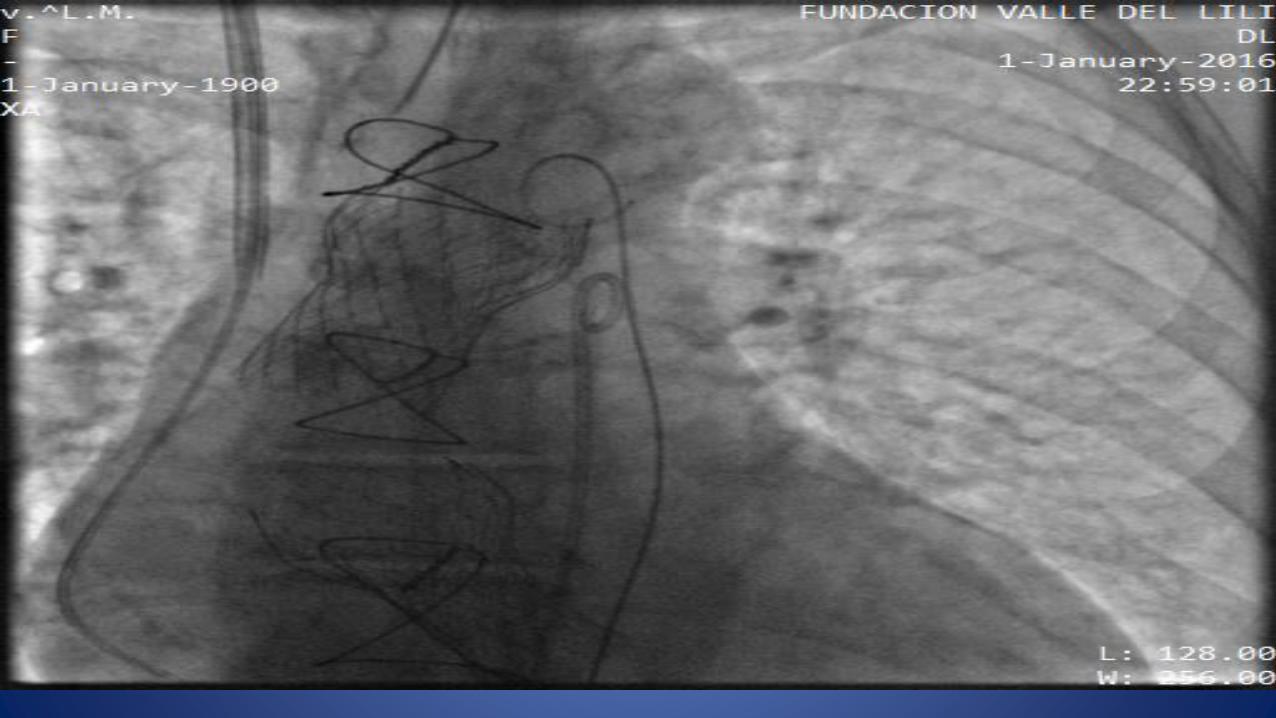
VALVE DISLOCATION EMBOLIZATION TO AORTA OR LEFT VENTRICLE (3-11%)
• Recapture or deploy in descending aorta if still attached to delivery system
• Valve in valve
• Endovascular (snare)
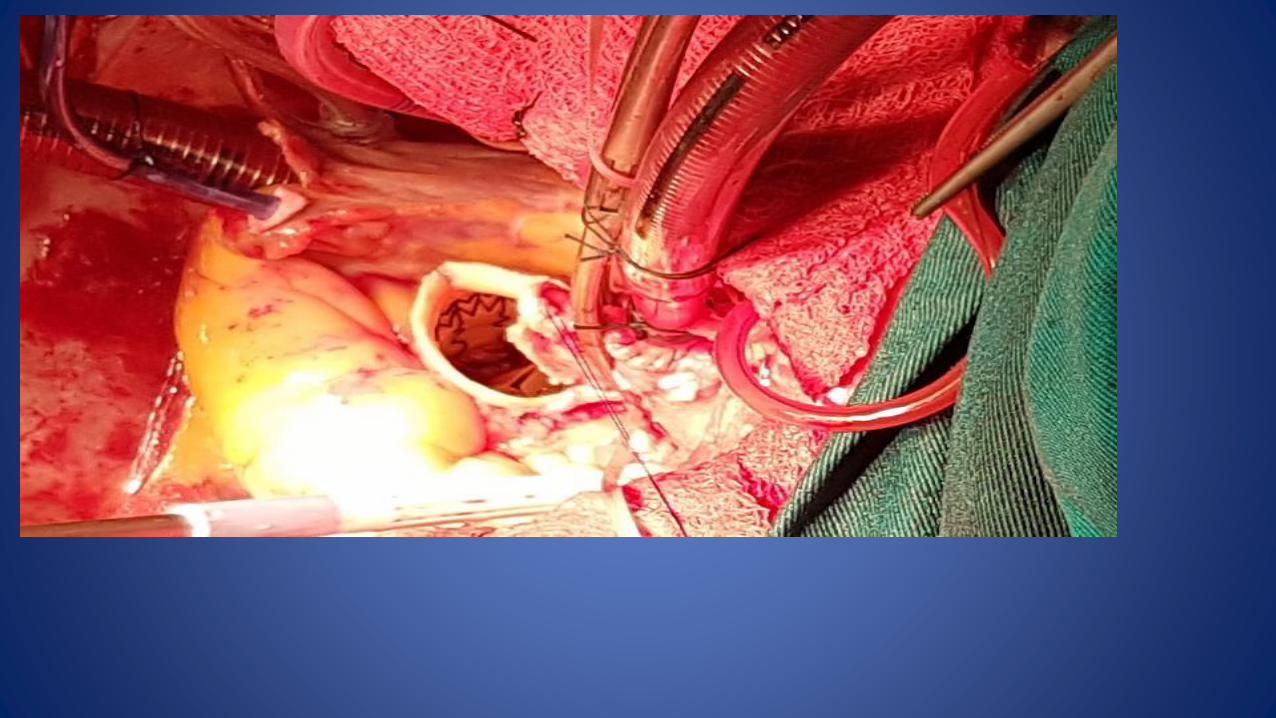
• SAVR and extraction
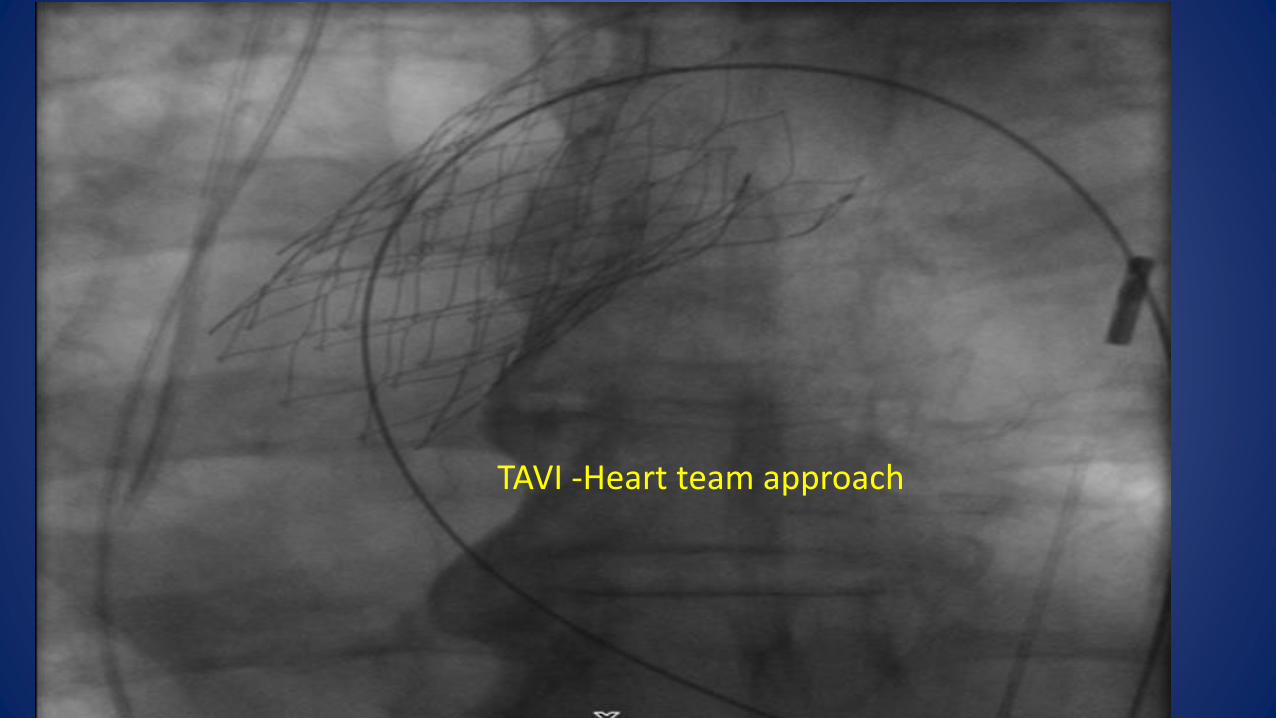
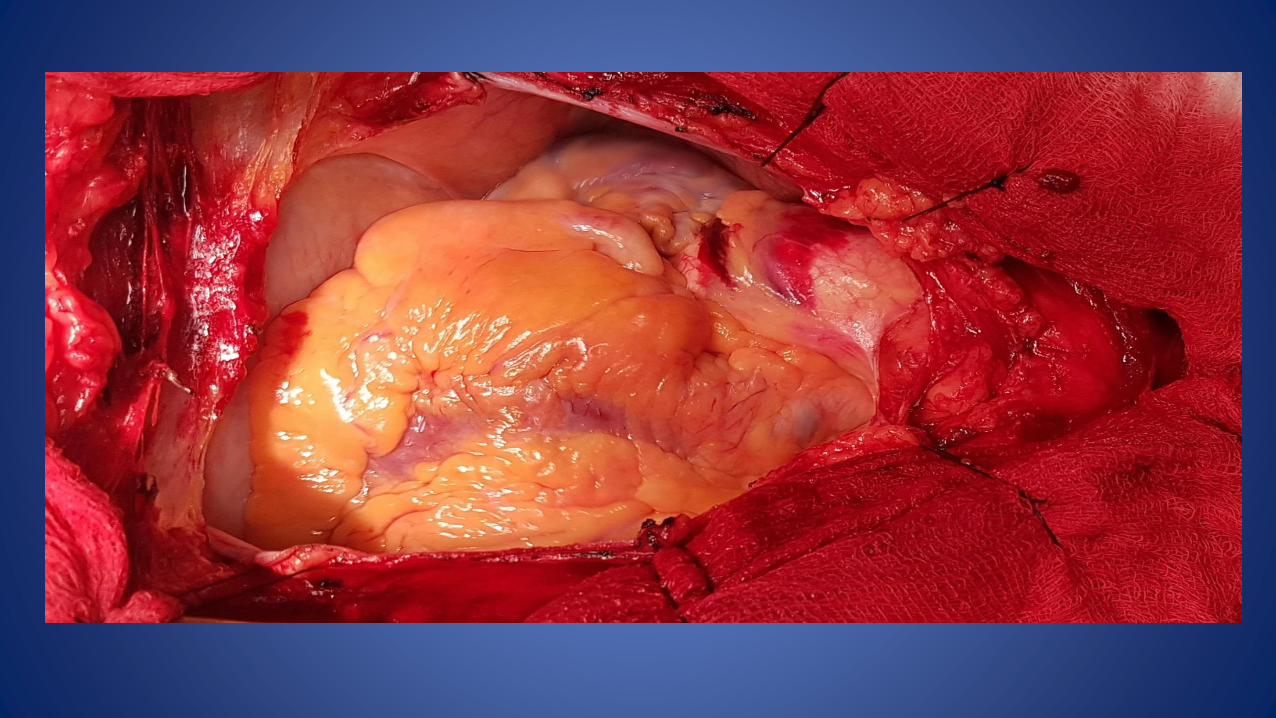
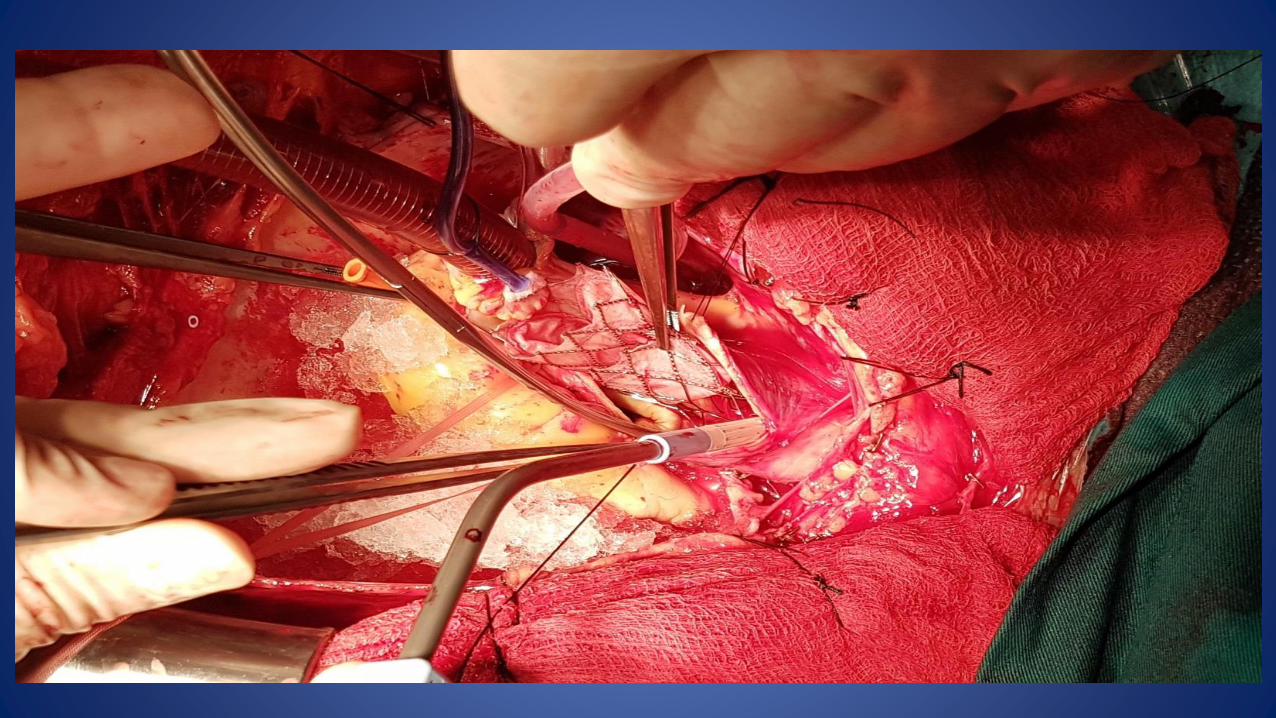
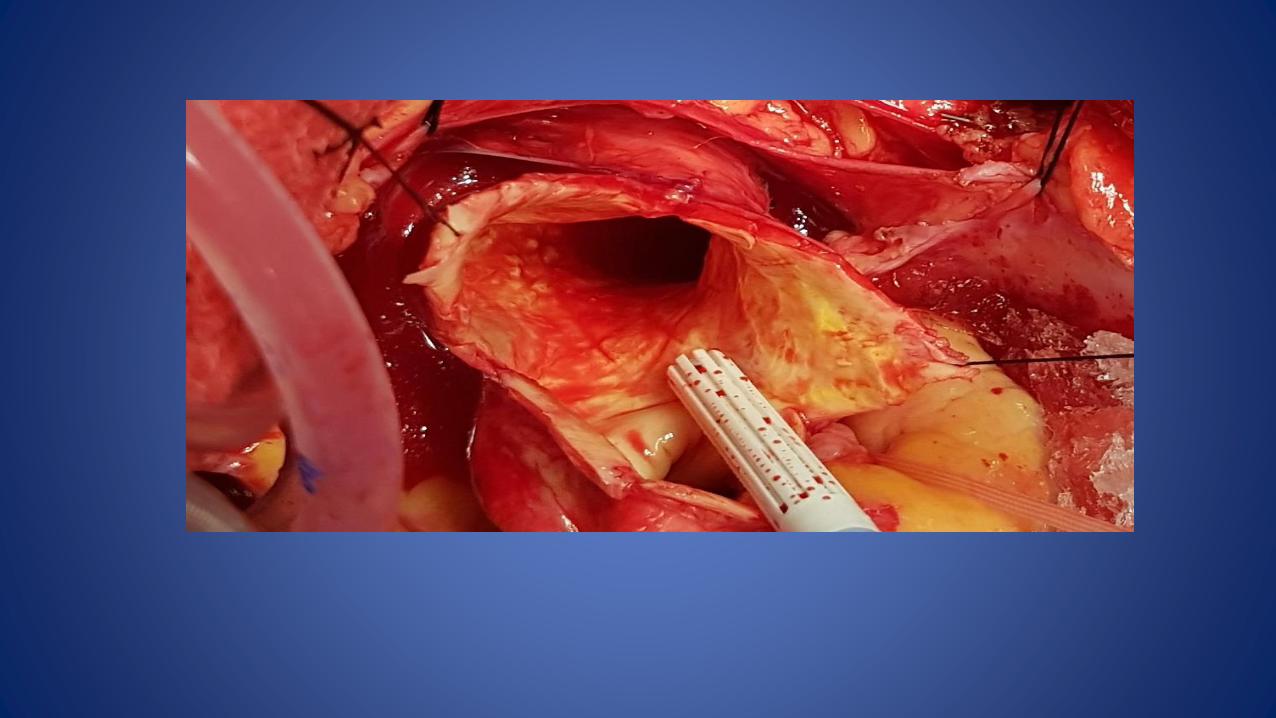
TAVI -Heart team approach
Other TAVI complications
• Acute renal failure requiring renal replacement therapy (1-6%)
• Prosthesis- related endocarditis (0.4-1.1%)
• Transcatheter valve thrombosis (7%)
Sudden and unexplained hypotension during TAVI =
The earliest indication of a major complication
EXCLUDE Retroperitoneal bleeding
Aortic dissection or Aortic annulus –root rupture
Pericardial tamponade
Coronary ostial obstruction
Acute severe aortic regurgitation
Shock-Hemodynamic collapse
• Assess and treat underling cause
• Inotropic support
• Mechanical circulatory support
• CPB
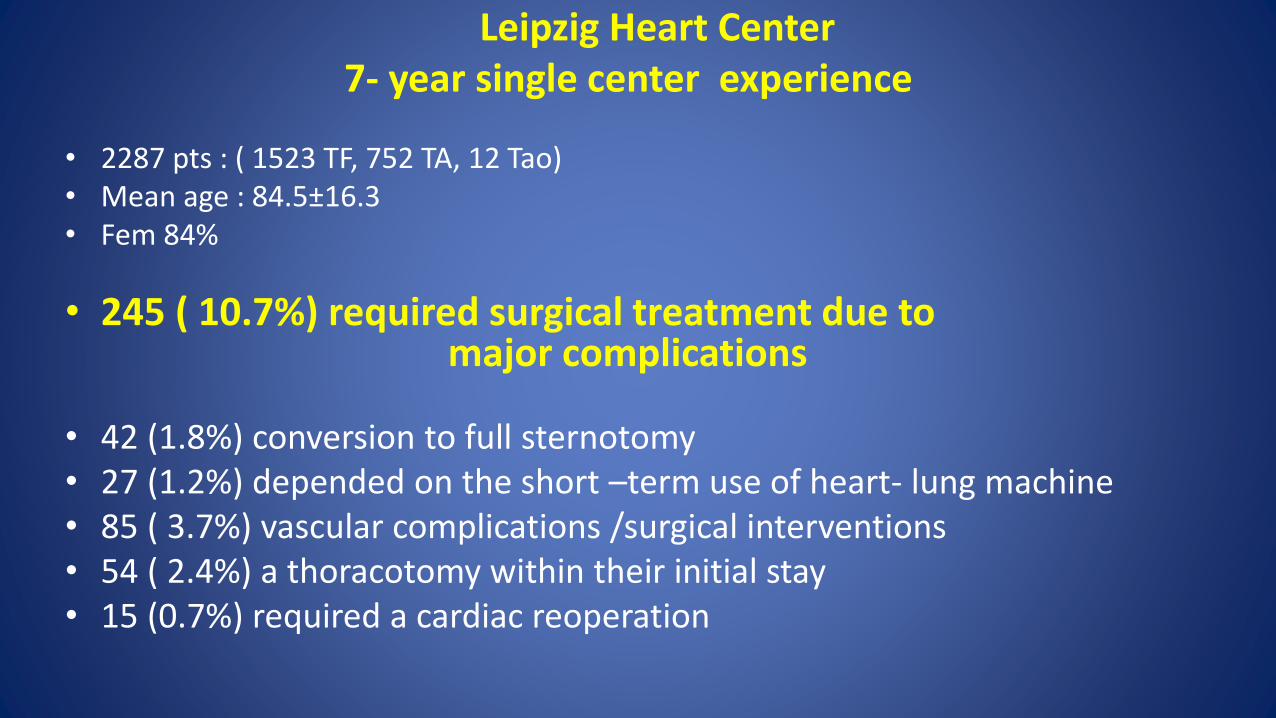
Leipzig Heart Center 7- year single center experience
• 2287 pts : ( 1523 TF, 752 TA, 12 Tao)• Mean age : 84.5±16.3• Fem 84%
• 245 ( 10.7%) required surgical treatment due to major complications
• 42 (1.8%) conversion to full sternotomy• 27 (1.2%) depended on the short –term use of heart- lung machine• 85 ( 3.7%) vascular complications /surgical interventions• 54 ( 2.4%) a thoracotomy within their initial stay• 15 (0.7%) required a cardiac reoperation
Outcome of patients after emergency conversion from TAVR to surgery
• 2 of 8 died in the Hybrid OR• 3 of 8 died in the surgical OR• 6 of 8 died in the catheterization -laboratory
• Hein R et al. Eurointervention 2013;9:446-51
SUGESTIONS- CONCLUSIONS
• Cardiac anesthesiologist
• General anesthesia
• Primed ECC machine for the difficult cases
• Present , active ,experienced and involved cardiac surgery team
• The procedure should be done ideally in a hybrid theater , so the conversion of a TAVI -catastrophe to an emergency surgical procedure can be done immediately

ΣΑΣ ΕΥΧΑΡΙΣΤΩ ΓΙΑ ΤΗΝ ΠΡΟΣΟΧΗ ΣΑΣ

• TELOS