ΥΠΟΓΛΥΚΑΙΜΙΑ -...
107
ΥΠΟΓΛΥΚΑΙΜΙΑ: ινσουλίνη-αντιδιαβητικά δισκία A. Μητράκου Αν.Καθηγήτρια Ιατρικής Σχολής Πανειστηµίου Αθηνών Θεραευτική Κλινική Μονάδα Σακχαρώδη ∆ιαβήτη - Μεταβολισµού
Transcript of ΥΠΟΓΛΥΚΑΙΜΙΑ -...
-
:-
A. .
-
-
HYPOGLYCEMIA HYPERGLYCEMIA
Insulin
Counter
regulatio
n Insulin
Counterregulation
-
Iatrogenic hypoglycemia is a major limiting factor in
the strict glycemic management of diabetes
-
Whipple:
( )
-
mg/dl
90
80
70
60
50
40
30
20
-
------ -
Mitrakou A, et al. American Journal of Physiology 1991; 260(Endocrinol. Metab. 23): E67-E74
euglycemia
hypoglycemia
-
Mitrakou A, et al. American Journal of Physiology 1991; 260(Endocrinol. Metab. 23): E67-E74
euglycemia
hypoglycemia
-
Mitrakou A, et al. American Journal of Physiology 1991; 260(Endocrinol. Metab. 23): E67-E74
-
.
Mitrakou A, et al. Journal of Clinical Endocrinology and Metabolism 1993; 76(2): 462-465
-
10
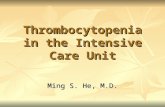
Prior Hypoglycemia Blunts Counterregulatory Response to Subsequent Comparable Hypoglycemia in Adults Without
Diabetes
Heller SR. Diabetes. 1991;40(2):223226. Permission pending.
Hyperinsulinemic hypoglycemic clamps on 2 consecutive mornings, with interval
afternoon clamped hypoglycemia in adults without diabetes.
**
**** ***
To
tal S
ym
pto
m S
co
re
Clock Time (h)
0
20
40
0
20
40
0915 0930 0945 1015 1030 1045
****
Glu
cag
on
Clock Time (h)
100
200
300
100
200
300
0915 0930 0945 10151030 1045
Morning before Morning after
*P
-
11
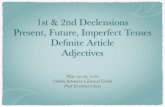
Matyka K et al. Diabetes Care. 1997;20(2):135141.
Change in Plasma Glucose
200
Time, min
402.0
3.0
4.0
5.0
6.0
0 40 80 120 160
Young Men Without Diabetes
Elderly Men Without Diabetes Chan
ge in
To
tal S
ym
pto
m S
co
re
0
14
12
10
8
6
4
2
Pla
sm
a G
luco
se, m
mo
l/L
Glucose
Infusion
maintained at
5 mmol/L
(90 mg/dL)
Glucose Infusion
reduced stepwise from
5 mmol/L to 2.4 mmol/L
(90 mg/dL to 43 mg/dL)
Glucose
Infusion
restored to
5 mmol/L
(90 mg/dL)
-
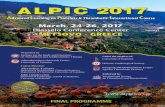
12
Change in Plasma Glucose
Time, min
40
Pla
sm
a G
luco
se, m
mo
l/L
2.0
3.0
4.0
5.0
6.0
0 40 80 120 160 200
Ch
an
ge in
Reactio
n T
ime, m
s
0
350
300
250
200
150
100
50
200
*
*
Matyka K et al. Diabetes Care. 1997;20(2):135141.
*
Glucose
Infusion
maintained at
5 mmol/L
(90 mg/dL)
Glucose Infusion
reduced stepwise from
5 mmol/L to 2.4 mmol/L
(90 mg/dL to 43 mg/dL)
Glucose
Infusion
restored to
5 mmol/L
(90 mg/dL)
Young Men Without Diabetes
Elderly Men Without Diabetes
-
1
-
(
100
-
)
DCCT:
(
100
-
)
Adapted from: N Engl J Med 1993;329:97786
0
2
4
6
8
10
12
0 5.5 6 6.5 7 7.5 8 8.5 9 9.5 10 10.5
120
60
0
HbA1c (%)
-
Normal
CDAN +
CDAN -
IMPAIRED COUNTERREGULATION in TYPE 1 DIABETES
-
1
-
1
-
HYPOGLYCAEMIA
(HAAF)
-
Insulinoma
Mitrakou A.N.Engl J Med 329: 834-839;1993
-
1
-
REVERSIBILITY
-
1
-
36
stress 610
, !!!
-
1
(18 )
1, problem solving;
2, learning;
3, immediate memory;
4, delayed recall;
5, spatial information;
6, attention;
7, psychomotor efficiency; and
8, motor speed
N Engl J Med 2007;356:1842-52.
-
Brain Activation During Working Memory in Patients With Type 1 Diabetes During Hypoglycemia
Diabetes 60:32563264, 2011
Controls Type 1 Diabetes
-
1
-
Does A1C tell the whole story ?
-
Get the complete picture
Even patients with acceptable A1C levels can
experience glycemic variability
-
Professional CGM vs Personal CGM
Ideal for short term blinded CGM
evaluation and retrospective analysis
Quick and easy to set up,
minimal patient training
no alarm
Can be used on all patients with
diabetes to reveal excursions and
patterns
Glucose Sensor readings are
updated every 5min on the monitor
Trend Graphs, Arrows and Alerts
help the patient avoiding lows and
highs
Patients motivation and training
are key to success
-
n = 272 Type 1 patients
5-Nations Study CSII A1C
Hoogma RP. et al. Diabet Med. 2006; 23:141-147.
-
CSII 1/4
1 Rudolph JW, Hirsch IB. Endocrine Pract 2002: 8; 401 4052 Bode, BW et al., Diabetes Care 1996, 19:325-7. 3 Boland, EA et al., Diabetes Care 1999, 22:1779 - 84. 4 Pickup JC & Sutton, AJ. Diabet Med 2008;25:765-774
1 2 3
Severe Hypoglycaemic Episodes: CSII vs MDI
-
New!!! Paradigm Veo
-
?
User settable: On/Off
Range: 40 110 mg/dLFictional illustration of Low Glucose
Suspend function in use 2
4
-
Reduction in Duration of Hypoglycemiaby Automatic Suspension of Insulin Delivery:
The In-Clinic ASPIRE Study
DIABETES TECHNOLOGY & THERAPEUTICS
Volume 14, Number 3, 2012
-
2
-
UKPDS 33: Intensive treatment and Hypoglycemiain type 2 Diabetes
(%
)
Adapted from: Lancet 1998;352:83753
50
40
30
20
10
0
0 3 6 9 12
All eventsSevere hypo
8
4
2
0
0 3 6 9 12
6
CONVENTIONAL
INTENSIVE
-
UKPDS 33
-
Insulin
InsulinInsulin
o----o Diabetics
Controls
o----o Diabetics
Controls
o----o Diabetics
Controls
o----o Diabetics
Controls
Insulin
Time (min) Time (min)
Time (min) Time (min)
Counterregulation in type 2 diabetes -normal endocrine and glycemic
Heller, et al. Diabetologia 1987; 30: 924-929
-
, , 2
Spyer G, et al. Lancet 2000 ; 356(9246): 1970-1974
-
, 2
Spyer G, et al. Lancet 2000 ; 356(9246): 1970-1974
-
Spyer G, et al. Lancet 2000 ; 356(9246): 1970-1974
-
2
insulin
normal
Oral hyp agents
Glu
ca
go
n (
pg
/ml)
Ep
ine
ph
rin
e (
pg
/ml)
-
( HbA1c) 2
Burakowska A. Diabetes Care 21:283-290,1998
Type 2
oControls
-
Poor control
oImproved control
Burakowska A. Diabetes Care 21:283-290,1998
-
Poor control
oImproved control
Burakowska A. Diabetes Care 21:283-290,1998
-
: 2
2 .
, .
.
-
:
DavisS Diabetes 58:701-709,2009bA1c 10.2 to 6.7%
-
:
DavisS Diabetes 58:701-709,2009
-
Glu
ca
go
n (
pg
/ml)
Ep
ine
ph
rin
e (
pg
/ml)
After hypergl
After Hypogl
-
1 2
Amiel SA, et al. Diabetic Medicine 2008; 25: 245254
Proportion of patients with Type 2 and Type 1 diabetes of differing durations and receiving different regimens experiencing at least one s eve re hypog lycaemic attack during 912 monthsfollow-up. All patients were receiving insulin except the g r o u p t r e a t e d w i t h s u l p h o n y l u r e a
Proportion of patients with Type 2 and Type 1
diabetes experiencing at least one severe
hypoglycaemic attack
-
1 2
1 2
-
.. 2
.. ,
.. Addison's disease, ,
.. , ..
..
..
-
Moderate quality of evidence (QQQ)
Cibenzoline
Gatifloxacin *
Pentamidine
Quinine
Indomethacin ( )
Glucagon (during endoscopy)
Low quality of evidence (QQ)
Chloroquineoxaline sulfonamide
Artesunate/artemisin/artemether
IGF-I
Lithium
Propoxyphene/dextropropoxyphene
Very low quality of evidence (Q)
Drugs with 25 cases of
hypoglycemia identified
Angiotensin converting enzyme
inhibitors
Angiotensin receptor antagonists
-Adrenergic receptor antagonists
Levofloxacin
Mifepristone
Disopyramide
Trimethoprim-sulfamethoxazole*
Heparin*
6-Mercaptopurine
*
-
.
,
.
-
Bolen S, et al. Ann Intern Med 2007;147:386-399.
Reproduced with permission
-
A1C
0
10
20
30
40A
nnua
l ra
te (
%)
0 4 5 6 7 8 9 10 11
Most recent A1C (%)
Wright et al. J Diabetes Complications. 2006;20:395-401.
Reproduced with permission
-
(UKPDS)
UKPDS 33. Lancet 1998;352:837-853.
Diet Chlorpropamide Glibenclamide Insulin
Any Severe
1.2
11
17.7
36.5
0
10
20
30
40
Mean (
%)
0.1
0.4
0.6
2.3
0.0
0.5
1.0
1.5
2.0
2.5
3.0
Mean (
%)
-
ADOPT Study N Engl J Med 2006;355:2427-2463.
(the ADOPT study)
38.7
11.69.8
0.6 0.1 0.10
10
20
30
40
Perc
ent
of
patients
with e
pis
odes
All hypoglycemia Severe
hypoglycemia
Glyburide Metformin Rosiglitazone Glyburide Metformin Rosiglitazone
-
2
9-12 6 UK
: 39% SU
7% of SU
14% SU
-
Patients reporting grade 2 or grade 3 hypoglycaemic events
Holman RR, et al. N Engl J Med 2007;357:1716-1730.
-
2
24,000
-
0
5
10
15
20
ACCORD ADVANCE
Intensive control
Standard control
% P
atients
with a
t le
ast
one e
ve
nt
during t
he t
rial
25
VADT
-
ADVANCE vs. UKPDS
UKPDS ADVANCE
0
1
2
Even
ts p
er
100 p
ati
en
ts/y
ear
0,7%
1,4%
ADVANCE collaborative group. NEJM,
-
2: The Fremantle Diabetes Study
:
,
< 60 ml/min per 1.73 m(2),
,
,
.
HbA1c
.
DavisClin Endocrinol Metab. 2010
-
ACCORD
ACCORD study. N Engl J Med 2008;358(24): 2545-2559.
16.2
5.1
10.5
3.5
0
3
6
9
12
15
18
Patients
(%
)
3
Intensive therapy
(target HbA1c
-
ACCORD:
1.2%
3.3%
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
Never experienced SH Experienced SH
Overa
ll m
ort
alit
y r
ate
(%
)
SH = severe hypoglycaemia
The cause of the increased mortality could not be proven;
severe hypoglycaemia was implicated
-
(IHD,autonomic neuropathy)
/
-
Antecedent hypoglycemia impairs
autonomic cardiovascular function
Adler GK, Diabetes 58:360 366, 2009
-
Altered Ventricular Repolarization During Hypoglycaemia in
Patients with Diabetes type 2 on insulin Diabet. Med 199714: 648654
-
CCORD
2
.
2
ACCORD , ( HbA1C
)
.
HbA1C
4
HbA1C
.
-
HbA1c and Risk of SevereHypoglycemia in Type 2 Diabetes
The Diabetes and Aging StudyDiabetes Care July 2013
-
Intensive glucose lowering on brain structure and function in people with type 2 diabetes
(ACCORD MIND)
40
3
-
Poor Cognitive Function and Risk of Severe
Hypoglycemia in Type2Diabetes (ACCORD)
Diabetes Care 35:787793, 2012
-
B. E. de Galan Diabetologia (2009) 52:23282336
ADVANCE-ACCORD
-
vs
DPP4/
-
0
1
2
3
4
5
6
7
8
No severe hypos
Severe hypos
Media
n d
ura
tio
n o
f in
sulin
thera
py (
years
)
Type 2 diabetes Type 1 diabetes
Hepburn et al. Diabetic Med 1993; 10(3): 231-7.
-
2
1
.2
6 .3
15% 2 1,4
1. McAulay V, et al. Diabet Med. 2001;18:690-705.2. Amiel SA, et al. Diabetic Medicine 2008;25:245-254.
3. Gold AE, et al. Diabetes Care 1994;17:697-703.4. Leiter LA, et al. Can J Diab. 2005;29(3):186-192.
-
GLP-1
.
30 0 30 60 90 120 150 180 210 240 270 300 330 360
Glucose Clamp Steps
Pla
sm
a G
lucagon (
ng/L
)
0
50
100
150
200
300
250
(mmol/L): 5.0 4.0 3.2 2.7 Recovery
GLP-1=glucagon-like peptide-1
*P
-
Vilda and Hypo response of Glucagon
J Clin Endocrinol Metab. 2009;94:1236-1243
-
Vildagliptin :
Fonseca V et al. Diabetologia 2007;50:1148-1155.
No. of events No. of severe events
0
40
80
120
160
200
Placebo + insulin
Vildagliptin + insulin
0
2
4
6
8
10
Num
ber
of
severe
events
113
185
0
6
**
*
Num
ber
of
events
Severe defined as grade 2 or suspected grade 2 hypoglycaemia.
*p
-
vs
Basal Bolus
-
. 2
.
.
-
Adapted from Fredrickson L, et al. Optimal Pumping: A Guide to Good Health with Diabetes.
Medtronic MiniMed, Inc.; 1998.
3 AM
Bolus
Bolus Wizard calculator
bolus
-
15 15 15 grams
3 4 tablets
45 mL
1
15 -
1
!!!!
v2
-
93
v2 1 fluid ounce = 118 mlvavruh1; 30/10/2006
-
, ( )
-
GlucaGenHypoKit
,
1ml
10-15
1mg(1 ml) 0,5mg(0,5
ml) 25
-
!!
6.5
-
1
73 2 .
basal-bolus A1c 6.4%.
.
sliding scale
-
2
-
3
62 2 10.
HbA1c
9.7%. BMI 34.
.
+
Basal bolus
DPP-4
-
(
)
-
Summary of Impaired Counterregulation
-
in ACCORD, hypoglycemia was judged to have a definite role in only one death, a probable role in three deaths,and a possible role in 38 deathswhich represents a role in less than 10%of the deaths recorded in the study population while the glycemic intervention was active. The investigators thus suggest that hypoglycemia at the time of death was probably not responsible for the increasedmortality rate in the intensive arm of ACCORD
-
that an episode of severe hypoglycemia was associated with an increased risk of subsequent mortality. In ACCORD, those who had one or more severe hypoglycemic episodes had higher rates of death than those without such episodes across both study arms (hazard ratio 1.41 [95%CI 1.031.93]) (46). One-third of all deaths were due to cardiovascular disease, and hypoglycemia was associated with higher cardiovascular mortality. In VADT, a recent severe hypoglycemic event was the strongest independent predictor of death at 90 days (3). In ADVANCE, where rates of hypoglycemia were low, a similar pattern was found (47).
-
ADVANCE