





γλώσσες
Σελίδες
Νομικός

Primary Health Care in a time of crisis
Evangelos A. Fragkoulis, MD, GPSecretary General of the Greek Union of GPs
MSc in Health Care ManagementNational Delegate VdGM

Financial sustainability of health systems in Europe
• ageing populations/ cost-increasing developments in technology/ changing public expectations
how to pay for health care in thirty years’ time
• economic crisis
how to pay for it in the next three months
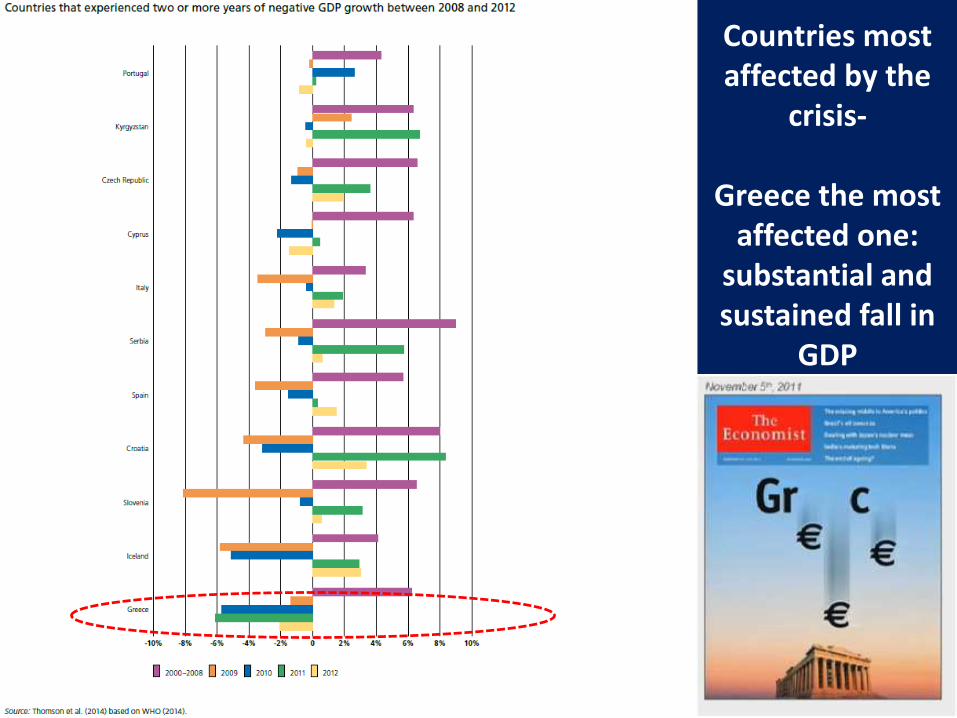
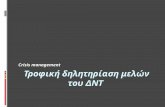
Countries most affected by the
crisis-
Greece the most affected one:
substantial and sustained fall in
GDP
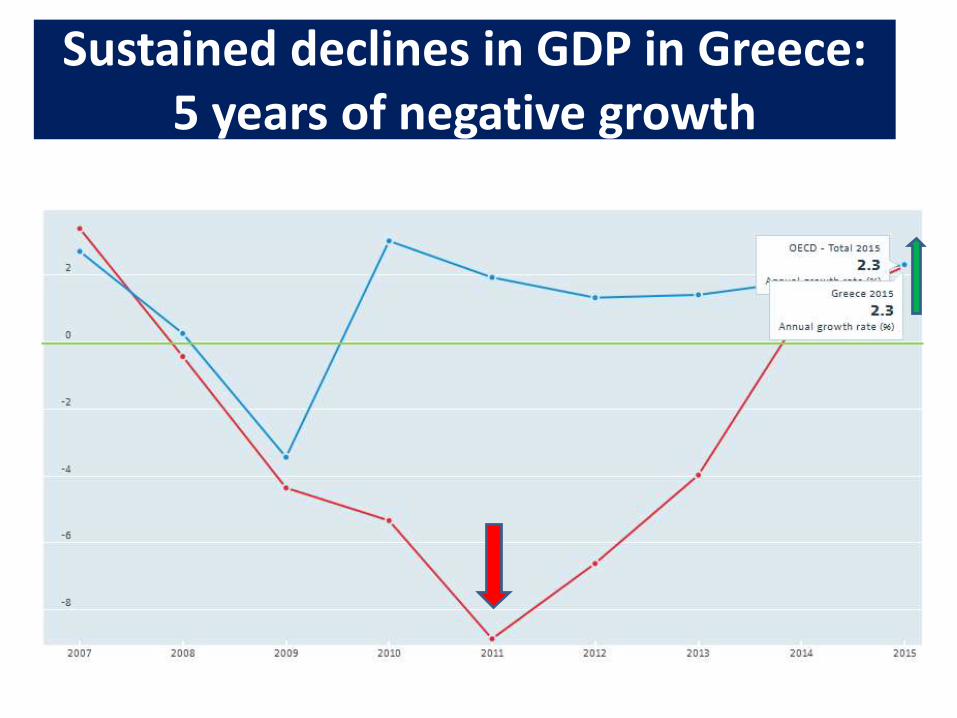
Sustained declines in GDP in Greece: 5 years of negative growth
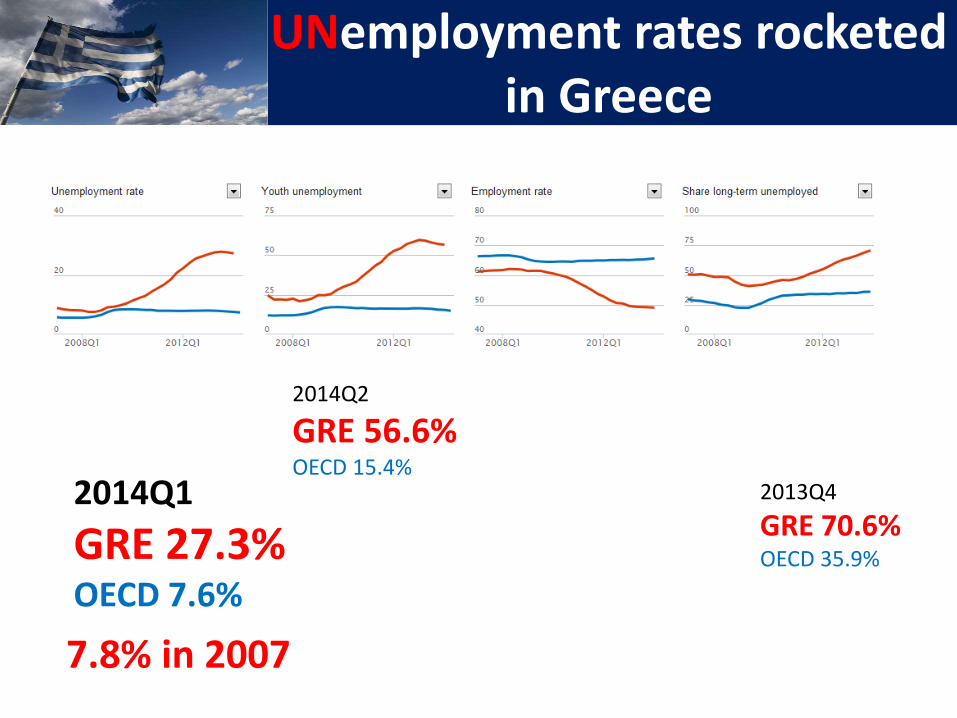
UNemployment rates rocketed in Greece
2014Q1
GRE 27.3%OECD 7.6%
2014Q2
GRE 56.6%OECD 15.4%
2013Q4
GRE 70.6%OECD 35.9%
7.8% in 2007
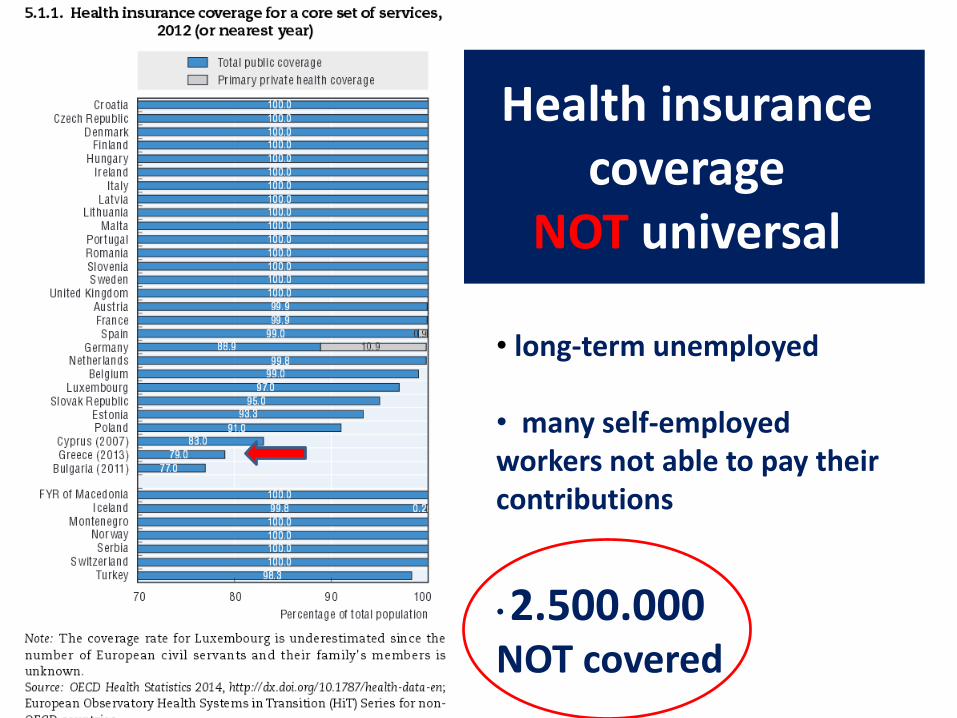
Health insurance coverage
NOT universal
• long-term unemployed
• many self-employed workers not able to pay their contributions
•2.500.000NOT covered
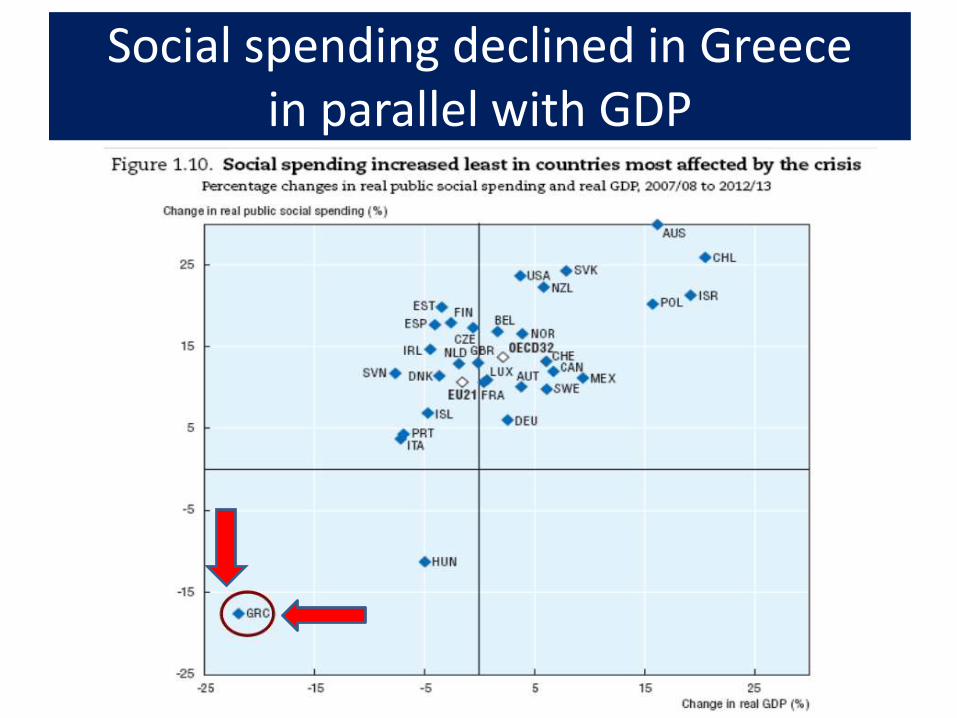
Social spending declined in Greece in parallel with GDP
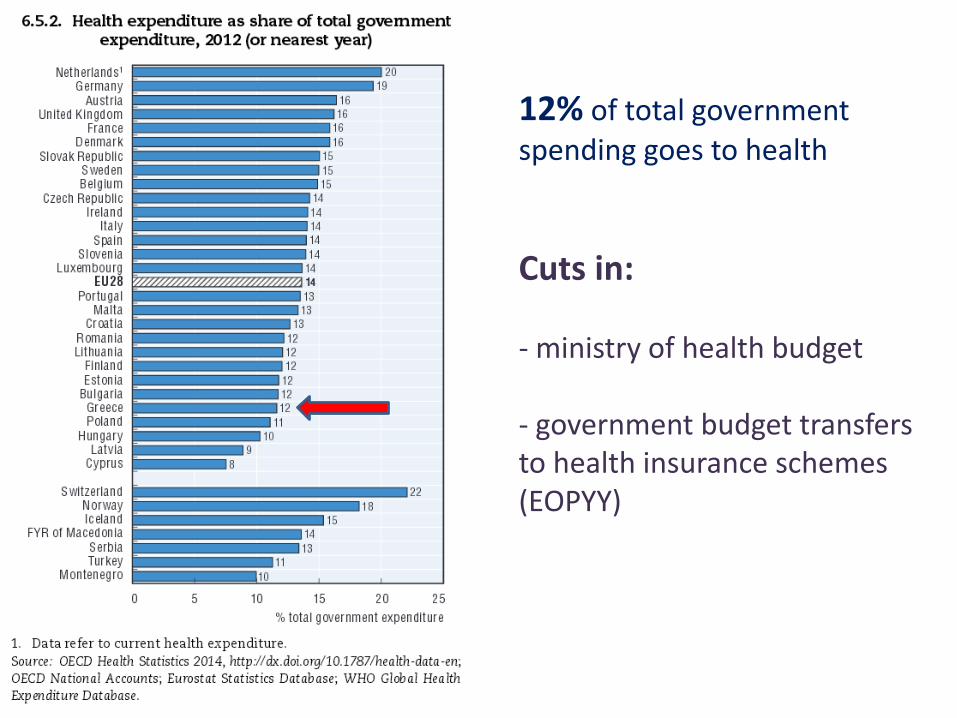
12% of total government spending goes to health
Cuts in:
- ministry of health budget
- government budget transfers to health insurance schemes (EOPYY)
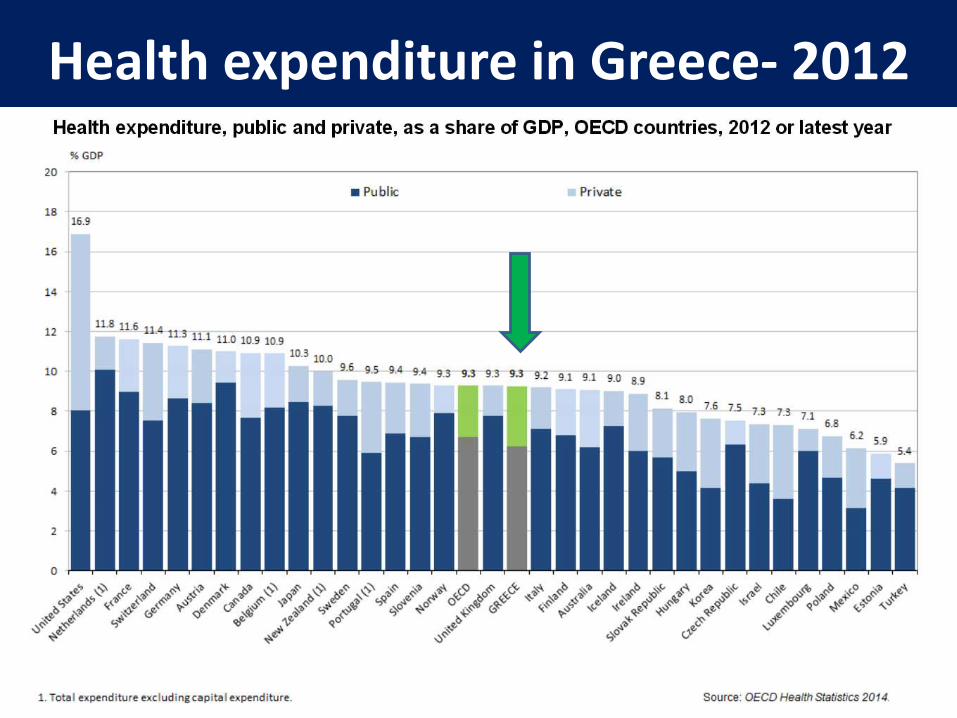
Health expenditure in Greece- 2012
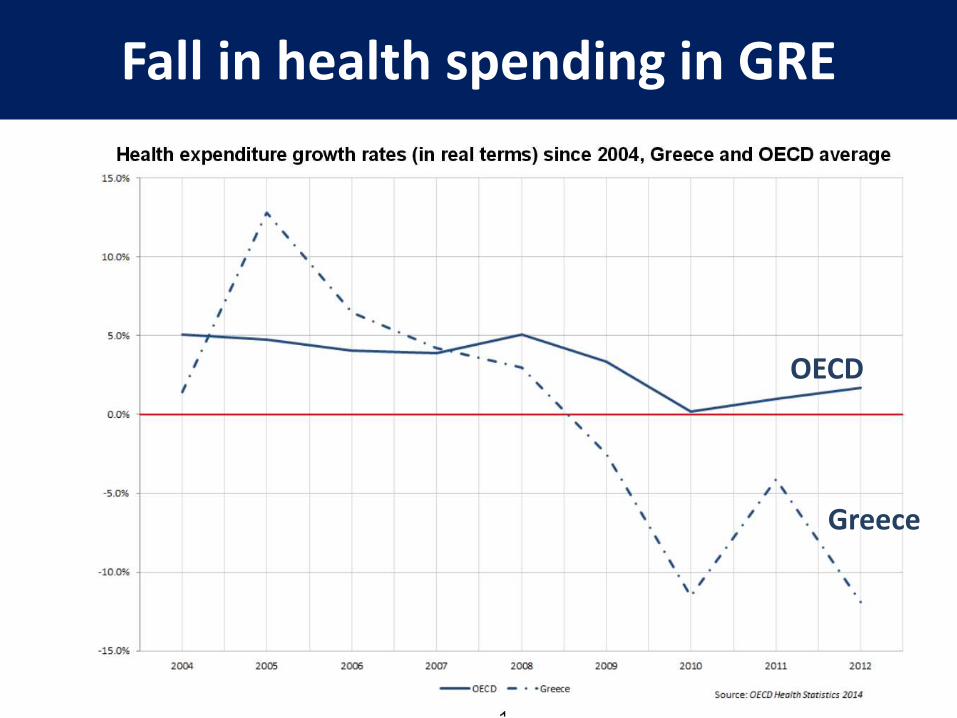
Fall in health spending in GRE
Greece
OECD
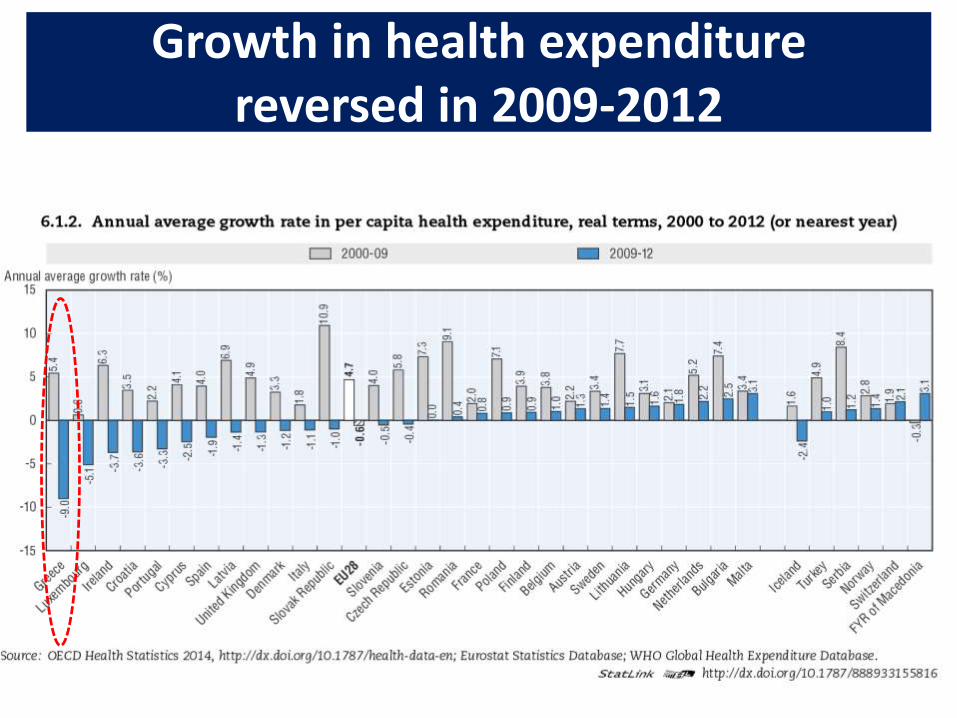
Growth in health expenditure reversed in 2009-2012
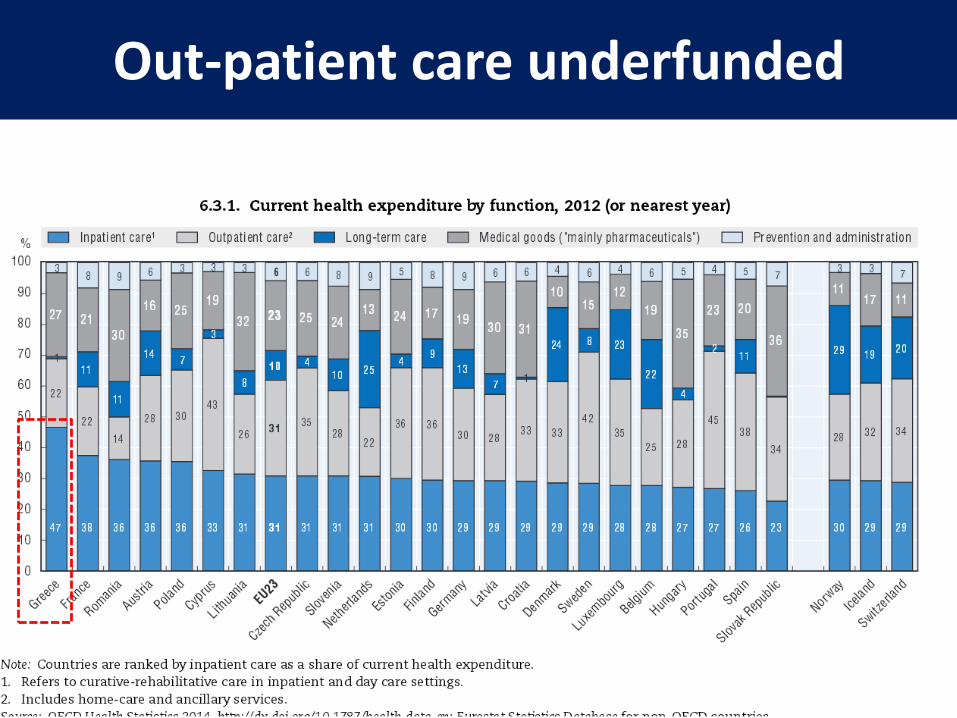
Out-patient care underfunded
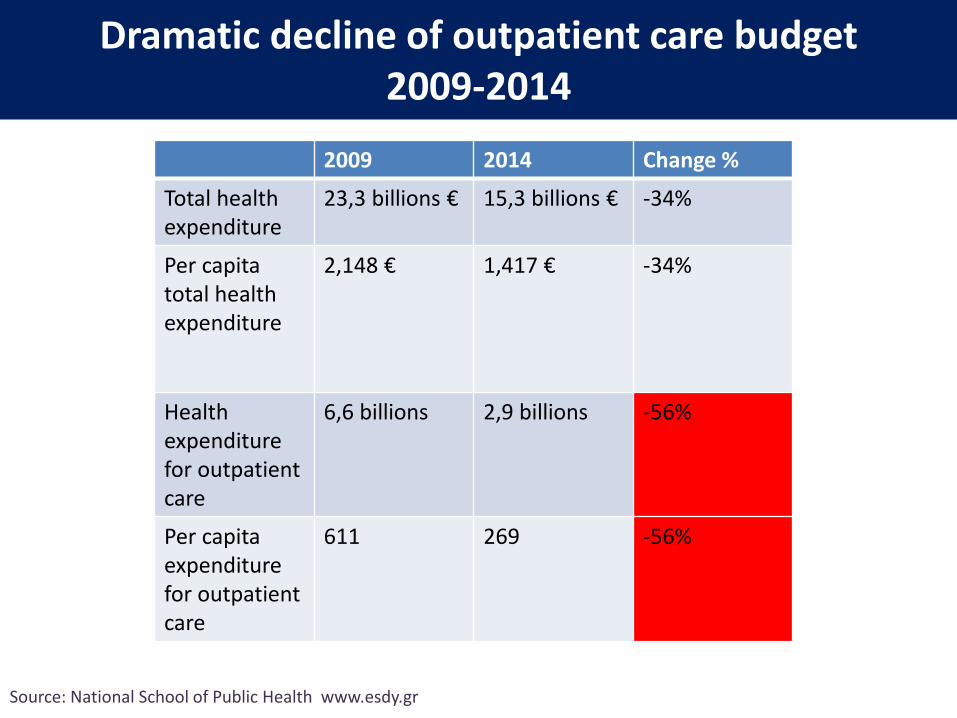
Dramatic decline of outpatient care budget2009-2014
2009 2014 Change %
Total health expenditure
23,3 billions € 15,3 billions € -34%
Per capita total healthexpenditure
2,148 € 1,417 € -34%
Health expenditure for outpatient care
6,6 billions 2,9 billions -56%
Per capita expenditure for outpatient care
611 269 -56%
Source: National School of Public Health www.esdy.gr
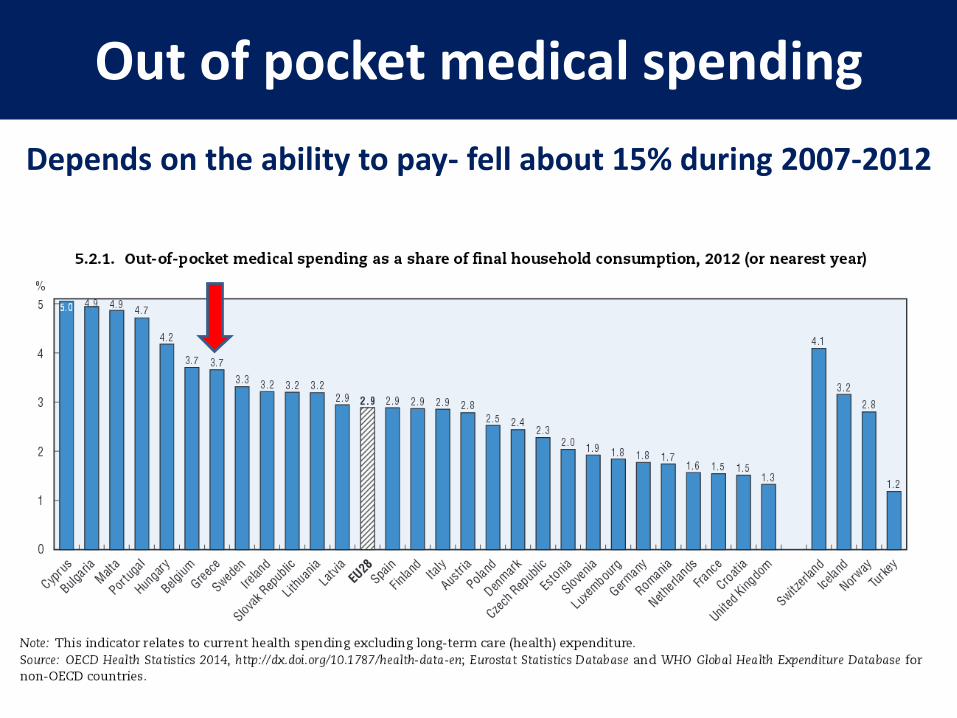
Out of pocket medical spending
Depends on the ability to pay- fell about 15% during 2007-2012
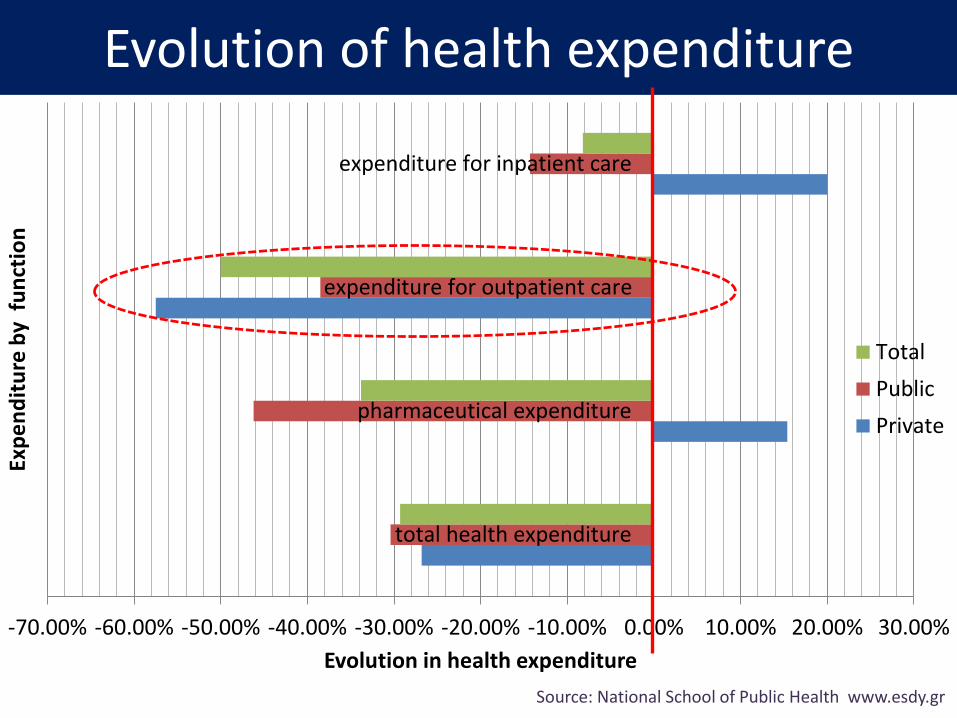
Evolution of health expenditure
-70.00% -60.00% -50.00% -40.00% -30.00% -20.00% -10.00% 0.00% 10.00% 20.00% 30.00%
total health expenditure
pharmaceutical expenditure
expenditure for outpatient care
expenditure for inpatient care
Evolution in health expenditure
Exp
en
dit
ure
by
fu
nct
ion
Total
Public
Private
Source: National School of Public Health www.esdy.gr
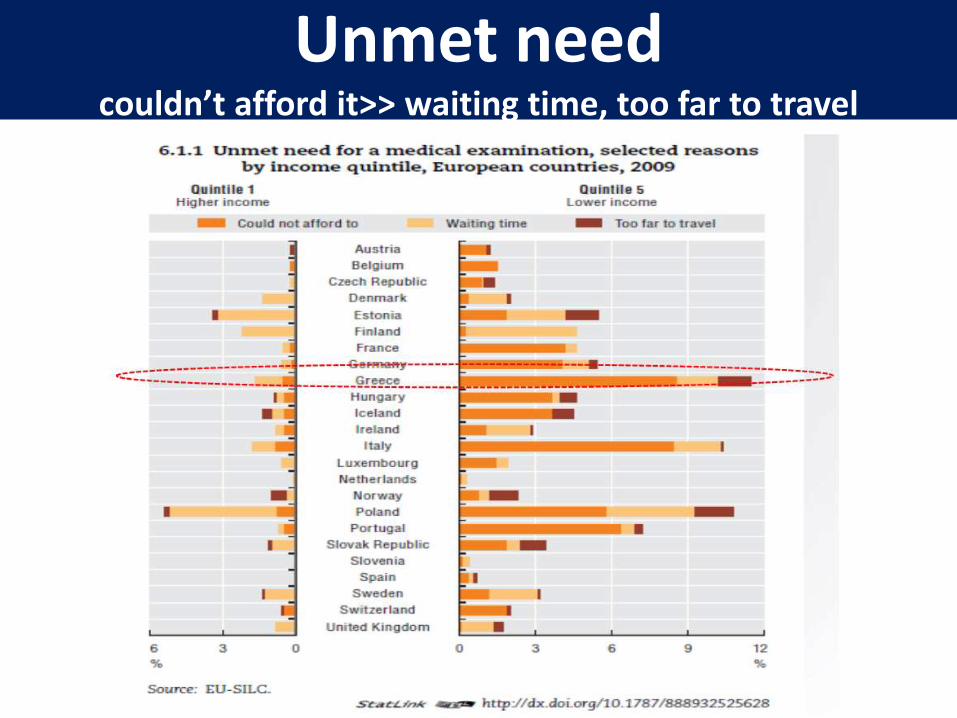
Unmet needcouldn’t afford it>> waiting time, too far to travel
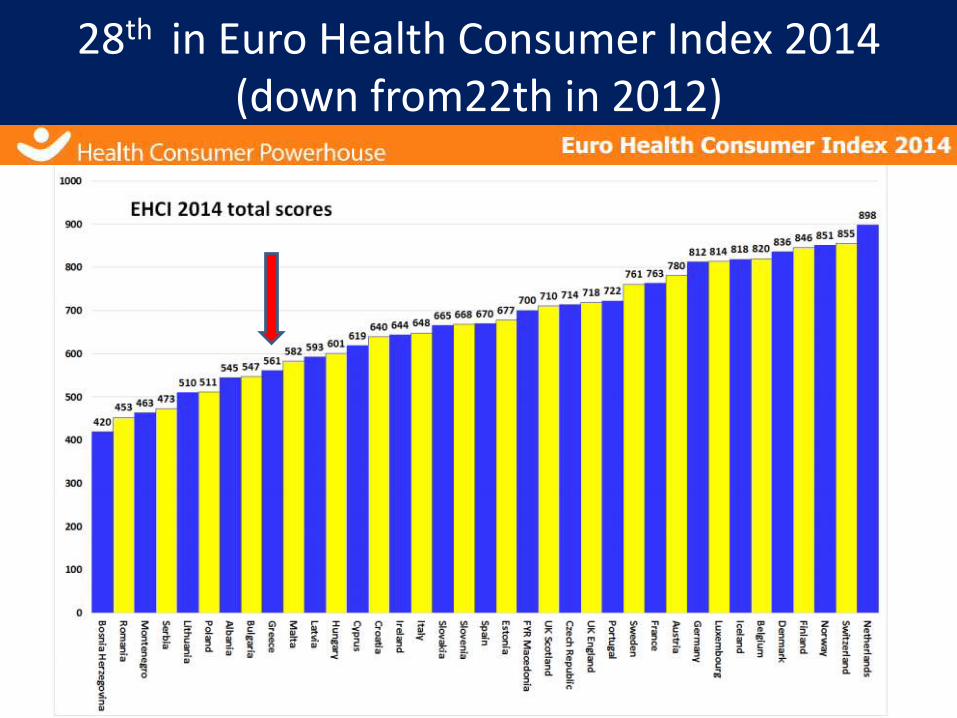
28th in Euro Health Consumer Index 2014 (down from22th in 2012)
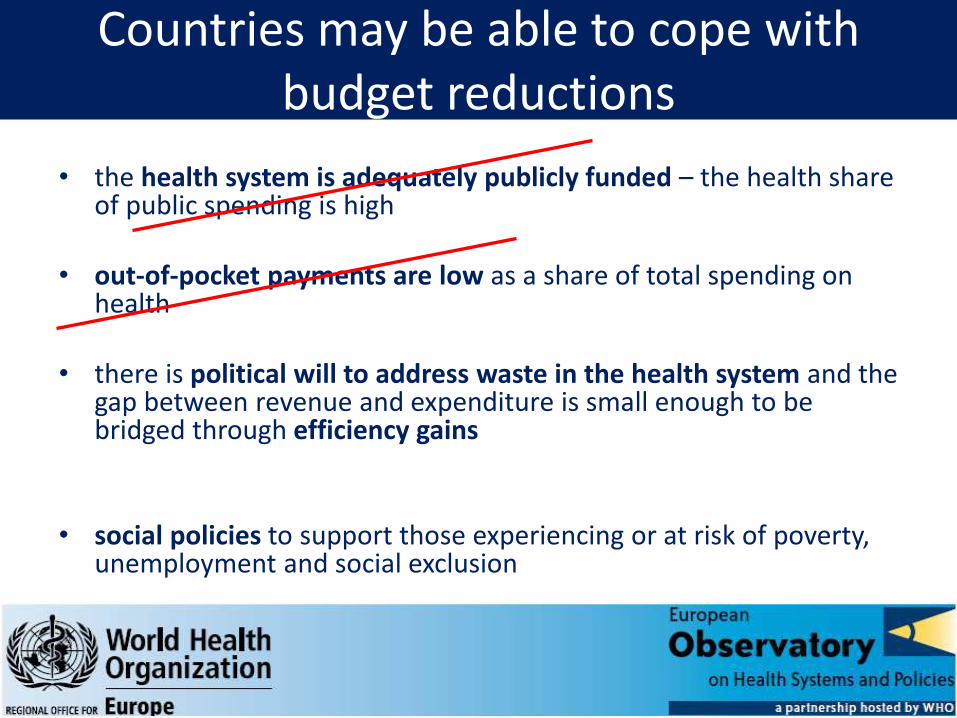
Countries may be able to cope with budget reductions
• the health system is adequately publicly funded – the health share of public spending is high
• out-of-pocket payments are low as a share of total spending on health
• there is political will to address waste in the health system and the gap between revenue and expenditure is small enough to be bridged through efficiency gains
• social policies to support those experiencing or at risk of poverty, unemployment and social exclusion
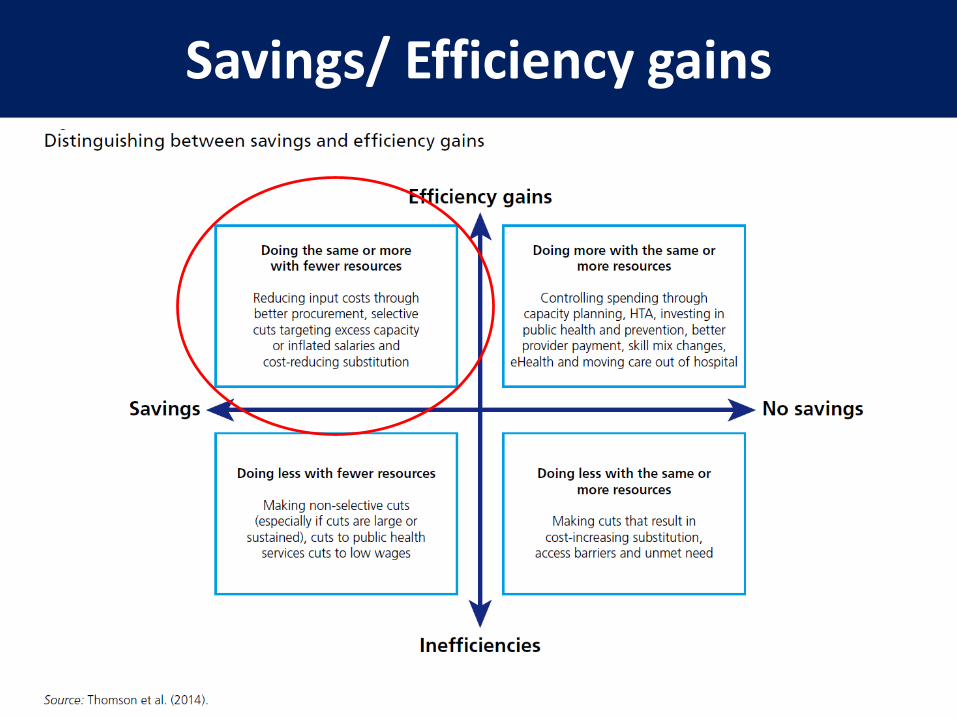
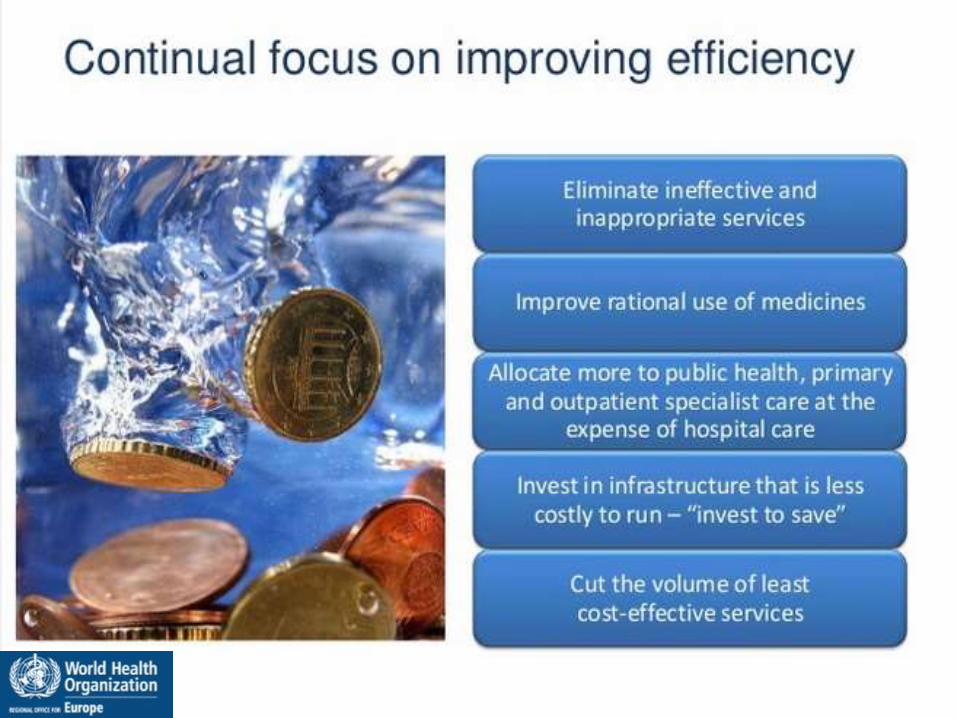
Savings/ Efficiency gains
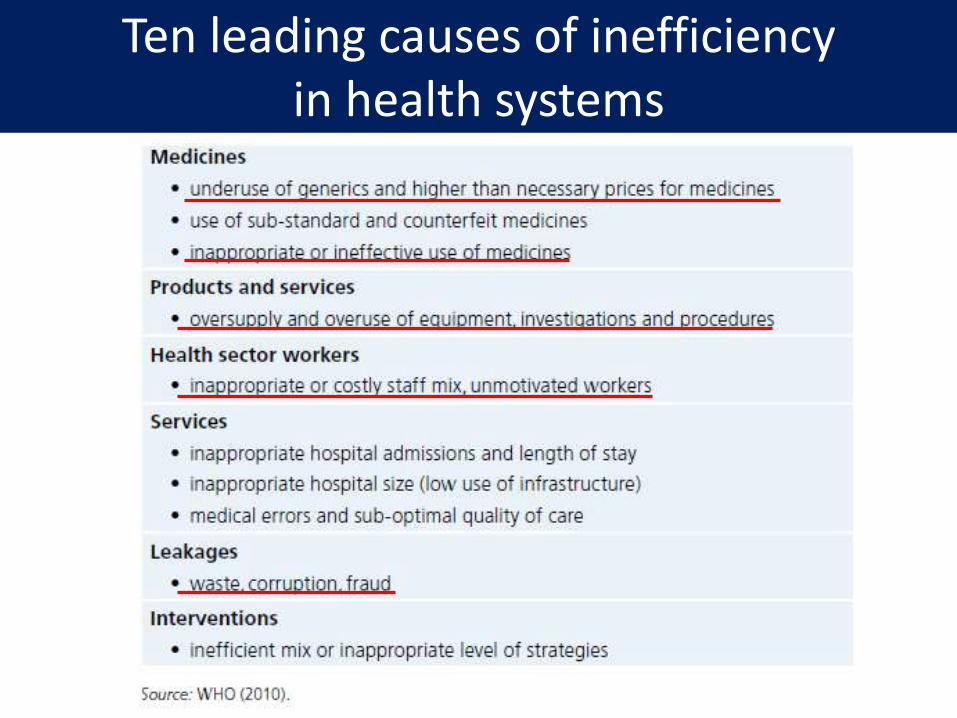
Ten leading causes of inefficiency in health systems
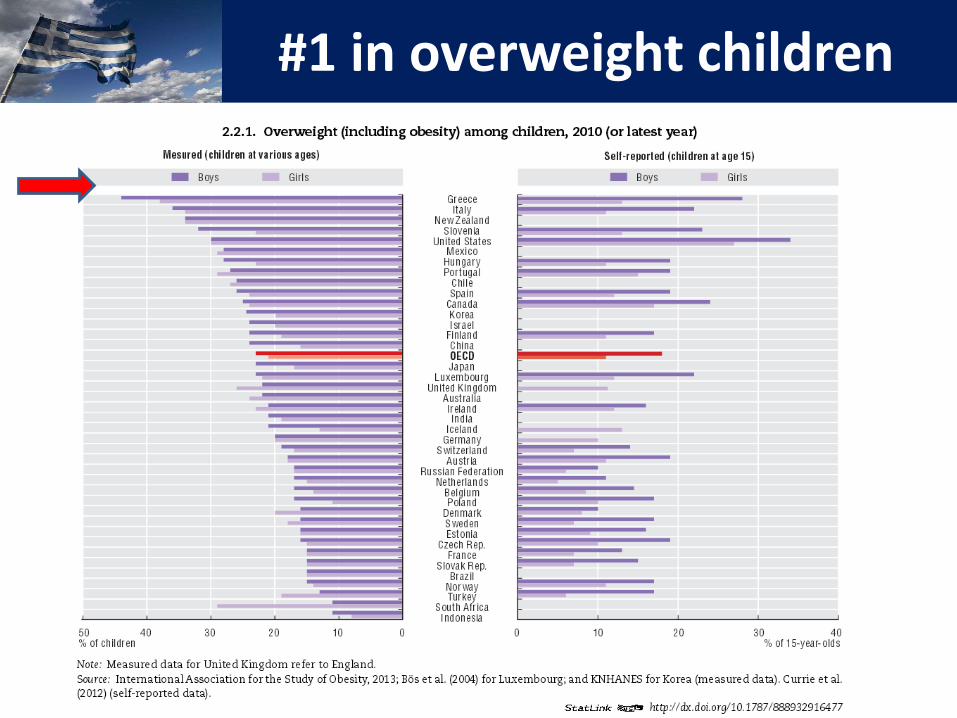
#1 in overweight children
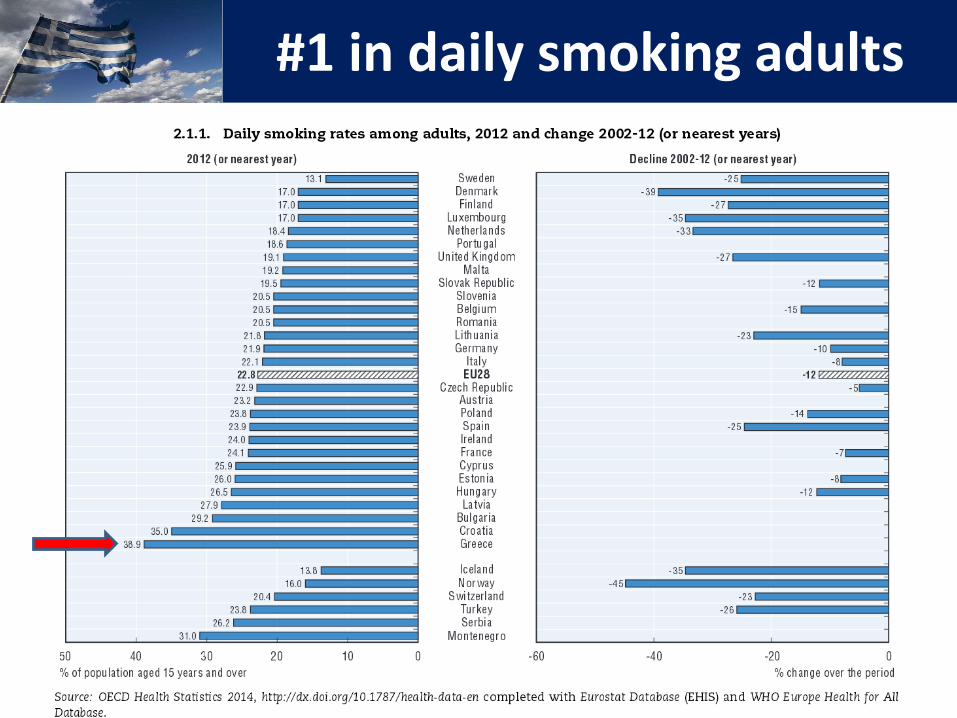
#1 in daily smoking adults
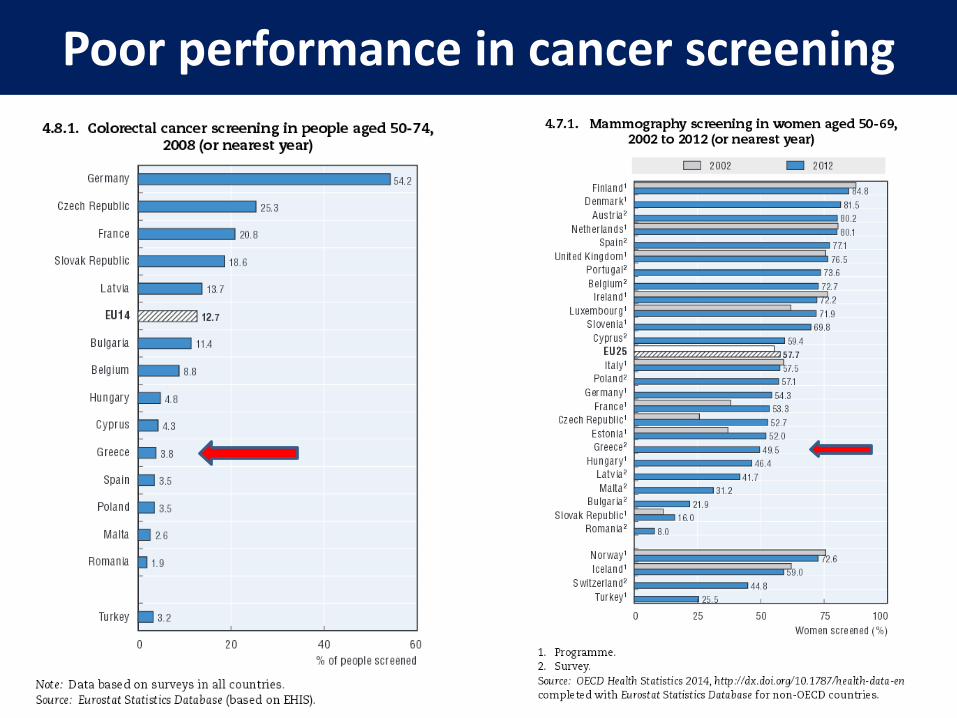
Poor performance in cancer screening
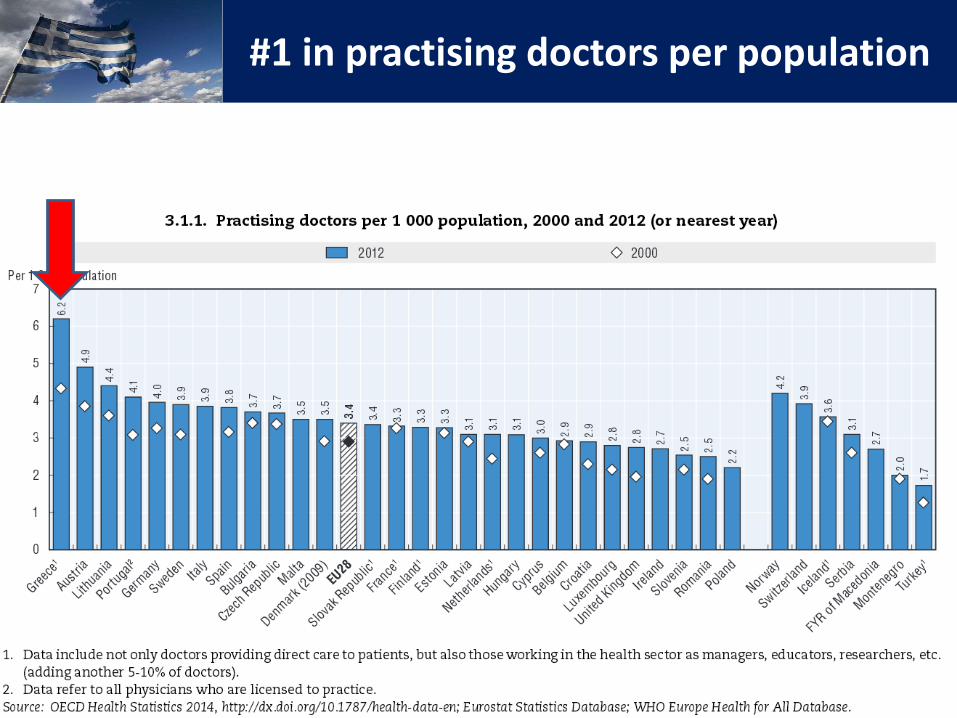
#1 in practising doctors per population
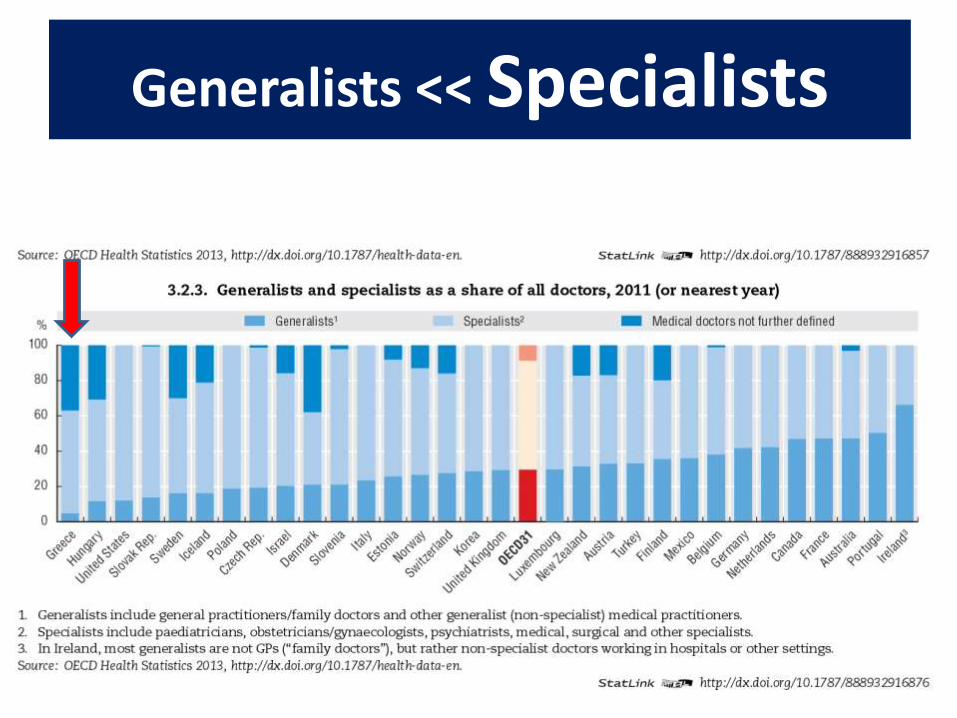
Generalists << Specialists
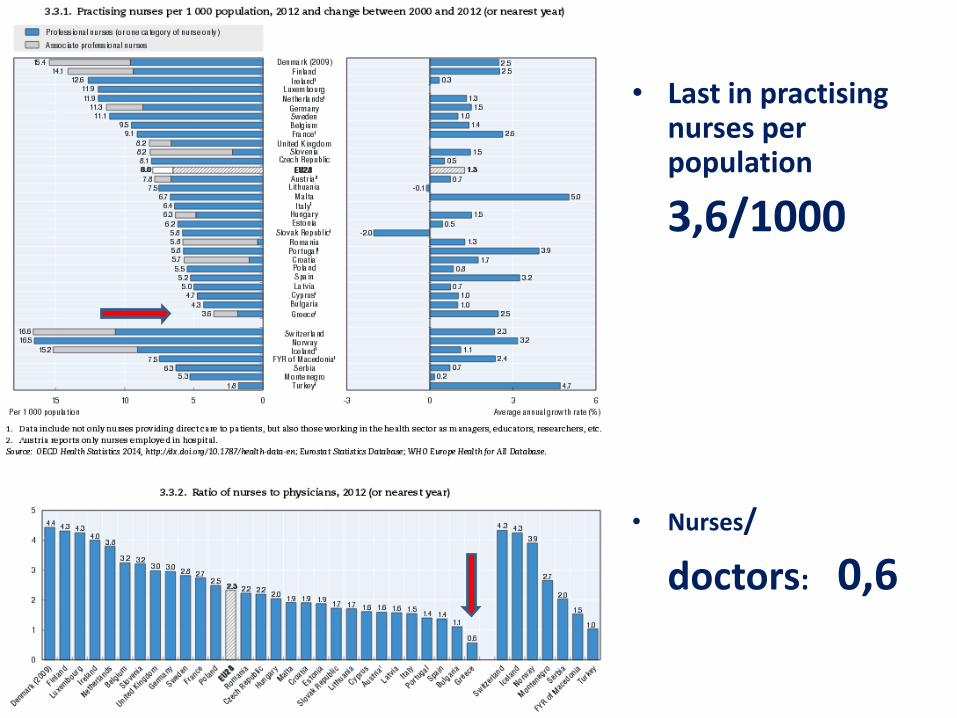
• Last in practising nurses per population
3,6/1000
• Nurses/
doctors: 0,6
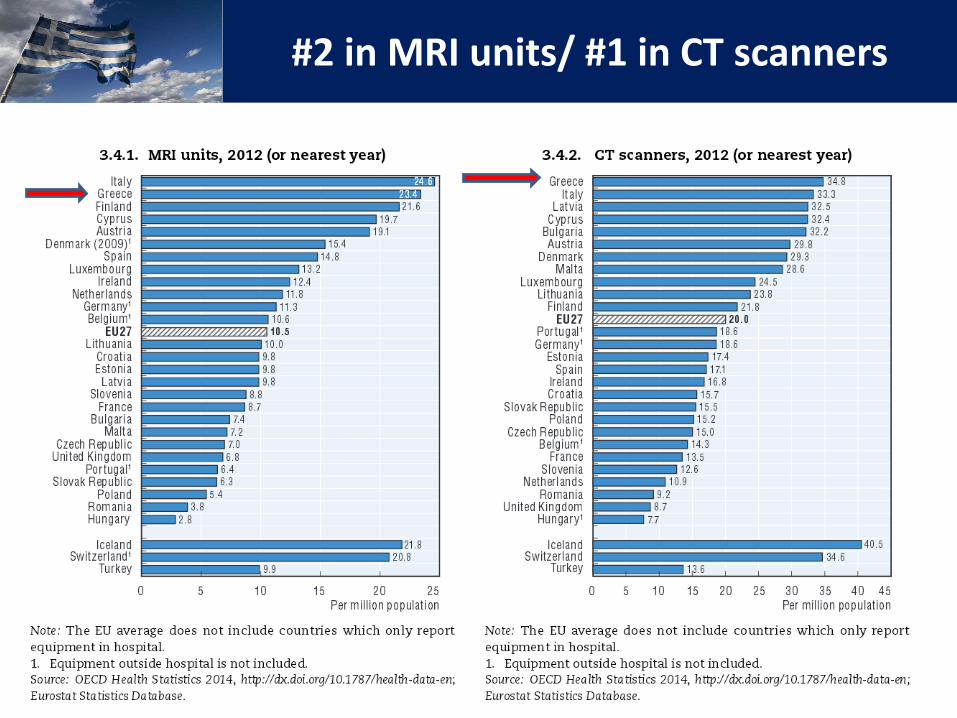
#2 in MRI units/ #1 in CT scanners
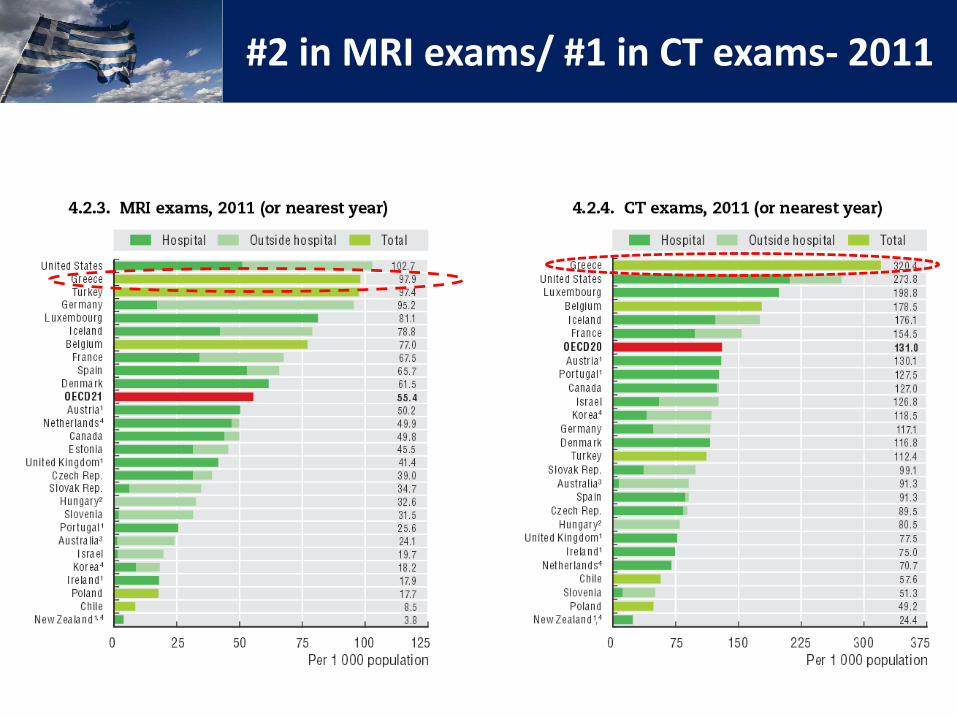
#2 in MRI exams/ #1 in CT exams- 2011
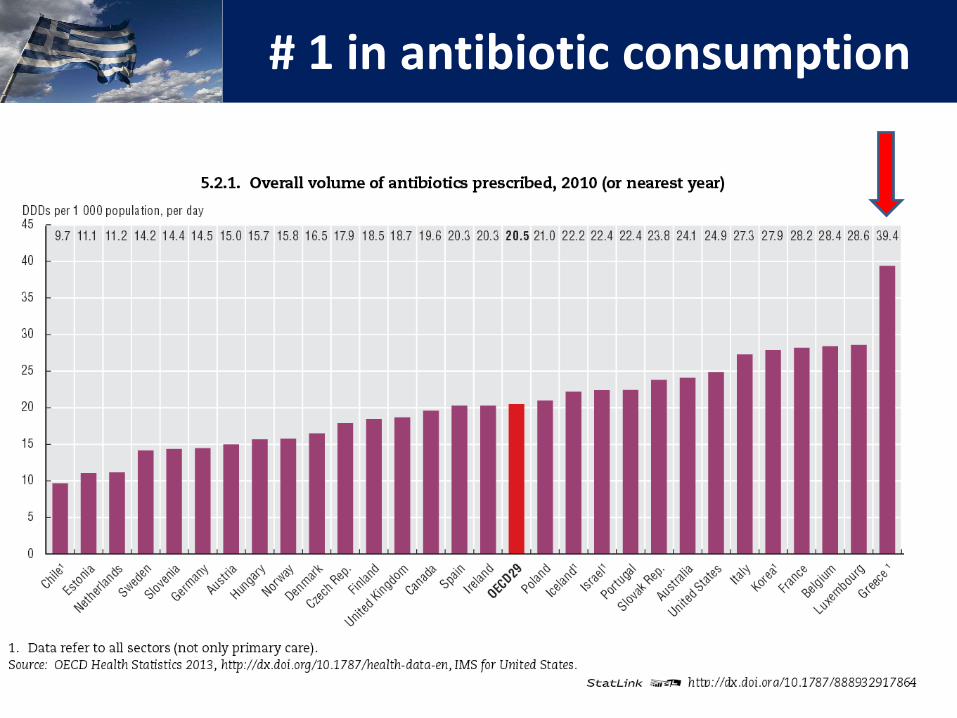
# 1 in antibiotic consumption
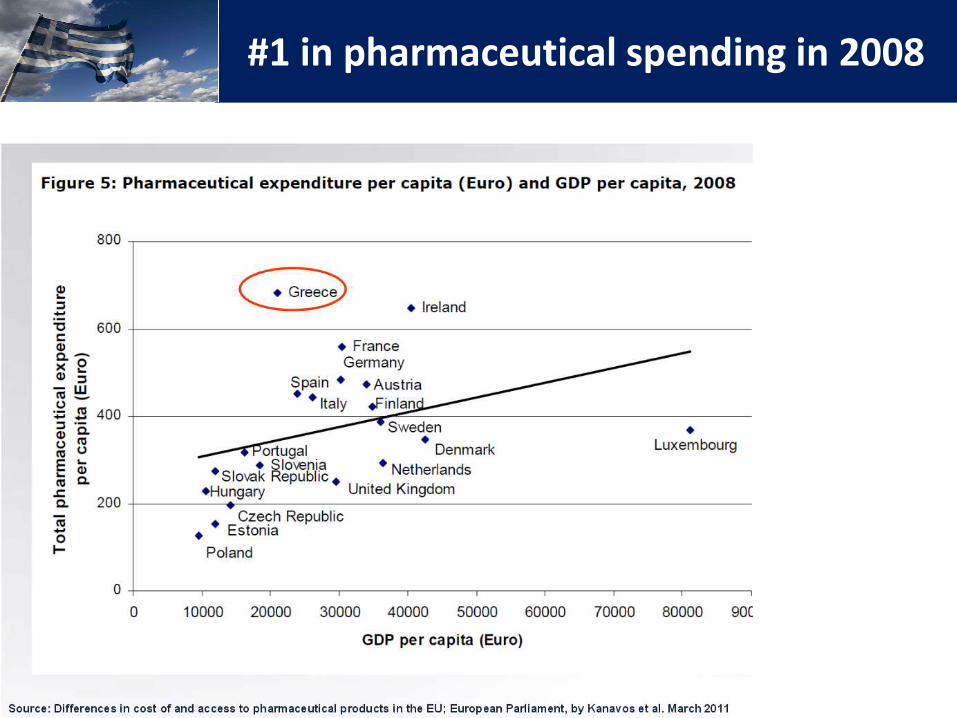
#1 in pharmaceutical spending in 2008
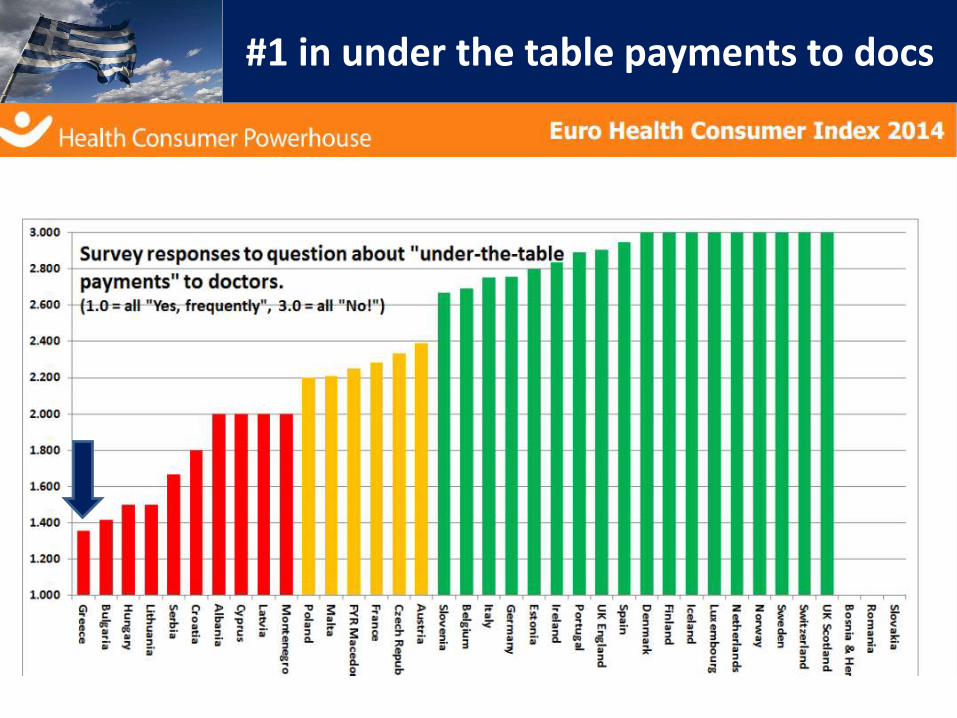
#1 in under the table payments to docs
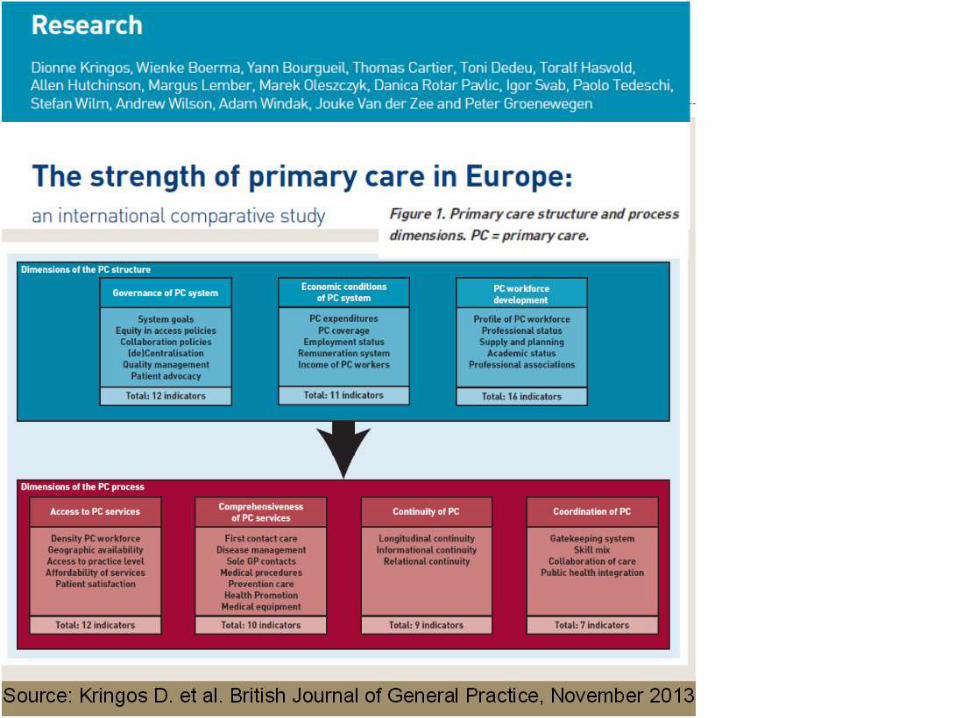
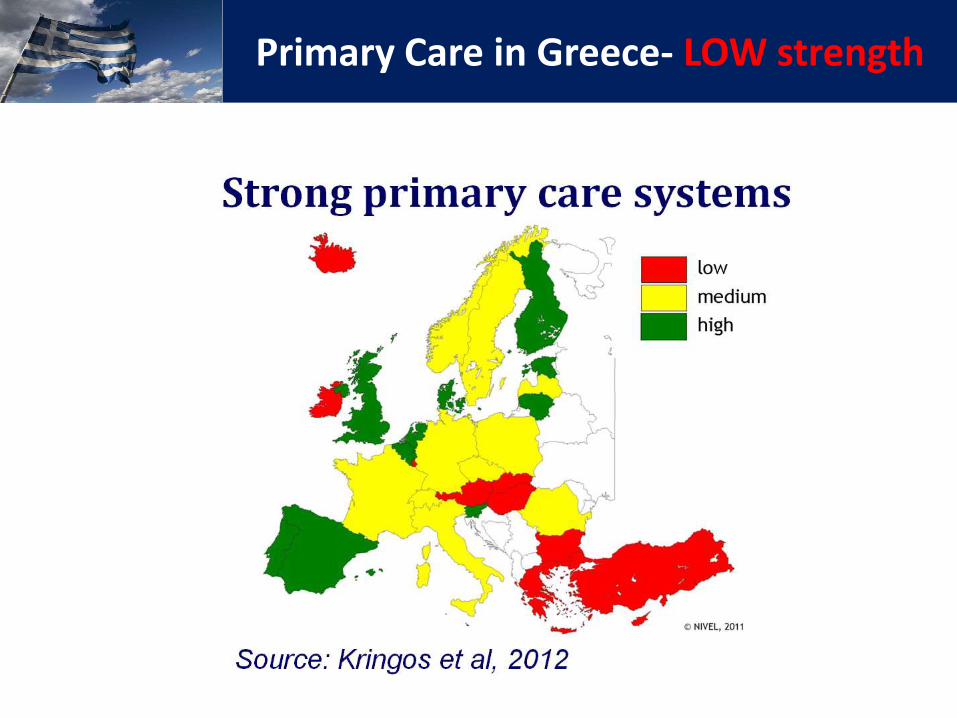
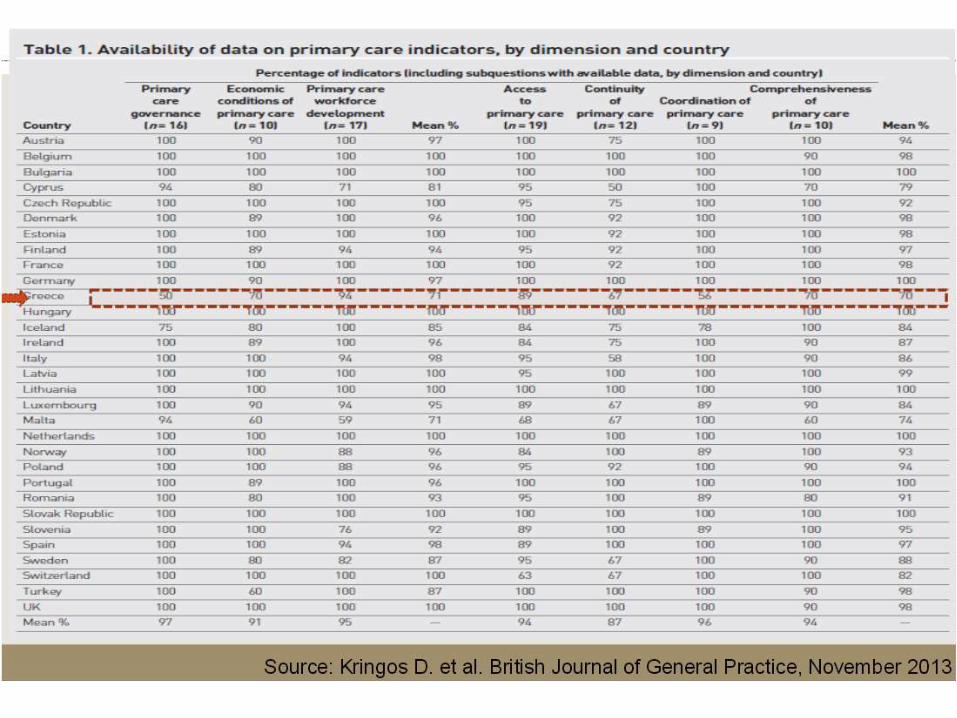
Primary Care in Greece- LOW strength
Governance
• Unclear distribution of responsibilities between central government and local authorities, health insurance funds and NHS, public and private sector.
• No broadly supported vision of Primary Care, priority setting, financing, supply planning and management, service provision or quality monitoring.
Technical Assessment Report: Primary Health Care,Groenewegen P, Jurgutis A- TFGR of the EC
Source: Theodorakis P
Economic conditions for PC
• Low payment for GPs (compared to other specialists / other countries), mainly in salaried service, but also self-employed on fee-for-service basis (potential problem of incentives).
• Large share of private spending and under the table payments
Technical Assessment Report: Primary Health Care
Workforce development
• Unbalanced, lack of GPs and nurses in PC
• No clear job/task description for GPs and other PC providers.
• No policy in health education to redress the balance between generalists and specialists.
• Lack of proper attitudes and public health management competences for the managers of PHC institutions.
Technical Assessment Report: Primary Health Care
Access
• Patient satisfaction with the ease to access GPs was relatively low.
• Access depends on the cost of money (Cost sharing for consultations) or time
• Regional differences in access due to low number of GPs, vacancies
Technical Assessment Report: Primary Health Care
Comprehensiveness
• Often very small role of GPs, limited to prescribing and referring
• Often lacking a community orientation (especially in urban regions).
• Private practices (mostly solo) mainly focus on the patients visiting practice
• Sometimes lack of crucial equipment.
Technical Assessment Report: Primary Health Care
Continuity
• Personal continuity is a problem due to the fragmented health care system. Too many first contact points. Everyone can decide to visit whoever.
• Referral letters are not common.
• No communication between specialists and GPs after the completion of an episode of treatment.
Technical Assessment Report: Primary Health Care
Coordination
• No referral system.
• No information about actual coordination.
Technical Assessment Report: Primary Health Care
Quality
• No information
• Some private practices and diagnostic centres have more advanced quality assurance systems.
Technical Assessment Report: Primary Health Care
Efficiency
• Not enough information to assess
• Monitoring of quantity of services (visits, lab tests etc), but not of the value of care (the outcomes to health)
Technical Assessment Report: Primary Health Care
Equity
• Clear and increasing inequities in health care in Greece.
• Relate to health status, socio-economic status and place of living.
Technical Assessment Report: Primary Health Care
EOPYY
• a new purchasing agency through the merger of health insurance funds, unified benefit package, e-prescribing, monitoring, auditing, claw back, rebates, global budgets
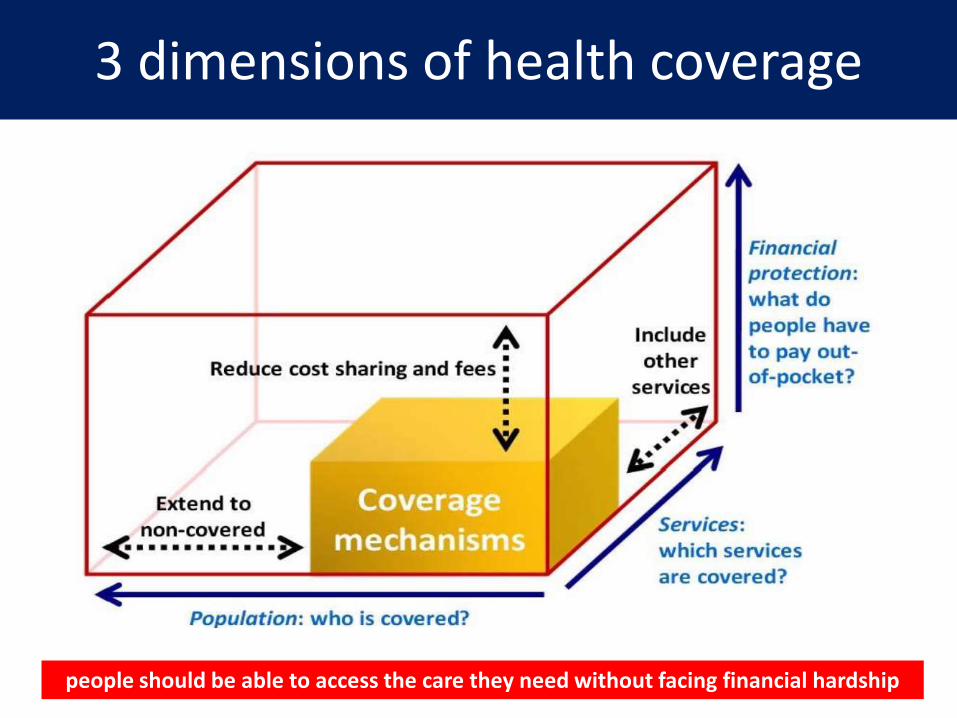
3 dimensions of health coverage
people should be able to access the care they need without facing financial hardship
Extended entitlement of coveragePolicies to extend entitlement to vulnerable groups-
action to protect these people was initially limited, slow and ineffective
OAED: covers long term unemployed for maximum 2 years: 500.000 people
enrolled (7/2014) for more than a year
Coverage of poor: covers poor, uninsured people under strict conditions- low
demand for this coverage: 100.000 people in 2012
Health vouchers (9/2013): covers outpatient visits and diagnostic tests for a
restricted period (4 months). Low demand, only 21.000 issued till 31/1/2014 out of the 230.000 announced for 2013-2014.
PEDY (2/2014): open access to all in PEDY public health centers, but only for visits-
medications, tests not covered
Ministerial decision (6/2014): covers all uninsured, outpatient prescriptions
and inpatient care, as long as they have a referral from the PEDY Public Health Centers and they pay their copayments (as if they were insured)
Lowered depth of coverage by instituting or increasing
patient user charges• outpatient prescription drugs: copayment from 12.85%
(2012) to 29.30%(2014)• diagnostic tests: 15% flat co-payments when private
sector is chosen• inpatient care: 30-50% charge when contracted with
EOPYY private hospital is chosen• outpatient specialist care: 5€ per visit in outpatient
departments of public hospitals/ 45-90 € per private-afternoon visit to a public hospital specialist
• primary care: 5€ per visit in Primary Health Centers, Full payment of GP consultations under ΕΟPΥΥ once cap on consultations is reached (200/month)
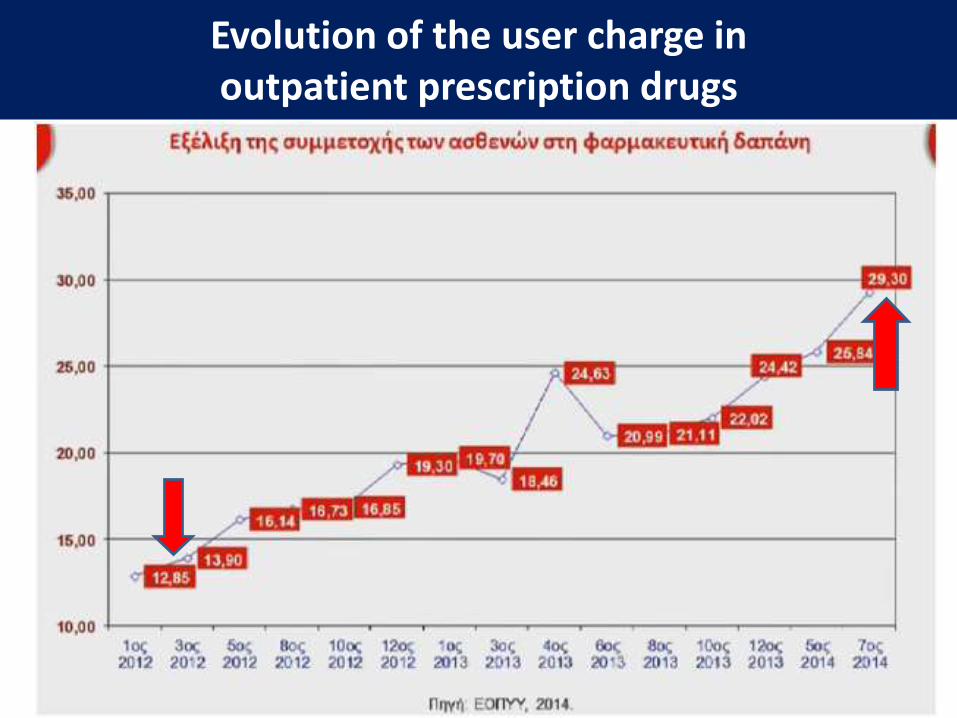
Evolution of the user charge in outpatient prescription drugs
Patient user charges
undermine health system performance:
• little selective effect, reducing appropriate and inappropriate use
• deter people from appropriate and cost-effective care (especially preventive and patient-initiated services)
• negatively affect health, particularly among poorer people
• result in cost-increasing substitution (resource-intensive emergency services instead of cost-effective primary care)
Pharmaceutical expenditure
• National Pharmaceutical Policy (NPP), Pricing, Reimbursement, Generics, Pharmacists profit, Cost sharing, Clinical Practice Guidelines, HTA, Positive list, e-prescription, budget per doctor, monitoring, risk sharing agreement, claw back, rebate, uninsured…
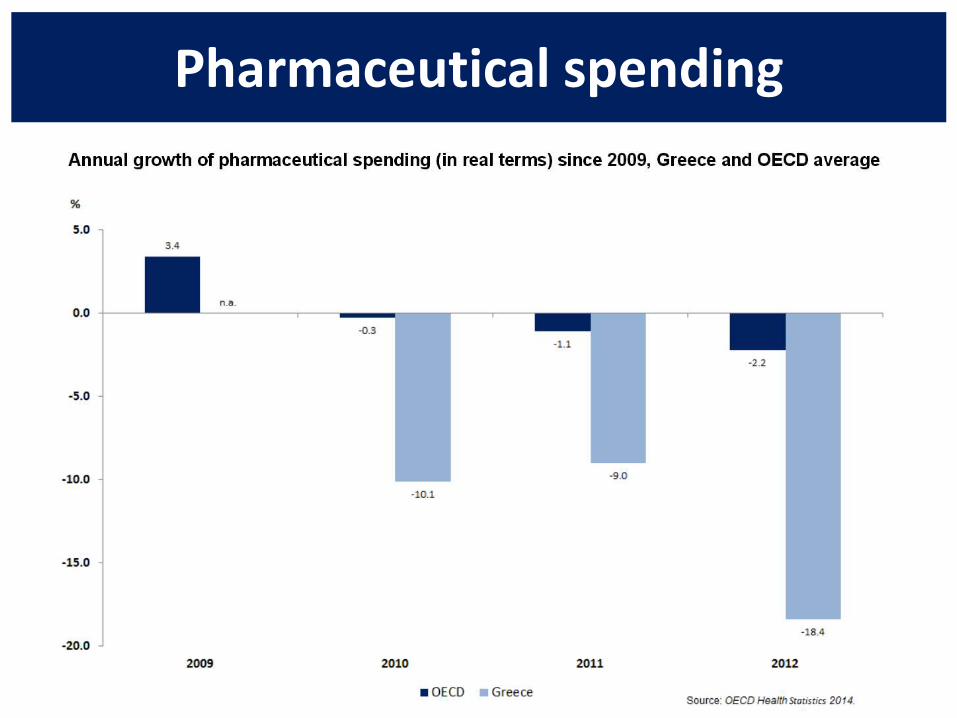
Pharmaceutical spending
Strengthening Primary Care
• Increase funding for primary care
• Reform primary care payment methods
• Shift care out of hospitals
• Improve access to primary care
• Change the skill mix
Economic crisis, health systems and health in Europe: impact and implications for policyWHO Europe/ European Observatory on Health Systems and Policies, 2014
Strong Primary Care
• clear vision on strengthening primary care with GPs as core profession.
• Access to PC with the lowest possible cost-sharing.
• System of stepped access through mandatory referrals to specialist/ hospital care/ diagnostic services.
• Redefined links between PHC and specialist and hospital care
• Patients should be on the list of specific physicians (personal list system).
• freedom of choice for patients of their preferred primary health care provider
• Community orientation of PHC through relations with preventive services, community care and primary level mental health care
Technical Assessment Report: Primary Health Care
Strong Primary Care
• Funding of PC geared to population needs through an adequate resource allocation formula
• Payment of GPs: a mix of capitation, fee-for-services and/or bonuses for specific targets (incentives)
• The level of payment of GPs should be in line with their increased responsibilities.
• Development of PC clinical guidelines
Technical Assessment Report: Primary Health Care
Strong Primary Care
• Development of a system of quality indicators- part of quality improvement cycles at different levels.
• Continuity of care facilitated by well-developed medical records.
• independent monitoring and evaluation
• investment in collecting and analyzing information.
Technical Assessment Report: Primary Health Care
Strong Primary Care
• PC professionals should have clear job descriptions that guide: - educational requirements - contracts
- inform patients on what they can expect from primary care providers.
• Assessment of training needs for PHC doctors and nurses
• Short training courses to obtain core competences, required by job description.
• Policies for education and training of health professionals should address the misbalance between generalists- specialists
Technical Assessment Report: Primary Health Care
Development of a unified Primary Health Care Network-Implementation of the Family Physician
impact of economic crisis on population health
• full scale of the effects may not be apparent for years –especially those due to inadequate and delayed access to health services and breakdowns in the management of chronic disease.
• Mental health has been most sensitive to economic changes. Unemployment and financial insecurity increase the risk of mental health problems.
• There has been a notable increase in suicides.
• Limited evidence of a decrease in general health status and increases in communicable diseases, such as HIV and malaria.
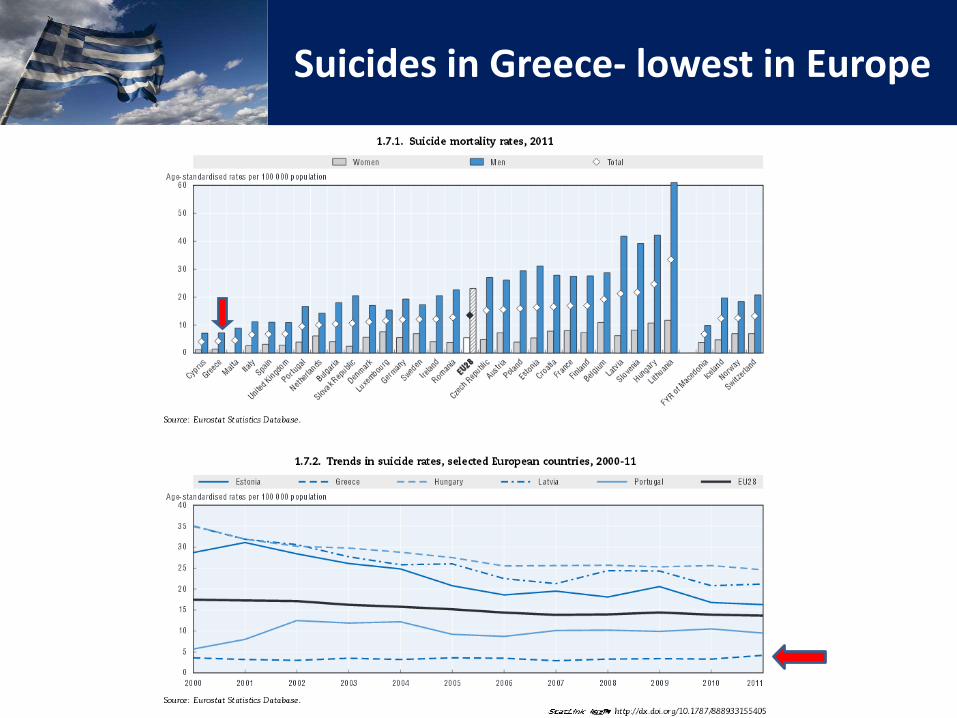
Suicides in Greece- lowest in Europe
Will the new government endanger the PHC reform?
We hope and believe NOT this time!
Top Related